Embed Size (px)
Citation preview
A Modified Technique for Removing Earlobe Keloids
Earlobe keloids are frustrating to patients and
surgeons for their aesthetic deformity. The purpose
of surgery is to remove the fibrous core of the
keloid and to cover the defect, restoring the normal
contour of the ear. There have been numerous
methods described to achieve this, including
healing by secondary intention, direct closure, skin
grafts, and local flaps.
Many different types of local flaps of varying com-
plexity have been described for different situations.
Lee et al.1 and Kim et al.2 proposed an interesting
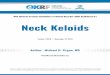
and effective design in which the skin over the
keloid was dissected from the keloid core and pre-
served as a flap to cover the defect. Based on the
principles of this technique, we describe a modifi-
cation that allows for accurate preoperative mea-
surement and planning, allowing for safe and
simple elevation and insetting of the flap during
the procedure (Figure 1).
Preoperative Measurements and Marking
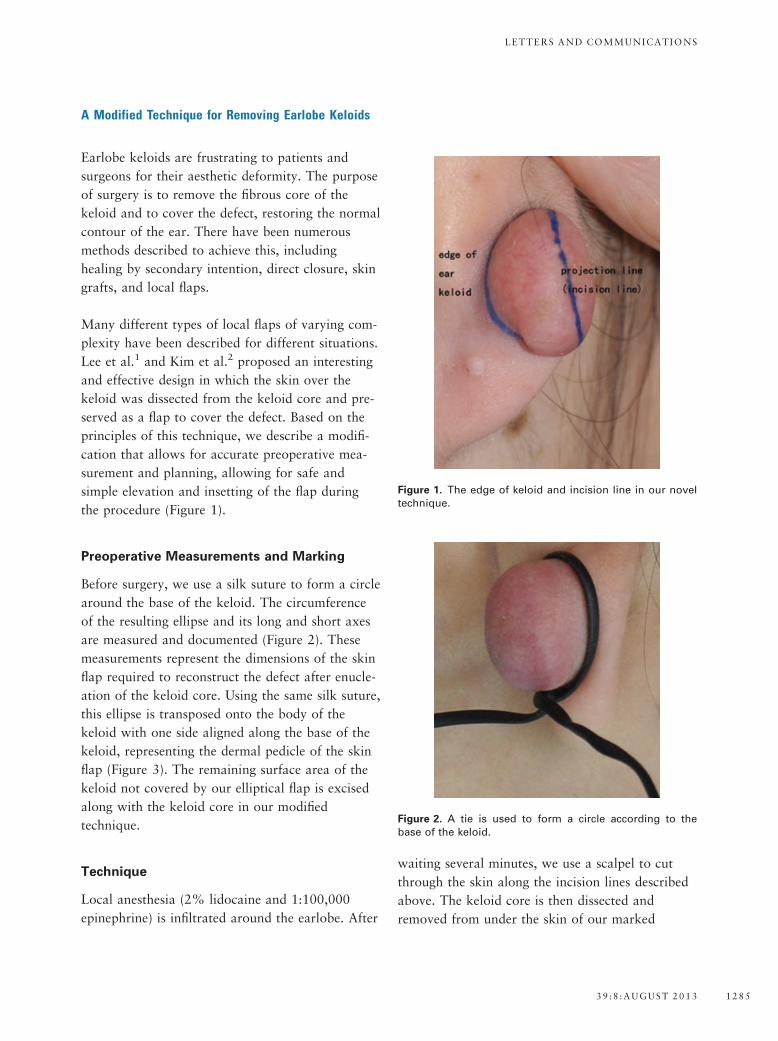
Before surgery, we use a silk suture to form a circle
around the base of the keloid. The circumference
of the resulting ellipse and its long and short axes
are measured and documented (Figure 2). These
measurements represent the dimensions of the skin
flap required to reconstruct the defect after enucle-
ation of the keloid core. Using the same silk suture,
this ellipse is transposed onto the body of the
keloid with one side aligned along the base of the
keloid, representing the dermal pedicle of the skin
flap (Figure 3). The remaining surface area of the
keloid not covered by our elliptical flap is excised
along with the keloid core in our modified
technique.
Technique
Local anesthesia (2% lidocaine and 1:100,000
epinephrine) is infiltrated around the earlobe. After
waiting several minutes, we use a scalpel to cut
through the skin along the incision lines described
above. The keloid core is then dissected and
removed from under the skin of our marked
Figure 1. The edge of keloid and incision line in our noveltechnique.
Figure 2. A tie is used to form a circle according to thebase of the keloid.
LETTERS AND COMMUNICATIONS
39 :8 :AUGUST 2013 1285
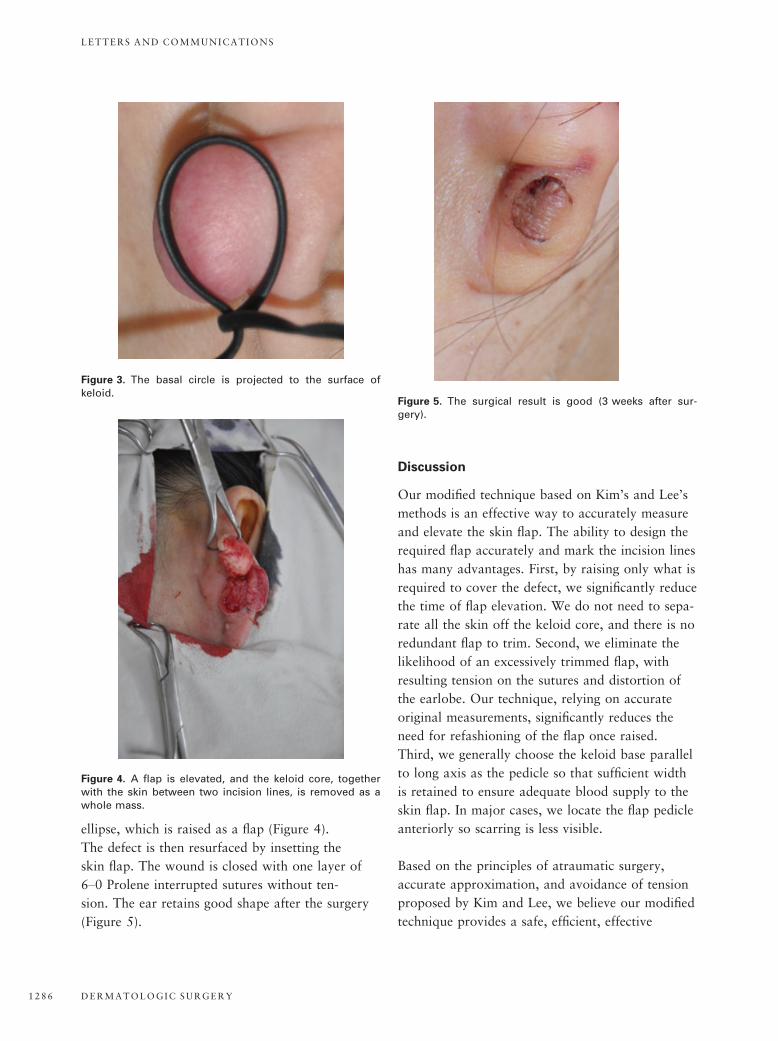
ellipse, which is raised as a flap (Figure 4).
The defect is then resurfaced by insetting the
skin flap. The wound is closed with one layer of
6–0 Prolene interrupted sutures without ten-
sion. The ear retains good shape after the surgery
(Figure 5).
Discussion
Our modified technique based on Kim’s and Lee’s
methods is an effective way to accurately measure
and elevate the skin flap. The ability to design the
required flap accurately and mark the incision lines
has many advantages. First, by raising only what is
required to cover the defect, we significantly reduce
the time of flap elevation. We do not need to sepa-
rate all the skin off the keloid core, and there is no
redundant flap to trim. Second, we eliminate the
likelihood of an excessively trimmed flap, with
resulting tension on the sutures and distortion of
the earlobe. Our technique, relying on accurate
original measurements, significantly reduces the
need for refashioning of the flap once raised.
Third, we generally choose the keloid base parallel
to long axis as the pedicle so that sufficient width
is retained to ensure adequate blood supply to the
skin flap. In major cases, we locate the flap pedicle
anteriorly so scarring is less visible.
Based on the principles of atraumatic surgery,
accurate approximation, and avoidance of tension
proposed by Kim and Lee, we believe our modified
technique provides a safe, efficient, effective
Figure 3. The basal circle is projected to the surface ofkeloid.
Figure 4. A flap is elevated, and the keloid core, togetherwith the skin between two incision lines, is removed as awhole mass.
Figure 5. The surgical result is good (3 weeks after sur-gery).
LETTERS AND COMMUNICATIONS
DERMATOLOGIC SURGERY1286

method to reconstruct the earlobe after keloid
removal.
Acknowledgments The authors thank Hua L,
Ying H (Department of Plastic and Reconstructive
Surgery, Sir Run Run Shaw Hospital, Medical
College, Zhejiang University) and Frank Lin (Royal
Melbourne Hospital, Australia) for their excellent
assistance in this work.
References
1. Lee Y, Minn K, Baek R, Hong JJ, et al. A new surgical treatment
of keloid: keloid core excision. Ann Plast Surg 2001;46:135–40.
2. Kim D, Kim E, Eo S, Kim K, et al. A surgical approach for
earlobe keloid: keloid fillet flap. Plast Reconstr Surg
2004;113:1668–74.
YAN SHAO, PHD
XING HE, PHD
Department of Plastic and Reconstructive Surgery
Sir Run Run Shaw Hospital
Medical College
Zhejiang University
Hangzhou, China
Regarding Assisting Pincer Nail Deformity by Haneke's Procedure
We read with interest the article “Pincer Nails:
Definition and Surgical Treatment” by Baran
and colleagues1 that encompassed a variety of
surgical “tricks” to assist the correction of
pincer nail deformity. They mentioned Haneke’s
technique followed by a median incision of the
nail bed from the border of the lunula to 2 mm
beyond the hyponychium and extending down to
the bone. During this incision, the traction
osteophyte was felt with the scalpel, although it
was not obvious on the roentgenogram. The
pinched nail bed was dissected from the
terminal phalanx, the distal dorsal tuft with
the osteophyte was rongeured off, and the nail
bed was expanded and sutured using 6–0
monofilament absorbable sutures. Reverse tie-over
sutures were placed in the lateral nail folds, with
small rubber tubes used as cushions to prevent
the sutures from cutting through the nail folds.
These sutures kept the nail bed stretched over
the bone and were removed after approximately
3 weeks.
We have five important suggestions that could
further refine this procedure. First, fungal nail
infection should be treated and then excluded by
negative results on microscopic examination
(KOH test) and fungal culture before reconstruc-
tion. Second, after exsanguination of the toe, the
deformed nail plate should be removed using the
rolling method, preventing unnecessary trauma to
the nail bed and matrix. Third, after the nail bed
is exposed, the surrounding fibrous tissues can be
excised using scissors to obtain a regular nail bed
for smooth growth of the new nail (Figure 1A).
Fourth, surface irregularities such as traction
osteophytes and the periosteum are more easily
removed using a bone burr or rasp than using a
bone rongeur (Figure 1B). Fifth, the original nail
could also be trimmed thin using the bone burr or
rasp for final coverage of the nail bed
(Figure 1C).
We examined the cases of four patients who
underwent treatment on five great toes using
Haneke’s procedure. Satisfactory results were
obtained using this simple, effective, nail matrix–
sparing technique without any complications
(Figure 1D). In conclusion, we believe that by
adopting the abovementioned steps for further
refining this technique, Haneke’s procedure can
be easily performed with low morbidity and can
be a good option for treatment of pincer nail
deformity.
LETTERS AND COMMUNICATIONS
39 :8 :AUGUST 2013 1287