Embed Size (px)
Citation preview

A Framework for Discussing Outcome Measures in
Stuttering
J. Scott Yaruss, Ph.D., CCC-SLPUniversity of Pittsburgh
ASHA SID4 Leadership ConferenceTucson, AZ — May 1, 1997

Purpose
• To present a conceptual framework for viewing treatment outcomes in terms of the “ABC” reactions to stuttering
Affective
Behavioral
Cognitive

What should we measure?

Roadblocks
• Diversity of Treatments
• Scope of Treatments
• Definitions of Success
• Diversity of Clients
• Inconsistencies in Terminology

The International Classification of Impairments, Disabilities, and
Handicaps (ICIDH)• Designed to describe the consequences of
health-related problems (i.e., the individual’s experience of diseases or disorders)
Disease orDisorder
DisabilityImpairment Handicap
World Health Organization (1980) Original Framework

Definitions of I, D, and H(WHO, 1980)
• Impairment: “any loss or abnormality of psychological, physiological, or anatomical structure or function.”
• Disability: “any restriction of lack of ability to perform an activity in the [normal] manner”
• Handicap: “a disadvantage for an individual, resulting from an I or D, that limits...the fulfill-ment of a role that is normal...for that individual.”

ICIDH Example• A skeletal impairment may be difficulty moving the arm
(§71.0: Mechanical impairment of... upper arm). – The etiology of the impairment may be a broken arm, MS,
or another problem—this does not matter for the ICIDH
• This impairment may lead to disabilities, such as difficulty writing (§28), dressing (§35) or reaching (§53)
• The impairment and disability may then lead to handicaps, such as disadvantages related to physical independence (§2), mobility (§3), or occupation (§4, e.g., curtailed occupation in fields that require arm mobility).

I, D, and H for Stuttering(after Yaruss, in prep)
• Impairment: Disruption in the functioning of the speech mechanism characterized by interruption in the forward flow of speech (i.e, stuttering)
• Disability: Limitations in an individual’s ability to communicate with others or to engage in social or work-related activities
• Handicap: Disadvantages experienced by an individual that limit the individual’s ability to fulfill social, occupational, or economic roles

ICIDH and Stuttering Example
• The basic stuttering impairment is the production of disfluencies (§37.0: Impairment of speech fluency) – There are many theories re the etiology of this
impairment, it seems safe to say that it involves multiple factors
• This impairment may lead to disabilities, such as difficulty talking (§21), performing at work (§18.4) or coping with situations (§14.2)
• The impairment and disability may lead to handicaps, such as disadvantages related to occupation (§4.2),social participation (§5.1), or economic well-being (§6.3)

Confusion regardingthe ICIDH andStuttering
• Previous definitions of I, D, and H in stuttering have equated impairment with etiology and disability with handicap, so they were not consistent with the WHO’s definitions
• The link between the stuttering impairment and resulting disabilities is not as direct as with many physical impairments and disabilities

Mediating Disability:The ABCs of Stuttering
• The link between I and D is mediated by the individual’s reactions to stuttering– Affective: Feelings, attitudes, emotions
– Behavioral: Avoidance, tension, struggle
– Cognitive: thought-processes, self-evaluation
DisabilityImpairment HandicapABC
ReactionsUnderlying
Etiology

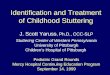
A Conceptual Framework for Discussing Treatment Outcomes in Stuttering
(after Yaruss, in prep)
Disability
Reactions
EnvironmentalInfluences andOther Factors
Note: Solid lines indicateobligatory relationships
(i.e., "A leads to B").Dashed lines indicateoptional relationships
(i.e. "A may lead to B")
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology

A Conceptual Framework for Discussing Treatment Outcomes in Stuttering
(after Yaruss, in prep)
Disability
Reactions
EnvironmentalInfluences andOther Factors
Note: Solid lines indicateobligatory relationships
(i.e., "A leads to B").Dashed lines indicateoptional relationships
(i.e. "A may lead to B")
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology

A Conceptual Framework for Discussing Treatment Outcomes in Stuttering
(after Yaruss, in prep)
Disability
Reactions
EnvironmentalInfluences andOther Factors
Note: Solid lines indicateobligatory relationships
(i.e., "A leads to B").Dashed lines indicateoptional relationships
(i.e. "A may lead to B")
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology

A Conceptual Framework for Discussing Treatment Outcomes in Stuttering
(after Yaruss, in prep)
Disability
Reactions
EnvironmentalInfluences andOther Factors
Note: Solid lines indicateobligatory relationships
(i.e., "A leads to B").Dashed lines indicateoptional relationships
(i.e. "A may lead to B")
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology

A Conceptual Framework for Discussing Treatment Outcomes in Stuttering
(after Yaruss, in prep)
Disability
Reactions
EnvironmentalInfluences andOther Factors
Note: Solid lines indicateobligatory relationships
(i.e., "A leads to B").Dashed lines indicateoptional relationships
(i.e. "A may lead to B")
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology

Applying the Framework to Treatment Outcomes Research
• Helping to answering the question,What should we measure?”
• Two approaches to measuringtreatment outcomes– Documenting that a specific treatment program accomplishes the specific goals it
sets
– Establishing criteria for success across the entire field and testing all programs against that criterion

Assessing Outcomesfor Specific Treatments
• Every treatment program should
document whether or not it achieves its goals
– Describe, in detail, the nature of the program
– Define success clearly
– Operationalize clinical decision-making
– Measure outcomes (before, during, & after treatment)
– Report changes objectively (good and bad)

Assessing Outcomes forSpecific Treatment Programs
Disability
Reactions
EnvironmentalInfluences andOther Factors
Note: Solid lines indicateobligatory relationships
(i.e., "A leads to B").Dashed lines indicateoptional relationships
(i.e. "A may lead to B")
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology

Level of measurement = level of treatmentTreatmentLevel
Examples ofTreatment Approach
Examples ofOutcome Measures
Etiology Retraining speech motor patterns;Improving language formulation
Changes in kinematics ortiming of movement, wordretrieval skills, etc.
Impairment Prolonged speech and otherspeech modification approaches
Changes in speech fluency(observable characteristics)
Reactions Counseling, desensitization;stuttering modifications to reducetension and struggle
Changes in speech attitudes,avoidance behaviors, cognitivereactions, etc.
Disability Generalization/Transfer activities,Desensitization on situationalhierarchy
Changes in ability to entersituations, perform tasks atwork (functional outcomes)
Environment Reducing environmental demands Changes in parents speakingrate, turn-taking pause, etc.
Handicap (?) Educating public and others aboutstuttering to reduce disadvantages
Quality of life scales ??
Level of measurement = level of treatment

Assessing OutcomesAcross the Field• Need to reach an agreement
about appropriate level of measurement
– Option #1: Restrict assessment to speech (i.e. impairment-level) measures, since stuttering is a speech event (Joy Armson will discuss this)
– Option #2: Assess at several different levels• Probably not etiology…too much disagreement
• Probably not handicap…out of our realm

A Proposal for Measuring the Outcome of Stuttering Treatment
• Three Realms of Measurement:
– Impairment: speech fluency
– Reactions: affective, behavioral, cognitive responses
– Disability: ability to perform tasks (functional outcome)
• Rationale
– Allows different opinions about what is most important (including
features that are “under the surface”)
– Recognizes that the most successful client is one who can function
better in society (regardless of type of tx)

Tests and Measures ofImpairment and Reactions
• Impairment: speech-level measures
– Frequency, Duration, Type, Severity of Disfluency
– Speech Naturalness, Speaking Rate
• Reactions: ABCs
– Affective (e.g., Speech attitudes S-24, ICA, Self-Ratings)
– Behavioral (e.g., Avoidance of speaking situations, tension,
struggle Speech Situation Checklist, ICA, SESAS)
– Cognitive (e.g., Locus of control, thoughts about speaking abilities
ICA, LCB/LOC, SESAS)

Assessing Functional Outcomes• Assesses ability to communicate in real-life setting
• One model is the ASHA FACS
– Scores communication independence in several realms
• social communication; communication of basic needs; reading, writing, and number concepts; daily planning
– Uses 7-point scale (does...does with assistance...does not)
• In stuttering, we could assess clients’ ability to:– verbally communicate (disability in talking)
– function at work (disability in work performance)
– function in social situations (situation coping disability)

Ability to Verbally Communicate• How often does the client do the following? (1=never,
3=sometimes, 5=frequently)
– Have difficulty communicating verbal messages
– Have difficulty initiating, maintaining, or completing conversations
(e.g., because of listener’s reactions)
– Have difficulty speaking under time pressures
– Substitute less appropriate words to avoid stuttering
– Avoid introducing self, answering questions, or making socially
appropriate talk when meeting a new person
– Not respond when s/he knows the answer to a question

Ability to Communicate at Work• How often does the client have difficulty with the
following? (1=never, 5=frequently)
– Answering the phone / Making phone calls at work
– Interacting with superiors, co-workers, employees
– Interacting with customers, clients, colleagues
– Participating in meetings (contributing ideas, etc.)
– Gathering information (i.e., asking questions)
– Giving oral presentations
– Performing other work-related tasks (completing training, making favorable impression, etc.)

Ability to Communicate in Speaking Situations
• How often does the client have difficulty with the
following? (1=never, 5=frequently)
– Using the telephone (for a variety of purposes)
– Interacting with family/friends/children
– Interacting with strangers/groups/authority figures
– Making speeches to small/large groups
– Asking for directions, Asking for advice
– Ordering food at a restaurant/drive-thru

Functional Outcomes vs.Other Outcomes Measures
• Some functional outcomes questions seem similar to those in
existing scales of speech attitudes, behaviors, situations, etc.
– The focus is not on how clients feel or think about stuttering, but on
their ability to do tasks
• ICA: feelings and beliefs about speaking and situations
• SESAS: thoughts (confidence) about speaking situations
• Functional assessment: ability to do certain life tasks
– Instruments should be used together in evaluation

Summary
Disability
Reactions
EnvironmentalInfluences andOther Factors
Behavioral
Affective
Cognitive
HandicapImpairmentPresumedEtiology