Embed Size (px)
Citation preview

389Annals of Vascular Diseases Vol.5, No.3 (2012)
Case Report
A Rare Case of Septic Deep Vein Thrombosis in the Inferior Vena Cava and the Left Iliac Vein in an Intravenous Drug AbuserYe Xin Koh, MRCS, Jack Kian Chng, MRCS, and Seck Guan Tan, FRCS, FAMS
The patient was a 41 year-old Chinese female, a known intravenous drug abuser (IVDA), who presented with a left inguinal discharging sinus. A computed tomography (CT) scan showed inflammation in the left groin involving the left femoral vein and resulting in thrombus within the iliac veins extending to the distal portion of the inferior vena cava.Septic deep vein thrombosis is a well-recognized complication in intravenous drug abusers (IVDA) when large proximal veins are used for drug injection. Life threatening complications such as septic pulmonary embolism and right sided infective endocarditis may result.The aims of treatment are to prevent the septic thrombus from further embolisation and also to remove the thrombus. Treatment options include catheter directed thrombolysis, mechanical thrombectomy, endovascular treatment, surgical thrombectomy and excision of the involved venous segment.In our patient, we have opted for open surgical thrombectomy without excision of the involved venous segments.
Keywords: inferior vena cava (IVC), septic, deep vein thrombosis (DVT)
Case RepoRt
The patient was a 41 year-old Chinese female, a known intravenous drug abuser (IVDA), who presented with
a history of a 4-day left inguinal discharging sinus. She had associated fever, chills, and rigors. She injected drugs into her left groin two weeks prior to presentation to the hospital. She had no previous history of deep vein throm-bosis (DVT) or PE. There was no history of previous malignancies, oral contraceptive use or recent air travel.
Physical examination was significant for fever at 40 ̊C and a left-inguinal-region sinus discharging purulent material. The lump was not pulsatile. Heart Sounds were dual, and lungs sounds were normal. There was neither
inguinal lymphadenopathy nor evidence of left distal limb infections. The left calf was not swollen or tense.
The laboratory investigation was significant for a raised white cell count 10.75 × 10(9)/L, C-reative protein (CRP) was 66.8 mg/dL. Blood cultures grew Staphylo-coccus aureus and Streptococcus anginosus. The patient was started on IV Crystalline penicillin and Cloxacillin as guided by the antibiotic sensitivities of the cultures. However, despite treatment for a week, there was still persistent bacteremia with Staphylococcus Aureus de-tected in the blood cultures. IV gentamicin was added subsequently.
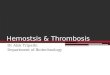
A computed tomography (CT) scan showed inflamma-tion in the left groin involving the left femoral vein and resulting in thrombus within the iliac veins extending to the distal portion of the inferior vena cava. CT pulmonary angiogram showed small cavitary nodules scattered in bilateral lung fields (Fig. 1).
The patient was started on a therapeutic dose of enoxaparin for anticoagulation and underwent an open surgical thrombectomy. The inferior vena cava (IVC)
Department of General Surgery, Singapore General Hospital, Singapore
Received: May 10, 2012; Accepted: June 22, 2012Corresponding author: Jack Kian Chng, MRCS. Department of General Surgery, Singapore General Hospital, SingaporeTel: +65-6321-4051, Fax: +65-6220-9329E-mail: [email protected]
Ann Vasc Dis Vol.5, No.3; 2012; pp 389–392©2012 Annals of Vascular Diseases doi: 10.3400/avd.cr.12.00036
Koh YX, et al.
390 Annals of Vascular Diseases Vol.5, No.3 (2012)
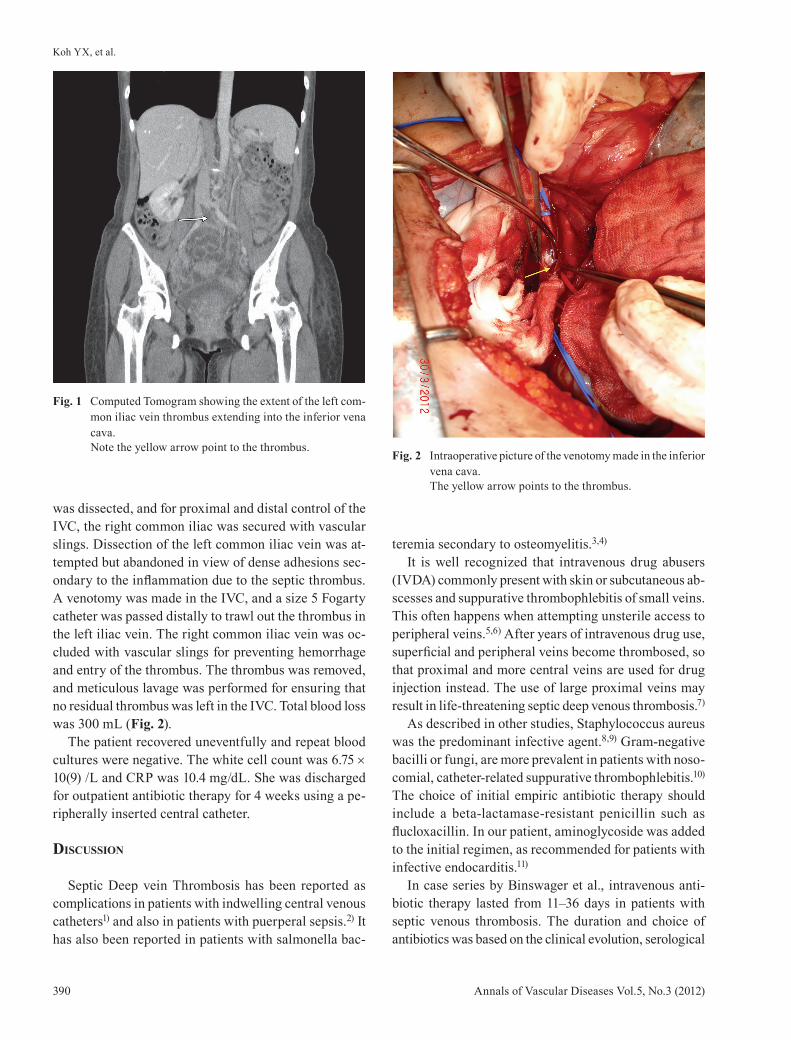
was dissected, and for proximal and distal control of the IVC, the right common iliac was secured with vascular slings. Dissection of the left common iliac vein was at-tempted but abandoned in view of dense adhesions sec-ondary to the inflammation due to the septic thrombus. A venotomy was made in the IVC, and a size 5 Fogarty catheter was passed distally to trawl out the thrombus in the left iliac vein. The right common iliac vein was oc-cluded with vascular slings for preventing hemorrhage and entry of the thrombus. The thrombus was removed, and meticulous lavage was performed for ensuring that no residual thrombus was left in the IVC. Total blood loss was 300 mL (Fig. 2).
The patient recovered uneventfully and repeat blood cultures were negative. The white cell count was 6.75 × 10(9) /L and CRP was 10.4 mg/dL. She was discharged for outpatient antibiotic therapy for 4 weeks using a pe-ripherally inserted central catheter.
DisCussion
Septic Deep vein Thrombosis has been reported as complications in patients with indwelling central venous catheters1) and also in patients with puerperal sepsis.2) It has also been reported in patients with salmonella bac-
teremia secondary to osteomyelitis.3,4)
It is well recognized that intravenous drug abusers (IVDA) commonly present with skin or subcutaneous ab-scesses and suppurative thrombophlebitis of small veins. This often happens when attempting unsterile access to peripheral veins.5,6) After years of intravenous drug use, superficial and peripheral veins become thrombosed, so that proximal and more central veins are used for drug injection instead. The use of large proximal veins may result in life-threatening septic deep venous thrombosis.7)
As described in other studies, Staphylococcus aureus was the predominant infective agent.8,9) Gram-negative bacilli or fungi, are more prevalent in patients with noso-comial, catheter-related suppurative thrombophlebitis.10) The choice of initial empiric antibiotic therapy should include a beta-lactamase-resistant penicillin such as flucloxacillin. In our patient, aminoglycoside was added to the initial regimen, as recommended for patients with infective endocarditis.11)
In case series by Binswager et al., intravenous anti-biotic therapy lasted from 11–36 days in patients with septic venous thrombosis. The duration and choice of antibiotics was based on the clinical evolution, serological
Fig. 1 Computed Tomogram showing the extent of the left com-mon iliac vein thrombus extending into the inferior vena cava.Note the yellow arrow point to the thrombus.
Fig. 2 Intraoperative picture of the venotomy made in the inferior vena cava.The yellow arrow points to the thrombus.
Septic DVT in the IVC in an IVDA
391Annals of Vascular Diseases Vol.5, No.3 (2012)
infection markers and drug side effects.12) According to treatment guidelines, it is recommended that, in patients with infective endocarditis, intravenous treatment should last at least four weeks.11)
Possible complications of the septic thrombus in-clude septic emboli from the infected thrombus, which can result in life threatening pulmonary embolus, and possible right-sided infective endocarditis.13) Thus, the importance of treatment of this problem cannot be over emphasized. In our patient, there was already evidence of septic emboli causing septic pulmonary embolism, hence indicating the need for surgical intervention to prevent a life threatening saddle pulmonary embolus or right-sided infective endocarditis.
The aims of treatment are to prevent the septic throm-bus from further embolisation and also to remove the thrombus which is the source of sepsis. Treatment options of catheter directed thrombolysis, mechanical thrombec-tomy, endovascular treatment, surgical thrombectomy and excision of the involved venous segment have been described in various case reports.6,9,14–16)
In our patient, we have opted for open surgical throm-bectomy without excision of the involved venous seg-ments. As the IVC and iliac veins are major structures and best not sacrificed in the presence of other less destructive treatment options. The successful use of thrombolysis in septic thrombophlebitis has been reported.17) However, there are reports of thrombolysis triggering significant deteriorations presumably from the release of infected emboli into the systemic circulation.14) This patient already had evidence of septic emboli to the lungs and thrombolysis may further worsen these emboli. An IVC filter was not employed due to anatomical location of the IVC septic thrombus, the potential for prosthetic infection, IVC thrombosis, DVT, and even technical interference of the IVC filter with endovascular treat-ment options.18)
Furthermore, there was significant inflammation and adhesion of the left iliac vein and which might have made percutaneous and endovascular methods more difficult. Eventually, venotomy was performed via the inferior vena cava and thrombectomy performed with a Fogarty catheter to good effect.
In conclusion, septic deep vein thrombosis is a rare disease with severe sequelae if not treated aggressively and swiftly. With the advancement of vascular surgery, there are a variety of options available to the modern vascular surgeon. However, the choice of therapy should take into consideration the myriad of variations of the
clinical presentation and anatomy of the problem.
aCknowleDgement
The authors would like to acknowledge Dr Goh Aik Wei for her editorial assistance.
DisClosuRe statement
Koh Ye Xin and coauthors have no conflicts of interest.
RefeRenCes
1) Andes DR, Urban AW, Acher CW, et al. Septic thrombosis of the basilic, axillary, and subclavian veins caused by a peripherally inserted central venous catheter. Am J Med 1998; 105: 446-50. [Medline] [CrossRef]
2) Garcia J, Aboudjaoude R, Apuzzio J, et al. Septic pelvic thrombophlebitis: diagnosis and management. Infect Dis Obstet Gynecol 2006; 2006: 15614. [Medline] [CrossRef]
3) Benenson S, Raveh D, Schlesinger Y, et al. The risk of vascular infection in adult patients with nontyphi Salmonella bacteremia. Am J Med 2001; 110: 60-3. [Medline] [CrossRef]
4) Schifferdecker B, Merchán JA, Ahmar C, et al. Endo-vascular treatment of septic thrombophlebitis: a case report of a rare complication and review of the litera-ture. Vascular Medicine 2009; 14: 47-50. [Medline] [CrossRef]
5) Scheidegger C, Zimmerli W. Infectious complications in drug addicts: seven-year review of 269 hospitalized narcotics abusers in Switzerland. Rev Infect Dis 1989; 11: 486-93. [Medline] [CrossRef]
6) Scheidegger C, Zimmerli W. Incidence and spectrum of severe medical complications among hospitalized HIV-seronegative and HIV-seropositive narcotic drug users. AIDS 1996; 10: 1407-14. [Medline] [CrossRef]
7) Weinberg G, Pasternak BM. Upper-extremity suppura-tive thrombophlebitis and septic pulmonary emboli. JAMA 1978; 240: 1519. [Medline] [CrossRef]
8) Ang AK, Brown OW. Septic deep vein thrombosis. J Vasc Surg 1986; 4: 563-6. [Medline]
9) Kniemeyer HW, Grabitz K, Buhl R, et al. Surgical treatment of septic deep venous thrombosis. Surgery 1995; 118: 49-53. [Medline] [CrossRef]
10) Rupp ME. Infections of intravascular catheters and vascular devices. In: Crossley KB, Archer GL, eds. The Staphylococci in Human Disease. New York: Churchhill Livingstone; 1997; 379–399.
11) Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention, diagnosis, and treatment of infective en-docarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology
Koh YX, et al.
392 Annals of Vascular Diseases Vol.5, No.3 (2012)
(ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J 2009; 30: 2369-413. [Medline] [CrossRef]
12) Binswanger IA, Kral AH, Bluthenthal RN, et al. High prevalence of abscesses and cellulitis among commu-nity-recruited injection drug users in San Francisco. Clin Infect Dis 2000; 30: 579-81.
13) Carozza A, De Santo LS, Romano G, et al. Infective endocarditis in intravenous drug abusers: patterns of presentation and long-term outcomes of surgical treat-ment. J Heart Valve Dis 2006; 15: 125-31.
14) Umeda A, Mori M, Yamaguchi K, et al. Acute septic shockduring thrombolysis in a patient with acute pul-monary thromboembolism. J Infect Chemother 1996;
2: 194-6. [CrossRef] 15) Krauthamer R, Milefchik E. Endovascular treatment
of upperextremity septic thrombophlebitis without thrombolysis. Am JRoentgenol 2004; 182: 471-2.
16) Munster AM. Septic thrombophlebitis. A surgical dis-order. JAMA 1974; 230: 1010-1. [Medline] [CrossRef]
17) Volkow P, Cornejo-Juárez P, Arizpe-Bravo AB, et al. Catheter-related septic thrombophlebitis of the great central veins successfully treated with low-dose strep-tokinase thrombolysis and antimicrobials. Thromb J 2005; 3: 11. [Medline] [CrossRef]
18) Nazzal M, Chan E, Nazzal M, et al. Complications related to inferior vena cava filters: a single-center experience. Ann Vasc Surg 2010; 24: 480-6. [Medline] [CrossRef]