Embed Size (px)
Citation preview

A New Formula for Rapid Assessmentof Pericardial Effusion Volume
by Computed Tomography
Michael Groth, MD, Marc Regier, MD, Kai Muellerleile, MD,Peter Bannas, MD, Gerhard Adam, MD, Frank Oliver Henes, MD
Ac
FranCGHNto
ªdo
71
Rationale and Objectives: The aim of this study was to evaluate a new formula for the rapid assessment of pericardial effusion (PE)
volume by computed tomography.
Materials and Methods: Twenty computed tomographic scans positive for PE were reviewed by two observers. Diameters of PE were
measured at four locations. Additionally, PE volume was assessed by volumetry. The correlation between PE diameters and volume
was evaluated, and a linear equation was derived for each diameter location. To test validity and reliability of the measurements, intraclass
correlation and Bland-Altman analysis were performed.
Results: Good validity was expressed by strong correlations between diameter measurements at all four locations and PE volume (all
R values >0.80 and P values <.0001). Intraclass correlation (all coefficients >0.75) and Bland-Altman analysis revealed good interobserver
and intraobserver reliability of diameter measurements. The best values were observed for apical diameter measurements. The followinglinear equation was derived for apical diameter measurements: PE volume = 296 (mL/cm) � apical diameter (cm) � 32 mL.
Conclusions: PE volume can rapidly be assessed by apical PE diameter measurement using the simplified formula PE volume =
0.3 (L/cm) � apical diameter (cm).
Key Words: Pericardial effusion; computed tomography; volume; formula.
ªAUR, 2012
The heart is surrounded by the pericardium, which
consists of two layers. The outer layer is called the
parietal pericardium and the inner layer the visceral
pericardium (1,2). The space between the two layers, the
pericardial cavity, normally contains a small amount of
pericardial fluid, typically between 15 and 50 mL (1,3,4),
which reduces friction within the pericardium by allowing
the pericardial layers to glide over each other with every
heartbeat. Abnormal accumulation of fluid in the pericardial
cavity is called pericardial effusion (PE). The etiology of
PE can be idiopathic, iatrogenic, metabolic, or caused by
neoplasia, infection, or connective tissue disease (5–8). If
a critical rate of pericardial fluid accumulation relative to
pericardial stretch is reached, increasing intrapericardial
pressure can lead to a severe decrease in cardiac function (9).
This life-threatening condition is called cardiac tamponade.
The critical pericardial fluid volume that leads to cardiac
ad Radiol 2012; 19:718–722
om the Center for Radiology and Endoscopy, Department of Diagnosticd Interventional Radiology (M.G., M.R., P.B., G.A., F.O.H.), and theenter for Cardiology and Cardiovascular Surgery, Department ofeneral and Interventional Cardiology (K.M.), University Medical Centeramburg-Eppendorf, Martinistraße 52, 20246 Hamburg, Germany. Receivedovember 24, 2011; accepted January 25, 2012. Address correspondence: M.G. e-mail: [email protected]
AUR, 2012i:10.1016/j.acra.2012.01.008
8
tamponade depends on whether the volume increases slowly
or rapidly over time. Nevertheless, volumes of nonhemorrha-
gic effusions ranging from 300 to 600 mL have been reported
to cause cardiac tamponade (9).
In certain patient cohorts, PE can be frequently detected
as an incidental finding on computed tomographic (CT)
examinations. For example, the incidence rate of PE in
patients undergoing CT imaging of the pulmonary arteries
for suspected pulmonary embolism ranges between 2% and
5% (10–12).
PE volume can be calculated using CT volumetry (13).
Because of the need to measure PE area on various CT slices,
CT volumetry is very time consuming. Nevertheless, estima-
tion of PE volume is important for clinicians to evaluate
hemodynamic relevance and to consider relief by pericardial
paracentesis.
For this reason, the aim of this study was to introduce a new
formula for the rapid assessment of PE volume by CT
imaging.
MATERIALS AND METHODS
Study Population
With the use of our radiology information system, 20 patients
(eight women, 12 men; mean age, 61.6� 14.0 years) with PE

Academic Radiology, Vol 19, No 6, June 2012 PERICARDIAL EFFUSION VOLUME ASSESSMENT BY CT
were identified among 915 contrast-enhanced thorax-only
CT examinations and included in this study. Institutional
review board approval was obtained for this retrospective
study.
Imaging Technique
All CT studies were performed by one of three multidetector
CT (MDCT) scanners available at our institution, which
include a 16-slice MDCT scanner (MX 8000IDT; Philips
Healthcare, Best, The Netherlands), a 64-slice MDCT
scanner (Brilliance 64; Philips Healthcare), and a 256-slice
MDCT scanner (Brilliance iCT; Philips Healthcare). All
examinations were performed with either the contrast-
enhanced thorax protocol (protocol A) or the pulmonary
angiographic protocol (protocol B).
The scan parameters for protocol A using the 16-slice,
64-slice, and 256-slice MDCT scanners, respectively, were
as follows: rotation time, 0.75, 0.75, and 0.5 seconds; collima-
tion, 16 � 1.5, 64 � 0.625, and 128 � 0.625; and tube
voltage, 120, 120, and 120 kV. Effective tube current was
automated.
The following scan parameters were used for protocol B
using the 16-slice, 64-slice, and 256-slice MDCT scanners,
respectively: rotation time, 0.75, 0.75, and 0.33 seconds;
collimation, 16 � 1.5, 64 � 0.625, and 128 � 0.625; and
tube voltage, 120, 120, and 120 kV. Effective tube current
was automated.
Scan volume included the entire chest from the lung apex
to the lung base. CT images were obtained in a single
breath-hold at end-inspiration in the supine position.
Protocol A consisted of the administration of 70 to 80 mL
of nonionic contrast material with an iodine concentration of
300 mg/mL (Imeron 300; Bracco Altana Pharma, Milan,
Italy) injected at a rate of 2 mL/s through a 20-gauge or
18-gauge peripheral intravenous catheter. Imaging was
performed 40 seconds after injection.
Protocol B included the administration of 80 to 100 mL of
nonionic contrast material with an iodine concentration of
400 mg/mL (Imeron 400; Bracco Altana Pharma) injected
at a rate of 4 mL/s through an 18-gauge peripheral intrave-
nous catheter placed in the antecubital vein. The threshold
level for triggering the scan was achieved when the attenua-
tion of the main pulmonary artery measured $130 Houns-
field units (HU).
Image Analysis
All studies were evaluated using standard window and level
settings (protocol A: width, 360 HU; level, 60 HU; protocol
B: width, 560 HU; level, 60 HU). The reviewers were
allowed to change these settings and to zoom into areas of
interest. The CT data set was reconstructed at 5.0-mm and
3.0-mm slice thicknesses for protocols A and B, respectively.
Additional coronal reformations with section thicknesses of
5.0 and 3.0 mm, respectively, were reconstructed as well.
CT scans were reviewed independently by two observers
(M.G. and F.O.H., each with 4 years of experience in CT
imaging). Measurements of pericardial fluid volumes were
measured once by each of the two observers. Diameter
measurements were measured twice by the first (M.G.) and
once by the second (F.O.H.) investigator. There was a 4-
week interval between the readings of the first investigator.
For the calculation of PE volume, a region of interest was
drawn around the PE area on every CT slice (13). The volume
was calculated by multiplying the sum of areas from each slice
by the reconstruction interval.
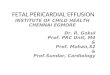
PE diameters were measured at four predetermined
locations: superior aortic recess (SAR), anterior, posterior,
and apical (Fig 1).
The SAR is the superior extent of the pericardial transverse
sinus. It is located anterior to the aorta and pulmonary artery,
forming a cleft as it indents between the great vessels (1). The
transverse extension of the SAR was measured from the
indention between the great vessels at the level of right pulmo-
nary artery and the most ventral portion of the SAR (Fig 1a).
Anterior PE was measured as the largest diameter in front of
the right ventricle and posterior pericardial fluid as the largest
diameter behind the mid posterior free wall of the left
ventricle (Fig 1b). Both measurements were done in the
transverse plane.
The diameter of apical PE was assessed as the widest
distance between the left ventricular apex and the most apical
part of the parietal pericardium in the coronal plane (Fig 1c).
Statistical Analysis
Statistical analysis was performed using Microsoft Excel 2003
(Microsoft Corporation, Redmond, WA) and MedCalc for
Windows (MedCalc Software, Mariakerke, Belgium).
Reliability is the capability of a method to give the same
results in the same observer on different occasions (intraob-
server reliability) or with different observers on the same occa-
sion (interobserver reliability). It expresses the reproducibility
of a method (14). Validity assessesses whether a test is actually
measuring what it is indicating to measure and therefore
expresses the measurement accuracy (14).
Reliability was examined using the intraclass correlation
coefficient (ICC) to assess the agreement of measurements
and Bland-Altman analysis to present the bias and limits of
agreement (15–17). For interobserver reliability of diameter
measurements, the first or second measurement from the
first observer was compared to the measurement from the
second observer. For even consecutive inclusion numbers,
the first measurement of the first observer was used, and for
uneven numbers, the second was used. An ICC >0.75 was
considered to signify good agreement.
Validity was assessed by comparing the volumetric and diam-
eter measurements of both observers using Pearson’s correlation
coefficient. Moreover, a linear equation was derived for each
diameter location. A correlation coefficient >0.80 has been
considered strong, between 0.80 and 0.50 moderate, between
719

Figure 1. Diameter measurements ofpericardial effusion (PE) at four predefined
landmarks. The largest diameter of fluid
within the superior pericardial recess was
measured in transverse orientation betweenthe ascending aorta (AA) and the main
pulmonary artery (MPA) at the level of right
pulmonary artery (RPA) (white double arrow
in a). Anterior PE was measured in front ofthe right ventricle (RV) (white double arrow
in b) and posterior pericardial fluid behind
themid posterior freewall of the left ventricle(LV) (black double arrow in b). The diameter
of apical PE was assessed as the largest
PE extension apical to the left ventricle in
coronal orientation (white double arrow inc). LA, left atrium; RA, right atrium.
TABLE 1. Reliability of Pericardial Diameter Measurements at Distinct Locations
Anterior Posterior Apical Superior Aortic Recess
Intraobserver reliability
Intraclass correlation coefficient 0.80 0.87 0.97 0.92
Bland-Altman (cm) 0.04 � 0.82 �0.08 � 0.79 0.01 � 0.42 0.06 � 0.72
Interobserver reliability
Intraclass correlation coefficient 0.81 0.82 0.95 0.89
Bland-Altman (cm) 0.03 � 0.88 0.12 � 0.99 0.07 � 0.55 0.06 � 0.85
GROTH ET AL Academic Radiology, Vol 19, No 6, June 2012
0.50 and 0.30 weak, and between 0.30 and 0 almost nonexis-
tent. P values <.05 indicated statistical significance.
Diameter and volume measurements were tested for
normality with using the Kolmogorov-Smirnov test for
normal distribution.
For validity testing, a sample size $16 provided >80%
power to detect a correlation >0.60 with an a value of 0.05.
RESULTS
Data Distributions
The Kolmogorov-Smirnov test for normal distribution
accepted normality for all measurements: anterior (P = .21),
posterior (P = .40), apical (P = .11), SAR (P = .94), and
volume measurements (P = .14).
Reliability of Volume Measurements
PE volume measurements showed excellent agreement
between the two observers, with an ICC of 0.99. Bland-
Altman analysis displayed a mean bias of �2.5 mL (95% limits
of agreement, �67.2 mL).
Reliability of Diameter Measurements
ICCs revealed good interobserver agreement for all measure-
ment locations, with the strongest ICC for apical measure-
ments (Table 1). Moreover, Bland-Altman analysis displayed
the smallest limits of interobserver agreement for apical
measurements (Table 1, Fig 2a).
720
Good intraobserver agreement was found for all measure-
ment locations as well (Table 1). However, apical measure-
ments showed the strongest ICC and the smallest limits of
agreement (Table 1, Fig 2b).
Validity of Diameter Measurements
Significant and strong Pearson’s correlation coefficients
between diameter measurements and PE volume were
demonstrated for all measurement locations. Pearson’s corre-
lation coefficients, P values,R2 values, and equations are listed
in Table 2. The strongest Pearson’s correlation coefficient was
found for apical measurements (Fig 3).
Derivation of Equation for PE Volume Estimation
Of the four measured PE diameters, the one with best validity
and reliability was chosen to derive a simplified formula for PE
volume estimation. For this purpose, a linear regression equa-
tion for apical diameter measurements against PE volume
(Table 2) was simplified into the following formula: PE
volume = 0.3 (L/cm) � apical diameter (cm).
DISCUSSION
PE volume can be estimated easily and rapid with the intro-
duced formula. For clinical applications, the estimation of
PE volume can be useful for planning surgical drainage and
pericardiocentesis (18).
In this study, PE diameters were measured at four distinct
locations: SAR, anterior, posterior, and apical.

Figure 2. Bland-Altman plots showing inter-
observer (a) and intraobserver (b) reliability ofapical diameter measurements.
TABLE 2. Correlation (Validity) between Diameter Measurements and Pericardial Effusion Volume Assessed by Volumetry andDerived Linear Equation
Anterior Posterior Apical Superior Aortic Recess
Correlation coefficient 0.83 0.88 0.89 0.83
P <.0001 <.0001 <.0001 <.0001
Coefficient of determination 0.69 0.78 0.80 0.70
Linear equation y = 332x � 132 y = 308x � 35 y = 296x � 32 y = 263x � 287
Figure 3. Plot of pericardial effusion volume against apical diameter
measurements (n = 40 measurements performed by the two
observers). Ninety-five percent confidence intervals (dotted lines)
were fitted to the regression line (solid line).
Academic Radiology, Vol 19, No 6, June 2012 PERICARDIAL EFFUSION VOLUME ASSESSMENT BY CT
Apical PE measurements for the estimation of PE volume
revealed the best validity and reliability. This fact might be
especially useful in daily clinical routine, because the heart
apex is normally displayed in thorax-only as well as
abdomen-only CT examinations. Therefore, the evaluated
formula allows the assessment of PE volume not only if the
whole heart is imaged but even on abdomen-only CTexam-
inations without coverage of the whole heart.
Nevertheless, our study showed that anterior and posterior
as well as diameter measurements obtained at the level of the
SAR showed strong correlation with PE volume as well.
In 1991, D’Cruz and Hoffman (19) evaluated a formula for
estimating the volume of PE by echocardiography. Leibowitz
et al (20) investigated the accuracy of this formula to estimate
PE volume by echocardiography and CT imaging. Although
their study showed a significant correlation between PE
quantification by CT imaging and actual PE volume
(r = 0.40, P = .004), echocardiographic quantification was
more accurate. Because the formula of D’Cruz and Hoffmann
was validated only by echocardiography, Leibowitz et al
considered a CT imaging–derived anatomic formula to be
more accurate. However, the CT imaging–based formula
evaluated in our study shows a stronger correlation with actual
PE volume than the formula of D’Cruz and Hoffmann.
Therefore, our formula seems to be more appropriate for
the estimation of PE volume by CT imaging.
Some limitations of our study must be addressed. First,
PE volume was calculated only by tomographic volumetry,
and no comparison with surgically drained volume was per-
formed, because none of the investigated subjects underwent
surgical PE drainage. Nevertheless, a previous study demon-
strated PE volume calculated by tomographic volumetry to
be almost consistent with volume drained surgically (10).
Moreover, this study showed that aspiration of PE by inserting
a small-gauge tube showed smaller PE volumes, most probably
because complete aspiration of the fluid was not possible (13).
Second, because of the retrospective character of our study,
CTexaminations positive for PE were selected from the daily
clinical program at our institution. Hence, in most cases, PE
was an incidental finding in patients without clinical signs or
symptoms of PE. This might have led to the inclusion of
a larger number of small PEs.
Third, the need for radiation exposure limits the use of CT
imaging for the evaluation of PE. Especially because of the
wide availability of other diagnostic modalities, such as echo-
cardiography, CT imaging should not be used for the first-line
evaluation of PE. Therefore, at our institution, most patients
with symptomatic PE undergo echocardiography rather than
721

GROTH ET AL Academic Radiology, Vol 19, No 6, June 2012
CT imaging for diagnostic evaluation, which might have
influenced the study population as well.
Fourth, the study collective was small and contained just 20
patients with PE. These patients were identified among 915
CT examinations of the thorax, which were retrospectively
reviewed for the presence or absence of PE. To include larger
number of patients, a study carried out prospectively would be
preferable. However, because of the need for radiation expo-
sure, conducting such a prospective study would be
questionable.
However, although echocardiography enables the differen-
tiation of large PE from moderate or small PE, it lacks accu-
racy in quantitating PE volume (21). Another limitation of
echocardiography may be hampered performance due to
the lack of an optimal ultrasound window after chest surgery
(18). Thus, CT imaging for the evaluation of PE might be
indicated in special cases. However, because PE is a common
additional finding in patients undergoing CT imaging
(10,11), a formula for easy and fast assessment of PE is very
helpful in daily clinical routine.
CONCLUSIONS
We recommend a simplified equation for the rapid assessment
of PE volume detected by CT imaging:
PE volume ¼ 0:3ðL=cmÞ � apical diameterðcmÞ:
This formula might be very helpful for clinicians in the
evaluation of hemodynamic relevance and in considering
relief by pericardial paracentesis.
REFERENCES
1. Truong MT, Erasmus JJ, Gladish GW, et al. Anatomy of pericardial
recesses on multidetector CT: implications for oncologic imaging. AJR
Am J Roentgenol 2003; 181:1109–1113.
2. Scherer A, Choy G, Kropil P, et al. Cardiac pathologies incidentally
detected with non-gated chest CT [article in German]. Rofo 2009; 181:
1127–1134.
3. Restrepo CS, Lemos DF, Lemos JA, et al. Imaging findings in cardiac
tamponade with emphasis on CT. Radiographics 2007; 27:1595–1610.
722
4. YaredK, Baggish AL, PicardMH, et al. Multimodality imaging of pericardial
diseases. JACC Cardiovasc Imaging 2010; 3:650–660.
5. Tian L, Liu LZ, Cui CY, et al. CT findings of primary non-teratomatous
germ cell tumors of the mediastinum—a report of 15 cases. Eur J Radiol.
In press.
6. Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the
management of pericardial diseases. Circulation 2010; 121:916–928.
7. Eichler K, Zangos S, Thalhammer A, et al. CT-guided pericardiocenteses:
clinical profile, practice patterns and clinical outcome. Eur J Radiol 2010;
75:28–31.
8. Da Ines D, Chabrot P, Motreff P, et al. Cardiac tamponade after malignant
superior vena cava stenting: two case reports and brief review of the liter-
ature. Acta Radiol 2010; 51:256–259.
9. Spodick DH. Acute cardiac tamponade. N Engl J Med 2003; 349:
684–690.
10. Hall WB, Truitt SG, Scheunemann LP, et al. The prevalence of clinically
relevant incidental findings on chest computed tomographic angiograms
ordered to diagnose pulmonary embolism. Arch Intern Med 2009; 169:
1961–1965.
11. Lee EY, Kritsaneepaiboon S, Zurakowski D, et al. Beyond the pulmonary
arteries: alternative diagnoses in children with MDCT pulmonary
angiography negative for pulmonary embolism. AJR Am J Roentgenol
2009; 193:888–894.
12. Groth M, Henes FO, Mayer U, et al. Age-related incidence of pulmonary
embolism and additional pathologic findings detected by computed
tomography pulmonary angiography. Eur J Radiol. In press.
13. Tomoda H, Hoshiai M, Furuya H, et al. Evaluation of pericardial effusion
with computed tomography. Am Heart J 1980; 99:701–706.
14. Busing KA, Kilian AK, Schaible T, et al. Reliability and validity of MR image
lung volumemeasurement in fetuses with congenital diaphragmatic hernia
and in vitro lung models. Radiology 2008; 246:553–561.
15. Bland JM, Altman DG. Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet 1986; 1:307–310.
16. Costa-Santos C, Bernardes J, Ayres-de-Campos D, et al. The limits
of agreement and the intraclass correlation coefficient may be
inconsistent in the interpretation of agreement. J Clin Epidemiol 2011;
64:264–269.
17. Groth M, Henes FO, Bannas P, et al. Intraindividual comparison
of contrast-enhanced MRI and unenhanced SSFP sequences of
stenotic and non-stenotic pulmonary artery diameters. Rofo 2011; 183:
47–53.
18. Tsang TS, Barnes ME, Hayes SN, et al. Clinical and echocardiographic
characteristics of significant pericardial effusions following cardiothoracic
surgery and outcomes of echo-guided pericardiocentesis for manage-
ment: Mayo Clinic experience 1979-1998. Chest 1999; 116:322–331.
19. D’Cruz IA, Hoffman PK. A new cross sectional echocardiographic method
for estimating the volume of large pericardial effusions. Br Heart J 1991;
66:448–451.
20. Leibowitz D, Perlman G, Planer D, et al. Quantification of pericardial
effusions by echocardiography and computed tomography. Am J Cardiol
2011; 107:331–335.
21. Prakash R, Moorthy K, Del Vicario M, et al. Reliability of echocardiography
in quantitating pericardial effusion: a prospective study. J Clin Ultrasound
1977; 5:398–402.