Upload
others
View
1
Download
0
Embed Size (px)
Citation preview
Copyrig
Ventevogel et al.
An Intervention Special IssueIntegrating mental health care intoexisting systems of health care:during and after complexhumanitarian emergencies
PeterVentevogel, Pau Pe¤ rez-Sales, Alberto Fe¤ rnandez-Liria & FlorenceBaingana
Complex humanitarian emergencies, whetherarising from armed con£ict or natural disaster,challenge the mental health system of a country inmany ways. Not least because they increase therisk ofmental disorder in the population, and under-mine the pre-existing structures of care.They may,however, also bring new opportunities to createchange. In this way, new structures and paradigmsmay emerge from the midst of a crisis. Theprobabilities for such a change to occur vary fromone setting to another. Regardless, it has been seenthat interventions in complex humanitarian emer-gencies should not be limited to the deploymentof specialised resources that will disappear oncethe emergency has lost its urgency, or visibility.Apart from provision ofdirect services, interventionsin these circumstances should also aim to buildlocal capacity and install sustainable systems ofmental health care at the time of the intervention.This paper serves as an introduction to this specialissue of ‘Intervention’ and examines the variousaspects surrounding integration of mental healthcare and psychosocial support into overall healthsystems during, or after, complex humanitarianemergencies.
Keywords: capacity building, complexhumanitarian emergencies, documentation,mental health care, sustainability
ht © War Trauma Foundation. Unautho
Complex humanitarianemergencies: contextA disaster is the result of a vast ecologicalbreakdown between a population and theenvironment, on such a vast scale that thedemands exceed available resources (Gunn,2003). The disaster situation overwhelmsthe response capacity of the a¡ected com-munity and causes disruption and disinteg-ration of the social fabric by prohibitingthe survivors from functioning normally(Pe¤ rez-Sales, 2004). Traditionally, disastersare categorised as either natural disasters(such as earthquakes or £oods) or man-made disasters (such as technologicaldisasters, environmental disasters, terroristacts, armed con£icts or refugee crises). How-ever, this historical dichotomy is losing itsutility. For example, the impact of ‘natural’disasters is often compounded when occur-ring in already fragile ecological or politicalcontexts, while armed con£icts and massivedisplacements are, in turn, fuelled by eco-logical factors such as population pressure,and struggles for control over scarce naturalresources such as fertile land and water.Many disasters do not have a single cause.The 2010 earthquake in Haiti occurred in acontext characterised by social inequalities,
rized reproduction of this article is prohibited.195
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
grossly ine⁄cient public services and illprepared physical infrastructures. As aresult, the earthquake had a much moredevastating impact than it would have hadin a politically stable, high income countrywith fully functional public services. Forthese situations, the term complex humani-tarian emergency was coined, speci¢cally todescribe settings in which multiple, oftenhistorically and politically determined,aetiological factors both predispose an areato disaster, and mitigate its outcomes.Complex humanitarian emergencies areoften characterised by factors such as:dislocation of populations, destruction ofsocial networks and ecosystems, insecuritya¡ecting civilians and others not engagedin ¢ghting, and abuses of human rights(Leaning, Briggs, & Chen, 1999). In suchmultidimensional disasters, natural andman-made factors are closely intertwined.High levels of violence and social insecurity,in particular, threaten the capacity of thepopulation to sustain livelihood and life(Zwi & Ugalde,1991).
Complex humanitarianemergencies: three phases ofassistanceThe conventional classi¢cation for thesequence of humanitarian assistance usesthree phases: relief, rehabilitation anddevelopment. Activities included in therelief phase aim to provide essential servicesto those whose survival is threatened. Thisphase is followed by rehabilitation, in whichbasic services such as schools, health care,andwater supply are restored, and damagedinfrastructure is rebuilt. Finally, the assist-ance can focus onbroader goals, such as eco-nomic growth, improving living standardsand creation of wealth and social capital(Ryscavage, 2003). While this relief^rehabilitation^development continuum is
ht © War Trauma Foundation. Unautho196
meant to organise the post disaster responsein a logical way, there are fundamental£awswith it in complex humanitarian emer-gencies. For example, this continuum tendsto obscure the social, macro-economic andenvironmental factors contributing to thedisaster in these settings, and it may serveto legitimate restoration of a socially andmorally unjust, fragile status quo.Documents that provide consensus frame-works to guide humanitarian responsesafter disasters, emphasise community basedapproaches and the need to reinforce theresponses of the local population (IASC,2007; The Sphere Project, 2011). Typically,these frameworks limit their scope to theresponses occurring in themidst ofan emergency,generally the ¢rst months after a disaster.Within one to two years after an emergency,many organisations have ended theirprogrammes and moved to new emergencysettings. The changing nature of humani-tarian emergencies, however, from shortterm emergencies in con¢ned areas to pro-longed emergencies in large geographicalareas, need a di¡erent approach, withdue attention given to capacity buildingof national sta¡ and public institutions(Salama et al., 2004). In this post disasterphase, the need for new leaders and uncon-ventional approaches may arise. This cancall into question the status quo of ‘how thingswere always done’, and may lead to rethinkingand rede¢ning public service delivery.The in£ux of local and foreign quali¢edprofessionals, and the provision of aidfunds, can provide additional factors tocreate opportunities for change, if theopportunities are seized at the rightmoment. This requires the use of long termperspectives that go beyond immediateservices delivery, and aim to restore andrestructure the systems that provide theseservices (deJong, 2002).
rized reproduction of this article is prohibited.
Copyrig
Ventevogel et al.
Mental health and psychosocialsupport in complexhumanitarian emergenciesAttention to mental health and psychosocialsupport (MHPSS) in the aftermath ofdisasters is relatively new, and has led to¢erce and often polarised debates aboutwhat kind of mental health care and psycho-social support needs to be organised (Ager,Strang & Wessells, 2006; Galappatti, 2003;van Ommeren, Morris, & Saxena, 2006;Williamson & Robinson, 2006). The widelydiverging views among MHPSS prac-titioners working in complex humanitarianemergencies contributed heavily to poorcoordination across approaches, resultingin fragmented services and a lack of com-prehensive support. The wide range ofopinions about what should be done ispartly related to the absence of a solid baseof evidence on the results of MHPSS inter-ventions in complex humanitarian emer-gencies (Wessells & van Ommeren, 2008).The need to create such an evidence base isobvious (Tol et al., 2011), yet too often, inter-vention strategies are employed where thee¡ectiveness is not at all clear. It is also, asyet, unclear how emergency MHPSS maycontribute to lasting mental health reformsin the post disaster/post con£ict phases,and whether the e¡orts during emergenciesactually do lead to an improved mentalhealth care delivery for the population (All-den et al., 2009). MHPSS service providersin complex humanitarian emergencies canlearn from experiences elsewhere in thedeveloping world, and, in turn, may providedata that are useful for the emerging globalmental health movement.
Mental health, an emergingglobal priorityMental health is becoming a globalhealth priority because of the relative high
ht © War Trauma Foundation. Unautho
prevalence of mental disorders and theassociated disability (Prince et al., 2007).Among the most prevalent mental disordersare: depression, schizophrenia and alcoholor drug abuse disorders (World HealthOrganization, 2005).While non-communic-able diseases, including mental disorders,already pose a substantial global economicburden, this burden is expected to rise morethan double in the next two decades.Withinthis group of noncommunicable disorders,the most important contributors to theglobal economic burden are mental healthconditions and cardiovascular disease(Bloom et al., 2011). In low income countries,the resources for mental health care arevery limited, typically less than 1% of analready low health care budget (Saxenaet al., 2007). Although there has been alobby to promote mental health care in thedevelopment agenda in low incomecountries, there are also major challengesabout how to integrate mental health careinto health sector reform plans. Some ofthese challenges include: engaging mentalhealth professionals in general health sectorreforms; strengthening the links betweenmental health and social development; andintensifying resource mobilisation (Jenkinset al., 2010). One key to improving mentalhealth in communities is to look beyondnarrowly de¢ned health care systems.Treat-ment of mental disorders requires more thanjust individual therapies for the su¡erers.They should also foster the inclusion of men-tal health interventions into general healthsystems, thereby strengthening policies(Jenkins et al., 2011), as well as foster integ-ration of mental health aspects in generalsocial policies to improve the wellbeing ofthe population (Friedli, 2009). A recentconsensus seeking exercise among hundredsof researchers, advocates and clinicians,identi¢ed themost urgent research priorities
rized reproduction of this article is prohibited.197
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
for improving the lives of people withmental illness around the world. The ¢vemost important areas to be researched arerelated to:1) strengthening themental healthcomponent in the training of all health carepersonnel, 2) integrating screening and corepackages of services into routine primaryhealth care,3) reducing the cost and improv-ing the supply of e¡ective medications, 4)providing e¡ective and a¡ordable com-munity based care and rehabilitation,and 5) improving children’s access to evi-dence based careby trained health providersin low andmiddle income countries (Collinset al., 2011).One of the main strategies to improveaccess of the population to mental healthservices is to integrate such services withinthe general health care system, and to avoidstand-alone systems based on specialisedpsychiatric hospitals. Integrating mentalhealth services into primary health care(PHC) is often considered the most viableway of ensuring that people get the mentalhealth care they need (World HealthOrganization & Wonca, 2008). Primaryhealth care is de¢ned as the ¢rst level ofhealth system contact with the population.It includes various aspects, such as: healthpromotion, prevention, care for commonillnesses, and management of on-goingchronic health problems. Primary healthservices act as the principal point of consul-tation for patients within a health caresystem, and depending on the conditions ofthe system in the area, and the type ofstructure, it can be carried out by a doctor,nurse, midwife, community health worker,traditional healer, or members of the groupor the community. There is no single bestpractice model for the integration of mentalhealth care into PHC that ¢ts all contexts.In documenting 11 examples of successfulintegration of mental health care into
ht © War Trauma Foundation. Unautho198
primary care, only one country, Uganda,was a post con£ict or post emergencysetting (World Health Organization &Wonca, 2008). Among the basic require-ments to make the integration a success areelements such as adapting mental healthpolicies, ensuring that primary care workersare adequately trained, organisingappropri-ate supervision, ensuring that primary careworkers are not burdened with unrealisticamounts of tasks, and making specialistmental health care professionals andfacilities available to support primary care.One important practical lessonwas the needto collaborate with other government nonhealth sectors, nongovernmental organis-ations (NGOs) and community networks.The World Health Organization haslaunched the comprehensive mental healthGap Action Programme (mhGAP) toaddress this lack of care, especially in lowand middle income countries, for peoplesu¡ering from mental, neurological andsubstance use disorders. This includes anintervention guide with evidence basedmental health interventions for generalhealth workers (World Health Organiz-ation, 2010). There is now an urgent needto use these available tools on a largerscale, and to document what we canlearn from the process to scale up mentalhealth services in low resource settings(Eaton et al., 2011).
A closer look at mental healthinterventions in emergencies:what should be done?There is an important and large gapbetween the rapidly increasing knowledgebase on community mental health care inlow and middle income countries, and themental health and psychosocial work that isactually done in emergencies (Allden et al.,2009). One important challenge in planning
rized reproduction of this article is prohibited.
Copyrig
Ventevogel et al.
mental health services in complex emer-gencies is how to ensure that the servicehas immediate, measurable bene¢ts, whileat the same time building a model that is-sustainable and ultimately integratedwithin the broader primary health service(Silove,2004b).TheWorld Health Organiz-ation advocates strengthening pre-existingmental health services. Particularly afterthe most acute distress has decreased, andthe most basic needs have been addressed,e¡orts should be directed towardsestablishing a more comprehensive rangeof community based mental health inter-ventions, ensuring that 1) people withsevere mental disorders (e.g. psychosis,severe depression) have access to e¡ectivecare in the community, 2) mental healthcare is available within general healthsettings and 3) links to outside the formalhealth sector are established and madefunctional. This last point could include,for example, training and supervisingof social workers, teachers, communityleaders, and, when feasible, and traditionalhealers (van Ommeren, Saraceno, &Saxena,2004).Many papers published on mental healthproblems in humanitarian emergenciesfocus on the prevalence of mental disorders,with a strong emphasis on posttraumaticstress disorder (PTSD) and depression.Reported prevalence ¢gures of depressionand PTSD vary widely between surveysof con£ict a¡ected populations.While thismay be a result of contextual factors,such as the extent of exposure to adversity,they are also strongly a¡ected bymethodological di¡erences (Rodin & vanOmmeren, 2009). Trauma focused surveysare also often unable to identify the e¡ectsof a complex emergency on a population’sability to care for itself (Ager, 2002), or toidentify locally used cultural expressions
ht © War Trauma Foundation. Unautho
on the lack of wellbeing (Miller, Kulkarni,& Kushner, 2006). Prevalence rates ofsevere mental disorders, such as psychosisand bipolar disorder, are largely unknown.A rough estimation is that a humanitariancrisis leads to an increase of the prevalenceof severe mental disorders from 2^3% to3^4% in the ¢rst 12 months, and forcommon mental disorders from anestimated 10% at baseline (pre-crisis) to20% (van Ommeren, Saxena, & Saraceno,2005). In striking contrast to the impressiveamount of scienti¢c papers on prevalence¢gures in complex emergencies, is thedearth of papers describing the outcome ofactual interventions to tackle such pro-blems. The published literature is skewedtowards psychological interventions forPTSD. This emphasis on trauma relatedmental problems is not consistent with thekind of programmes that are usually imple-mented, and for which there is an urgentneed to assess the e¡ectiveness. MHPSSinterventions initiated by external actors,such as international NGOs, frequently arenot well connected to existing systems ofcare. A recent survey of 160 reports of actualinterventions found that the vast majority ofthem took place and were funded outsideexisting systems of care, such as nationalmental health care systems (Tol et al., 2011).A World Bank report in 2005 identi¢edthis lack of systematic documentation ofmental health and psychosocial inter-ventions in post emergency and postcon£ict settings as the major obstacle tomore e¡ective and better targeted interven-tions (Baingana, Bannon, & Thomas, 2005).Others have called for a public discussion onthe results of assessments and evaluations ofmental health activities in complex humani-tarian emergencies, so that lessons canbe learnt for future interventions (Mollicaet al., 2004).
rized reproduction of this article is prohibited.199
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
How trying to help can makethings worse: the example ofSri LankaIn the aftermath of some humanitarianemergencies, the in£ux of organisationsand groups providing all kinds of assistancecan be quite overwhelming. More to thepoint, they may also inadvertently under-mine existing assistance structures, and dis-credit local ways of coping with adversity.This has been poignantly described in posttsunami Sri Lanka, where delivering ofmental health care and psychosocial supportin a¡ected areas was compromised by themassive destruction of infrastructure, anddi⁄culties coordinating responses betweenmany organisations were involved (Ashraf,2005). A Sri Lankan psychiatrist, Ganesan(2006), saw dozens of experts in mentalhealth and psychosocial support being‘parachuted’ in to the east coast of Sri Lankato start a multitude of trauma- focussedactivities, while there was far less attentiongiven to much more urgent social workprojects and programmes to care for thosewith severe mental disorders such as psy-chosis. In his chapter ‘The wave that broughtPTSD to Sri Lanka’, Watters (2010) providesdisconcerting examples of the rather toxiccombination of cultural naivete¤ and thetherapeutic arrogance of many of theseexperts. Humanitarian interventions, suchas mental health training of local sta¡,may amount to the imposition of westernconcepts of distress and disorder, to popu-lations with di¡erent ways of understandinghuman su¡ering (Abramowitz, 2010). More-over, the e¡orts of outsiders to providemental health assistance tends to obscurethe e¡orts by local stakeholders (Fernando,Pedersen, &Weerackody, 2010).There is alsoa risk that NGO programmes take awaymental health professionals from the publicsystem. As Ganesan (2011) mentions in this
ht © War Trauma Foundation. Unautho200
issue, he was the only psychiatrist in theheaviest a¡ected area of Sri Lanka posttsunami, and felt pressured by externalagencies and the media to decrease the timehe spent treating people with severe mentaldisorders, and to favour trauma focusedinterventions of the newly started pro-grammes instead.
How something good may comeout of a disaster: the example ofSri LankaFortunately, there are also good exampleswhere mental health interventions in thesetting of complex humanitarian emer-gencies have had long lasting, positivee¡ects on mental health service delivery.Again, Sri Lanka may serve as an example.The ¢nancial aid generated as a responseto the tsunami boosted the developmentof community centred, and therefore decen-tralised, mental health care in Sri Lanka.For example, in the northern town ofJa¡na, local organisations and authoritiesformed a joint Mental HealthTask Force inthe ¢rst months after the disaster, in orderto coordinate their activities (van der Veen& Somasundaram, 2006). The ad hoc taskforce was later transformed into a formalintrasectoral, coordinating body for localgovernmental and NGOs involved inmental health and psychosocial work, andcontinued to be a driving force for improv-ingMHPSS services in the area (Krishnaku-mar, Sivayokan, & Somasundaram, 2008).Prior to the tsunami, in the north-easternareas of Sri Lanka, there was a long historyof protracted armed con£ict. There, localmental health workers had already startedinnovative mental health services withinsecondary and primary care. The WorldHealth Organization advised using thismodel for other districts in Sri Lanka (Sara-ceno& vanOmmeren,2003). Unfortunately,
rized reproduction of this article is prohibited.
Copyrig
Ventevogel et al.
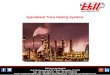
donors were initially uninterested, that isuntil the 2004 Asian tsunami. The suddenavailability of funds for mental health careprompted the development of a nationalmental health policy that encourageddecentralisation of service, and that wasde facto based on the innovative workdeveloped in the con£ict a¡ected areasin the north east (Saraceno, 2005). Theincreased awareness of the importance ofmental health care after the tsunami,prompted the establishment of decentralisedmental health services integrated intogeneral health care, and led to training ofgeneral health workers to provide treatmentfor people with mental health problems inthe tsunami a¡ected areas (Mahoneyet al., 2006). Several years after the tsunami,there are still mental health services inseven tsunami a¡ected districts of SriLanka, run by the Ministry of Health(WHO, 2008). A map of the diversityand spread of mental health servicesshows the improvements quite dramatically(Figure 1).
The importance of documentingexperiencesThe brief examples of Sri Lanka abovemay serve to highlight the importance ofdescribing the process of how interventionsin these settings, often starting with a reliefperspective, can lead to more fundamentalchanges in mental health service delivery.Perhaps there are many experiences ofmental health care being integrated intoexisting systems of care during humani-tarian emergencies, but to our knowledge,they are rarely documented. Edited volumeson mental health in post war and postcon£ict settings pay limited attention toaspects related to the integration of mentalhealth care into existing systems, and focus
ht © War Trauma Foundation. Unautho
instead on the development of NGO basedservices. Or they describe the immediatemental health response without taking alonger term perspective, while in turn,books on mental health care developmentin resource poor settings often do notaddress the speci¢c context of humanitarianemergencies.There are many reports of successful mentalhealth training of general health workersin humanitarian settings (Budosan, 2011;Budosan et al., 2007; Henderson et al.,2006; Mohit et al., 1999; Sadik et al., 2011;Ventevogel & Kortmann, 2004). Thesearticles usually describe how it was feasibleto install basic mental health care skills ingeneral healthworkers. However, we are leftwith the question of what happened after?Some articles describe how attempts tostart primary mental health services withinprimary care proved feasible within theproject period, showing clear increases ofnumbers of patients receiving treatment(Budosan & Jones, 2009; Jones et al., 2007a;Jones et al., 2009; Somasundaram et al.,1999; Souza, Yasuda, & Cristofani, 2009).Yet, most of these publications focus ondirect output (building mental health skillsin sta¡, increasing the number of patientsin treatment) with less attention to a sys-tematic description of how these inter-ventions could contribute to long lastingchanges in public mental health servicesdelivery. It is rare to ¢nd published docu-mentation on how mental health projects,that started in the aftermath of a humani-tarian emergency, moved from a projectwith an initial focus on relieving immediatesu¡ering to long term programmes tostrengthen mental health care services.There are exceptions. In the 1980 s inGuinea-Bissau, then recovering from an18 year long war of independence, a com-munity mental health programme was set
rized reproduction of this article is prohibited.201
Copyright © War Trauma Foundation. Unauthorized reproduction of this article is prohibited.
Exp
ansi
on
of m
enta
l hea
lth
ser
vice
s in
Sri
Lan
ka
2004
- 2
005
2006
- 2
007
2008
- 2
009
2010
- 2
011
Psy
chia
tris
tP
lan
ned
acu
te p
sych
iatr
y u
nit
Ver
y b
asic
men
tal h
ealt
h s
ervi
ces
(clin
ics)
Co
mp
reh
ensi
ve m
enta
l hea
lth
ser
vice
s (e
.g. p
sych
iatr
ist/
Dip
.in P
sych
., ac
ute
un
it, i
nte
rmed
iate
car
e u
nit
,o
utr
each
clin
ics
and
hu
man
res
ou
rces
for
men
tal h
ealt
h)
Bas
ic m
enta
l hea
lth
ser
vice
s (e
.g. p
sych
iatr
ist,
acu
te u
nit
an
d o
utr
each
clin
ics
)In
term
edia
te c
are
un
it
Pla
nn
ed In
term
edia
te c
are
un
it
Lo
ng
sta
y u
nit
Pla
nn
ed a
cute
psy
chia
try
un
it in
pro
gre
ssA
ctin
g c
on
sult
ant
Sen
ior
reg
istr
ars
MO
- d
iplo
ma
in p
sych
itar
y
Acu
te p
sych
iatr
y u
nit
Figure1:
Map
ofSriL
anka
show
ingthe developm
ent ofm
e ntalheal th
servi ces,
2004^2011.(Source:
Ministry ofH
eal th
&Nutr itionandW
orldHeal th
OrganizationSriL
anka.)
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
202
Copyrig
Ventevogel et al.
up to train primary health care workersin mental health, and the evolution of thisprogramme was described for a periodcovering more than a decade (de Jong,1996). InTimor Leste, overwhelmed by thee¡ects of mass violence, displacement anddestruction of infrastructure after its violentcessation from Indonesia in 1999, a mentalhealth care programme with a strongcommunity oriented outlook was describedfor a period covering more than a decade(Silove et al., 2011). In Afghanistan, afterthe fall of the Taliban in 2001, NGO ledmental health projects started with theaim of integrating mental health into exist-ing governmental health care services.Several NGOs and the WHO contributedto curriculum development and advocacyfor the inclusion of mental health intothe Basic Package of Health Services(Ventevogel, Faiz & van Mierlo, 2011).There are however many more complexhumanitarian emergencies in which govern-ments, local organisations and internationalNGO design and implement mental healthprogrammes. Unfortunately, little is knownabout these experiences. For example, inAceh, the emergency programme by aninternational NGO after the 2004 tsunami(Jones et al., 2007) was later taken overby another international NGO with astrong focus on development. The healthauthorities made annual budgetary allo-cation to continue the primary healthcentre based community mental healthservices, but this experience has not yetbeen documented (A. Mohanraj, personalcommunication). Much of the experienceof organisations that actually make thetransition from emergency relief to theadoption and promotion of structuralchanges in service delivery for people withmental disorders, remain undocumented tothis day.
ht © War Trauma Foundation. Unautho
Emergencies: risks andopportunities for strengtheningexisting mental health caresystemsComplex humanitarian emergencies createboth enormous challenges and opportunitiesfor structural improvement of mental healthservices. A discursive reading of the pub-lished literature led us to identify the follow-ing opportunities and challenges for thedevelopment of sustainable mental healthservices, during and after complex humani-tarian emergencies:
Risks
1. C
rize
reating parallel systemsThe breakdown of often already weakand ine⁄cient public services oftenprompts aid organisations to startservices by themselves.While there maynot always be an alternative, the risk isthat unsustainable programmes arecreated, with the result that instead ofsupporting the public system, it mayundermine it. Interventions may focuson one particular type of ‘mentaldisorder’, while ignoring that the spec-trum of mental health problems incomplex emergencies is much broader(Summer¢eld,1999). If separate servicesare started, it is often challengingNGOs to make the transition towardsintegrated, horizontal programming(deJong, 2007).
2. I
nterventions by outsiders may ignore whatpeople do themselvesHumanitarian interventions maysilence, or marginalise, local perspect-ives and local views (Abramowitz &Kleinman, 2008). The acceptable, ordominant form of healing communitiesafter mass upheaval, is expected to comefrom humanitarian aid and this tends toobscure the healing the social wounds of war.d reproduction of this article is prohibited.203
Copyright
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
204
In other words, how communitiesthemselves mobilise their own social,and other resources, in order to recoverin their own time and in their own way(Last, 2000).
3. M
edicalising non pathological distress andsocial problemsTheWorldHealthOrganizationwarnsofthe risk of misapplication of the medicalmodel by general health workers withbasic training in mental health care(van Ommeren et al., 2004). This hasbeen documented as a real problem incomplex humanitarian emergencies,such as Afghanistan (Ventevogel, Faiz,& vanMierlo, 2011).4. O
verburdening general health workers withskills and knowledge they cannot useGeneral health workers in overloadedhealth care facilities have limitedtime for each encounter, and often donot have the time to go deeper intothe presented complaints and thereforemiss mental health disorders thatpresent as physical problems (Afanaet al., 2002).5. P
roviding insu⁄cient supervision andfollowuptrainingSystematic supervision and training,preferably attached to existing institu-tions, is an essential ingredient ofcapacity building, but may also be givenlimited attention in practice (Silove,2004a).Many of these risks are not speci¢c to thesituation of complex humanitarian emer-gencies, but may become more pronouncedand urgent in such emergencies. Similarly,the unusual context of complex humani-tarian emergencies can also provide oppor-tunities that, again, may not be speci¢cfor these contexts, but may be morepronounced.
© War Trauma Foundation. Unautho
Opportunities
1. I
riz
ncreased funding opportunitiesSome complex humanitarian emergen-cies, particularly those involving acutenatural disasters such as earthquakes ortsunamis, may generate many millionsof dollars in emergency relief. This isusually distributed by multilateralagencies and foreign governments, andtranslated into short term projects byinternationalNGOs.The unprecedentedamount of funding, in an otherwisedisadvantaged or marginalised region,can provide opportunities to start newinitiatives that boost mental health care.
2. P
ossibilities to involve di¡erent categories ofhealth workers in mental health activitiesThemassiveneedsarising inemergenciesmay lead health authorities to acceptpiloting new initiatives formental healthcare provision, including the training ofgeneral health workers, the use of para-medical sta¡ and working closely withcommunities. Mental health care shouldbe linked with other sectors, outside thehealth care system in order to becomee¡ective on a community level (WorldHealth Organization, 2003). Perhaps themost powerful interventions to improvethe mental health status of people inimpoverished circumstances are outsidethe formal health sector. Interventionsdealing with mental health can playan important role in e¡ective postcon£ict reconciliation and reconstruc-tion (Baingana, Bannon, & Thomas,2005). The in£ux of organisations withcommunity focused orientations maymake help to improve such inter-sectorallinks.3. I
ncluding mental health care in health sectorreformsMental health care should not beisolated from other parts of health care.ed reproduction of this article is prohibited.
Copyright ©
Ventevogel et al.
It needs to be linked with other, moregeneral approaches to strengthen thehealth care sector, including aspects suchas general health sector reform andresults based ¢nancing. Emergenciesoften lead to health sector reforms, andin several post con£ict settings, such asAfghanistan, Somalia and Liberia, thishas led to the incorporation of mentalhealth into minimum packages of care(Ventevogel et al., 2002). Health policymakers are also more likely to acceptand implement mental health carereforms (Munir et al., 2004; PanduSetiawan & Viora, 2006)
This Special Issue of Intervention documentsa variety of examples from mental healthprogrammes in the aftermath of naturaldisasters and armed con£ict. Some of themain lessons learned are described in theclosing article of this issue (Pe¤ rez-Saleset al., 2011). We hope it will contribute tobuilding an evidence base for integratingmental health care into existing systems ofhealth care, in complex humanitarianemergencies.
AcknowledgementsThe authors would like to thank Julian Eaton,
Ananda Galappatti, Andrew Mohanraj and
Mark van Ommeren for their comments on
earlier versions of this paper.
ReferencesAbramowitz, S. &Kleinman, A. (2008). Humani-
tarian intervention and cultural translation:
a review of the IASC Guidelines on Mental
Health and Psychosocial Support in Emer-
gency Settings. Intervention, 6(3/4), 219-227.
Abramowitz, S. A. (2010). Trauma and humani-
tarian translation in Liberia: the tale of open
mole.Culture,Medicine&Psychiatry, 34,353-379.
War Trauma Foundation. Unautho
Afana, AH., Dalgard, OS., Bjertness, E. &
Grunfeld, B. (2002). The ability of general
practitioners to detect mental disorders
among primary care patients in a stressful
environment: Gaza Strip. Journal of PublicHealthMedicine, 24(4), 326-331.
Ager, A. (2002). Psychosocial needs in complex
emergencies. Lancet, 360(Suppl), s43-s44.
Ager, A., Strang, A. & Wessells, M. (2006).
Integrating psychosocial issues in humani-
tariananddevelopment assistance:A response
to Williamson and Robinson. Intervention, 4,29-31.
Allden,K., Jones, L.,Weissbecker, I.,Wessells,M.,
Bolton, P., Betancourt, TS. & Sumathipala,
A. (2009). Mental health and psychosocial
support in crisis and con£ict: report of the
mental health working group. Prehospital &DisasterMedicine, 24(Suppl 2), s217-s227.
Ashraf, H. (2005).Tsunami wreaks mental health
havoc. BulletinWorld Health Organization, 83(6),405-406.
Baingana, F., Bannon, I. & Thomas, R. (2005).
Mental health and con£icts. Conceptual Frameworkand Approaches.Washington, DC:World Bank.
Bloom, DE., Ca¢ero, ET., Jane¤ -Llopis, E.,
Abrahams-Gessel, S., Bloom, LR., Fathima,
S. & Weinstein, C. (2011).The Global EconomicBurden of Non-communicable Diseases. Geneva:World Economic Forum.
Budosan, B. (2011). Mental health training of
primaryhealthcareworkers: case reports from
Sri Lanka, Pakistan and Jordan. Intervention,9(2),125-136.
Budosan, B., & Jones, L. (2009). Evaluation of
e¡ectiveness of mental health training
rized reproduction of this article is prohibited.205
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
program for primary health care sta¡ in
HambantotaDistrict, SriLankapost-tsunami.
Journal of Humanitarian Assistance (May 2009).Retrieved from http://sites.tufts.edu/jha/
archives/509
Budosan, B., Jones, L.,Wickramasinghe,W. A. L.,
Farook, A. L., Edirisooriya,V., Abeywardena,
G., & Nowfel, M. J. (2007). After the Wave: APilot Project to Develop Mental Health Servicesin Ampara District, Sri Lanka Post-Tsunami.(September 2007). Retrieved from http://sites.
tufts.edu/jha/archives/53
Collins, P.Y., Patel,V., Joestl, S. S., March, D.,
Insel, T. R. & Daar, A. S. (2011). Grand
challenges in global mental health. Nature,475, 27-30.
de Jong, J. (2007). Nongovernmental organiza-
tions and the role of the mental health
professional. In R. J. Ursano, C. S. Fullerton,
L. Weisaeth & B. Raphael (Eds.),Textbook ofDisaster Psychiatry (pp. 206^224). Cambridge:Cambridge University Press.
de Jong, J. (Ed.). (2002).Trauma, war, and violence:Public mental health in socio-cultural context.NewYork, NY: KluwerAcademic /Plenum.
de Jong, JT (1996). A comprehensive public mental
health programme in Guinea-Bissau: a useful
model for African, Asian and Latin-American
countries. PsychologicalMedicine, 26(1),97-108.
Eaton, J., McCay, L., Semrau,M., Chatterjee, S.,
Baingana, F., Araya, R. & Saxena, S. (2011).
Scale up of services for mental health in low-
income and middle-income countries. Lancet,in press.
Fernando, S., Pedersen, D., & Weerackody, C.
(2010). Mental health in Sri Lanka. Lancet,376(9735), 89.
ht © War Trauma Foundation. Unautho206
Friedli, L. (2009). Mental health, resilience andinequalities. Copenhagen: World HealthOrganization, Regional O⁄ce for Europe.
Galappatti, A. (2003). What is a Psychosocial
Intervention?Mapping theField in SriLanka.
Intervention, 1(2), 3-17.
Ganesan, M. (2006). Psychosocial response to
disasters^some concerns. International Reviewof Psychiatry, 18(3), 241-247.
Ganesan, M. (2011). Building up mental health
services from scratch: experiences from
East Sri Lanka. Intervention, 9(3),This issue.
Gunn, S.W.A. (2003).The language of disasters: a
brief terminology of disaster management
and humanitarian action. In K. M. Cahill
(Ed.), Basics of International humanitarianmissions (pp. 35^46). New York: FordhamUniversity Press and Centre for International
Health and Cooperation.
Henderson, DC.,Mollica, RF.,Tor, S., Lavelle, J.,
Culhane, MA. &Hayden, D. (2006). Building
Primary Care Practitioners’ Attitudes and
Con¢dence in Mental Health Skills in a Post-
Con£ict Society: A Cambodian Example.
Journal of Nervous and Mental Disease, 193, 551-559.
IASC. (2007). IASC Guidelines on Mental Healthand Psychosocial Support in Emergency Settings.Geneva: Inter-Agency Standing Committee.
Jenkins,R.,Baingana,F.,Ahmad,R.,McDaid,D.
& Atun, R. (2011). How can mental health be
integrated into health system strengthening?
[Editorial].Mental Health in Family Medicine, 8,115-117.
Jenkins, R., Baingana, F., Belkin, G., Borowitz,
M., Daly, A., Francis, P. & Sadiq, S. (2010).
rized reproduction of this article is prohibited.
http://sites.tufts.edu/jha/archives/509http://sites.tufts.edu/jha/archives/509http://sites.tufts.edu/jha/archives/53http://sites.tufts.edu/jha/archives/53
Copyrig
Ventevogel et al.
Mental health and the development agenda
in Sub-Saharan Africa. Psychiatric Services,61(3), 229-234.
Jones, L., Asare, J., Elmasri, M. & Mohanraj, A.
(2007a). Mental health in disaster settings.
[Editorial]. BMJ, 335(7622), 679-680.
Jones, L., Asare, J. B., El Masri, M., Mohanraj,
A., Sherief, H. & van Ommeren, M. (2009).
Severe mental disorders in complex emergen-
cies. Lancet, 374(9690), 654-661.
Jones, L. M., Ghani, H. A., Mohanraj, A.,
Morrison, S., Smith, P., Stube, D., & Asare, J.
(2007). Crisis into opportunity: setting up
community mental health services in post-
tsunami Aceh. Asia-Paci¢c Journal of PublicHealth, 19 Spec No, 60-68.
Krishnakumar, G., Sivayokan, S. & Somasun-
daram, D. (2008). Coordination of psycho-
social activities at the Ja¡na District level in
Sri Lanka. Intervention, 6(3^4), 270-274.
Last, M. (2000). Healing the social wounds
of war. Medicine. Con£ict & Survival, 16, 370-382.
Leaning, J., Briggs, S. M., & Chen, L. C. (Eds.).
(1999). Humanitarian Crises: The Medical andPublic Health Response. Boston: HarvardUniversity Press.
Mahoney, J., Chandra, V., Gambheera, H., De
Silva,T. & Suveendran,T. (2006). Responding
to the mental health and psychosocial
needs of the people of Sri Lanka in disasters.
International Review of Psychiatry, 18, 593-597.
Miller, KE., Kulkarni, M. &Kushner, H. (2006).
Beyond Trauma-Focused Psychiatric Epide-
miology: bridging research and practice with
ht © War Trauma Foundation. Unautho
war-a¡ected populations. American Journal ofOrthopsychiatry, 76(4), 409-422.
Mohit, A., Saeed, K., Shahmohammadi, D.,
Bolhari, J., Bina,M., Gater, R. &Mubbashar,
M. (1999). Mental health manpower develop-
ment in Afghanistan: a report on a training
course for primary health care physicians.
EasternMediterraen HealthJournal, 5(2), 373-377.
Mollica, RF., Cardozo, BL., Osofsky, HJ.,
Raphael, B., Ager, A. & Salama, P. (2004).
Mental health in complex emergencies.
Lancet, 365(9462), 842-843.
Munir, K., Ergene, T., Tunaligil, V. & Erol, N.
(2004). A window of opportunity for the
transformation of national mental health
policy in Turkey following two major earth-
quakes. Harvard Review of Psychiatry, 12(4), 238/251.
Pandu Setiawan, G. & Viora, E. (2006). Disaster
mental healthpreparedness plan in Indonesia.
International Review of Psychiatry, 18(6), 563-566.
Pe¤ rez-Sales, P. (2004). Mental health in disasters:
the psychosocial approach. In T. Baubet, K.
Le Rouch, D. Bitar & M. Moro (Eds.),
Soigner malgre¤ tout.Trauma, cultures et soins Paris:Pense¤ e Sauvage.
Pe¤ rez-Sales, P., Fe¤ rnandez-Liria, A., Baingana, F.,
& Ventevogel, P. (2011). Integrating mental
health into existing systems of care during
and after complex humanitarian emergencies:
Rethinking the experience. Intervention, 9,this issue.
Prince, M., Patel, V., Saxena, S., Maj, M.,
Maselko, J., Phillips, MR. & Rahman, A.
(2007). No health without mental health.
Lancet, 370(9590), 859-877.
rized reproduction of this article is prohibited.207
Copyrig
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
Rodin, D. & vanOmmeren,M. (2009). Commen-
tary: explaining enormous variations in rates
of disorder in trauma-focused psychiatric
epidemiology after major emergencies.
InternationalJournal of Epidemiology, 38(4),1045-1048.
Ryscavage, R. (2003). The transition from
con£ict to peace. In K. M. Cahill (Ed.),
Emergency relief operations (pp. 284^294).New York: Fordham University Press
/Center for International Health and
Cooperation.
Sadik, S., Abdulrahman, S., Bradley, M. &
Jenkins, R. (2011). Integrating mental health
into primary health care in Iraq.MentalHealthin FamilyMedicine, 8, 39-49.
Salama, P., Spiegel, P.,Talley, L. &Waldman, R.
(2004). Lessons learned from complex emer-
gencies over past decade. Lancet, 364(9447),1801-1813.
Saraceno, B. & vanOmmeren,M. (2003). Five yearmental health planfor northeast Sri Lanka. Geneva,World Health Organization, Department of
Mental Health and Substance Dependence
(Unpublished report).
Saraceno, B. (2005). The WHO’s mental health
response to theAsian tsunami.World Psychiatry,4(2), 66-67.
Saxena, S.,Thornicroft, G., Knapp,M. &White-
ford, H. (2007). Resources for mental health:
scarcity, inequity, and ine⁄ciency. Lancet, 370,878-889.
Silove, D. (2004a). The challenges facing mental
health programs for post-con£ict and refugee
communities. Prehospital & Disaster Medicine,19(1), 90-96.
ht © War Trauma Foundation. Unautho208
Silove, D. (2004b). Considerations in Planning
Mental Health Services in Con£ict-A¡ected
Countries in the Developing World In R. F.
Mollica, R. Guerra, R. Bhasin & J. Lavelle
(Eds.), Book of best practices.Trauma and the role ofmental health in post-con£ict recover. (pp. 124^152).Retrieved fromhttp://siteresources.world
bank.org/DISABILITY/Resources/280658-
1172610662358/Proj1Billion.pdf.
Silove, D., Rees, S.,Tam, N., Liddell, B. & Zwi, A.
(2011). Sta¡ management and capacity build-
ingunderconditionsof insecurity: lessons from
developingmental health service and research
programs in post-con£ict Timor-Leste.
Australasian Psychiatry, 19(Suppl 1), S90-S94.
Somasundaram, DJ., van de Put, WA.,
Eisenbruch,M. & deJong, JT. (1999). Starting
mental health services in Cambodia. SocialScience&Medicine, 48(8),1029-1046.
Souza, R., Yasuda, S. & Cristofani, S. (2009).
Mental health treatment outcomes in
a humanitarian emergency: a pilot model for
the integration of mental health into primary
care in Habilla, Darfur. International JournalofMental Health Systems, 3(1),17.
Summer¢eld, D. (1999). A critique of seven
assumptions behind psychological trauma
programmes in war-a¡ected areas. SocialScience&Medicine, 48(10),1449-1462.
The Sphere Project. (2011). Humanitarian Charterand Minimum Standards in Disaster Response -2011Edition. Geneva, Switzerland:The SphereProject.
Tol,W. A., Barbui, C., Galappatti, A., Silove, D.,
Betancourt, T. S., Souza, R., van Ommeren,
M. (2011). Mental health and psychosocial
support in humanitarian settings: linking
practice and research. Lancet, 378, in press.
rized reproduction of this article is prohibited.
http://siteresources.worldbank.org/DISABILITY/Resources/280658-1172610662358/Proj1Billion.pdfhttp://siteresources.worldbank.org/DISABILITY/Resources/280658-1172610662358/Proj1Billion.pdfhttp://siteresources.worldbank.org/DISABILITY/Resources/280658-1172610662358/Proj1Billion.pdf
Copyrig
Ventevogel et al.
van der Veen, M. & Somasundaram, D. (2006).
Responding to the psychosocial impact of the
Tsunami in a war zone: Experiences from
northern Sri Lanka. Intervention, 4, 53-57.
vanOmmeren,M.,Morris, J.&Saxena, S. (2006).
Integrated programme planning and psycho-
social concepts in humanitarian response:
A response toWilliamson andRobinson. Inter-vention, 4, 26-28.
van Ommeren, M., Saraceno, B., & Saxena, S.
(2004). Role of theWorld HealthOrganisation
in Mental Health Post-Con£ict Recovery:
Assisting Governments to Develop or Recon-
structMentalHealthServices InR.F.Mollica,
R. Guerra, R. Bhasin & J. Lavelle (Eds.),
Book of best practices.Trauma and the role of mentalhealth in post-con£ict recovery. (pp. 199^215).Retrieved from http://siteresources.world
bank.org/DISABILITY/Resources/280658-
1172610662358/Proj1Billion.pdf.
van Ommeren, M., Saxena, S. & Saraceno, B.
(2005). Aid after disasters. [Editorial]. BMJ,330(7501),1160-1161.
Ventevogel, P., Azimi, S., Jalal, S.&Kortmann, F.
(2002). Mental health care reform in
Afghanistan. Journal of Ayub Medical College,14(4),1-3.
Ventevogel, P., Faiz, H., & van Mierlo, B. (2011).
Mental health in basic health care:
experiences from Nangarhar Province.. In J.
F.Trani (Ed.),Development e¡orts in Afghanistan:Is there a will and a way? The case of disabilityand vulnerability. (pp.215^241). Paris: l’Harmat-tan.
Ventevogel, P.&Kortmann,F. (2004).Developing
basic mental health modules for health care
workers in Afghanistan. Intervention, 2, 43-54.
ht © War Trauma Foundation. Unautho
Watters, E. (2010). Crazy like us.The globalization oftheAmerican psyche. NewYork: Free Press.
Wessells, M. & van Ommeren, M. (2008).
Developing inter-agency guidelines on men-
tal health and psychosocial support in
emergency settings. Intervention, 6(3^4), 199-218.
Williamson, J. & Robinson, M. (2006). Psy-
chosocial interventions, or integrated pro-
gramming for well-being? Intervention, 4,4-25.
World Health Organization (2003). Mental healthin emergencies. Mental and social aspects of healthof populations exposed to extreme stressors. Geneva,World Health Organization.
World Health Organization (2005).Mental HealthAtlas - Revised Edition. Geneva: World HealthOrganization.
World Health Organization (2008). Kalmunai:A model on Mental Health Services DeliveryRetrieved September 24th 2011, from http://
www.whosrilanka.org/LinkFiles/WHO_Sri_
Lanka_Kalmunai_feature_story.pdf
World Health Organization (2010). mhGAP Inter-ventionGuideforMental,NeurologicalandSubstanceUse Disorders in Non-Specialized Health Settings.Geneva, Switzerland:WHO.
World Health Organization & Wonca (2008).
Integrating mental health into primary care: a globalperspective. Geneva /London: World HealthOrganization and World Organization of
Family Doctors (Wonca).
Zwi, A. & Ugalde, A. (1991). Political violence in
theThirdWorld: a public health issue. HealthPolicy& Planning, 6(3), 203-217.
rized reproduction of this article is prohibited.209
http://siteresources.worldbank.org/DISABILITY/Resources/280658-1172610662358/Proj1Billion.pdfhttp://siteresources.worldbank.org/DISABILITY/Resources/280658-1172610662358/Proj1Billion.pdfhttp://siteresources.worldbank.org/DISABILITY/Resources/280658-1172610662358/Proj1Billion.pdfhttp://www.whosrilanka.org/LinkFiles/WHO_Sri_Lanka_Kalmunai_feature_story.pdfhttp://www.whosrilanka.org/LinkFiles/WHO_Sri_Lanka_Kalmunai_feature_story.pdfhttp://www.whosrilanka.org/LinkFiles/WHO_Sri_Lanka_Kalmunai_feature_story.pdf
Copyrig
PeterVentevogel is a psychiatrist and cultural anthropologist. He works with the international NGOHealthNetTPO as mental health advisor, with the international NGOWarTrauma Foundation asthe editor in chief of Intervention, and with Arq, the Dutch psychotrauma expert group, as a clinical psy-chiatrist. email: [email protected]¤ rez-Sales is apsychiatrist atHosputalLaPaz(Madrid), psychosocial andmental health advidorfor Me¤ dicos del Mundo ^ Espan‹ a (Doctors of theWorld^Spain) and initiator of of the CommunityActionGroup(www.psicosocial.net).Hehasworkedextensivelywithgrassroot communityorganizationsin context of war or political violence. email: [email protected]¤ ndez-Liria is a psychiatrist.Heworks as chiefof theDepartment of Psychiatry inUniversityHos-pital Pr|¤ ncipe de Asturias, Spain and is an associate professor at the University of Alcala¤ Alcala¤ deHenares,Madrid (Spain).Florence Baingana is a psychiatrist and a public health specialist presently workingas aWellcomeTrustResearchFellowwithPersonal Social ServicesResearchUnit, London School ofEconomicsandPoliticalScience, London UK, andMakerere University School of Public Health, Kampala, Uganda.
Integrating mental health care into existing systems of health care: during and after complex humanitarianemergencies, Intervention 2011, Volume 9, Number 3, Page 195 - 210
ht © War Trauma Foundation. Unauthorized reproduction of this article is prohibited.210
http://www.psicosocial.net/
Copyrig
Rose et al.
Integrating mental health intoprimary health care settings afteran emergency: lessons from Haiti
Nick Rose, Peter Hughes, Sherese Ali & LynneJones
Following the 2010 Haiti earthquake, there was aneed for specialist services for severely mentally illpeople whowere presenting to the emergency medicalclinics set up for displaced people. That need wasunmet. Using guidelines drawn up by the Inter-Agency Standing Committee (IASC), and pilotingtheHealth Information System(HIS) ofdiagnosticcategories in mental health, weekly mental healthclinics were begun in eight mobile clinics. A psy-chiatric liaison service was also started in the maincasualty hospital. Haitian general practitionersand psychosocial workers, who received on-the-jobtraining and supervision from the authors, ran theseservices. This integrated mental health/primaryhealth care modelwas successful in engagingseverelymentally ill patients in treatment; however, thescale of the disaster meant that only a relativelysmall proportion of the displaced population couldaccess help. This limitation raised a number ofquestions about the practicality and sustainabilityof the IASC model in resource poor countries, withpoorly developed community services, hit by largescale emergencies, which the authors address.
Keywords: earthquake, Haiti, large scaleemergencies, mental health services,resource poor countries
The Haitian Government reported thatan estimated 220,000 people were killedand 1.5 million displaced in the 2010Haitian earthquake (United Nations HighCommissioner for Refugees (UNHCR),2010), although a more recent draft report
ht © War Trauma Foundation. Unautho
commissioned by the United States Agencyfor International Development (USAID)has recently claimed that the mortality¢gures may have been overestimated at leastthreefold (BBC, 2011). Nevertheless, what-ever the ¢nal estimate, the scale of thedisaster was immense; occurring in acountry where four out of ¢ve people alreadylived below the poverty line, and where thehealth infrastructure was weak. Haitiranks last for health care spending in theWestern Hemisphere (World Bank, 2006)with health provision unregulated andpatchy. Only 30% of health facilities werepublic, mostly in urban areas, and 70% ofrural health services were provided bynongovernmental organisations (NGOs),with 40% of the rural population havingno access to primary health care (WorldBank, 2006; WHO, 2010a). Mental healthresources were highly centralised, and con-sisted of two psychiatric hospitals in Port-au-Prince, both of which were understa¡edand in apoor state of repair.Therewere only0.2 psychiatrists per 100,000 general popu-lation, as compared to 11 per 100,000 in theUnited Kingdom (WHO, 2005), most work-ing in the capital city. Outside of Port-au-Prince, therewas little access to psychosocialsupport or e¡ective social services. Therewas, however, a widespread network oftraditional religious healers. Vodou beliefsare common in Haiti, and these beliefs sup-port a religious health care system that
rized reproduction of this article is prohibited.211
Copyrig
Integrating mental health into primary health care settings after an emergency: lessons from HaitiIntervention 2011, Volume 9, Number 3, Page 211 - 224
incorporates healing practices (WHO,2010a).Vodou beliefs are also re£ected in thepresentation and causal explanation ofsevere mental illness. This fragile healthinfrastructure was overwhelmed followingthe destruction of at least eight hospitals, aswell as the deaths and injuries of essentialpersonnel during the earthquake. A massiveaid e¡ort was mobilised, which includedattempts to meet the needs of those withsevere mental illness. This paper describeshow one group of mental health pro-fessionals undertook this task.
Meeting mental health needsfollowing large scale disastersWHO guidelines, for providing mentalhealth assistance after disasters, have pre-viously suggested that there are three groupsof distressed people, each requiring a di¡er-ent response (WHO, 2007). Those withmild psychological distress that resolves ina few days or weeks, and needs no speci¢cintervention, estimated at 20^40% of thea¡ected population; Those with moderateor severe psychological distress, who wouldbene¢t from basic non specialist, psycho-social interventions, such as psychological¢rst aid and interventions that strengthencommunity and family, are estimated at30^50% of the a¡ected population. Finally,are those with a mental disorder, the inci-dence of which appears to temporarilydouble following a disaster. Within this lastgroup, the prevalence of mild to moderatedisorders, such as mild to moderate depres-sion or anxiety, would be expected toincrease from a baseline of 10% (WHO,2004) to 20%, while the prevalence of severedisorders could rise from 2^3% to 3^4%.As a result, how to undertake psychosocialand mental health work after disasters haslong been the subject of debate. For example,there has been no agreement on the public
ht © War Trauma Foundation. Unautho212
health value of the posttraumatic stressdisorder (PTSD) concept and no agreementon the appropriateness of ‘vertical’ traumafocused services (van Ommeren et al.,2005). The needs of people with severemental disorders, in post disaster situations,have also been slow to get recognition. AfterHurricane Katrina in 2005, it was estimatedthat the prevalence of severemental disorderalmost doubled from 6.1 to 11.3% of thea¡ected population, yet psychosocialagencies tended to focus on the immediatetraumatic responses (Kessler et al., 2006).This lack of consensus to the approachmeant that mental health was only brie£ydiscussed in the ¢rst edition of the Sphereguidelines on humanitarian standards, pro-duced by a group of leading internationalaid organisations in 1998 (published asThe Human Charter and Minimum Standards inDisaster Response, commonly referred to asthe Sphere Handbook, currently in its 2011edition). Controversy continued during theAsianTsunami, when psychosocial agencieswere widely criticised for lack of agreedstandards and varying approaches. Thisexperience led directly to the creation ofthe Inter-Agency Standing Committee(IASC) task force set up to agree guidelinesfor the practice of mental health andpsycho-socialwork in emergency settings. Represen-tatives from 27 international governmentaland nongovernmental organisations workedover two years, in consultation with expertsfrom more than 100 nongovernmentalorganisations, academic institutions, andprofessional organisations. The resultingIASC Guidelines on Mental Health and Psycho-social Support in Emergency Settings representan international consensus on the type ofcare, and care system that is suitablefor emergency situations (Inter-AgencyStanding Committee, 2007; Wessells & vanOmmeren, 2008).
rized reproduction of this article is prohibited.
Copyrig
Rose et al.
The hierarchy of responses recommendedby the IASC guidelines includes: advocacyfor equitable and digni¢ed access to basicnecessities and protection for the majority;social interventions that reconnect disruptedfamilies and communities, and help themrestart their lives; more focused individualpsychosocial support for those who su¡ermore severe non pathological reactions;and clinical interventions for the mostseverely a¡ected minority. Other authorshave emphasised the importance of acknow-ledging and building on the naturalresilience of individuals and communities.Resilience is seen as a process rather thanan end point, and is reinforced throughstrategies such as psychological ¢rst aid,and enabling displaced communities to beas self-reliant as possible (Raphael, 2008;Bonanno et al., 2010).In relation to care for people with severemental disorders, the IASC guidancerecommends integrating mental healthprovision with primary care clinics (Box 1),
ht © War Trauma Foundation. Unautho
Box 1: Minimum response actionssevere mental disorders in emergMental Health and Psychosocial Supp
1. Assess situation (including surviving he2. Ensure adequate supplies of essential p3. Enable at least one member of emergen
provide frontline mental health care4. Train and supervise available PHC sta¡
mental disorders5. Avoid overburdening PHC workers wit6. Establish mental health care at additio
emergency rooms)7. Try to avoid creating parallelmental he
or narrow groups8. Inform population about the availabili9. Work with local community structures
severe mental disorders10. Be involved in all inter-agency coordin
which is consistent with the WHOstrategy for mental health provision inpoor nations (WHO, 2008). This guidancealso recommends giving appropriate sup-port to local services and institutionscaring for people with severe mental dis-orders and other mental and neurologicaldisabilities.Saraceno et al. (2007) have identi¢eda number of barriers to integrating mentalhealth services into primary care. One isthe work overload su¡ered by most primaryhealth care workers, which means they seethemselves as having no time for mentallyill patients. The second is providing short,theoretical training courses without followup supervision. These constraints mayresult in a failure to distinguish distress fromdisorder, and consequent overmedicalisa-tion, and overprescribing of psychotropicdrugs, for minor complaints. A third barriercan be the lack of psychotropic drugs, sothat even trained workers lack the meansto treat severe mental disorders.
rized reproduction of this article is prohibited.
to address needs of people withencies (from IASC Guidelines onort in Emergency Settings)
alth capacity)sychiatric drugscy primary health care (PHC) team to
in the frontline care of severe
h multiple di¡erent training sessionsnal logical points of access (including
alth services focused on speci¢c diagnoses,
ty of mental health careto discover, visit, and assist people with
ation on mental health
213
Copyrig
Integrating mental health into primary health care settings after an emergency: lessons from HaitiIntervention 2011, Volume 9, Number 3, Page 211 - 224
The IASC Guidelines address each of thesebarriers, recommending that theoreticaltraining is always accompanied by super-vised on-the-job training, and that primaryhealth care (PHC) sta¡ are assisted andtrained in time management to allowdedicated time for mental health work. Theguidelines also recommend training insimple psychological interventions for nonpathological distress, and rational prescrib-ing. Also important is investment in systemsof care, rather than individual sta¡ mem-bers, and ensuring that treatment conformsto international standards of care (Cohen,2001).The IASC recommended model of inte-grating mental and physical healthcare inemergency and con£ict zone situationsis now well established practice (vanOmmeren et al., 2005; Budosan et al., 2007;Jones et al., 2009; Rose, 2011; Mueller et al.,2011). However, the scale of the disaster inHaiti and the complete absence of com-munity based mental health care prior tothe earthquake provided a challengingopportunity to test the Guidelines in anemergency, resource poor setting ofimmense proportions.
Our response to the HaitiemergencyA rapid assessment of need was done within12 days after the earthquake. This includedcoordination with other local and inter-national agencies planning to providemental health and psychosocial care. Littleinformation was available on Haiti’s pre-existing mental health needs, thereforethe assessment included visiting both of thenational psychiatric hospitals in Port-au-Prince, and talking with surviving sta¡.Emergency clinics for displaced people, setupbyanumber of medical aid organisations,were also visited aswas themain Emergency
ht © War Trauma Foundation. Unautho214
Room for Port^au-Prince situated in thegrounds of the partly destroyed UniversityHospital, l’Hopital de l’Universite¤ d’Etatd’Haiti (HUEH).At this stage, the International MedicalCorps was responsible for providing15 com-munity clinics, as well as Emergency Roomservices at HUEH.The assessment revealedthat the majority of people attending theemergency services reported feeling shockedand afraid, with common complaints ofpalpitations and a persistent feeling thatthe ‘ground was moving’. People were alsobeing seen with severe mood disorder andpsychotic illness, clinical problems that themedical teams were poorly equipped tomanage.The majority of the a¡ected populationwere living in overcrowded makeshiftshelters and/or crowded camps for displacedpeople. They were frustrated and angry atthe di⁄culties of obtaining basic necessities,and at the lack of security. Therefore,advocacy to change these conditions was apsychosocial priority from the start. Mostpeople had su¡ered losses of some kind.Some individuals had been trapped underthe rubble for long periods. A child patientof one of the authors had been discoveredafter nine days for example. Because of therapid disposal of bodies in mass graves andthe persistent problem of uncleared rubble,many had been unable to ¢nd or identifythe remains of their loved ones, whichmade mourning di⁄cult. Added to this, fearand stress was generated by continuinggovernment warnings of the likelihood ofnew quakes. Given these conditions, theresilience of the population and the degreeto which they were helping themselveswas remarkable. Markets appeared in themakeshift camps in the ¢rst days after thedisaster, as did small enterprises such asphone charging, hair dressing and the
rized reproduction of this article is prohibited.
Copyrig
Rose et al.
sale of prostheses, crutches and wheelchairs.Assessment of the two psychiatric institu-tions revealed a particularly disturbingsituation. In the acute psychiatric hospitalnear the city centre, 11 of the original 100inpatients lived in degraded and insanitaryconditions with no running water, nopower, ¢lthy accommodation, no bedding,and no clothes.Many of the sta¡ were understandablypreoccupied with their own a¡airs, becausethey were bereaved, or their homes weredestroyed, and did not return to work forweeks. Those who did come to work had tocare for at least 150 outpatients a day in atent surrounded by an encampment of 120displaced families that had taken refuge inthe hospital yard.In the long stay hospital on the outskirtsof Port-au-Prince, many patients had runaway when the wall collapsed and theremainder slept in the open-air as the roomswere considered unsafe.At least 90 international and localagencies were o¡ering psychosocial supportafter the earthquake. Coordination tookplace through the UN led mental healthand psychosocial support sub-cluster, whichmet twice a week. A representative fromthe Haitian Ministry of Health was jointchair of this meeting. Mapping of agencyactivities made it clear that very few ofthem were providing psychiatric servicesfor the more severely a¡ected section ofthe population, either in the communityor in existing psychiatric institutions. Onlytwo agencies, apart from our own, wereproviding psychiatric care through clinicsin Port-au-Prince. In the earthquakea¡ected areas outside the city, there wereno psychiatric services available. The Inter-national Medical Corps then made thedevelopment of accessible psychiatric
ht © War Trauma Foundation. Unautho
support and services for this group apriority.Interventions to support the acute psy-chiatric hospital included: the provision ofa sta¡ transport vehicle, a generator,bedding, patient clothes, hygiene kits, clean-ing materials and essential medication. Atthe request of sta¡, a series of twice weeklytraining seminars was organised for threemonths. Also at their request, these seminarswere then extended for eight weeks. Theseaimed to support sta¡ in evaluating anddeveloping their care and treatment prac-tices. A generator was also provided for thesecond hospital, which cared for longer staypatients. Other organisations provided foodand tents. However, in light of the continuedfunctioning of both hospitals, albeit at areduced level, we decided that furthersupport of the two institutions requiredresources beyond the capacity of an emer-gency health agency. In line with the IASCGuidelines, we therefore prioritised the rapiddevelopment of community based mentalhealth services that would both serve emer-gency needs and decrease the demand forinstitutional care. Since a large number ofpeople with mental health problems werebeing seen in the Emergency Room follow-ing the earthquake, it was also decided toprovide a temporary psychiatric liaisonservice for the University Hospital, HUEH.A psychiatric liaison service at the Univer-sity Hospital started two weeks after theearthquake. In consultation with the hospi-tal’s Haitian medical director and theGovernment’s Department of Health, itwas agreed that a Haitian psychosocialworker would be employed to triagereferrals, supervised by an international orHaitian psychiatrist. The psychologistprovidedboth group and individual therapy,and a psychiatrist was available daily to seecomplex cases, as well as patients whomight
rized reproduction of this article is prohibited.215
Copyrig
Integrating mental health into primary health care settings after an emergency: lessons from HaitiIntervention 2011, Volume 9, Number 3, Page 211 - 224
need psychotropic medication. After sixmonths, as earthquake related problemsdiminished, the medical and psychiatricliaison services were gradually withdrawn.Community based mental health servicesbegan within a month of the earthquake inlocations with the greatest concentration ofdisplaced people. The model used followedIASC Guidelines and was supported byMinistry of Health o⁄cials. Mental healthclinics were integrated into eight busyprimary healthcare centres, each serving adisplaced population of between 10 and15,000. Most took place under canvass sincemany surviving buildings remained unsafe,and sta¡ and patients understandably feltsafer in the open. The clinics were locatedin the western suburbs of Port-au-Prince,and in the earthquake damaged SouthWestand Southern provinces.To address the time management problem,we suggested that mental health care beorganised in a manner similar to antenatalcare, by providing a‘mental health’clinic oncea week. At each primary health care clinic,a Haitian general practitioner was thereforereleased from general duties for half a day aweek to run this service. Thus, rather thanseeing such cases as a time consuming inter-ruption, the practitioner could give themadditional time, and more dedicated atten-tion. It also allowed for concentratedperiodsof on-the-job supervisionby an internationalpsychiatrist (one of the authors), oraHaitianpsychiatrist learning to become a workplacetrainer. Each mental health clinic, includingthe one attached to the emergency room,was co-ordinated by a community psycho-social worker, usually a previously un-employed Haitian psychologist or nurse.These were recruited as full time mentalhealth sta¡ working with patients on a dailybasis. As well as their service coordinationrole therefore, they were able to undertake
ht © War Trauma Foundation. Unautho216
preliminary assessments, provide individualand group therapeutic activities, liaise withother community resources such as localleaders, aid organisations, and traditionalhealers, and act as the point of referral forvictims of sexual and gender based violence.Each psychosocial worker also had the taskof recruiting and supervising a dozen localcommunity volunteers who could promotegood mental health, support appropriatemourning processes, identify peoplesu¡ering from severe mental illness intheir neighbourhood, engage them intreatment, and help them access localresources. Psychosocial workers liaisedclosely with the general practitioner incharge of their weekly mental healthclinic, and were clinically supervised by thevisiting international or local psychiatrist.In addition, a senior psychosocial worker,who organised a separate training pro-gramme to support and develop the act-ivities and skills of the psychosocialworkers, managed them.A patient ¢le system was established torecord demographic, clinical and traumarelated information. In addition, teammembers were taught to use the mentalhealth categories and case de¢nitions newlydeveloped in theHealth Information System(HIS) of the UNHCR, for use by primarycare sta¡ working in refugee camps(UNHCR, 2010). We used a pilot version,which included case de¢nitions, loaned tous by UNHCR, as yet unpublished. Thecategories are based on a recommendationin IASC Guidelines (2007), and are designedto simplify the diagnosis of mental distressand disorders by primary health careworkers, so that they can identify probablepsychiatric cases.The prior failure to includeanything but the most gross mental healthdiagnostic categories in HIS systems, inmany low and middle income countries,
rized reproduction of this article is prohibited.
Copyrig
Rose et al.
has added to the di⁄culties of primaryhealth care workers giving these patientsattention and care. The categories used(Table 1) are straightforward, and easilyrecognised by health workers. They also, toa large degree, match the newly createdmental health Gap Action programme(mhGAP) priority conditions (WHO,2010b). Establishing the community servicein Haiti provided an opportunity to infor-mally ¢eld test these de¢nitions. Essentialpsychotropic medication, included in theWHO essential medicine list, The Inter-Agency Health Kit (WHO, 2006) was madeavailable in all clinics.Training played a central role in clinicactivities. For the general practitioners,the aim was for them to be able to clinicallymanage most people presenting with severemental illness within three months. Thiswas done through workplace training andattending a weekly half day teachingprogramme. Assessment involved a combi-nation of workplace Assessed ClinicalEncounters, Case Based Discussions, andan end-of-training examination consistingof Objective Structured Clinical Examin-ations (OSCEs) and an oral exam.
ht © War Trauma Foundation. Unautho
Table 1. Health Information System (UNH
Health Information System (HIS) for use in huCategories
HIS1 Epilepsy/seizuresHIS 2 Alcohol or other substHIS 3 Mental retardation/ inHIS 4 Psychotic disorderHIS 5 Severe emotional disoHIS 6 Other psychological c
in major day-to-dayHIS 7 Medically unexplaineNo HIS category for: Dementia
Other, for psychiatricNo psychiatric disorde
The curriculum of the teaching programmewas based on the textbook ‘WhereThere Is NoPsychiatrist’ (Patel, 2003), IASC Guidelines,and a draft of the mhGAP Intervention Guide(WHO, 2010b). Psychosocial workers alsoattended the half-day teaching programme,and were supervised in providing basic,individual and group interventions focusedmainly on anxiety management andproblem solving. Two part time Haitianpsychiatrists were recruited to train asworkplace supervisors and assessors of thegeneralpractitioners, so that the programmecould become independent of internationalsta¡, and therefore more sustainable.
Patients seenDuring the ¢rst ¢ve months of thecommunity clinics, a total of 431 patientswere assessed on eight sites. Assessmentsincluded a supervising psychiatrist in 65%of cases. Of the patients seen, 22% hadexperienced the loss of a ¢rst-degree relativein the earthquake, and 74% had su¡eredserious damage or collapse of their dwelling(Table 2). About half of those assessed hadseen a traditional healer for their complaint,often at great expense. By far the most
rized reproduction of this article is prohibited.
CR, 2010)
manitarian settings: Mental Health
ance use disordertellectual disability
rderomplaints (including anxiety) not resultingdysfunctiond somatic complaint
disorders not covered in the seven categoriesr present
217
Copyrig
Table 2. Clinic activity (data February^June 2010)
General hospitalPrimary careclinics (8 sites)
Number of new patients seen 201 431Total clinical consultations 356 722Mean age 30 (range 3^75) 32 (range 0.5^88)Number of females seen 59% 64%Children seen (under16) 13% 13%Loss of 1st degree relative 29% 22%Loss of non1st degree relative 12% 13%Housing destroyed by earthquake 27% 58%Housing damaged, but habitable 15% 16%Seen by traditional healer 15% 47%Assessment by GPor psychosocial
worker supervised by a psychiatrist55% 65%
Assessment only 5% 1%Main intervention:
Medication 20% 20%Psycho education 11% 40%Counselling 6% 5%Psychosocial support 57% 34%
Integrating mental health into primary health care settings after an emergency: lessons from HaitiIntervention 2011, Volume 9, Number 3, Page 211 - 224
common mental health category was‘other psychological complaints’ (HIS 6) whichaccounted for 55% of all patients seen(Table 3). These complaints were over-whelmingly of anxiety, usually focused ona fear of buildings falling, or of losingpeople close to them. Psychosis (HIS 4)accounted for 13% of patients seen andepilepsy (HIS 1) for 11%. Surprisingly only3% of patients had severe emotionaldisorder (bipolar or severe depression) andonly ¢ve cases of alcohol or other substanceuse disorder were diagnosed. Symptoms ofgrief were common, and it was often hardto disentangle what was culturally normal,from what was morbid. Concerning treat-ment, 40% received psycho education,which included anxiety management; 34%psychosocial support, usually in the form ofhelp in solving basic needs related problems;
ht © War Trauma Foundation. Unautho218
and 5% focused counselling. Only 20%were prescribed medication.Comparing diagnoses made in communityclinics during the ¢rst ¢ve months after theearthquake (February^June), with the next¢ve months (July^November), there was a10-fold reduction of patients presentingwith minor disorders as recorded underthe HIS category 6 of ‘other psychologicalcomplaints’ (Table 3). By contrast, severeemotional disorders increased from 3%to 21%, and medically unexplained com-plaints increased from1%to15%.Dementiaalso presented more frequently during thislater period, althoughtherewas little changein the referral pattern of other severe andchronic disorders, such as people with psy-chosis, learning di⁄culties or epilepsy.The general hospital clinic appeared to pickup a similar range of clinical problems as
rized reproduction of this article is prohibited.
Copyrig
Table 3. Diagnosis of newly assessed patients (data February^November 2010)
Health Information System(HIS) diagnosis for use inhumanitarian settings:Mental health categories(probable cases)
GeneralhospitalFeb^June
Primarycare clinicsFeb^June
Primarycare clinicsJuly-Nov Total
No psychiatric diagnosis 0 27 (6%) 5 (1%) 27 (3%)HIS1Epilepsy 5 (3%) 47 (11%) 78 (16%) 130 (12%)HIS 2 Alcohol/substance
misuse0 5 (1%) 11 (2%) 16 (1%)
HIS 3 Learning disability 0 21 (5%) 27 (6%) 48 (4%)HIS 4 Psychotic disorder 29 (17%) 58 (13%) 92 (19%) 179 (17%)HIS 5 Severe emotional
disorder30 (18%) 15 (3%) 98 (21%) 143 (13%)
HIS 6 Other psychologicalcomplaint
80 (47%) 239 (55%) 23 (5%) 342 (32%)
HIS 7Medically unexplainedsomatic complaint
5 (3%) 4 (1%) 72 (15%) 81 (8%)
Dementia 1 (1%) 5 (1%) 29 (6%) 35 (3%)Other 21 (12%) 10 (2%) 44 (9%) 75 (7%)Total number of assessments 171 431 474 1076
Rose et al.
the community clinics. This probablyre£ected the fact that large numbers ofdisplaced people in nearby city centrecamps used the hospital for primary care.However, there was a six-fold increase inthe number of patients seen with severeemotional disorders at the hospital, ascompared to primary care, during the sameperiod after the earthquake. Many of thesepatients had life threatening depressivedisorders, and were often in a state ofextreme physical neglect requiring medicalintervention. The general hospital emer-gency room received many cases of severegender based violence, sometimes withchildren as the victims. Poor security andlighting in many of the camps, as well asdisrupted community links, may haveaggravated this problem. Four particularlyseverely a¡ected victims of sexual abuse
ht © War Trauma Foundation. Unautho
were assessed and followed up by thehospital psychosocial worker.Concerning sta¡ training, over the ¢ve-month period starting from February 2010,140 health workers attended one of sixprogrammes of mental health seminars,each heldona di¡erent site.Of these,73werenurses and 31 medical practitioners. Therest included psychologists, health assistantsand a small number of translators. Twelvemedical practitioners completed the com-bined seminar and work place trainingprogramme, and successfully passed theassessment programme.
DiscussionThe patient information, recorded inTables 2 and 3, represent an audit of whopresented at the mental health clinics, butcannot give an accurate picture of needs
rized reproduction of this article is prohibited.219
Copyrig
Integrating mental health into primary health care settings after an emergency: lessons from HaitiIntervention 2011, Volume 9, Number 3, Page 211 - 224
within the community. The data does,however, give a snapshot of what people willbring to primary health care clinics in anemergency situation, and how that picturechanges over time. The signi¢cant presenceof epilepsy and psychosis justi¢ed theattention givenby the programme in provid-ing services for those with severe mental dis-orders, and is consistent with experiencesin other emergencies (Jones et al., 2009).The 10-fold drop in incidence of HIScategory 6, from 55% during the ¢rst ¢vemonths after the earthquake to 5% in thesubsequent ¢ve-month period, almostcertainly re£ects the temporary nature ofthe surge of anxiety following the disaster.These cases appear to have been partlyreplaced by cases of severe emotional dis-orders, for the most part depression, endur-ing grief reactions, and somatic complaints.This may re£ect the enduring problems ofloss, and the stress of daily life in temporaryand inadequate shelters.In terms of setting up the mental healthclinical and training programme, the IASCmodel proved to be a useful operationalframework. In £uid and insecure circum-stances, with enormous logistical challenges,it was possible to integrate a mental healthservice into at least half of the emergencymobile primary care clinics set up by theInternational Medical Corps within thedisaster hit areas.The UNHCRHIS systemalso proved to be a useful tool for trainingsta¡, and related neatly to the mhGAPcurriculum. However we had to add threenew HIS categories: no psychiatric disorder,dementia, and ‘other’ for psychiatricconditions not covered under the sevenheadings.
Dilemmas encounteredOf the many dilemmas faced in developingand running the programme, three related
ht © War Trauma Foundation. Unautho220
dilemmas stood out: the sustainability ofthe integrated mental health/primary caremodel, post emergency in a country withpoorly developed primary health infrastruc-ture, and no history of community psy-chiatry; the possibility of unintended badconsequences; and whether it was wise toinvest in community mental health services,rather than reinforcing already establishedcentral ones.The moral case for providing local emer-gency clinics after the earthquake is clear,but should a mass disaster be used as anopportunity forWestern agencies to promotecommunity mental health services, parti-cularly when central services are so under-developed? Additionally, is it reasonable toset up amodel thatmay prove unsustainable,since it is so dependent on the continuing£ow of foreign aid, and the future prepared-ness and capacity of the Haitian governmentto take over responsibility? As far the modelof care was concerned, we felt that this wassomething on which there was an inter-national consensus, rather than beingwestern imposed clinical practice (WHO,2009). Also, the patchily provided medicalsystem in Haiti, with its heavy dependenceon private, urban based services did notprovide an ideal structure in which to inte-grate community based mental health care.As far as donor commitment goes, althoughthis has been maintained to date, it remainssomething to be advocated for in theseuncertain economic times. It will needexpensive long term institution buildingif the model is to be rolled out nationally.At the very least, we hoped to demonstrateto the Haitian government the bene¢t offree services provided through the innumer-able mobile clinics that were running duringthe emergency, and to model how mentalhealth care could be integrated into primarycare.We were involved in discussions about
rized reproduction of this article is prohibited.
Copyrig
Rose et al.
the possibility of setting up publicallyfunded primary health care, but there wasno guarantee that this would happen. Sothe question arises as to the value of trainingprimary healthcare workers for a servicethat may not be sustained, and the ethics ofproviding care free of charge when thattoo may not last. Recognising that we couldnot predict the long term direction ofplanning with elections about to happen,we reasoned that it was worth training acadre of primary care sta¡ and psychosocialworkers who could be a resource for thecountry in the longer term.All humanitarian interventions risk unin-tended bad consequences. For example,providing services to hundreds of tentedcamps inevitably creates dependency,although the continuing failure to clearrubble and build e¡ective new homes hasmeant such services have remained essential.Another important consequence is thatthe presence of a competent outside agencyproviding free medical services may under-mine local incentives to manage problemswith local resources. There was certainlyno shortage of Haitian doctors in thecountry, many having run small privatepractices before the earthquake. Indeed,the mobile emergency clinics set up by theInternational Medical Corps were sta¡edby doctors easily recruited from the privatesector whose own clinics were out of action,as well as a small number of ministry ofhealth (MOH) sta¡ out of work becausetheir clinics had been destroyed. So,although we avoided recruiting fromfunctioningMOH services to prevent under-mining public services, we may haveinadvertently underminedthe private sector.Another consequence of providing freeservices, which included free medication,was that drugs donated to Haiti foundtheir way onto the market place. We had
ht © War Trauma Foundation. Unautho
direct evidence, for example, of donatedpsychotropic drugs being sold to patients.All of these unintended consequences ofintervention need further evaluation toinform future practice.The ¢nal dilemma arose fromthe decision