Embed Size (px)
Citation preview

Value-Based Purchasing Discussion
A Presentation to the
Committee on Health Coverage, Insurance and Financial Services
Michelle Probert
Director, Office of MaineCare Services
Maine Department of Health and Human Services 1

Goals for Session
1. Understand basic elements of Value-Based Purchasing
(VBP)
2. Review continuum of alternative payment models
3. Review MaineCare VBP initiatives and efforts toward multi-
payer alignment

3Maine Department of Health and Human Services
What is Value-Based Purchasing?
VALUE =COST
QUALITY
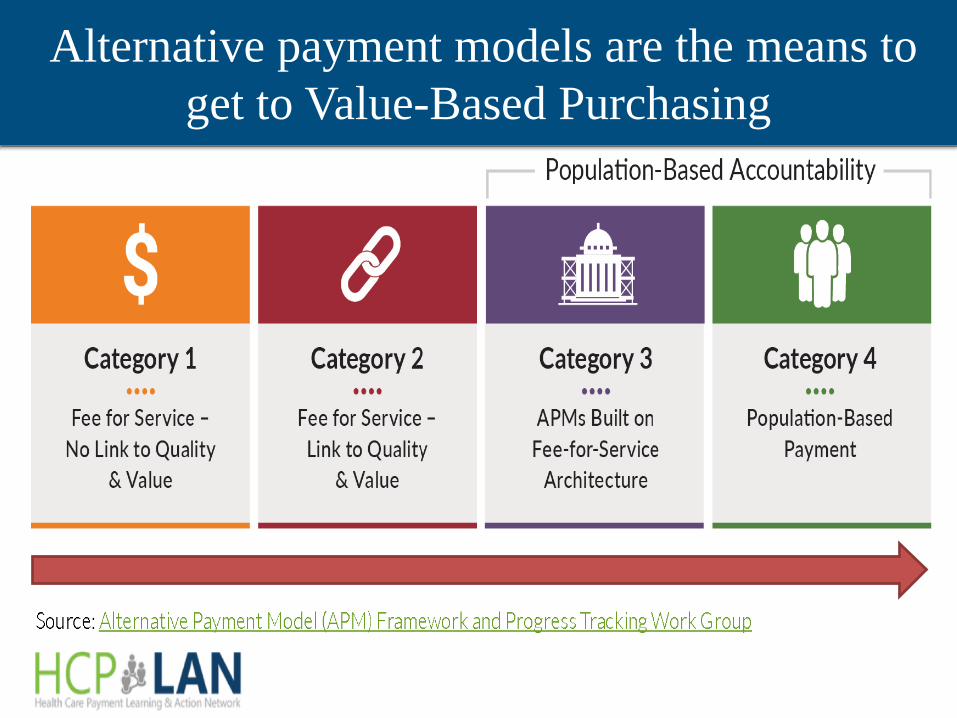
Alternative payment models are the means to
get to Value-Based Purchasing
r-=== Population-Based Accountability
Category 1 Category 2 Category 3 Category4 •••• •••• •••• ••••
Fee for Service - Fee for Service - APMs Built on Population-Based
No Link to Quality Link to Quality Fee-for-Service Payment & Value & Value Architecture
Source: Alternative Payment Model (APM) Framework and Progress Tracking Work Group

But I thought Value-Based Purchasing meant…
5Maine Department of Health and Human Services
• Accountable Care Organizations
• Patient Centered Medical Homes
• Centers of Excellence
?

Exam
ples o
f Initiativ
es Usin
g A
lternativ
e
Pay
men
t Models
6M
aine D
epartm
ent o
f Health
and H
um
an S
ervices
Med
ica
re Sh
ared
Savin
gs P
rogra
m
Carru
m C
enter o
f Excellen
ce, in u
se by S
tate of M
aine
Blu
e Cro
ss Blu
e Sh
ield: H
osp
ital P
4P
BC
BS
of M
ichig
an p
rov
ides b
onu
s pay
men
ts to h
osp
itals wh
o ach
ieve
success in
qu
ality, cost efficien
cy, and
po
pu
lation
health
man
agem
ent, as
lon
g as th
ey h
ave receiv
ed eith
er a CM
S S
tar Ratin
g o
f 2 o
r a Leap
frog
Safety
Grad
e of “C
”
Carru
m co
ntracts w
ith C
enters o
f Excellen
ce to receiv
e pro
spectiv
e bu
nd
led
pay
men
ts for p
roced
ures lik
e join
t replacem
ents an
d b
ariatric surg
ery.
Pro
vid
ers mu
st abso
rb th
e cost o
f any read
missio
ns.
Gro
up
s of p
rov
iders co
mm
it to b
eing
accou
ntab
le for th
e costs
of th
eir Med
icare mem
bers. T
hey
can receiv
e a shared
savin
gs
pay
men
t if they
spen
d lo
wer th
an p
rojected
costs an
d m
eet
qu
ality b
ench
mark
s
It f\
~
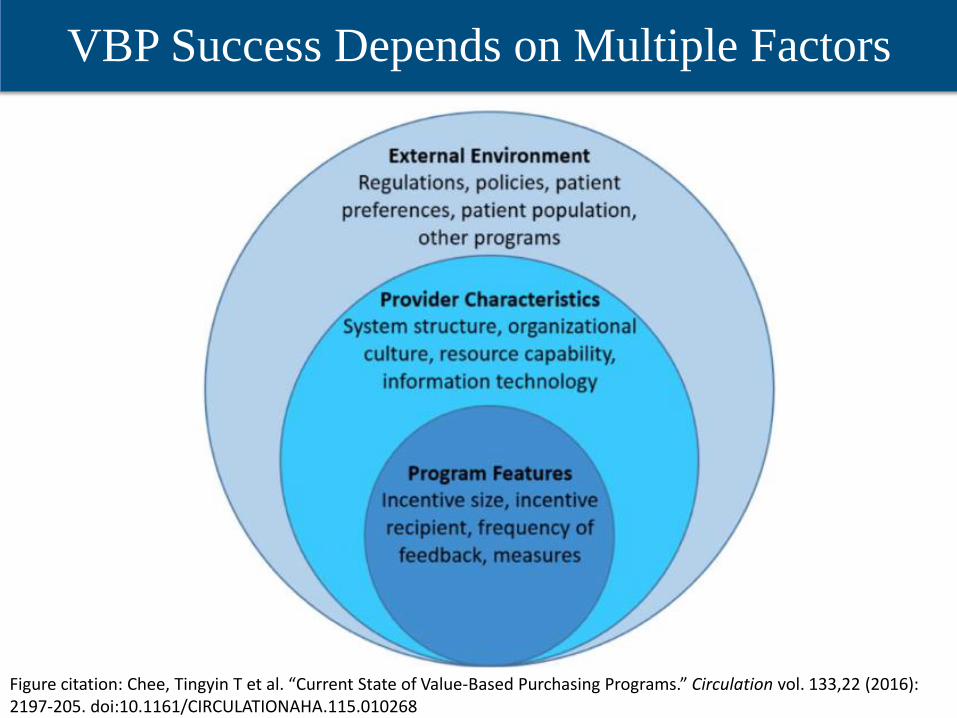
VBP Success Depends on Multiple Factors
7Maine Department of Health and Human ServicesFigure citation: Chee, Tingyin T et al. “Current State of Value-Based Purchasing Programs.” Circulation vol. 133,22 (2016): 2197-205. doi:10.1161/CIRCULATIONAHA.115.010268
External Environment Regulations, policies, pa ien
preferenc s, patien popul tion, o her programs
System s rue ure, organizational cu ure, resource capability,
in orma ion echnology

8Maine Department of Health and Human Services
How is quality measured?
StructureMeasures of a provider’s capacity, systems, & processes
e.g. Provider use of Electronic Health Records, Ratio of providers to patients
ProcessMeasures of actions taken in the course of medical care; often based on widely
accepted clinical recommendationse.g. Percentage of individuals with diabetes receiving blood glucose screening,
Percentage of adolescents with well-care visits
OutcomeMeasures of a group or individual’s health status
e.g. Readmission rate, percent of patients with controlled asthma, functional
outcomes
Patient ExperienceMeasures of an individual’s satisfaction with care
e.g. Consumer Assessment of Healthcare Providers and Systems (CAHPS)

9
Maine Department of Health and Human Services
New York: 15% of
managed LTC
expenditures in
Level 2 or above
by April 2020.Arizona: 70% of
payments for acute
physical claims
linked to VBP by
2021.
State Goals for APMs
Washington:
90% of publicly
funded health
payments linked
to VBP by 2021

2A: Health Homes 3N: Opioid Health Homes
2C: Behavioral Health Homes 3A:
Accountable Communities
CY2018 MaineCare Alternative Payment Model
Results
78% 4% 18% 0%
Population-Based Accountability I
Category 1 Category 2 Category 3 Category 4 •••• •••• •••• ••••
Fee for Service - Fee for Service - APMs Built on Population-Based
No Link to Quality Link to Quality Fee-for-Service Payment & Value & Value Architecture
Source: Alternative Payment Model (APM) Framework and Progress Tracking Work Group

Polling Instructions
11Maine Department of Health and Human Services
We are going to answer a question using a
tool called Poll Everywhere. Your
answers will populate on our computer
screen and display in real time. You will
see everyone’s answers in the visual
display. Responses are anonymous.
First, you will log into the tool via your
cell phone.
5:37 PM
22333
Enter SMS Message :
ERINRIPLEY44S
Send

12Maine Department of Health and Human Services
1) Open your cell phone SMS/text
application.
2) Log into Poll Everywhere by entering
the contact number as 22333 and
sending the message erinripley445.
3) You will receive a text stating you
have joined Poll Everywhere if this is
your first time using this tool.
4) Type your response to the question
into the message field and press send.
Polling Instructions
22333
Enter SMS Message :
ERINRIPLEY44S
Send
13Maine Department of Health and Human Services
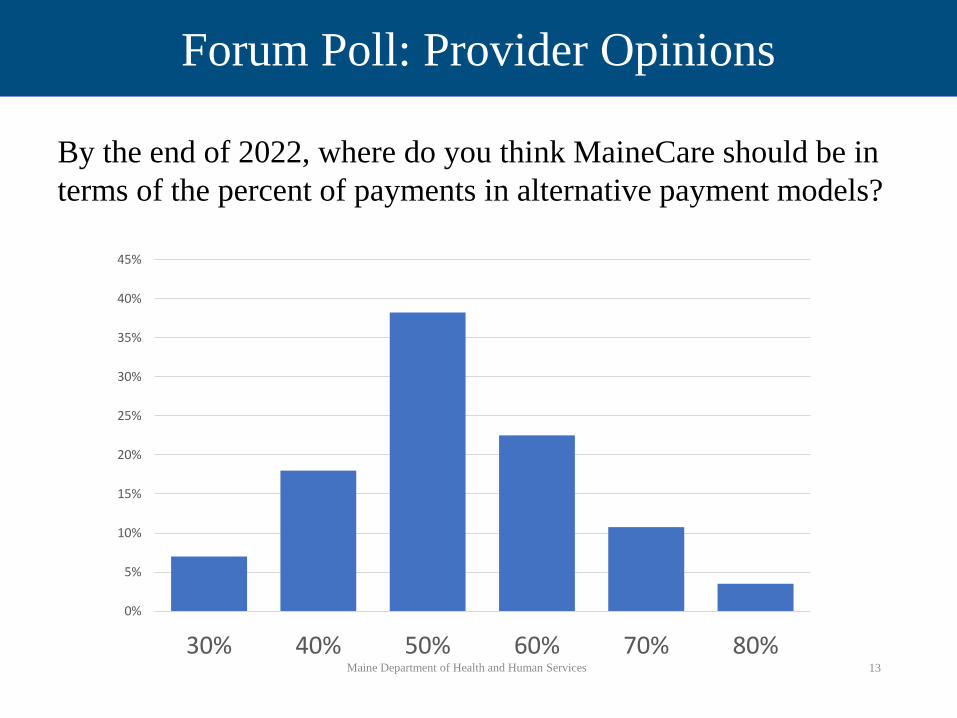
Forum Poll: Provider Opinions
By the end of 2022, where do you think MaineCare should be in
terms of the percent of payments in alternative payment models?
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
30% 40% 50% 60% 70% 80%-

National Goal for Percentage Payment in Shared
Savings and Population-Based APMs
23% 30% 54% 41%2018Maine: 18%
Medicare Traditional Medicaid Commercial Advantage Medicare
2020 .
2022
2025

15
Maine Department of Health and Human Services
MaineCare Value-Based Purchasing Programs
and Alternative Payment Models

Prim
ary C
are Health
Ho
mes, B
ehav
ioral H
ealth
Hom
es, and
Acco
untab
le Com
munities E
nro
llmen
t
16
Main
e Dep
artmen
t of H
ealth an
d H
um
an Services
0
10,0
00
20,0
00
30,0
00
40,0
00
50,0
00
60,0
00
70,0
00
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
2017
2018
2019
Acco
untab
le
Com
munities
Beh
avio
ral
Health
Ho
mes
Health
Ho
mes
There are 9
2,1
20
un
du
plicated
mem
bers acro
ss all three p
rog
rams
+ I +I +

17Maine Department of Health and Human Services
Primary Care
Primary Care Case Management
(PCCM)
• Providers receive a Per Member Per
Month (PMPM) payment for
providing 24/7 coverage and
coordinating care.
• About 60% of MaineCare members
are part of PCCM.
Primary Care Provider Incentive Program
(PCPIP):
• Bonus payment made to independent
primary care providers, based on their
comparative performance on certain
measures related to member access,
utilization, and quality.
• Payments total $2.6M annually.
C.ATEGORY2 FEE FOR SERVICE -LINKTO QUALITY
&VALUE
A Foundational Payments
for Infrastructure & Operations
(e.g. , care coordination
fees and paymen s for HIT inves ·men· s}
C Pay-for-Performance
(e.g., bonuses for uality per ormance)
18Maine Department of Health and Human Services
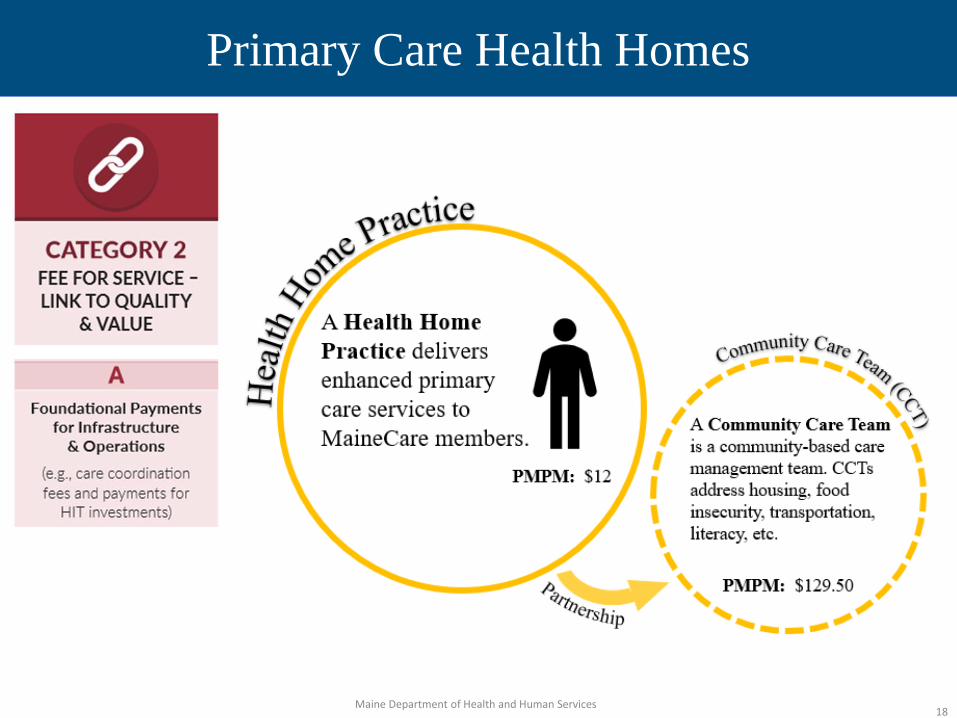
Primary Care Health Homes
CATEGORY2 FEE FOR SERVICE -LINK TO QUALITY
& VALUE
A Foundational Payments
for Infrastructure & Operations
(e.g., care coordina ·on fees a d paymen s or
HIT inves men s)
!i!
-oiact1ce e, \. ~ ~
:$" A Health Home ~ P1:actice delivers
~ enhanced pri.J.uary care services to MaineCare members.
PJ.\O>l\l: 12 I I
A Community Care TeaDl is a cominuni.ty-1based care managen1ent tea1n .. CCTs address housing food
I insecurity. transpm1atioo, \ literacy de.
\
I I I
I , .----,._ ' Pl\lP_ I: $129.50 ~

19Maine Department of Health and Human Services
Primary Care: MaineCare’s Next Steps
1. Grow enrollment in PCCM and Health Homes
2. Explore alignment with Center for Medicare &
Medicaid Innovation (CMMI) Primary Care First
Initiative
3. Simplify MaineCare’s primary care initiatives into one
4. Tie payment to quality for all foundational payments
5. Explore further movement along the APM continuum
and Beyond!
C.ATEGORY2 FEE FOR SERVICE -LINK TO QUALITY
&VALUE
A Foundational Payments -+
for Infrastructure & 01Perations
(e.g., care coordination
fees and pay en s or IT inves men s}
C Pay-for-Performance
(e.g., bonuses for uaility p-er ormance) ..

20Maine Department of Health and Human Services
Behavioral Health Homes (BHH)
CATEGORY2 FEE FOR SERVICE -LINK TO QUALITY
&VALUE
C Pay-for-Performance
(e.g., bonuses for uality performance)
. or amzatj0.J]
Behavioral Health Home

21Maine Department of Health and Human Services
Behavioral Health Homes (BHH) Next Steps
1. Evaluate BHH Model alongside comparable services
(Community Integration, Targeted Case Management)
2. Move toward a more unified model of care coordination
for adults with Serious Mental Illness and kids with
Serious Emotional Disturbance
3. Re-visit current Pay for Performance model and metric
4. Explore potential for integration of services such as
medication management into the model, or for the
introduction of a higher level of service to act as a step-
down for individuals reeving Assertive Community
Treatment (ACT)
CATEGORY2 FEE FOR SERVICE -LINK TO QUALITY
& VALUE
C Pay-for-Performance
(e.g., bonuses for uality performance)

22
Opioid Health Homes (OHH)
Does not get counted in APM %
CATEGORY3 APMS BUILT ON
FEE-FOR-SERVICE ARCHITECTURE
3N Risk I ents
NOT Unk:ed to Quality
• an1zatj01J
A Opioid Health Home is an organization that provides a team-based approach to care for individuals receiving office-based Medication Assisted treatment.
PMPM is based on servicelevel and team composition
C Dor.'<}· · IIJation
otb.et Service88 .
----- ii-Oct . ," ,,~~ , ~ 4, , ,~
I \ I • Behavioral health \ I • HIV ca1·e I I • Primary care I \ • Social service agencies I \ I ' , ', ,, , _____ ,

OHH Enrollment
23Maine Department of Health and Human Services
0 0 0 0 10 39 39 35 41 31
254 292364 373 425 410 403 447 496 519
594733
837966
1144
135814611491
1 2 3 2 1 4 2 3 10 7
2520
21 2142 86 124
150190 215
182
187
216
214
222
221
225 243
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
2017 2018 2019
Opioid Health Homes Member and Uninsured Monthly Attestations Opioid Health Home Member Attestations Opioid Health Home Uninsured Client Attestations■ ■
_ ______ 11 I

24
Opioid Health Homes (OHH) Next Steps
1. Continue to grow enrollment in
program
2. Introduce pay for performance
model and metrics
3. Propose additional changes to:
• Improve access to Opioid Use
Disorder treatment
• Better integrate with primary
care
• Meet the needs of individual
members in treatment
C.ATEGORV3 APMS BUILT ON
FEE-FOR-SERVICE ARCHITECTURE
3N Risk Based Payments
NOT Linked to Quality
CATEGORY4 POPULATION -
BASED PAYMENT
A Con diti o n-S peoific Population-Based
Payment
(e.g., per member per month paymen s, payments for
specialty serv ices, such as oncology or mental health)

25Maine Department of Health and Human Services
Accountable Communities (AC)
CATEGORV3 APMS BUILT ON
FEE-FOR-SERVICE ARCHITECTURE
A APMswith
Shared .Savings
(e.g., shared sav ings wi h upside risk only)
B APMswith
Shared .Savings and Downside Risk
(e.g., e iso e-based payme s or proce ures
and co prehensive payme ts with upside
an downsi e risk)
.~munit Gc\i~
~~ ~ ~
:::J An Accountable Community is a group 8 of providers who take responsibility for U the cost and quality of care for attributed
"'< 1nembers through a shared savings model.
(D Meet cost benchmarks
+ Q) Quality achievement
$ Shared Savings Payment

26Maine Department of Health and Human Services
Accountable Communities (AC) Performance
First 3 Years of AC Initiative
Shared Savings payments to 4 AC’s Over $4M
Savings to MaineCare from 4 AC’s Over $24M
Minimum # of ACs who have received shared savings each year
2
Largest shared savings payment to an AC $1.1M
Range of quality scores for ACs receiving shared savings payments
72% – 95%
27Maine Department of Health and Human Services
Accountable Communities (AC) Next Steps
1. Move ACs toward assumption of downside risk
2. Promote partnership with community-based
organizations to move ACs beyond accountability for
“traditional” healthcare services to better serve high
need members
3. Incent screening and referral for social health needs
CATEGORV3 APMS BUILT ON
FEE-FOR-SERVICE ARCHITECTURE
A APMswith
Shared .Savings
(e.g., shared sav ings w i h upside risk only)
Shared .Savings aind Downside Risk
(e.g., episo e-based paymen s or procedures
and comprehensive payments with upside
nd downside ris
28
Maine Department of Health and Human Services
What Else?
• MaineCare assessing opportunity for APMs as a part
of its evaluation of its current rate setting system
• CMMI’s multi-payer Rural Health Model
• Episodes of care/ bundled payments for maternity,
other services
• Provide greater flexibility through bundled payment
models with links to quality for:
• Assertive Community Treatment
• Care Coordination Services for individuals with
Long Term Services and Supports needs

Michelle Probert
Director
Office of MaineCare Services
29Maine Department of Health and Human Services
Questions





























