Embed Size (px)
Citation preview

8Brntish Journal ofOphthalmology 1994; 78: 568-571
A case of corneal keloid: clinical, surgical,pathological, and ultrastructural characteristics
Jose Miguel Risco, Antonio Huaman, Sobhi R Antonios
AbstractA 69-year-old patient developed a localised,whitish, elevated, corneal lesion with a smoothand glistening surface following trauma, with-out evidence of corneal perforation. Twelvemonths later, the lesion showed evidence ofslow growth. An excisional biopsy was thenperformed. Histopathologically, the lesionwas covered by non-keratinised squamousepithelium and was comprised of randomlyoriented collagen fibres containing activefibroblasts. Blood vessels were noted deep inthe lesion. Ultrastructurally, the cell popula-tion was formed by fibroblasts and myofibro-blasts, similar to keloids of the skin. Theclinical, pathological, and ultrastructuralfeatures of the corneal lesion are compatiblewith a corneal keloid.(BrJ7 Ophthalmol 1994; 78: 568-571)
Corneal keloids are rare lesions that can developin cases of corneal insult. 1-13 They can be presentat any age and can appear as a single, solitarynodule or involve the entire corneal stroma.Keloids in general represent forms of hyper-trophic scars produced by prolonged and exces-sive deposition of collagen and extend beyondthe confines of the original trauma. 14 15
Reported cases of corneal keloid are not com-mon in the literature.1''3 Only one case wasreported in a series of 302 cases of epibulbartumours in children.'6 We report a case of anadult patient who developed a well localisedcorneal keloid following trauma. We initiallyexamined the patient 5 months after the trauma,and observed the progression of the lesion over a12-month period.
Case reportA 69-year-old patient
King Khaled EyeSpecialist Hospital,Riyadh, Saudi ArabiaJ M RiscoA HuamanS R AntoniosCorrespondence to:J Miguel Risco, MD, c/oMedical Library, King KhaledEye Specialist Hospital,PO Box 7191, Riyadh 11462,Saudi Arabia.Accepted for publication8 February 1994
was referred to King
;. ff M
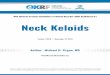
Figure I Appearance ofthe corneal keloid at the time ofinitial evaluation.
Khaled Eye Specialist Hospital and presentedfor the first time in February 1989 with a 5 monthhistory ofprogressive, painless decrease in visionof his left eye following trauma with a fingernail.Details of the condition of the eye before thetrauma as well as the extent and treatment of theinitial injury were not available. After the initialinjury, the patient noticed progressive 'opacifica-tion' of his left cornea. His ocular and medicalhistory was non-contributory. There was nohistory of exuberant scar formation. Eye exami-nation revealed a visual acuity of 20/200 in theright eye and hand motion in the left eye.Intraocular tensions were within normal limits.Scarring of the upper tarsal conjunctivae andsuperior limbic micropannus with Herbert's pitsindicated old inactive trachoma in both eyes.Mild climatic droplet keratopathy and an
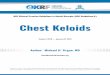
immature cataract accounted for the decreasedvision in his right eye. Slit-lamp examination ofthe left cornea (Fig 1) revealed a whitish,smooth, glistening, and localised lesion, measur-ing approximately 9 mm in diameter, anterior toBowman's layer. The remaining structures of thecornea were clear and the anterior chamberappeared to be of normal depth. Examinationof the lens following mydriasis showed earlycataractous changes. The rest of the examinationwas unremarkable. The patient was lost to followup until January 1990 when it was noticed thatthe lesion on his left eye covered a larger area ofthe cornea (Fig 2). Shortly afterwards, the lesionwas entirely removed by superficial keratectomyand was found to be easily dissected from theremaining corneal stroma (Fig 3). No evidence ofa previous corneal perforation was noted, but thecornea was found to have superficial scarring.The postoperative course was unremarkableexcept for the cornea remaining mildly oedema-tous for about 6 months after surgery, withoutevidence of recurrence of a similar corneallesion.
Figure 2 Aspect ofthe lesion 12 months after the initialexamination. The lesion covers a larger area ofthe cornealsurface.
568
on Septem
ber 11, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.7.568 on 1 July 1994. Dow
nloaded from

A case ofcorneal keloid: clinical, surgical, pathological, and ultrastructural characteristics
Material and methodsThe surgical specimen was a circular, denselyopaque piece of firm tissue measuring approxi-mately 8 mm in diameter and up to 2-5 mm inthickness at the centre. It was initially fixed inneutral buffered formalin. The specimen wasthen bisected, and one half was processed forparaffin embedding, sectioned, and examined bylight microscopy. The other half of the specimenwas postfixed in 1% osmium tetroxide for 2hours, and processed for electron microscopy.
Results
PATHOLOGICAL EXAMINATION
Light microscopyExamination of the paraffin sections and thickplastic sections revealed fibrous tissue coveredby non-keratinised squamous epithelium (Fig4). Bowman's layer was absent, and both stromaand epithelium were oedematous. The lesion wascomposed of active fibroblasts and looselyarranged collagen. The basal part of the excisedtissue stroma stained metachromatically withcrystal violet. This basal, amyloid-like deposit
TO:. CA."
.a.
es
.s~~~~~~~~~~~~~~~~~~~~~~~~.
z?o: .;e t
varied in thickness, but appeared in mostinstances as a continuous strip of about 3 urm inthickness. The fibroblasts had moderatelyhyperchromatic, spindle-shaped nuclei, withoccasional multinucleation, without loss of theirbenign character (Fig 5). Their cytoplasm wasfibrillar and darkly acidophilic. Blood vessels ofvarying calibre coursed irregularly in the deepstroma. Sporadic spheroidal deposits consistentwith climatic droplet degeneration (CDK) andincreased elastic fibres were present along theposterior surface of the specimen. Congo redstains were negative.
Electron microscopyThe epithelium showed five to six layers of cells.The epithelium was separated from the under-lying stroma by a basement membrane thatexhibited frequent discontinuities.The stroma was formed by collagen and by
the cellular component, mostly fibroblasts. Thecollagen fibrils of the anterior half revealedample interstitial spaces among them. Thecollagen fibrils of the posterior half of the stromawere relatively loose and randomly oriented (Fig6). The collagen fibrils measured about 24 nm indiameter and revealed a distinct periodicity of500 nm. Amyloid-like deposits were seen in theform of more or less continuous ribbons ofvarying thickness demarcating the posterioredge of the keloid stroma. The fibrillary materialof the amyloid-like deposits comprised anintricate meshwork of delicate filaments measur-ing about 10 nm.The fibroblasts were oval or, more commonly,
slightly elongated. Characteristic featuresof most fibroblasts were fibrillar cytoplasm,well developed rough surfaced endoplasmicreticulum, numerous mitochondria, and one,sometimes two, prominent nucleoli (Fig 7). Inmany fibroblasts, the rough surfaced endo-plasmic reticulum was markedly dilated andcontained homogeneous, medium densitymaterial, occasionally intermingled withelectron dense bodies or granules. Intracellularcollagen was detected also in some fibroblasts inwhich microfibrils were situated within mem-brane bound tubular structures in the cyto-plasm. Fibroblasts with dilated rough surfacedendoplasmic reticulum and glycogen storagewere detected mostly in the anterior half of thestroma. Frequently seen were myofibroblasts(Fig 8) that incorporated subplasmalemmaltracts of filaments-less than 4 nm in diameter andparallel to the long axis of the cell, with focaldensities along their length. Moderate numbersof macrophage-like cells and few lymphocyteswere also seen in the stroma.
DiscussionThe term keloid has classically been used in thedermatologic literature to describe bulky scars atthe site of injury.'7 They are indistinguishablefrom hypertrophic scar by histological examina-tion but clinically hypertrophic scars flattenspontaneously in the course of one to severalyears, while keloids persist and may even extendbeyond the site of injury. 4
Figure 3 The cornealkeloid at the time ofsurgicalremoval by a superficialkeratectomy.
Figure 4 Light micrographofthe keloid. A non-keratinised squamousepithelium covers thefibrousstroma (x 60).
'MQwRR
569
.'nMM *7
Amp.
on Septem
ber 11, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.7.568 on 1 July 1994. Dow
nloaded from

Risco, Huaman, Antonios
FigureS High power light micrograph shows the nature ofthefibroblasts and their benigappearance (x 60).
Figure 6 Electron micrograph ofthe collagenfibrils on the lesion. Thesefibrils are randooriented (magnification, x 18 000)
Figure 7 Electron micrograph ofan activefibroblast with two nucleoli. The rough surfacendoplasmic reticulum (E) is markedly dilated (magnification, x5400).
The term 'corneal keloid' has been usedpreviously in a wide range of clinical situationsand has been introduced in a few isolated case
v reports.''3 These reports include cases in whicha corneal fibrous lesion develops after trauma,29is present at birth,' 356 2 in adult life' aftercorneal perforation,5 following rubella kerato-pathy with perforation,4 following smallpox,' inassociation with other developmental anoma-lies,'2 in Lowe's syndrome,'" or as a result of anon-specific insult.' In most of these cases, thediagnoses were established after histopatho-logical examination of enucleated globes2'5"'and in specimens ofpenetrating keratoplasty.9"
In contrast with our patient's lesion, post-traumatic corneal scars are not elevated lesions.Clinically, corneal keloids are described aswhitish, fairly localised and poorly vascularisedlesions, with a smooth and glistening surface."On several occasions they have been associated
gn with corneal perforation,24 and it has beensuggested that keloids may originate from iristissue. O'Grady,5 however, in a report offour cases, denies that iris incarceration is an
,;% important constituent in the formation ofkeloids.Corneal keloids have been described in all age
< groups, from a congenital form,3' 12 to thoseoccurring in late adulthood.'9 Smith' in 1940collected data on 37 previously reported cases.Of these, 13 patients were less than 10 years ofage at the time of presentation, and 27 of the 37patients had a history of disease, injury, orsurgery preceding the appearance of the cornealgrowth. Most of these corneal keloids were
. thought to have risen in staphylomatous corneas.v<8 Some of the congenital cases'-3 may represent
--i* staphylomatous corneas secondary to a previouskeratopathy or possibly congenital glaucoma,"and probably do not represent a true corneal
?7 keloid, but end stage postinflammatory healingwith excessive scar formation.2 Spencer'8 even
. doubts true keloids occur in the cornea.;bhe It is pertinent that corneal keloid in children
be differentiated from well defined conditionssuch as sclerocornea, corneal dermoid, Peter'sanomaly, congenital hereditary endothelialdystrophy, congenital glaucoma, birth trauma,infections, and metabolic disease.'2 In adults, thepresence of a white, elevated, and localised lesionwith a smooth and glistening surface thatdevelops following trauma appears to be almostpathognomonic for a corneal keloid. In contrast,Salzmann's nodular degeneration occurs as areactive process to a chronic keratitits of longduration. The nodular lesions in the cornealsurface are small and tend to be multiple.Histopathologically the nodules reveal excessivesecretions of basement-like material withcollagen hyalinisation.Our case differs from most cases previously
reported and in our view, characterises thev corneal keloid clinically, histopathologically,
and surgically: historically, there is a well estab-3jii lished traumatic event, there is a progressive;;;2 growth of a white raised corneal opacity, there is,,*- a lesion populated by active fibroblasts and
myofibroblasts,'9 and a lesion completelyed resected with preservation of the corneal stroma.
The presence of CDK and amyloid at the
570
:. Am..M
....t:.w
-:.;.: flfl
-AdEOL-AF7
w 4'. ::,..
.. A!
.i,
.f.-:-
11 1"i': 1'. ;,F"
..'MWMPW-
wi.. .:A-,---,--,:
A
on Septem
ber 11, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.78.7.568 on 1 July 1994. Dow
nloaded from

A case ofcorneal keloid: clinical, surgical, pathological, and ultrastructural characteristics
Figure 8 Electron micrograph ofa myofibroblast showing characteristic subplasmalemmaltract ofmicrofilaments with focal densities (arrowheads) (magnification, x4800).
interface are interpreted as pre-existing climaticmanifestations.202'
The significance of myofibroblasts in woundhealing has been elucidated22: the myofibroblastactually represent a transformed fibroblastnormally present in granulation tissue, thattemporarily expresses smooth muscle phenotype(myofibrils, microtendons). It produces softcollagen type III and in time yields to conven-tional fibroblasts, producers of collagen type Ithat harden and retract the scar. In keloidsand other forms of abnormal healing such as
vitreoretinopathies,23 24 anterior subcapsularcataracts,25 or nodular fasciitis, myofibroblastspersist longer than necessary and often dominatethe cell population of the lesion. Eventuallykeloids collagenise slowly in the centre but donot retract. In our patient this abnormal, delayedhealing process manifested itself by the bulky
slow growth, the active fibroblasts and myofibro-blasts, and the absence of harder collagen.
1 Smith HC. Keloid of the cornea. Trans Am Ophthalmol Soc1940; 38: 519-38.
2 Fenton RH, Tridici TJ. Hypertrophic corneal scars (keloids).Surv Ophthalmol 1964; 9: 561-6.
3 Farkas TG, Znaida JP. Keloid of the cornea. Amj Ophthalmol1968; 66: 319-23.
4 Frederique G, Howard R, Boniuk V. Corneal ulcers in rubella.Amj Ophthalmol 1969; 68: 996-1003.
5 O'Grady RB, Kirk HQ. Corneal keloids. Am J Ophthalmol1972; 73:206-13.
6 Brown SL. Corneal transplantation of the infant cornea. TransAmAcad Ophthalmol Otolaryngol 1974; 78: OP461-6.
7 Shukla IM, Arora NP, Arora MM. Corneal keloid. Ind JOphthalmol 1975; 23: 18-9.
8 Cotlier E. Discussion. In: Bergsma D, Bron AJ, Cotlier E, eds.The eye and inborn errors ofmetabolism. Birth defects. 1976;12: 594.
9 Pouliquen Y, Dehrmy P, Chauvad M. Une lesion corneenebien particuliere; pannus hypertrophique. Bull SocOphtalmol Fr 1979; 79: 501-2.
10 Cibis GW, Tripathi RC, Tripathi BJ, Harris DJ. Cornealkeloid in Lowe's syndrome. Arch Ophthalmol 1982; 100:1795-9.
11 Lahav M, Cadet JC, Chirambo M, Rehani U, Ishii Y. Cornealkeloids - a histopathologic study. Graefes Arch Clin ExpOphthalmol 1982; 218: 256-61.
12 Weiner MJ, Albert DM. Congenital corneal keloid. ActaOphthalmol 1989; 192 (suppl): 188-%.
13 Holbach LM, Font RL, Shivitz IA, Jones DB. Bilateralkeloid-like myofibroblastic proliferation of the corneas inchildren. Ophthalmology 1990; 97: 1188-93.
14 Lever WF, Schaumburg-Lever G, eds. Tumors of fibroustissue. In: Histopathology of the skin. 6th ed. Philadelphia:JB Lippincott, 1984: 604-5.
15 Linares HA, Kischer CW, Dobrkovskym M, Larson DL. Thehistiotypic organization of the hypertrophic scar in humans.JIInvestDerin 1972; 59: 323-31.
16 Elsas FJ, Green WR. Epibulbar tumors in childhood. AmJOphthalmol 1975; 79: 1001-7.
17 Murray JC, Pollack SV, Pinell SR. Keloids: review. Am JAcad Derm 1981; 4: 461-70.
18 Spencer WH. Ophthalmic pathology. An atlas and textbook.Philadelphia: Saunders, 1985; 3: 289-92.
19 James WD, Besanceney CD, Odom RB. The ultrastructure ofa keloid.j AmAcad Derm 1980; 3: 50-7.
20 Hidayat AA, Risco JM. Amyloidosis of corneal stroma inpatients with trachoma. Ophthalmology 1989; 96: 1203-11.
21 Matta CS, Tabbara KF, Cameron JA, Hidayat AA, al-RajhiAA. Climatic droplet keratopathy with corneal amyloidosis.Ophthalmology 1991; 98: 192-5.
22 Schurch W, Seemayer TA, Gabbiani G. The myofibroblast.In: Stemnberg SS, ed. Histology for pathologists. 1st ed.Chapter 5. New York: Raven Press, 1992: 109-44.
23 Machemer R, van Horn D, Aaberg TM. Pigment epithelialproliferation in human retinal detachment with massiveperiretinal proliferation. AmJ Ophthalmol 1978; 85: 181-91.
24 Kampik A, Kenyon KR, Michels RG, Green WR, de la CruzZC. Epiretinal and vitreous membranes: comparative studyof 56 cases. Arch Ophthalmol 1981; 99: 1445-54.
25 Novotny GE, Pau H. Myofibroblast-like cells in humananterior capsular cataracts. Virchows Arch (A) 1984; 404:393-401.
571 on S
eptember 11, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.7.568 on 1 July 1994. D
ownloaded from