Embed Size (px)
Citation preview
10.1192/bjp.141.1.50Access the most recent version at DOI: 1982, 141:50-53.BJP
G D Shukla, S C Sahu, R P Tripathi and D K GuptaA psychiatric study of amputees.
Referenceshttp://bjp.rcpsych.org/content/141/1/50#BIBLThis article cites 0 articles, 0 of which you can access for free at:
permissionsReprints/
[email protected] To obtain reprints or permission to reproduce material from this paper, please write
to this article atYou can respond http://bjp.rcpsych.org/letters/submit/bjprcpsych;141/1/50
from Downloaded
The Royal College of PsychiatristsPublished by on October 11, 2014http://bjp.rcpsych.org/
http://bjp.rcpsych.org/site/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to

Brit. J. Psychiat. (1982), 141, 50—53
A Psychiatric Study of Amputees
G. D. SHUKLA, S. C. SAHU, R. P. TRIPATHI and D. K. GUPTA
Summary: Psychiatric manifestations were studied in 72 amputees in thepost-operative period. All were right handed. Besidesphantom limb phenomena,which were observed in nearly four-fifths of the cases and are described inanother paper, nearly two-thirds had psychiatric symptoms in the form ofdepression (45 patients), anxiety (38), crying spells (38), insomnia (34), lossof appetite (23), suicidal ideas (21) and psychotic behaviour (2). Right armamputees had phantom phenomena artd insomnia significantly more oftenthan left.
Nearlyone-fifthofthecaseswere diagnosedas havingpsychoticdepressivereactions,two-fifthsas havingdepressiveneurosisand two, both with rightupper limb amputations, asschizophrenic.
Psychiatric aspects of amputation have receivedscarcely any attention. Various aspects of the phantomlimb phenomenon have been studied, to the totalexclusion of other psychiatric sequelae (Handersonand Smyth, 1948; Cronhoim, 1951; Sunderland, 1968;Meizack, 1971 ; Dc Gutierrez-Mahoney, 1970; Carlenet a!, 1978 ; and Wilson et a!, 1978). This is surprising,in view of the significance of the procedure and itsimpact on the patient's future life and adjustment.
The present communication reports a prospectivepsychiatric study of seventy-two consecutive casesundergoing various amputations in an Indian teachinggeneral hospital.
Material and MethodsThe study was carried out in the M.L.B. Medical
College, Jhansi (India). It included seventy-twoconsecutivecasessubjectedto amputationduringaperiod of three years, excluding those with a historyof previous psychiatric illness. The patients wereinterviewed daily for one week and at weekly intervalsthereafter so long as they could be contacted. Patientsdeveloping psychiatric symptoms were seen morefrequently, depending upon their condition. The meanperiod of follow-up was 5.2±1.1 weeks, usuallylimited to the in-patient stay. In every case a reliablerelative was also interviewed. The interviews werebased on a prearranged schedule encompassingsocio-demographic aspects, the cause and site of theamputation, psychiatric features following the procedure and their progress with treatment.
The psychiatric abnormalities were classified inaccordance with the Diagnostic and Statistical Manual
(DSM-2) of the American Psychiatric Association(1968). Patients developing depressive symptoms weretreated with tricyclic antidepressants, anxiolytics andhypnotics. Neuroleptics and hypnotics were used forschizophrenic symptoms. In addition to pharmacotherapy all patients were listened to frequently,patiently and sympathetically and offered emotionalsupport by the psychiatric team. Psychiatric progresswas watched and the findings recorded. At the end ofthe study the data were tabulated and the resultsanalysed statistically.
ResultsGeneral characteristics of cases
The age distribution of our cases is given in Table I.Nearly two-thirds of them were in the age group 10—30years, most commonly in the second decade (26 cases).Most of the patients (68) were male, the sex ratiotherefore being 17:1. The majority were poorlyeducated (24) or uneducated (32), only 11 having beento secondary school and seven to university. Threefifthswerepoorand therestmiddle-class.
Indications for amputation
More thantwo-thirds(50)ofthepatientshad limbsamputated during or following accidents. Of these,43 had crush and the remaining seven had blastinjuries. Threshing-machines accounted for morethan half of the crush injuries. Osteosarcoma necessitated amputation in seven cases. Six limbs werechopped off by dacoits or enemies, Burger's diseaseand electric burns were responsible for three ampu
50
Age(years) No.%of total
sample10—20
263620—30
202830—40
121740—50
45.550—60
45.560andabove
68Total
72100TABLE
II
Site ofamputation (N =72)Right
LeftSiteof
amputation No. % No. %TotalNo.¾Upperlimb
24 63 14 373853Lowerlimb
18 53 16 473447Total
42 58 30 4272 100
SymptomsTotal (72)Upper
limbsLowerlimbsTotal
(38)Right (24)Left (14)Total (34)Right (18)Left(16)Anxiety38(53)19(50)11
(46)8(57)19(56)9(50)10(63)Phantom
limb62 (86)34 (90)24 (lOO)10 (7l)28 (82)15 (83)13(81)Sadness45
(62)23 (61)16 (67)7 (50)22(65)11(61)11(69)Crying
spells38 (53)22 (58)14 (58)8 (57)16 (47)9 (50)7(44)Insomnia34
(47)19 (50)16 (67)13 (2l)t15 (44)7 (39)8(50)Loss
of appetite23 (32)15 (40)11 (46)4 (29)8 (24)3 (17)5(31)Suicidal
ideas@21(29)10 (26)10 (42)—11(32)5 (28)6(38)Psychotic
behaviour2 (3)2 (5)2 (8)————
510. D. SHUKLA, S. C. SAHU, R. P. TRJPATHI AND D. K. GUPTA
tations each and leprosy, madura foot and chronicosteomyelitis for oneeach.
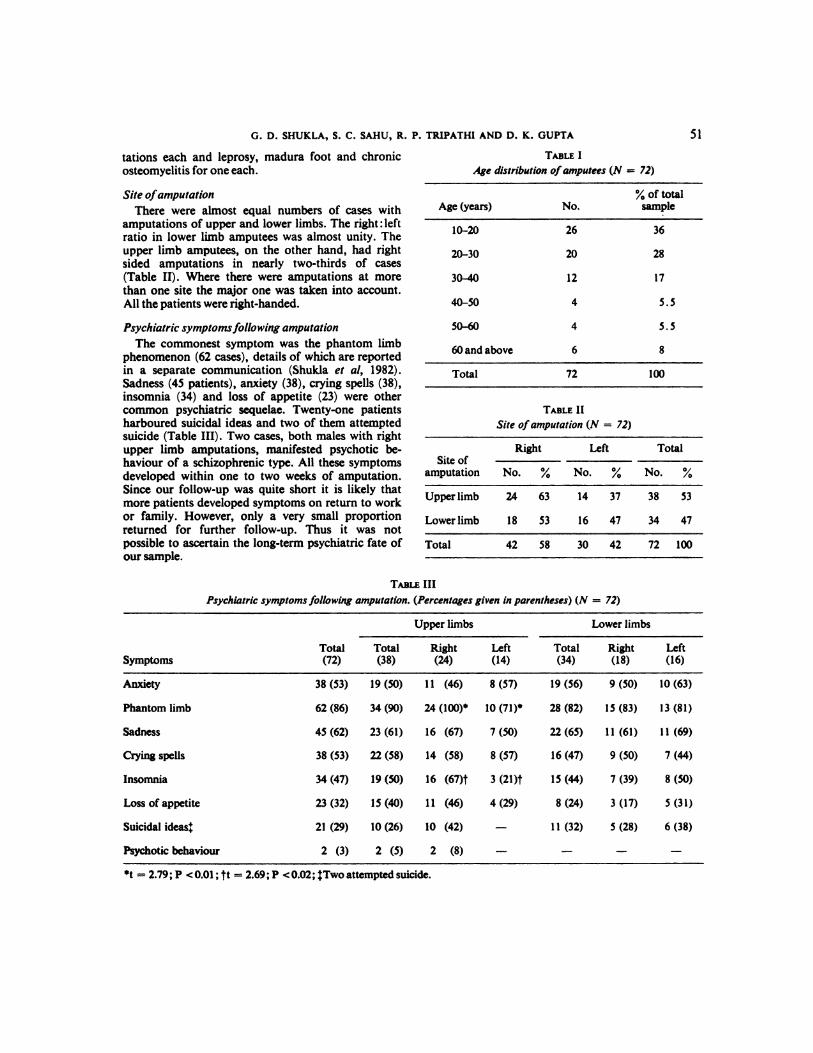
Site of amputationThere were almost equal numbers of cases with
amputations of upper and lower limbs. The right :leftratio in lower limb amputees was almost unity. Theupper limb amputees, on the other hand, had rightsided amputations in nearly two-thirds of cases(Table II). Where there were amputations at morethan one site the major one was taken into account.All the patients wereright-handed.
Psychiatricsymptomsfoiowing amputationThe commonest symptom was the phantom limb
phenomenon (62 cases),details of which are reportedin a separate communication (Shukla et a!, 1982).Sadness(45 patients), anxiety (38), crying spells (38),insomnia (34) and loss of appetite (23) were othercommon psychiatric sequelae. Twenty-one patientsharboured suicidal ideas and two of them attemptedsuicide (Table III). Two cases, both males with rightupper limb amputations, manifested psychotic behaviour of a schizophrenic type. All these symptomsdeveloped within one to two weeks of amputation.Since our follow-up was quite short it is likely thatmore patients developedsymptoms on return to workor family. However, only a very small proportionreturned for further follow-up. Thus it was notpossible to ascertain the long-term psychiatric fate ofour sample.
Psychiatric symptomsfollowing amputation. (Percentagesgiven in parentheses)(N = 72)
TABLE I
Age distribution ofamputees (N = 72)
•¿�t= 2.79; P <0.01 ; tt = 2.69; P <0.02; @Two attempted suicide.

DiagnosisNo.%Normal2535Psychotic
depressivereaction1622Depressive
neurosis29.40Schizophrenia23Total72100.0
52 A PSYCHIATRIC STUDY OF AMPUTEES
Age, sex, education, social class and cause ofamputation did not influence the frequency ofpsychiatric symptoms. Further, there was no differencein the frequency of such symptoms between lower andupper limb amputees or between right and left lowerlimb amputees. In contrast, right upper limb amputeeshad phantom limb phenomena (t = 2.79; P < 0.01)and insomnia (t = 2.69 ; P < 0.02) significantly moreoften than left upper limb amputees (Table III).
Psychiatric diagnosis
When phantom limb phenomena were excludedonly one third of the cases could be considered normalpsychiatrically. Nearly two-thirds had depressivefeatures, ranging from depressive neurosis (29patients) to reactions severe enough to be labelled aspsychotic depression (16 patients). Two patientsmanifested frank thought disorder and emotionalinappropriateness and were diagnosed as schizophrenic(Table IV).
Response to treatment
All the 16 patients with psychotic depressivereactions were feeling better at the time of discharge,nearly two-thirds of them (10 cases) having recoveredalmost completely. Those with depressive neurosishad a somewhat poorer response, nearly three-quarters(22 cases) still having some symptoms at the time ofdischarge. Nine of these 22 had been nervous alltheir lives.
Both the patients with schizophrenic symptomsresponded well to neuroleptics and became symptomfree within a month.
DiscussionAmputation isperhapsthemost ancientof allthe
surgical procedures. However, the earliest amputationswere performed mostly as a form of punishment inmany of the ancient so-called civilized societies, and
[email protected] diagnoses (N = 72)
are still carried out as such even today in someprimitive cultures (Tooms, 1971). It is therefore hardlysurprising that the procedure is, consciously orunconsciously, looked upon as a punitive measure bysome patients.
Facing and undergoing an operation are uniquepsychological and physical experiences for any person(Abrams, 1975). The impact, understandably, islikely to be much more if the procedure entails lossof bodily parts, particularly of limbs. Such procedurestend to become associated with castration anxiety,infantile fear of punishment and whatever cathexesare attached to the organ to be operated upon(Freedman et a!, 1976). Personal mutilation byamputation leads to hostility directed towardssignificant others which, being unacceptable, isrepressed and is replaced by guilt and/or depression(Koib, 1954). Further, psychiatric symptoms may bemanifestations of mourning the loss of a limb thatwas an essential part ofthe patient's body schema.
Some workers have reported certain personalitycorrelates of psychiatric symptoms following amputation or, for that matter, any operation (Parkes,1973; and Solomon and Schmidt, 1978). The patientsdeveloping such symptoms have been found to be atthe rigid end of an ‘¿�adaptable-rigid' dimension andshow dislike of and resistance to change, thus makingcoping with amputation more difficult (Parkes, 1973).Parkes' patients also showed ‘¿�compulsiveselfreliance'. For such individuals the experience ofrelative helplessness and the need to rely on others,however loving, would be a galling and humiliatingone.
However, these personality correlates were difficult,if not impossible, to ascertain in our patients who,being poorly educated and rather unsophisticated,could not provide the necessary details to elucidatetheir personality characteristics. in them it would bereasonable to assume that amputation posed a realthreat to their very livelihood, and to the existence ofthe whole family, the patient generally having beenits most active and probably its only earning member.This was particularly so if the lost limb happened tobe the most active one, i.e. the right arm in a righthanded person. Thus psychological symptomsoccurred more commonly following the amputationof the right arm, though the difference was significantonly with respect to two symptoms, viz phantom limbphenomena and insomnia.
ReferencesAaiw.is,H. 5. (1975)Psychiatryand surgery.In Com
prehensive Textbook of Psychiatry (eds. A. M. Freedman, H. I. Kaplan and B. J. Sadock). Vol. II. Baltimore: Williams & Wilkins.

53G. D. SHUKLA, S. C. SAHU, R. P. TRIPATHI AND D. K. GUPTA
AMERICAN PSYCHIATRIC ASSOCIATION (1968) Diagnosticand Statistical Manual (D.S.M.-2). Washington:AmericanPsychiatricAssociation.
CARLEN, P. L., WALL, P. D., HADVORNA, M. D. & SmmiBACH, T. (1978) Phantom limb and related phenomenain recent traumatic amputations. Neurology,28,211-7.
CRoNHOLM, B. (1951) Phantom limb in amputees. AdaPsychiatricaNeurologicaScandinavica(Supplement),72,1—310.
DE GUTIERREZ-MAHoNEY, C. G. (1970) The treatment ofpainful phantom limb. Surgical Clinics of NorthAmerica, 28,705-8.
FREEDMAN, A. M., KAPLAN, H. I. .& SADocK, B. J. (1976)Modern Synopsis of ComprehensiveTextbook ofPsychiatry.Baltimore:Williams& Wilkins.
HANDERSON, A. M. & Sr&ym, G. E. (1948) Phantom limb.Journal of Neurology, Neurosurgery and Psychiatry,11, 88—112.
Koi@, L. C. (1954) The Painful Phantom:Psychology,Physiology and Treatment. Springfield, Illinois:CharlesC.Thomas.
G.D.Shukia,M.D.,HeadofDepartmentofPsychiatry
S.C. Sahu,M.S.,Readerin Orthopaedics
R. P. Tripathi, M.5..Lecturer in Orthopaedics
D. K. Gupta, M.S.,Lecturer in Orthopaedics
M.L.B. Medical College, Jhansi(U-P), India
MELZACK, R. (1971) Phantom limb pain. Anaesthesiology,35,409—19.
PARKES, C. M. (1973) Factors determining the persistanceof phantom pain in amputees.Journalof PsychosomaticResearch,17,87—108.
SHUKLA, G. D., SAJIu, S. C., TRIPATHI, R. P. & Gupm,,D. K. (1982) Phantom limb: A phenomenologicalstudy. British Journal of Psychiatry.(Acceptedforpublication). 141,54—58.
SOLOMON, P. F. & Scin@imr, K. M. (1978) A burningissue: Phantom limb pain and psychologicalpreparation of the patient for amputation.ArchivesofSurgery,113,185-6.
SuNDriu.ANn, S. (1968) Nerves and Nerve h*JurIes. Baltimore:Williams& Wilkins.
TooMs,R. F. (1971)Amputations.In Campbell'sOperativeOrthopedics (ed. A. H. Crenshaw). Vol. I. Tokyo:IgakuShoin.
WILSON,P. R., PERSON,J. R., Su, D. W. & WANG,J. K.(1978) Herpes zoster reactivation of phantom limbpain. Mayo Clinic Proceedings,53,336-8.
(Received3November;revised28 December1981)