Embed Size (px)
Citation preview
A menu to providequality communityplacementsNeil Smith, Division of Primary Care, University of Manchester, UK
THE RELEVANCE OF THISMENU
Community placements are atopical growth area inmedical education.1 As stu-
dents encounter ever more spec-ialised hospital firms and fewerhospital patients, community-based medical education offersstudents the opportunity to see awide range of problems that aresupported increasingly bythe community rather than bysecondary care. Medical schoolshave responded to General MedicalCouncil (GMC) recommendations2
to move more undergraduateeducation into the community.Strategies of expansion need to beevidence-based and involve thestudent perspective.
In the United Kingdom thereis an ongoing increase in thenumber of medical students.Medical schools are exploringinnovative ways of raising thestandards of community place-ments, and departments of com-munity-based medical educationhave to decide where and how toplace resources.3
In many parts of the UK thereare not enough doctors for thenumber of patients. An antici-pated mass retirement of an age-ing general practitioner (GP)population increases the need torecruit and retain more GPs.4 Onesolution would be for localities to‘grow their own’ from among theavailable medical students.5 Thisinvolves offering the medicalstudents a quality placement, and
a positive experience of generalpractice. Improving the quality ofundergraduate placements couldlead to a long-term increase inthe recruitment and retention ofGPs.
With the expansion in post-graduate training, particularly inthe foundation years, there ispotential competition for GPinvolvement. However, GP prac-tices are in danger of retreatingfrom providing undergraduateplacements, as the new GP con-tract has increased the clinicaland administrative burden onpractices. There is therefore apressing and timely need toincrease both the quality andquantity of general practiceundergraduate placements.A simple framework to clarify
In many parts ofthe UK there are
not enoughdoctors for the
number ofpatients
Community-basedmedicaleducation
176 � Blackwell Publishing Ltd 2008. THE CLINICAL TEACHER 2008; 5: 176–180

what is needed would help toaddress these issues.
THE ORIGINS OF THE MENU
My original aim was to identify,describe and prioritise the factorsthat, from a medical student’sperspective, improve the qualityof community placements. I de-signed a qualitative approachusing three methods: focusgroups; face-to-face, and semi-structured interviews; and a lit-erature review.6
The participants were 32medical students in their finalyear at Manchester MedicalSchool. At the time they were allat the end of a 5th-year com-munity placement in East Lanca-shire, an under-priveleged areawith a shortage of doctors. Allthe students had experienced atleast four different communityplacements, most of which werein general practice and in theNorth West region, but not inEast Lancashire.
I asked for volunteers fromtwo problem-based learninggroups, each including eight stu-dents, to participate in two focusgroups. I then invited two moreproblem-based learning groups of
eight students to participate inthe interviews. I stressed in boththe written material and withverbal reassurances that they wereunder no obligation to partici-pate. I emphasised that refusal tobe involved, or anything theydivulged during the interview,would not jeopardise their successat medical school or their futurecareer. All 32 students agreed toparticipate.
I planned the facilitation of thefocus groups in advance, toencourage participants to discusstheir experiences in relation to thefactors that had affected thequality of their community place-ments. Initially, I simply eaves-dropped on their conversations,but then moved on to prompting,probing and summarising, andfinally adopted a more interven-tionist style. This resulted in arange of views, differences ofopinions, a deeper interpretation,and hence a better understandingof the students’ views.
Themes that emerged from thefocus group helped to inform andprepare for the interviews. Thecore question was to ask eachstudent to identify the factorsthat, in their experience, affectedthe quality of community place-
ments, then to describe eachfactor in more detail, and finallyto attempt to prioritise thesefactors in order of importance tothem. I used a clear, open-endedand non-directive interview style.Continuous scrutiny of ongoinginterviews allowed me to testemerging theories and involvedeviant case analysis.
The focus groups andinterviews were tape-recorded,fully independently transcribed,with each student labelled foranonymity, and checked by me foraccuracy. I made field notes ofreflected observation in myresearch diary. ‘ATLAS-ti’ softwarewas used to code text. Hence thedata collection and analysisproceeded in an iterative manner,in accordance with groundedtheory.7
I deliberately left the litera-ture review until last in anattempt not to bias the emergingresults from the students’ view-point. I performed an onlinemedical literature review using all‘aditus’ databases (http://www.aditus.nhs.uk) over a10-year time-frame. I searched ondifferent combinations of two ormore of the terms ‘medical stu-dents’, ‘community placements’,‘general practice’ and ‘quality’.
The factors identified anddescribed were prioritised byconsensus group ranking amongthe focus groups, and individualexpressions of importance by theinterviewees. The literaturereview reinforced the validity ofthese priorities, based on thebreadth and depth of the litera-ture that explored or justifiedthese quality factors.
A total of 26 separate factorsthat affected the quality ofcommunity placements wereidentified and described. Duringthe first focus group, one studentsuggested that what I wastrying to achieve was a ‘menu’ ofquality factors. This concept
Figure 1. Enthusiastic GP tutors in East Lancashire.
A total of 26separate factorsthat affectedthe quality ofcommunityplacementswere identifiedand described
� Blackwell Publishing Ltd 2008. THE CLINICAL TEACHER 2008; 5: 176–180 177
evolved during the second focusgroup, with the idea that thepriority factors are the maincourse. Throughout the inter-views, each student reflected andrefined this concept, leading tofurther development of the ‘menu’notion. Another studentsuggested that the less importantfactors could be classified asbeing ‘starters’ and ‘desserts’ – or,as one student put it very aptly,‘the icing on the cake’. This idearemained with me while perform-ing the literature review. Whatdeveloped was a strong concep-tual link between the gathereddata and a menu of factors ofvarying preference.
PREPARING THEINGREDIENTS OF THE MENU
Starter (set up)Medical schools need to providequality control of communityplacements by visiting practicesand ensuring that robust channelsof communication exist. It ispossible that specialised univer-sity-linked practices taking sev-eral students at a time may offera better student experience.3
When timetabling modules,Universities need to recognise thetimes when GPs are under pressure(for example, Monday mornings).Tutors need to offer definedyet flexible student timetablesto help fulfil learning needs.Students prefer to be in commu-nity placements close to mainhospital sites, and appreciateaccess to IT resources. It isinteresting to note that thiscohort rarely mentioned, and didnot prioritise, either their ownmotivation or patient issues asfactors influencing the quality oftheir placements.
Main course (priority factors)
EnthusiasmThere was universal agreementthat the cornerstone of a healthycommunity placement was a largeportion of GP tutors’ enthusiasm.GP tutors are positive role models
for students to aspire toemulate.8–10 The ingredientsmaking an enthusiastic tutorinclude: motivation; friendliness;approachability; interest in thestudents; patience; insight;experience; and being respectedand caring. However, tutors needadequate support to avoid beingoverstretched and burning them-selves out.
Teaching surgeriesThe view of the interviewedstudents, echoed in the literaturewas ‘participating’, ‘doing’, ‘handson’ and ‘active involvement’, all ofwhich kept the placementfresh.8,9,11 A quality communityexperience involves setting upteaching surgeries to incorporateand invest tutor time in stu-dents.3,12
FeedbackThe students wanted to spice upthe placement with constant,immediate, ongoing, informal,supportive, face-to-face, two-wayfeedback. Some students found itchallenging to give constructivefeedback to their tutors, butfeedback is a key factor to effec-tive learning11 and has beenshown to improve performanceand change practice.10 It is animportant attribute of a goodteacher.8,10 GPs may in fact bebetter than hospital consultantsat providing feedback on clinicalskills.8 Feedback should beconstructive, be provided in asafe atmosphere, and includepositive as well as negativeaspects.11
Learning environmentThere is a recipe for a positivelearning environment: qualitypractices have a group philosophyof proactive investment in learn-ing, where ‘everyone is willing tohelp you’. There is a need toinvest in the seasonal resources ofbooks, journals, IT, video record-ers and appropriate teachingequipment.13 Students havecommented that the main bene-fits of IT provision in the practice
are as a tool for communicationand a learning resource.14
Matching learning needs withopportunitiesStudents need to find ways oftaking responsibility for their ownlearning, and defining learningobjectives. A good tutor wasconsidered by the students to beone that helped to do this byexploring gaps in students’knowledge, then empowering andchallenging them to fill thesegaps by offering a flexible bal-anced diet of resources and clin-ical options.8,10
SpaceA student consultation roomallows students to see patients,consider what is wrong and whatshould be done, prepare, rehearseand present their findings.15
Space constraints have beenwidely reported as an obstacle toquality community placements,and a need for revenue costs forteaching accommodation hasbeen identified.3,12–14,16
Developing skills and attitudeA valuable placement is one inwhich students can broaden theirpalate and develop new tastes.The skills they cultivate involvecommunication, problem-solvingand patient management. Stu-dents perceive that developingtheir attitude is the major andmost attainable benefit of theircommunity experience.8 However,the students in this study wereuncomplimentary about GP tutors’ability to teach examinationskills. The reason for this wasgiven as GPs employing short-cutswhen examining patients, andthen being unable to explain howor why they did this.
Being part of a practice teamFeeling welcome, an inductionprocess and early acquaintanceswere vital to a quality experi-ence.8,12,17 The students enjoyedpractices where the staff and envi-ronment were ‘inclusive’ and‘involving’. Students wanted to be
The cornerstoneof a healthycommunity
placement was alarge portion of
GP tutors’enthusiasm
178 � Blackwell Publishing Ltd 2008. THE CLINICAL TEACHER 2008; 5: 176–180
‘valued’, ‘noticed’ and ‘respected’.They appreciated the blend of con-sultation styles that a practice witha mixture of tutors could offer.
Tutor trainingStudents respected tutors whomthey perceived to be bothcompetent and open to profes-sional development. This wasparticularly so if the tutor at-tended specialised training thatwas helpful to the student. GPtutors are more likely to under-take training than their districtgeneral hospital or teaching hos-pital counterparts.15
Dessert (icing on the cake)Students appreciated beinginvolved in tasks to organisepatient care, such as arranginghospital referrals or admissions.Accommodation and transportwere factors, but came low on thelist of priorities (which contra-dicts my personal experience oflistening to student complaints).Opportunities to meet other stu-dents for group teaching, jointhospital and community place-ments, and attendance at othercommunity clinics (for example,family planning) offered added
value. There was a recommenda-tion to improve problem-basedlearning by reflecting on thereal cases and experiences thestudents were witnessing.Students respected tutors whowere involved in academicactivities and held universityposts.
CHEF’S RECOMMENDATIONS
There are clearly limitations inthis small study, localised to onegeographical area and involvingparticipants potentially wantingto please the researcher. However,an attempt to improve the qualityof community placements is bothtopical and worthwhile, as theseimportant findings may be trans-ferable to other community loca-tions. As a portfolio GP with acareer spanning both educationand primary care trust leadership,I have been keen to offer practicaladvice to individuals and organi-sations involved in undergraduateeducation. During the focusgroups and interviews, I exploredwith the students what recom-mendations should be made tothese individuals and organisa-tions. I have evaluated the results
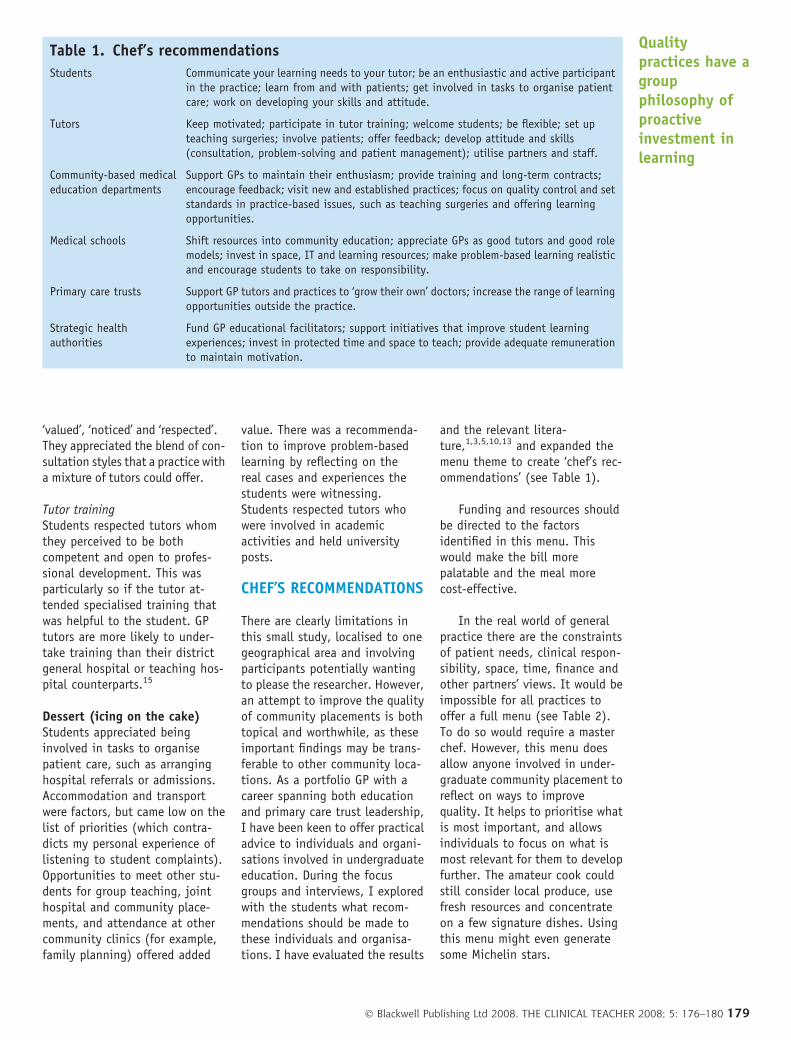
and the relevant litera-ture,1,3,5,10,13 and expanded themenu theme to create ‘chef’s rec-ommendations’ (see Table 1).
Funding and resources shouldbe directed to the factorsidentified in this menu. Thiswould make the bill morepalatable and the meal morecost-effective.
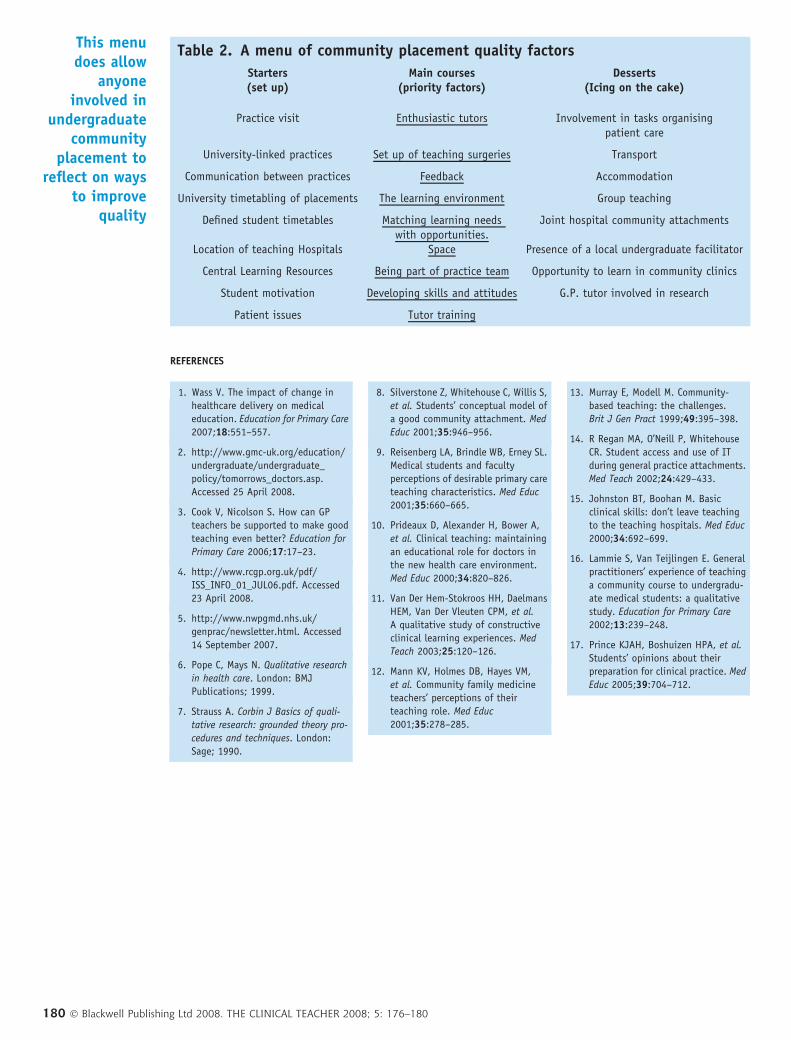
In the real world of generalpractice there are the constraintsof patient needs, clinical respon-sibility, space, time, finance andother partners’ views. It would beimpossible for all practices tooffer a full menu (see Table 2).To do so would require a masterchef. However, this menu doesallow anyone involved in under-graduate community placement toreflect on ways to improvequality. It helps to prioritise whatis most important, and allowsindividuals to focus on what ismost relevant for them to developfurther. The amateur cook couldstill consider local produce, usefresh resources and concentrateon a few signature dishes. Usingthis menu might even generatesome Michelin stars.
Table 1. Chef’s recommendations
Students Communicate your learning needs to your tutor; be an enthusiastic and active participantin the practice; learn from and with patients; get involved in tasks to organise patientcare; work on developing your skills and attitude.
Tutors Keep motivated; participate in tutor training; welcome students; be flexible; set upteaching surgeries; involve patients; offer feedback; develop attitude and skills(consultation, problem-solving and patient management); utilise partners and staff.
Community-based medicaleducation departments
Support GPs to maintain their enthusiasm; provide training and long-term contracts;encourage feedback; visit new and established practices; focus on quality control and setstandards in practice-based issues, such as teaching surgeries and offering learningopportunities.
Medical schools Shift resources into community education; appreciate GPs as good tutors and good rolemodels; invest in space, IT and learning resources; make problem-based learning realisticand encourage students to take on responsibility.
Primary care trusts Support GP tutors and practices to ‘grow their own’ doctors; increase the range of learningopportunities outside the practice.
Strategic healthauthorities
Fund GP educational facilitators; support initiatives that improve student learningexperiences; invest in protected time and space to teach; provide adequate remunerationto maintain motivation.
Qualitypractices have agroupphilosophy ofproactiveinvestment inlearning
� Blackwell Publishing Ltd 2008. THE CLINICAL TEACHER 2008; 5: 176–180 179
REFERENCES
1. Wass V. The impact of change in
healthcare delivery on medical
education. Education for Primary Care
2007;18:551–557.
2. http://www.gmc-uk.org/education/
undergraduate/undergraduate_
policy/tomorrows_doctors.asp.
Accessed 25 April 2008.
3. Cook V, Nicolson S. How can GP
teachers be supported to make good
teaching even better? Education for
Primary Care 2006;17:17–23.
4. http://www.rcgp.org.uk/pdf/
ISS_INFO_01_JUL06.pdf. Accessed
23 April 2008.
5. http://www.nwpgmd.nhs.uk/
genprac/newsletter.html. Accessed
14 September 2007.
6. Pope C, Mays N. Qualitative research
in health care. London: BMJ
Publications; 1999.
7. Strauss A. Corbin J Basics of quali-
tative research: grounded theory pro-
cedures and techniques. London:
Sage; 1990.
8. Silverstone Z, Whitehouse C, Willis S,
et al. Students’ conceptual model of
a good community attachment. Med
Educ 2001;35:946–956.
9. Reisenberg LA, Brindle WB, Erney SL.
Medical students and faculty
perceptions of desirable primary care
teaching characteristics. Med Educ
2001;35:660–665.
10. Prideaux D, Alexander H, Bower A,
et al. Clinical teaching: maintaining
an educational role for doctors in
the new health care environment.
Med Educ 2000;34:820–826.
11. Van Der Hem-Stokroos HH, Daelmans
HEM, Van Der Vleuten CPM, et al.
A qualitative study of constructive
clinical learning experiences. Med
Teach 2003;25:120–126.
12. Mann KV, Holmes DB, Hayes VM,
et al. Community family medicine
teachers’ perceptions of their
teaching role. Med Educ
2001;35:278–285.
13. Murray E, Modell M. Community-
based teaching: the challenges.
Brit J Gen Pract 1999;49:395–398.
14. R Regan MA, O’Neill P, Whitehouse
CR. Student access and use of IT
during general practice attachments.
Med Teach 2002;24:429–433.
15. Johnston BT, Boohan M. Basic
clinical skills: don’t leave teaching
to the teaching hospitals. Med Educ
2000;34:692–699.
16. Lammie S, Van Teijlingen E. General
practitioners’ experience of teaching
a community course to undergradu-
ate medical students: a qualitative
study. Education for Primary Care
2002;13:239–248.
17. Prince KJAH, Boshuizen HPA, et al.
Students’ opinions about their
preparation for clinical practice. Med
Educ 2005;39:704–712.
This menudoes allow
anyoneinvolved in
undergraduatecommunity
placement toreflect on ways
to improvequality
Table 2. A menu of community placement quality factors
Starters(set up)
Main courses(priority factors)
Desserts(Icing on the cake)
Practice visit Enthusiastic tutors Involvement in tasks organisingpatient care
University-linked practices Set up of teaching surgeries Transport
Communication between practices Feedback Accommodation
University timetabling of placements The learning environment Group teaching
Defined student timetables Matching learning needswith opportunities.
Joint hospital community attachments
Location of teaching Hospitals Space Presence of a local undergraduate facilitator
Central Learning Resources Being part of practice team Opportunity to learn in community clinics
Student motivation Developing skills and attitudes G.P. tutor involved in research
Patient issues Tutor training
180 � Blackwell Publishing Ltd 2008. THE CLINICAL TEACHER 2008; 5: 176–180





























