Embed Size (px)
Citation preview

I
Aw
Ap
P
DB
I
Caaaiarsoilwm
C
Aho
E
0h
r e v a s s o c m e d b r a s . 2 0 1 3;5 9(6):531–533
Revista da
ASSOCIAÇÃO MÉDICA BRASILEIRA
www.ramb.org .br
mage in Medicine
giant aneurysm from the petrous carotid presentingith isolated peripheral facial palsy�
neurisma gigante da carótida petrosa apresentando paralisia facialeriférica isolada
edro Tadao Hamamoto Filho ∗, Vitor Cesar Machado, Carlos Clayton Macedo-de-Freitas
iscipline of Neurosurgery, Faculdade de Medicina de Botucatu, Universidade Estadual Paulista Julio de Mesquita Filho (Unesp),otucatu, SP, Brazil
ntroduction
arotid aneurysms from the petrous segment are rare. Theyre usually asymptomatic and do not present with a sub-rachnoid haemorrhage. Clinical presentation depends onneurysm’s location, size, and direction of growth. Aneurysmsn close proximity to the medium ear may cause hypoacusisnd tinnitus. Otorrhagia and epistaxis may also occur after theupture of an aneurysm, as well as Horner’s syndrome andymptoms of the jugular foramen nerves. The involvementf the VII nerve is not common. Current treatment options
nclude carotid artery balloon occlusion, whether or not fol-owed by a bypass through the external carotid; embolization
ith coils; remodelling with stents; or a conservative manage-ent by serial imaging exams.1
ase report
77-year-old woman, previously diagnosed with arterialypertension, was referred to this service within two monthsf her diagnosis of progressive right facial palsy. She presented
� Study conducted at the Department of Neurology, Psychology, anstadual Paulista Júlio de Mesquita Filho, Botucatu, SP, Brazil.∗ Corresponding author.
E-mail: [email protected] (P.T. Hamamoto Filho)104-4230/$ – see front matter © 2012 Elsevier Editora Ltda. All rights rettp://dx.doi.org/10.1016/j.ramb.2013.07.004
no other symptoms. Aside from right peripheral facial palsy(House-Brackmann score grade IV), her neurological examina-tion appeared normal. A magnetic resonance image showed alarge aneurysm arising from the petrous segment of the rightinternal carotid (Figs. 1 and 2).
An angiogram was performed (Fig. 3). The patient couldnot tolerate a balloon occlusion test. On the next day, an unre-markable embolization with coil placement was performed.Cerebral blood flow was not modified, and the aneurysm waspartially occluded with coils. The patient was discharged aftertwo days, without any other deficit besides facial palsy.
Discussion
Carotid aneurysms from the petrous segment are not com-mon, and its presentation with an isolated peripheral facialpalsy is even more rare. This article reported this rare condi-tion.
The internal carotid petrous segment extends from the
d Psychiatry of the Faculdade de Medicina of the Universidade
carotid’s entrance to the cranium, through the carotid channel(anterior to the jugular foramen and medial from the sty-loid processes), until their emergence through the cavernous
served.

532 r e v a s s o c m e d b r a s . 2 0 1 3;5 9(6):531–533
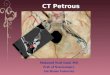
Fig. 1 – A high-resolution magnetic resonance angiographyshowing the aneurysm within the right carotid channel.
Fig. 2 – A 3-D magnetic resonance angiographyreconstruction showing the aneurysm (*) in tight relation tothe petrous bone.
Fig. 3 – An angiogram with selective catheterization of rightcarotid showing the aneurysm.
sinus. In the petrous segment, the carotid has two main com-ponents: vertical and horizontal, with a knee in between.Two branches may arise from the petrous carotid: the vid-ian and caroticotympanic arteries. The vidian artery passesanteriorly and inferiorly through the foramen lacerous, andanastomoses with external carotid branches. The carotico-tympanic artery is an embrionary vestige of the hyoid arterythat originates from the petrous carotid knee and passes supe-riorly through the stapedius to supply blood into the mediumear cavity.1,2
There are three proposed mechanisms in the etiology ofaneurysms from the carotid petrous portion: mycotic, trau-matic, and congenital.
Infections and inflammations of the medium ear mayerode bony structures and involve the artery adventitia, whichcan become weak and predispose the medium ear to aneurys-mal dilatation.3–6
The cervical petrous transition of the carotid artery makesit susceptible to stretch forces, which in turn make this seg-ment amenable to dissections and pseudoaneurysms, sincethe cervical portion is mobile and the petrous portion is not.2
Fibromuscular dysplasias have been suggested to be thecause of congenital aneurysms of the petrous carotid. Muscledefects were found at the acute angle of the artery branches’emerging areas. In fact, most of the aneurysms of this segmentwere found at the caroticotympanic segment.7,8
In the present patient, there was no previous history oftrauma or ear infection, and thus, a congenital abnormalitywas considered.
These aneurysms are generally asymptomatic, and diag-nosed as imaging findings. Therefore, the clinical presenta-
tion, when present, is variable and depends on the location,size, and direction of growth. Horner’s syndrome may occurdue to the involvement of sympathetic fibres. Defects in the
s . 2 0
Ipapms
pTtociciidpi
swsa
bwatcramgtls
r
1
2
3
4
5
6
7
8
basilar junction in a child. Neurosurgery. 1990;26:322–7.
r e v a s s o c m e d b r a
X, X, XI, and XII nerves may occur when the aneurysm extendsosteriorly and inferiorly. Ocular movements are affected withneurysms from the cavernous segment, but not from theetrous segment. The involvement of the VII nerve is uncom-on, and generally accompanied by VIII nerve symptoms,
uch as hypoacusis and tinnitus.A report by McCarron demonstrated a peripheral facial
alsy caused by a carotid dissection through the petrous area.wo hypotheses were considered for this clinical manifesta-ion: a mechanical compression of the nerve, and an alterationf its vascular supply due to emboli or local hemodynamichanges.9 These pathophysiological mechanisms are possiblen the case of an anatomical variation, in which the internalarotid is responsible for the supply of the VII nerve. Althoughn the majority of the cases the VII nerve vascular supplys maintained by the external carotid system via the mid-le meningeal arterial branches, it is believed that McCarron’sroposed mechanism could explain the present patient’s clin-
cal presentation.Treatment options include conservative management with
erial images; carotid surgical trapping and revascularizationith a bypass; endovascular internal carotid balloon occlu-
ion; embolization with coil placement, with or without stentssistance; and flow diverting techniques.
Asymptomatic patients with an incidental diagnosis coulde managed conservatively with serial images. Patientsho present with bleeding should quickly undergo a more
ggressive treatment, either open surgery or endovascularechniques. In cases of symptomatic patients presenting withranial nerve changes without an aneurysm rupture, theisks and benefits of each procedure should be carefullynalyzed. These risks include carotid occlusion and surgicalorbidity. Any benefits would revolve around avoiding the
rowth of the aneurysm. In patients with a pseudoaneurysm,here is a higher risk for rupture and bleeding, leading to aife-threatening condition; thus, more aggressive optionshould be considered.
9
1 3;5 9(6):531–533 533
Carotid occlusion may not be possible in patients withoutsufficient collateral flow, as bypass revascularization surgeryis not commonly available. The use of stents is inconvenientdue to prolonged anti-aggregation therapy.
Conflicts of interest
The authors declare no conflicts of interest.
e f e r e n c e s
. Liu JK, Gottfried ON, Amini A, Couldwell WT. Aneurysms of thepetrous internal carotid artery: anatomy, origins, andtreatment. Neurosurg Focus. 2004;17:E13.
. Palacios E, Gómez J, Alvernia JE, Jacob C. Aneurysm of thepetrous portion of the internal carotid artery at the foramenlacerum: anatomic, imaging and otologic findings. Ear NoseThroat J. 2010;89:303–5.
. Ehni G, Barrett JH. Hemorrhage from the ear due to ananeurysm of internal carotid. N Engl J Med. 1960;262:1323–5.
. Morantz RA, Kirchner FR, Kishore P. Aneurysms of the petrousportion of the internal carotid artery. Surg Neurol. 1976;6:313–8.
. McGrail KM, Heros RC, Debrun G, Beyerl BD. Aneurysm of theICA petrous segment treated by baloon entrapment after EC-ICbypass. J Neurosurg. 1986;65:249–52.
. Oyama H, Hattori K, Tanahashi S, Kito A, Maki H, Tanahashi K.Ruptured pseudoaneurysm of the petrous internal carotidartery caused by chronic otitis media. Neurol Med Chir (Tokyo).2010;50:578–80.
. Bergès C, Pollak A, Valavanis A, Fisch U. Gradual facial palsyand intrapetrous internal carotid aneurysm: a case report.Skull Base Surg. 1993;3(3):164–9.
. Guha A, Montanera W, Hoffman HJ. Congenital aneurysmaldilatation of the petrous-cavernous carotid artery and vertebral
. McCarron MO, Metcalfe RA, Muir KW. Facial nerve palsysecondary to internal carotid artery dissection. Eur J Neurol.2000;7:723–5.