Embed Size (px)
Citation preview

A comparison of patients with intellectual disabilityreceiving specialised and general services inOntario’s psychiatric hospitals
Y. Lunsky,1,2 E. Bradley,2,3 J. Durbin1,2 & C. Koegl1
1 Centre for Addiction and Mental Health,Toronto, Ontario, Canada2 University of Toronto,Toronto, Ontario, Canada3 Surrey Place Centre,Toronto, Ontario, Canada
Abstract
Background Over the years, the closure of institu-tions has meant that individuals with intellectualdisabilities (IDs) must access mainstream (i.e.general) mental health services. However, concernthat general services may not adequately meet theneeds of patients with ID and mental illness has ledto the development and implementation of morespecialised programmes. This study comparespatients with ID receiving specialised services topatients with ID receiving general services in Ontar-io’s tertiary mental healthcare system in terms ofdemographics, symptom profile, strengths andresources and clinical service needs.Method A secondary analysis of Colorado ClientAssessment Record data collected from all tertiarypsychiatric hospitals in the province was completedfor all 371 inpatients with ID, from both specialisedand general programmes.Results Inpatients in specialised programmes weremore likely to have a diagnosis of mood disorderand were less likely to have a substance abuse or
psychotic disorder. Individuals receiving specialisedservices had higher ratings of challenging behaviourthan those in more general programmes. The twogroups did not differ significantly in terms of rec-ommended level of care, although more inpatientsfrom specialised programmes were rated as requir-ing Level 4 care than inpatients from generalprogrammes.Conclusions In Ontario, inpatients in specialisedand general programmes have similar overall levelsof need but unique clinical profiles that should betaken into consideration when designing interven-tions for them.
Keywords inpatients, intellectual disabilities,mental health, psychiatric services
Introduction
In many countries, the practice of normalisationand the related closure of institutions have meantthat individuals with intellectual disabilities (IDs)are increasingly being expected to use generalpopulation mainstream health services, includingmental health care. There is growing consensus,however, that general inpatient and outpatient
Correspondence:Yona Lunsky, Psychologist, Dual DiagnosisProgram, Centre for Addiction and Mental Health, 1001 QueenStreet W., Unit 4-4, Toronto, Ontario, Canada M6J 1H4 (e-mail:[email protected]).
Journal of Intellectual Disability Research doi: 10.1111/j.1365-2788.2008.01049.x
volume 52 part 11 pp 1003–1012 november 20081003
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

psychiatric care is inadequate to manage thecomplex needs of at least some individuals with IDand mental health/behaviour concerns. According toChaplin (2004), general services may be sub-optimal because of a lack of specialist training,limited resources and unhelpful attitudes of health-care providers. Also patients with ID receivinggeneral inpatient care are particularly vulnerableto exploitation by other patients (Kwok 2001;Xenitidis et al. 2004; Charlot & Beasley 2005).
Limitations of general psychiatric services haveled to the development of specialised psychiatricprogrammes for patients with ID. Specialised ser-vices can be smaller, with higher staff to patientratios and greater safety, and supported by interdis-ciplinary teams that are well versed in the biopsy-chosocial approach to assessment and treatment ofindividuals with ID (Reid 1995; Chaplin 2004;Charlot & Beasley 2005; Morris 2005). Daily pro-gramming in specialised inpatient units can be tai-lored to the cognitive level and adaptive behaviourof the patients and thus can be more stimulatingand beneficial to them.
A number of studies have described patients withID using general inpatient services (Addington et al.1993; Burge et al. 2002; Saeed et al. 2003). Otherstudies have described sociodemographic and clini-cal characteristics of individuals with ID receivingspecialised inpatient services (e.g. Ashaye et al.1997; Raitasuo et al. 1999; Xenitidis et al. 1999;Tajuddin et al. 2004; Hall et al. 2006). These studiesfail to address an important question, however: in ahealthcare system where both services exist, how doindividuals with ID accessing specialised vs. generalpsychiatry services differ? The answer can offerinsight into whether individuals are triaged intothese different types of care based on higher levelsof need, and can set the stage for assessing whatpatient groups benefit from more specialised treat-ment settings.
In our review, we found two studies that com-pared inpatients with ID who accessed specialisedvs. general mental health services. Alexander et al.(2001) contrasted services in two London districts,both with well-developed community teams in ID,one with a specialised psychiatric inpatient unit,and one with access to beds in a general psychiatricinpatient unit. Through retrospective chart reviews,they found that the most commonly referred indi-
viduals to both settings were young men withaggressive behaviour. Patients receiving specialisedinpatient services were more likely to have moresevere ID but were less likely to be living indepen-dently at time of admission, and had significantlylonger lengths of stay compared to those in generalunits. In another London-based study (Xenitidiset al. 2004), individuals in the specialised unit werecontrasted to adults with ID in general inpatientunits. The two groups did not differ with regard todemographics or diagnosis at time of admission, butdid differ in terms of length of stay and outcome;Individuals in specialised units had significantlylonger lengths of stay than patients in general unitsand they were less likely to be discharged to an ‘outof catchment area’ placement.
These results suggest that some triaging is occur-ring in the UK service system, where health policyand statutory health and social service requirementsrelated to mental health and ID are in place, andwhere ID is a recognised subspecialty of psychiatryand nursing. Practices regarding access to care maydiffer in other countries, depending on how servicesare funded, educational opportunities and the exist-ence or lack thereof of specialised service policies(Holt et al. 2000; Smiley et al. 2002). The presentpaper takes advantage of a province-wide study ofthe needs of patients (that include a subgroup withID) using psychiatric hospitals in the province ofOntario (largest province in Canada). In Ontario,individuals with ID have been accessing generalpsychiatry services for the past three decades withthe first policy document on their specialisedmental health needs appearing in 1997 (OntarioMinistries of Health and Community and SocialServices, 1997).
The Comprehensive Assessment Projects (CAPs)explored the clinical profile and service needs ofindividuals with ID receiving tertiary level mentalhealth care across Ontario. In an earlier paper(Lunsky et al. 2006), all inpatients and outpatientswith ID and psychiatric diagnoses were comparedwith other Ontario psychiatric hospital users andindividuals with ID were found to have more severeclinical symptoms and fewer resources than indi-viduals without ID. In this earlier study no distinc-tion was made between patients with ID inspecialised vs. general services, however. The goal ofthe present study was to further examine the group
1004Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

with ID in the CAPs planning study in terms ofthose who received care in general compared withspecialist inpatient programmes. If indeed theaccess continuum from general to specialised ser-vices is working well, we hypothesised that thosewith the most severe needs, whose needs cannot bemet through general services, would be filtered tospecialised programmes.
Methods
Sample and data collection
The sample for this study was drawn from a mentalhealth services planning study (CAPs) conducted inOntario during 1998–2003. Study patients weredrawn from all nine psychiatric hospitals respon-sible for providing tertiary inpatient mental healthservices to urban, semi-urban and rural communi-ties. Tertiary inpatient programmes in Ontario aremandated to serve individuals with complex orchronic mental health disturbances. Such pro-grammes provide the highest level of care (seeTable 1 for description of other levels of care) in themental health service continuum in Ontario. Allprogrammes included in this study serve personsaged 16 or older with severe and persistent mentalhealth illness.
The planning study employed a cross-sectionaldesign, assessing all facility inpatients on a desig-nated census day. The census date varied by facility,because the planning study occurred over 5 years,one hospital at a time. In total the study assessed2218 inpatients. The cross-sectional design wasexpected to produce a reasonably accurate estimateof patient needs, given the stability of the inpatientpopulation. The assessed patients averaged3.65 years in hospital at the time of the assessment,and only 13% of inpatients had been in the hospitalfor less than 1 month (Lunsky et al. 2006).
Standardised assessments were completed bytrained staff based on their familiarity with thepatients being rated and medical chart documenta-tion (Durbin et al. 2001). For each patient, staffindicated the presence or absence of a developmen-tal disability in the disability section of the assess-ment. (In Ontario, the term ‘developmentaldisability’ is equivalent to the term ‘mental retarda-tion’ in DSM-IV-TR). Staff also reported any psy-chiatric diagnoses, including mental retardation, byselecting categories (e.g. mood disorder, substanceabuse disorder, anxiety disorder, etc.) based on psy-chiatric diagnoses in the ICD-9. A patient wasincluded in this study if he or she was recorded ashaving a developmental disability or a mental retar-dation diagnosis in addition to a psychiatric diagno-sis (Lunsky et al. 2003). Using these criteria, weexcluded a small number of cases (n = 21) forwhich there was a designation of developmental dis-ability or a diagnosis of mental retardation, but aprecise psychiatric diagnosis was unknown orunavailable. This approach resulted in a final totalof 371 inpatients with ID.
Of the 371 inpatients included in this study, 102
(27.5%) were enrolled in one of five specialised psy-chiatric inpatient units across Ontario (for detaileddescription of these units, see Morris 2005). Whendata for the present study were collected, these spe-cialised units were in transition. There was anacknowledgement over many years of the need foradditional services beyond general inpatient psychi-atric hospital services. By 1998–2003 when theCAPs study was done, each of the five designatedwards had a mix of long-term and short-termpatients with ID, with a range of functioning levels.Each such unit offered specialised programmes ofcare and an interdisciplinary staff team, but all
Table 1 Recommended level of care template
Level Description
Level 1: Self-management with intermittent use of corecommunity services and supports.
Level 2: Individualised support on a weekly basis.Psychiatric care provided through regularcontact with a psychiatrist or mental healthnurse in an outpatient setting.
Level 3: Community living with intensive integratedtreatment and support (daily with 24 h access).Usually associated with Assertive CommunityTreatment.
Level 4: Residential treatment with a strong rehabilitationcomponent.This level is appropriate for personswhose behaviours make it difficult to liveindependently and at times need a secureenvironment.
Level 5: Tertiary inpatient care.
1005Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

struggled with staff recruitment and retention(Morris 2005). At this time, these specialised hospi-tal programmes were designed to serve individualswith ID and mental health needs. General units,although specialised in some cases (e.g. forensic,schizophrenia), were not specialised for patientswith IDs.
Institutional ethics review board approval for con-ducting secondary analyses comparing inpatientswith ID in general and specialised programmes wasobtained.
Measure
Colorado Client Assessment Record
The Colorado Client Assessment Record (CCAR)is a standardised tool for conducting a comprehen-sive assessment of patient functioning (Ellis et al.1984, 1991). The CCAR allows staff to record basicpatient information such as current diagnosis andhistory of illness; legal, marital, employment andeducation status; residential stability and service/support needs. Based on their knowledge of thepatient, input from other staff and case notes, staffalso assess patient impairments and strengths across25 domains of functioning and two global ratings.Each domain is rated on a 9-point scale from 1
(high functioning/no special problem) to 9 (lowfunctioning/extreme problem of difficulty). Adetailed administration manual defines the CCARdomains and rating anchors, and all raters attendeda 1-day training session and practice using the toolwith case examples. Data from both US andOntario studies support the reliability and validityof the CCAR (Schwartz 1999; Durbin et al. 2001;Coffman 2004). As the Ontario CAPs study, theCCAR and level of care template (see Table 1) havebeen adopted in other Canadian provinces.
Level of care assessment
For all of the CAPs related studies, a level of caretemplate was developed to provide a systematicapproach for matching an individual to a particularlevel of care, based on need. The template isintended to support needs-based service planningfor various patient groups. It aims to assign thepatients to the least restrictive level of care to meettheir needs, hence, was intended to support system
wide efforts to expand the community care systemand discharge long stay individuals who could beserved in the community.
An individual was assigned to a recommendedlevel of care through use of a standardised algo-rithm using ratings from six of the 25 CCARdomains: security/management risk, overall problemseverity, self care/basic needs, overall lack ofresources, danger to self and danger to others.Patients were assigned to one of five recommendedlevels of care (see Table 1) ranging from self-management (Level 1) to tertiary level inpatientcare (Level 5) based on this algorithm. The tem-plate was developed through a combination of lit-erature review and stakeholder input, resulting ingood face and content validity. Comparison ofpatients assigned to different levels of care based onindependent measures of need showed that patientswith more complex conditions were assigned to ahigher recommended level of care, supporting con-current validity of the algorithm (Durbin et al.2001). This template is currently being used acrosshospitals and community mental health services inthe province.
Analyses
Differences between patients with ID receiving spe-cialised and general psychiatric services on demo-graphics, diagnoses and recommended level of carewere compared using Chi-squared tests. Differencesbetween patients in specialised and general pro-grammes on symptom severity and strengths andresources were compared using t-tests. Analyseswere performed with spss (version 14, SPSS Inc,2005).
Results
Patient characteristics and symptom profile
Inpatients receiving specialised and those receivinggeneral mental health services were compared onthe basis of personal characteristics and psychiatricdiagnoses. Inpatients in specialised programmeswere significantly younger (X̄ = 37.9, SD = 10.44)than their counterparts accessing general inpatientservices [X̄ = 49.4, SD = 16.8; t(1, 363) = 6.43,P < 0.05] but did not differ in terms of number of
1006Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd
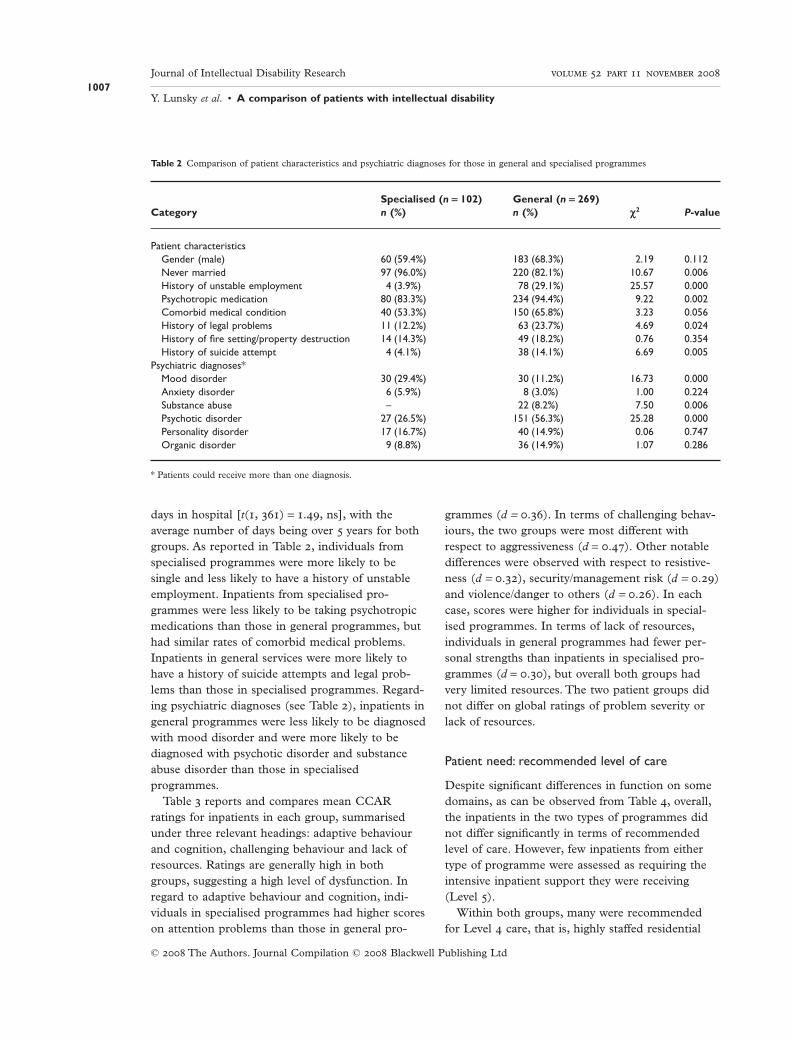
days in hospital [t(1, 361) = 1.49, ns], with theaverage number of days being over 5 years for bothgroups. As reported in Table 2, individuals fromspecialised programmes were more likely to besingle and less likely to have a history of unstableemployment. Inpatients from specialised pro-grammes were less likely to be taking psychotropicmedications than those in general programmes, buthad similar rates of comorbid medical problems.Inpatients in general services were more likely tohave a history of suicide attempts and legal prob-lems than those in specialised programmes. Regard-ing psychiatric diagnoses (see Table 2), inpatients ingeneral programmes were less likely to be diagnosedwith mood disorder and were more likely to bediagnosed with psychotic disorder and substanceabuse disorder than those in specialisedprogrammes.
Table 3 reports and compares mean CCARratings for inpatients in each group, summarisedunder three relevant headings: adaptive behaviourand cognition, challenging behaviour and lack ofresources. Ratings are generally high in bothgroups, suggesting a high level of dysfunction. Inregard to adaptive behaviour and cognition, indi-viduals in specialised programmes had higher scoreson attention problems than those in general pro-
grammes (d = 0.36). In terms of challenging behav-iours, the two groups were most different withrespect to aggressiveness (d = 0.47). Other notabledifferences were observed with respect to resistive-ness (d = 0.32), security/management risk (d = 0.29)and violence/danger to others (d = 0.26). In eachcase, scores were higher for individuals in special-ised programmes. In terms of lack of resources,individuals in general programmes had fewer per-sonal strengths than inpatients in specialised pro-grammes (d = 0.30), but overall both groups hadvery limited resources. The two patient groups didnot differ on global ratings of problem severity orlack of resources.
Patient need: recommended level of care
Despite significant differences in function on somedomains, as can be observed from Table 4, overall,the inpatients in the two types of programmes didnot differ significantly in terms of recommendedlevel of care. However, few inpatients from eithertype of programme were assessed as requiring theintensive inpatient support they were receiving(Level 5).
Within both groups, many were recommendedfor Level 4 care, that is, highly staffed residential
Table 2 Comparison of patient characteristics and psychiatric diagnoses for those in general and specialised programmes
CategorySpecialised (n = 102) General (n = 269)
c2 P-valuen (%) n (%)
Patient characteristicsGender (male) 60 (59.4%) 183 (68.3%) 2.19 0.112Never married 97 (96.0%) 220 (82.1%) 10.67 0.006History of unstable employment 4 (3.9%) 78 (29.1%) 25.57 0.000Psychotropic medication 80 (83.3%) 234 (94.4%) 9.22 0.002Comorbid medical condition 40 (53.3%) 150 (65.8%) 3.23 0.056History of legal problems 11 (12.2%) 63 (23.7%) 4.69 0.024History of fire setting/property destruction 14 (14.3%) 49 (18.2%) 0.76 0.354History of suicide attempt 4 (4.1%) 38 (14.1%) 6.69 0.005
Psychiatric diagnoses*Mood disorder 30 (29.4%) 30 (11.2%) 16.73 0.000Anxiety disorder 6 (5.9%) 8 (3.0%) 1.00 0.224Substance abuse – 22 (8.2%) 7.50 0.006Psychotic disorder 27 (26.5%) 151 (56.3%) 25.28 0.000Personality disorder 17 (16.7%) 40 (14.9%) 0.06 0.747Organic disorder 9 (8.8%) 36 (14.9%) 1.07 0.286
* Patients could receive more than one diagnosis.
1007Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd
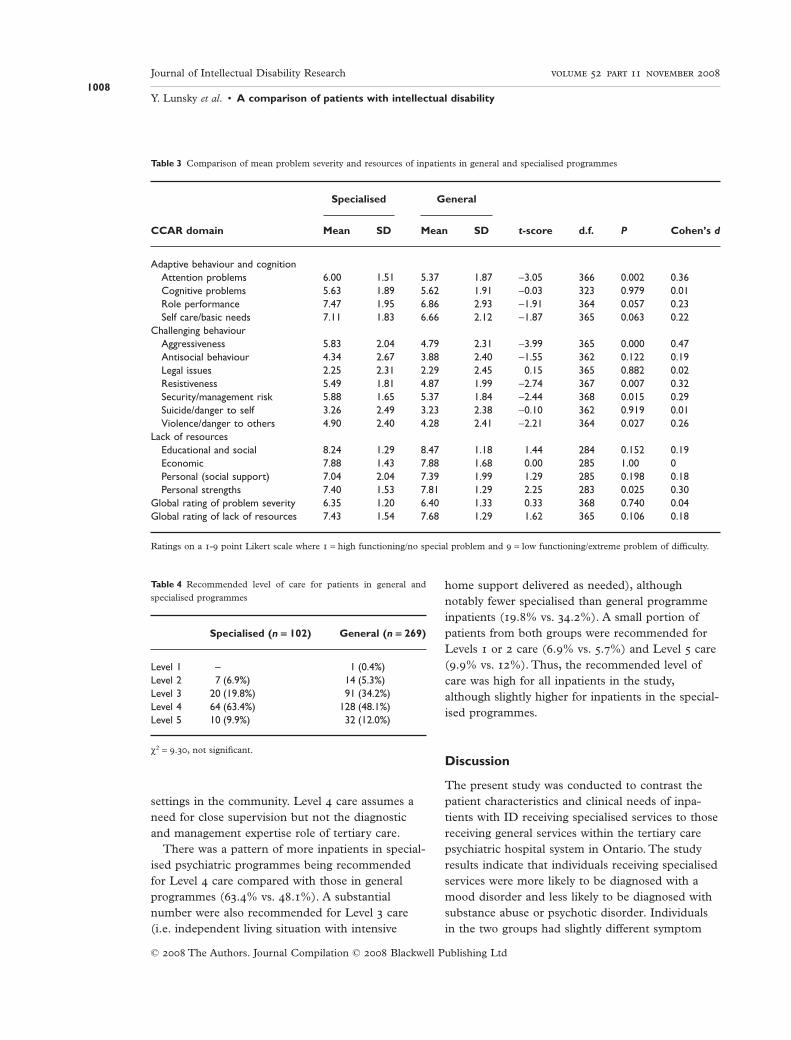
settings in the community. Level 4 care assumes aneed for close supervision but not the diagnosticand management expertise role of tertiary care.
There was a pattern of more inpatients in special-ised psychiatric programmes being recommendedfor Level 4 care compared with those in generalprogrammes (63.4% vs. 48.1%). A substantialnumber were also recommended for Level 3 care(i.e. independent living situation with intensive
home support delivered as needed), althoughnotably fewer specialised than general programmeinpatients (19.8% vs. 34.2%). A small portion ofpatients from both groups were recommended forLevels 1 or 2 care (6.9% vs. 5.7%) and Level 5 care(9.9% vs. 12%). Thus, the recommended level ofcare was high for all inpatients in the study,although slightly higher for inpatients in the special-ised programmes.
Discussion
The present study was conducted to contrast thepatient characteristics and clinical needs of inpa-tients with ID receiving specialised services to thosereceiving general services within the tertiary carepsychiatric hospital system in Ontario. The studyresults indicate that individuals receiving specialisedservices were more likely to be diagnosed with amood disorder and less likely to be diagnosed withsubstance abuse or psychotic disorder. Individualsin the two groups had slightly different symptom
Table 3 Comparison of mean problem severity and resources of inpatients in general and specialised programmes
CCAR domain
Specialised General
t-score d.f. P Cohen’s dMean SD Mean SD
Adaptive behaviour and cognitionAttention problems 6.00 1.51 5.37 1.87 -3.05 366 0.002 0.36Cognitive problems 5.63 1.89 5.62 1.91 -0.03 323 0.979 0.01Role performance 7.47 1.95 6.86 2.93 -1.91 364 0.057 0.23Self care/basic needs 7.11 1.83 6.66 2.12 -1.87 365 0.063 0.22
Challenging behaviourAggressiveness 5.83 2.04 4.79 2.31 -3.99 365 0.000 0.47Antisocial behaviour 4.34 2.67 3.88 2.40 -1.55 362 0.122 0.19Legal issues 2.25 2.31 2.29 2.45 0.15 365 0.882 0.02Resistiveness 5.49 1.81 4.87 1.99 -2.74 367 0.007 0.32Security/management risk 5.88 1.65 5.37 1.84 -2.44 368 0.015 0.29Suicide/danger to self 3.26 2.49 3.23 2.38 -0.10 362 0.919 0.01Violence/danger to others 4.90 2.40 4.28 2.41 -2.21 364 0.027 0.26
Lack of resourcesEducational and social 8.24 1.29 8.47 1.18 1.44 284 0.152 0.19Economic 7.88 1.43 7.88 1.68 0.00 285 1.00 0Personal (social support) 7.04 2.04 7.39 1.99 1.29 285 0.198 0.18Personal strengths 7.40 1.53 7.81 1.29 2.25 283 0.025 0.30
Global rating of problem severity 6.35 1.20 6.40 1.33 0.33 368 0.740 0.04Global rating of lack of resources 7.43 1.54 7.68 1.29 1.62 365 0.106 0.18
Ratings on a 1-9 point Likert scale where 1 = high functioning/no special problem and 9 = low functioning/extreme problem of difficulty.
Table 4 Recommended level of care for patients in general andspecialised programmes
Specialised (n = 102) General (n = 269)
Level 1 – 1 (0.4%)Level 2 7 (6.9%) 14 (5.3%)Level 3 20 (19.8%) 91 (34.2%)Level 4 64 (63.4%) 128 (48.1%)Level 5 10 (9.9%) 32 (12.0%)
c2 = 9.30, not significant.
1008Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

presentations with higher ratings in challengingbehaviour in those receiving specialised services.However, the two groups did not differ in theiroverall recommended level of care or in theirnumber of days in hospital at time of survey. Thusindividuals in both types of programmes havecomplex needs that warrant special attention.
This study has several limitations, which shouldbe taken into consideration when interpreting itsfindings. First, data reported here are based on sec-ondary analyses of data developed for anotherpurpose. Information regarding level of ID was notavailable and issues such as accuracy of ID and psy-chiatric diagnosis cannot be addressed using thisdatabase, but should be given consideration infurther research (see Lunsky & Bradley 2007).Second, the level of care algorithm adopted herehas demonstrated concurrent validity, yet is stillrelatively new and would benefit from furthertesting, especially in psychiatric populations withcomplex comorbidities such as ID. Third, findingsare based on the subgroup of individuals with IDand mental health needs being served by Ontario’stertiary level care psychiatric hospitals. This studydoes not address the needs of those who access ser-vices outside of the tertiary care system or who arenot receiving any services. Findings may not applyto individuals in other areas where different servicemodels and policies exist. Thus, more research fromother countries is required.
Hall et al. (2006) argue that a combination ofspecialised and general services is necessary becausespecialised services do not have the capacity toserve everyone. Decisions regarding who shouldaccess the most specialised services should beinformed by research. There was some evidence inthis study that certain patients were triaged to spe-cialised services. Patients in specialised programmestended to be younger and have a more stableemployment/day programme history. They were lesslikely to have a history of suicide attempts andmore likely to have always been single and to bediagnosed as depressed. However, they displayedmore challenging behaviour (e.g. aggression, secu-rity risk, resistiveness, violence) than other patients.This patient profile is consistent with a qualitativefollow-up study conducted across the province toreview and interpret the CAPS data that are pre-sented here (Lunsky & Puddicombe 2005). Com-
munity staff participating in regional focus groupsreported that the typical patient referred for special-ised services tended to be receiving residential ser-vices from agencies that support people with IDs,but displaying levels of aggression that could not besafely managed without specialist attention. In con-trast, patients referred to general inpatient pro-grammes were less likely to be connected toresidential services for individuals with IDs prior tohospital admission and were more likely to havehad instability (e.g. more unemployment, substanceuse and suicidal behaviour) that could not bemanaged in the community, hence, were admittedto hospital.
Similarly, focus group input from inpatient hospi-tal staff suggested that patient behaviour influencesdecisions to admit patients to one type of pro-gramme vs. another (Lunsky & Puddicombe 2005):staff from general programmes talked about feelingmore competent to serve higher functioning indi-viduals and reserving referral to more specialisedprogrammes for more vulnerable and difficult indi-viduals who would not be able to participate insome general treatments offered (e.g. group therapysituations) because of limited communication abilityor inappropriate behaviour. Staff also reported thatsome of the clients who could benefit from generalprogrammes preferred such programmes, becausethey do not see themselves as having an ID andwould feel demoralised or doubly stigmatised in aspecialised programme. For such clients, staffrequested access to specialist consultation as neededrather than specialised beds. In the current study,inpatients receiving general services were morelikely to be diagnosed with a substance abuse disor-der and to have a history of suicide attempts thanthose in specialised programmes, suggesting thatthere are numerous issues among individuals withingeneral services that may warrant specialist input.
Significantly more individuals with concurrentsubstance abuse problems were served in generalthan specialised inpatient programmes. Rates ofsubstance abuse diagnoses in the general unitsreported here are similar to rates in other studies ofinpatients in general psychiatry services (Addingtonet al. 1993; Saeed et al. 2003). Unfortunately, sub-stance abuse diagnoses are rarely mentioned instudies describing specialised inpatient unit samples(e.g. Raitasuo et al. 1999; Alexander et al. 2001;
1009Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

Xenitidis et al. 2004). One wonders whether this isbecause specialised programmes are not gearedtowards these individuals or because individualswith ID who abuse substances access mentalhealthcare through a different pathway. Clearlythere is a subgroup of individuals with ID accessingmental health services for which comorbid sub-stance abuse problems is a significant issue.Although level of ID was not available for the inpa-tients in this study, it is likely that the majority ofthe subgroup with substance abuse problems werefunctioning within the mild range and had moreindependence, less supervision and thus, greateraccess to substances. More research is needed onthese individuals (see also Barrett & Paschos 2006;McGillicuddy 2006).
Patients in specialised and general programmesdiffered in terms of their psychiatric diagnosticprofile. In the larger study of hospital patients com-paring those with and without ID (Lunsky et al.2006), the overall rate of psychotic disorder diag-noses was similar in both groups (50%), while therate of mood disorder was significantly higher in thenon-ID group (Non-ID : ID (%) = 37:20). In thisstudy, diagnoses of psychotic disorders were morecommon in ID patients in the general services(Specialised : General (%) = 27:56) and diagnosesof mood disorders were more common among IDpatients in specialist services (Specialised : General(%) = 29:11). While one cannot disentangle differ-ences in diagnostic profiles from differences in diag-nostic practices with the current dataset,independent evidence that non-specialist cliniciansoverdiagnose psychotic disorders in persons with IDis emerging (Myers & Pueschel 1993; Bresch 2004;Hurley et al. 2003). The same symptoms may resultin different diagnoses depending on the expertise ofclinicians, with specialist clinicians, experienced inID and mental health, making fewer diagnoses ofpsychotic disorder (see Lunsky & Bradley 2007 forfurther discussion) than other clinicians. Furtherresearch is required where individuals in both typesof programmes are assessed using assessment anddiagnostic approaches standardised on the popula-tion with ID and administered by clinicians trainedin these approaches and blind to the programmetype.
Using the CAP methodology provided an oppor-tunity to assess the appropriateness of inpatient ter-
tiary care for both groups. The bulk of patients inboth programme types were assessed as requiringLevels 3 and 4 care, but only 10% were rated asrequiring the inpatient care they were receiving(Level 5) despite the mean number of days in hos-pital being greater than 5 years. Problems discharg-ing long-term patients is an acknowledged problemin the Ontario system (Lewis 2004) and is serious,as it means that specialised units cannot admit thecomplex patients they were designed to serve (seealso Morgan & Lowin 1989; Watts et al. 2000;Mackenzie-Davies & Mansell 2007).
Discharge problems are due in part to a lack ofappropriate community residential placements.TheOntario government has recently prioritised special-ised community-based accommodation for individu-als, such as these currently in hospital but ready fordischarge (Ministry of Community and Social Ser-vices, 2006). A follow-up project at the hospitalssince this initiative could assess whether the changeshave resulted in shorter lengths of stay overall, andmore admitted individuals receiving Level 5 recom-mended level of care ratings. A second barrier todischarge is a shortage of community based nursesand physicians trained to work with this population(Lunsky & Bradley 2001; McCreary 2002; Lunsky &Puddicombe 2005; Summers et al. 2005). Currently,the challenge of discharging inpatients to appropri-ate community programmes is a challenge for bothgeneral and specialised inpatient services and islikely to remain so in the absence of adequate clini-cal expertise in community settings.
Future research should examine the pathway tospecialised services prospectively with a cohort ofindividuals with ID and mental health issues todetermine clinical predictors (e.g. severity of symp-toms) and systemic predictors (e.g. already receiv-ing services for people with ID) of specialised care.Future studies evaluating such specialist servicescould further disentangle the components of whatconstitutes ‘specialist’ as opposed to ‘segregated’services. This could be achieved by careful examina-tion of the supports, expertise, vision, value base,etc. within such services and from this, identifywhat structures are needed to integrate these ‘spe-cialist’ components into mainstream services (e.g.Green Light Toolkit, Department of Health, 2004).Such examination will ultimately empower personswith ID in their desire and their legitimate human
1010Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

rights for full inclusion into mainstream mentalhealth services.
Acknowledgements
This research was supported by an Ontario MentalHealth Foundation New Investigator Award. Theauthors also wish to acknowledge Carolyn Graceyfor her assistance in preparation of this manuscript.
References
Addington D., Addington J. & Ens I. (1993) Mentallyretarded patients on general hospital psychiatric units.Canadian Journal of Psychiatry 38, 134–6.
Alexander R. T., Piachaud J. & Singh I. (2001) Two dis-tricts, two models: in-patient care in the psychiatry oflearning disability. The British Journal Developmental Dis-abilities 47, 105–10.
Ashaye O., Mathew G. & Dhadphale M. (1997) A com-parison of older longstay psychiatric and learning dis-ability inpatients using the health of the nation outcomescales. International Journal of Geriatric Psychiatry 12,548–52.
Barrett N. & Paschos D. (2006) Alcohol-related problemsin adolescents and adults with intellectual disabilities.Current Opinion in Psychiatry 19, 481–5.
Bresch D. (2004) Problems and questions in the dual diag-nosis of schizophrenia and intellectual disability. MentalHealth Aspects of Developmental Disabilities 7, 81–90.
Burge P., Ouellette-Kuntz H., Saeed H., McCreary B.,Paquette D. & Sim F. (2002) Acute psychiatric inpa-tient care for people with a dual diagnosis: patient pro-files and lengths of stay. Canadian Journal of Psychiatry47, 243–9.
Chaplin R. (2004) General psychiatric services for adultswith intellectual disability and mental illness. Journal ofIntellectual Disability Research 48, 1–10.
Charlot L. R. & Beasley J. B. (2005) Specialized inpatientmental health care for people with intellectual disabili-ties. Mental Health Care for People with Intellectual Dis-abilities 8, 100–3.
Coffman J. M. (2004) Assessing the validity of the Colo-rado client assessment record for measurement ofmental health status and outcomes. Poster Presented Atthe 132nd Annual Meeting of the American PublicHealth Association. (November, 2004).
Department of Health (2004) Green light for mental health:how good are your mental health services for people withlearning disabilities? A service improvement toolkit. Avail-able at: http://www.valuingpeople.gov.uk/documents/MentalHealthGLGuide.pdf (retrieved 15 July2004).
Durbin J., Cochrane J., Goering P. & Macfarlane D.(2001) Needs-based planning: an evaluation of a level-of-care planning model. The Journal of Behavioral HealthServices & Research 28, 68–80.
Ellis R. J., Wackwitz J. H. & Foster M. (1991) Uses of anempirically derived client typology based on level offunctioning: twelve years of the CCAR. Journal ofMental Health Administration 18, 88–100.
Ellis R., Wilson N. & Foster F. (1984) State wide treat-ment outcome assessment in Colorado: the Coloradoclient assessment record. Community Mental HealthJournal 20, 72–89.
Hall I., Parkes C., Samuels S. & Hassiotis A. (2006)Working across boundaries: clinical outcomes for anintegrated mental health service for people with intellec-tual disabilities. Journal of Intellectual Disabilities 50, 598–607.
Holt G., Costello H., Bouras N., Diareme S., Hillery H.,Moss S. et al. (2000) BIOMED-MEROPE Project:service provision for adults with mental retardation: aEuropean comparison. Journal Intellectual DisabilityResearch 44, 685–96.
Hurley A., Folstein M. & Lam N. (2003) Patients withand without intellectual disability seeking outpatientpsychiatric services: diagnoses and prescribing patterns.Journal Intellectual Disability Research 47, 39–50.
Kwok H. W. M. (2001) Development of a specialized psy-chiatric service for people with learning disabilities andmental health problems: report of a project from KwaiChung Hospital, Hong Kong. British Journal of LearningDisabilities 29, 22–5.
Lewis C. (2004) Ombudsman’s message. 2003–2004 AnnualReport. Ombudsman Ontario. Available at: http://www.ombudsman.on.ca/annrep0304/message.html(retrieved 20 August 2004).
Lunsky Y. & Bradley E. (2001) Developmental disabilitytraining in Canadian psychiatry residency programs.Canadian Journal of Psychiatry 46, 138–46.
Lunsky Y. & Bradley E. (2007) Dual diagnosis or dualconfusion: Limitations when utilizing non-specialistclinical data. Journal on Developmental Disabilities 13,185–90.
Lunsky Y. & Puddicombe J. (2005) Dual Diagnosis inOntario’s Specialty (Psychiatric) Hospitals: QualitativeFindings and Recommendations (Phase II SummaryReport). Centre for Addiction and Mental Health,Toronto, ON. Available at: http://www.camh.net/Care_Treatment/Program_Descriptions/Mental_Health_Programs/Dual_Diagnosis/dual_diagnosis_ontpsyhos_ph2dec05.pdf. (retrieved 7
January 2005).
Lunsky Y., Bradley E., Durbin J., Koegl C., Canrinus M.& Goering P. (2003) Dual Diagnosis in Provincial Psychi-atric Hospitals: A Population Based Study. Centre forAddiction and Mental Health, Toronto, ON. Availableat: http://www.camh.net/Publications/Resources_
1011Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd

for_Professionals/dualdiagnosis_provpsychhosp_1styr2003.pdf (retrieved 8 July 2003).
Lunsky Y., Bradley E., Durbin J., Koegl C., Canrinus M.& Goering P. (2006) The clinical profile and serviceneeds of hospitalized adults with mental retardationand a psychiatric diagnosis. Psychiatric Services 57, 77–83.
McCreary B. (2002) Developmental disabilities: still thecinderella of Canadian psychiatry. Symposium con-ducted at the meeting of the State of the HART: Habili-tative Achievements in Research in DevelopmentalDisabilities, Vancouver, British Columbia.
McGillicuddy N. B. (2006) A review of substance useresearch among those with mental retardation. MentalRetardation and Developmental Disabilities ResearchReviews 12, 41–7.
Mackenzie-Davies N. & Mansell J. (2007) Assessment andtreatment units for people with intellectual disabilitiesand challenging behaviour in England: an exploratorysurvey. Journal Intellectual Disability Research 51, 802–11.
Ministry of Community and Social Services (2006) Oppor-tunities and Action:Transforming Supports in Ontario forPeopleWho Have a Developmental Disability. Queen’sPrinter for Ontario, Toronto.
Morgan D. & Lowin A. (1989) A Study of Dually Diag-nosed Psychiatric Inpatients: Adults with DevelopmentalDisabilitiesWhoWere Also Psychiatric Inpatients at State orCommunity Hospitals. Washington State Department ofSocial and Health Services, Olympia, WA.
Morris S. (2005) Specialized mental health units inOntario: their history and program characteristics.Mental Health Aspects of Developmental Disabilities 8,69–76.
Myers B. & Pueschel S. (1993) Differentiating schizophre-nia from other mental and behavioural disorders inpersons with developmental disabilities. The HabilitativeMental Healthcare Newsletter 12, 93–8.
Ontario Ministries of Health and Community and SocialServices (1997) Policy guideline for the provision of servicesfor persons with a dual diagnosis (developmental disability/mental health needs). Available at: http://www.psychiatry.med.uwo.ca/ddp/resources/dualdiagnosis/policyguideline.htm (retrieved 25 August 1997).
Raitasuo S., Taiminen T. & Solokangas R. K. (1999)Characteristics of people with intellectual disability
admitted for psychiatric inpatient treatment. Journal ofIntellectual Disability Research 43, 112–8.
Reid A. H. (1995) Psychiatric services for people withlearning disabilities: specialist knowledge and servicesare needed. British Medical Journal 310, 1549–50.
Saeed H., Ouellette-Kuntz H., Stuart H. & Burge P.(2003) Length of stay for psychiatric inpatient services:A comparison of admissions of people with and withoutdevelopmental disabilities. The Journal of BehaviouralHealth Services and Research 30, 406–17.
Schwartz R. C. (1999) Reliability and validity of the func-tional assessment rating scale. Psychological Reports 84,389–91.
Smiley E., Cooper S. A., Miller S. M., Robertson P. &Simpson N. (2002) Specialist health services for peoplewith intellectual disability in Scotland. Journal of Intellec-tual Disability Research 46, 585–93.
SPSS Inc. (2005) SPSS Base 14.0 for Windows. SPSSInc., Chicago, IL.
Summers J., Adamson J., Bradley E., Boyd K., Collins S.,Levinson A. et al. (2005) The need for more communitynursing for adults with intellectual disabilities andmental health problems. Canadian Journal of Psychiatry50, 187.
Tajuddin M., Nadkarni S., Biswas A., Watson J.M. &Bhaumik S. (2004) A study of the use of an acute inpa-tient unit for adults with learning disability and mentalhealth problems in Leicestershire, UK. The BritishJournal of Developmental Disabilities 50, 59–68.
Watts R., Richold P. & Berney T. (2000) Delay in the dis-charge of psychiatric in-patients with learning disabili-ties. Psychiatric Bulletin 24, 179–81.
Xenitidis K., Gratsa A., Bouras N., Hammond R., Ditch-field H., Holt G. et al. (2004) Psychiatric inpatient carefor adults with intellectual disabilities: generic or spe-cialist units? Journal of Intellectual Disability Research 48,11–8.
Xenitidis K., Henry J., Russell A. J., Ward A. & MurphyD. G. (1999) An inpatient treatment model for adultswith mild intellectual disability and challenging behav-iour. Journal of Intellectual Disability Research 43, 128–34.
Accepted 13 February 2008
1012Journal of Intellectual Disability Research volume 52 part 11 november 2008
Y. Lunsky et al. • A comparison of patients with intellectual disability
© 2008 The Authors. Journal Compilation © 2008 Blackwell Publishing Ltd