Embed Size (px)
Citation preview
ORIGINAL ARTICLE
A Clinical Review of InfectedWound Treatment withVacuum Assisted Closure®
(V.A.C.®) Therapy: Experienceand Case SeriesAllen Gabriel, Jaimie Shores, Brent Bernstein, Jean de Leon, Ravi Kamepalli,Tom Wolvos, Mona M Baharestani, Subhas Gupta
Gabriel A, Shores J, Bernstein B, de Leon J, Kamepalli R, Wolvos T, Baharestani MM, Gupta S. A Clinical Reviewof Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy: Experience and Case Series. IntWound J 2009; 6:1–25
ABSTRACTOver the last decade Vacuum Assisted Closure® (KCI Licensing, Inc., San Antonio, TX) has been establishedas an effective wound care modality for managing complex acute and chronic wounds. The therapy has beenwidely adopted by many institutions to treat a variety of wound types. Increasingly, the therapy is being used tomanage infected and critically colonized, difficult-to-treat wounds. This growing interest coupled with practitioneruncertainty in using the therapy in the presence of infection prompted the convening of an interprofessional expertadvisory panel to determine appropriate use of the different modalities of negative pressure wound therapy (NPWT)as delivered by V.A.C.® Therapy and V.A.C. Instill® with either GranuFoam™ or GranuFoam Silver™ Dressings.The panel reviewed infected wound treatment methods within the context of evidence-based medicine coupledwith experiential insight using V.A.C.® Therapy Systems to manage a variety of infected wounds. The primaryobjectives of the panel were 1) to exchange state-of-practice evidence, 2) to review and evaluate the strength ofexisting data, and 3) to develop practice recommendations based on published evidence and clinical experienceregarding use of the V.A.C.® Therapy Systems in infected wounds. These recommendations are meant to identifywhich infected wounds will benefit from the most appropriate V.A.C.® Therapy System modality and provide aninfected wound treatment algorithm that may lead to a better understanding of optimal treatment strategies.
Key words: negative pressure wound therapy • NPWT • V.A.C.® Therapy System • Vacuum Assisted Closure® • infected woundcare
Authors: A Gabriel, MD, The Department of Plastic Surgery, Loma Linda University School of Medicine, Loma Linda, CA; J Shores, MD,The Department of Plastic Surgery, Loma Linda University School of Medicine, Loma Linda, CA; B. Bernstein, DPM, St Lukes Hospital,Bethlehem, PA; J de Leon, MD, Baylor Specialty Hospital, Dallas, TX; R. Kamepalli, MD, Regional Infectious Diseases-Infusion Center,Lima, OH; T Wolvos, MS, MD, FACS, Scottsdale Healthcare Hospitals, Scottsdale, AZ; MM Baharestani, PhD, ANP, CWON, CWS, EastTennessee State University and the James H. Quillen Veterans Affairs Medical Center, Johnson City, TN; S Gupta, MD, PhD, FRCSC, FACS,The Department of Plastic Surgery, Loma Linda University School of Medicine, Loma Linda, CAAddress for correspondence: Subhas Gupta, MD, PhD, FRCSC, FACS, The Department of Plastic Surgery, Loma Linda UniversitySchool of Medicine Coleman, Pavilion 21126 11175 Campus Street, Loma Linda, CA 92354 Phone: 909-558-8085 Fax: 909-558-4175E-mail: [email protected]
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd • International Wound Journal • Vol 6 (suppl. 2) 1

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
INTRODUCTION
Infection
Infections complicate the treatment of woundsand impede the healing process by damag-ing tissue, reducing wound tensile strengthand inducing an undesirable inflammatoryresponse (1,2). It is generally believed thatwound infection advances in stages fromcontaminated, colonized, critically colonizedto infected (3,4). When wound surface bac-teria begin replication and increase theirmetabolic activity, the resulting by-products,such as endotoxins and metalloproteinases(MMPs), negatively impact all phases ofwound healing (5).
The control and prevention of infections iscritical in order for the normal wound heal-ing cascade to occur. Heavy wound biobur-den increases metabolic requirements, stim-ulates a proinflammatory environment, andencourages the in-migration of monocytes,macrophages and leukocytes that can neg-atively impact healing. Bacteria also secreteharmful cytokines which can lead to vasocon-striction and resultant decreased blood flowto the wound (5). From a healthcare economicperspective, decreased infection rates yield sig-nificant overall cost savings, as infections resultin significant morbidity, mortality, excess med-ical expenses and lengthened hospital staysannually (6).
The ancient Egyptians were the first civi-
Financial Disclosures:
• Allen Gabriel, MD - Consultingagreement with Kinetic Con-cepts, Inc.
• Jaimie T. Shores, MD - Nofinancial interests or commer-cial associations
• Brent Bernstein DPM - Con-sulting agreement with KineticConcepts, Inc.
• Jean de Leon, MD - Consultingagreement with Kinetic Con-cepts, Inc.
• Ravi Kamepalli, MD - No finan-cial interests or commercialassociations
• Tom Wolvos, MD- Consultingagreement with Kinetic Con-cepts, Inc.
• Mona M. Baharestani, PhD,ANP, CWON, CWS–No finan-cial interests or commercialassociations
• Subhas Gupta, MD, PhD -Agreement with Kinetic Con-cepts, Inc. to serve as GuestCo-editor of current supple-ment
lization to provide detailed information aboutmanagement of disease, including woundmanagement with the application of variouspotions and grease to assist healing. Hip-pocrates, known as the father of medicine,used vinegar to irrigate open wounds andwrapped dressings around wounds to pre-vent further injury (7). In 1867, Joseph Listerintroduced the antiseptic treatment of woundswhich fostered a growing understanding ofthe importance of technical surgical skill cou-pled with a reduction in bacterial introduc-tion into surgical wounds (8). During the firsthalf of the 20th century, sulfa drugs andantibiotics (eg, penicillin, streptomycin, etc)were developed for the systemic treatment ofinfection.
The scale of wound infections has beenmost evident in times of war. During theAmerican Civil War, arms and legs weresubsequently amputated despite a 25–90%
risk of amputation residual limb infection (9).World War I produced new wound etiolo-gies such as high-velocity bullet and shrapnelinjuries, as well as those contaminated bymud from the trenches. During World WarII, modern surgical reconstructive and tissue-preserving techniques began to replace ampu-tation. Debridement, irrigation, and closure bydelayed primary intention became fundamen-tal management techniques to facilitate woundclosure (10,11). Wars following World War IIhave used a combination of debridement, asep-tic techniques, wound treatment systems, andtopical and systemic drugs for the treatment ofinfection.
In 2001, the United States Centers forDisease Control and Prevention (CDC) esti-mated that about 290,000 surgical site infec-tions (SSIs) occurred annually, with approx-imately 8,000 patient deaths resulting fromSSIs (12). An SSI occurs when an infectiondevelops at the surgical site within 30 daysor within 1 year of an operation if a for-eign body (eg, heart pacemaker or artificialjoint) is implanted as part of the surgery.About 70% of SSIs are superficial infectionsinvolving skin only. However, the remaininginfections are more serious and can involvetissues under the skin, organs, or implantedmaterials (12).
Unfortunately, the quest to eradicate infec-tion is nowhere near being resolved, dueto an insurgence of antibiotic-resistant bac-terial strains and the increasingly complexsurgical interventions performed in immuno-compromised patients and implant surg-eries. Therefore, one of the panel’s purposeswas to offer recommendations for the useof V.A.C.® Therepy modalities on infectedwounds.
V.A.C.® Therapy and infected woundsNegative pressure wound therapy (NPWT),as delivered by Vacuum Assisted Closure®
(V.A.C.® Therapy, KCI Licensing, Inc., SanAntonio, TX), was cleared for marketing in1995. This system applies localized nega-tive pressure to the wound bed througha polyurethane reticulated open-cell foam(ROCF) dressing (V.A.C.® GranuFoam™ Dress-ing) or a polyvinyl alcohol foam (V.A.C.®
WhiteFoam) dressing. When tissue is stretchedand drawn into the open pores of the foam
2 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
dressing under negative pressure, cell mito-sis is stimulated, leading to proliferation ofreparative granulation tissue (13). When usedin conjunction with appropriate antibiotictherapy, NPWT/ROCF has been reported tofacilitate wound closure through its abilityto reduce localized edema, increase woundedge vascularity, remove inhibitory agents,stimulate granulation tissue formation, pro-vide a moist wound healing environmentpromote perfusion and promote wound con-traction (14–17).
Current indications of NPWT/ROCF includechronic, acute, subacute and traumatic wounds,pressure and diabetic ulcers, partial-thicknessburns, dehisced wounds, flaps and grafts (18).A large body of literature has been pub-lished regarding clinical experience withNPWT/ROCF. A number of these publica-tions have reported the use of adjunctiveNPWT/ROCF treatment of contaminated ster-nal, abdominal, and extremity wounds (19–22).Reported benefits of NPWT/ROCF in the man-agement of colonized or infected wounds arelisted in Table 1.
Panel members agreed that treatment ofinfected wounds or those at high risk for infec-tion requires cautious and judicious use ofNPWT/ROCF. This therapy should be pro-vided against a background of best practicewith regard to early recognition of infection,administration of appropriate antibiotic ther-apy, thorough wound irrigation and surgicaldebridement (23). Despite expanded usage ofNPWT/ROCF in contaminated wounds (18,24,25), some clinicians avoid use of the ther-apy in the presence of infection and con-tinue to treat wound infection with standardtherapies, including moistened gauze dress-ings, antiseptics, antibiotics, and enzymaticointments.
Table 1 Reported benefits of NPWT/ROCF on infectedwounds
• Positive patient outcomes• Limb preservation• Positive patient comfort and pain relief• Low number of dressing changes• Less complexity required in surgical procedures• Relatively short time to closure• Short hospital stay• Low failure rate• Low overall costs
Most studies documenting use of NPWT/ROCF for adjunctive management of com-plex colonized or infected wounds were per-formed with V.A.C.® GranuFoam™ Dressing.V.A.C. GranuFoam Silver® (NPWT/ROCF-silver) Dressing and V.A.C. Instill® WoundTherapy (NPWT with instillation) were devel-oped to specifically provide the antimicrobialbenefits of silver and wound irrigation toNPWT/ROCF, respectively. The panel mem-bers reviewed three NPWT/ROCF systemsduring their discussion.
1. V.A.C.® Therapy with GranuFoam™
Dressing2. V.A.C.® Therapy with GranuFoamSilver™ Dressing3. V.A.C. Instill® Wound Therapy withGranuFoam™ or GranuFoam Silver™
Dressings
The primary purpose of this article is to: 1)review and evaluate existing evidence regard-ing use of NPWT/ROCF to manage infectedwounds; 2) develop practice recommendationsbased on published evidence and clinical expe-rience regarding use of the V.A.C.® TherapySystems on infected wounds; and 3) demon-strate how each of three different V.A.C.®
Therapy modalities may be incorporated intoan infection treatment algorithm.
BACKGROUNDPathophysiology of wound healingWound healing progresses through a numberof highly interdependent phases in an attemptto not only repair but also to compensate forreduced function that has occurred as a resultof the wound’s loss of tissue integrity. This pro-cess can be divided into four general phasesthat often overlap in time: 1) hemostasis (con-trol of bleeding); 2) inflammation (removalof debris, control of infection, clearance ofinflammation); 3) proliferation (angiogenesis,deposition of granulation tissue, contraction);and 4) remodeling (remodeling of the con-nective tissue matrix, and maturation) (26–28).Because growth factors, cytokines, proteases,and cellular and extracellular elements all playimportant roles in different stages of the heal-ing process, imbalances of one or more of thesecomponents may account for the impairedhealing observed in chronic wounds.
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 3

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
Levels of various MMPs (MMP-1 [colla-genase], MMP-2 [gelatinase A] and MMP-9 [gelatinase B]) and serine proteases aremarkedly increased in fluids from chronicwounds (29), whereas MMP levels are lowerin acute wound healing (30). Other proteases,such as neutrophil elastase, have also beenobserved to be significantly higher in chronicwounds (31). Elevated levels of serine pro-teases degrade fibronectin, an essential proteininvolved in the remodeling of the extracellularmatrix (ECM) (29,32).
Although inflammation is part of normalwound healing, healing may be prolongedwhen inflammation is excessive (33). In chronicwounds, necrotic tissue and slough tend tocontinually accumulate due to underlyingpathogenic abnormalities that alter the bio-chemical and cellular environment (34). Theaccumulation of necrotic tissue or slough ina wound promotes bacterial colonization andprevents complete repair of the wound. Thewound ‘‘stalls’’ in the inflammatory stageindefinitely, since increasing bacteria in awound produce pro-inflammatory mediatorssuch as IL-1, TNF-α, prostaglandin E2, andthromboxane (35).
Wound infection continuum andhealingAll wounds contain bacteria at levels rangingfrom contamination to infection. The increasedbacterial bioburden may be confined to thesuperficial wound bed or may be presentin deep compartments and the surroundingtissue of the wound margin. Once wound-ing occurs, whether through surgery, trauma,or endogenous mechanisms, the probabilityfor contamination to occur is 100% (36,37).Contaminating microorganisms arise from theexternal environment, surrounding skin, andendogenous sources, such as the gastrointesti-nal tract (36,37).
While previously accepted terms of con-taminated versus infected seemed clear cut,a more complex ‘‘continuum of wound infec-tion’’ has emerged in recent years. The con-tinuum consists of the surgical wound, con-taminated wound (presence of non-replicatingorganisms), the colonized wound (replicatingorganisms without tissue necrosis), the criti-cally colonized wound, and the infected wound.The four terms of interest used in reference tothe bacterial bioburden of a wound in wound
healing within this context are contaminated,colonized, critically colonized, and infected (3,4).These terms are defined in detail later in thispaper.
The development of an infected wound isan ‘exponential progression’ which may startwith sterility, but more often with contam-ination, colonization, critical colonization, orinfection. An untreated superficial infectioncan potentially become systemic and result insepsis. All stages are linked and if attemptsare not made to stop the progression at anylevel, bacteria may continue to replicate andproduce a polymeric matrix (glycocalyx), orbiofilm, that adheres to any inert or living sur-face and allows bacteria to live protected inan otherwise hostile environment (33). Theseprotected colonies can undergo genetic muta-tion to alter their sensitivity to antimicrobialsand are generally resistant to topical and sys-temic antibacterials. Thus, debridement is usu-ally necessary to remove a biofilm (33,38–40),although complete biofilm eradification cannotbe assured.
It has been postulated that the microor-ganisms in an infected wound consume thenutrients and oxygen that would otherwisebe directed toward tissue repair (41). Thebacteria release enzymes that break down pro-teins, a critical component of wound regenera-tion. Schmidtchen et al reported that elastase-producing bacterial isolates were shown tosignificantly degrade plasma proteins andextracellular products of human skin andfibroblasts, and inhibit fibroblast growth (42).These effects, in conjunction with the find-ing that proteinase production was detectedin wound fluid ex vivo, suggest that bac-terial proteinases play a pathogenic role inchronic wounds. Reducing the bacterial loadof a wound may enable the body to redirectresources from fighting infection to healing.
Extensive debridement (ie, removal ofnecrotic tissue, foreign material, and bacte-ria from an acute or chronic wound) andopen wound management have been widelyadvocated to prevent progression to infectionin traumatic wounds, contaminated soft tis-sue defects, postoperative complications andchronic, non-healing wounds. The goal isremoval of necrotic tissue, exudate, and infec-tious material from the wound bed to enableprogression through the normal wound heal-ing phases, assuming that systemic and local
4 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
factors are functioning normally (43). Aggres-sively debriding a chronic wound helps con-vert it to an acute wound. Debridement isaccomplished through non-surgical (eg, bio-logic, enzymatic, autolytic, or mechanical) andsurgical (eg, sharp, hydro-surgical, or laser)methods.
The combination of debridement to a viabletissue base and the application of topicalantimicrobials has been shown to aid in thesuccessful management of complex infectedor critically colonized wounds (25,44,45).Once the wound has been debrided, ade-quate vascularization has been confirmed,and appropriate antimicrobial therapy has
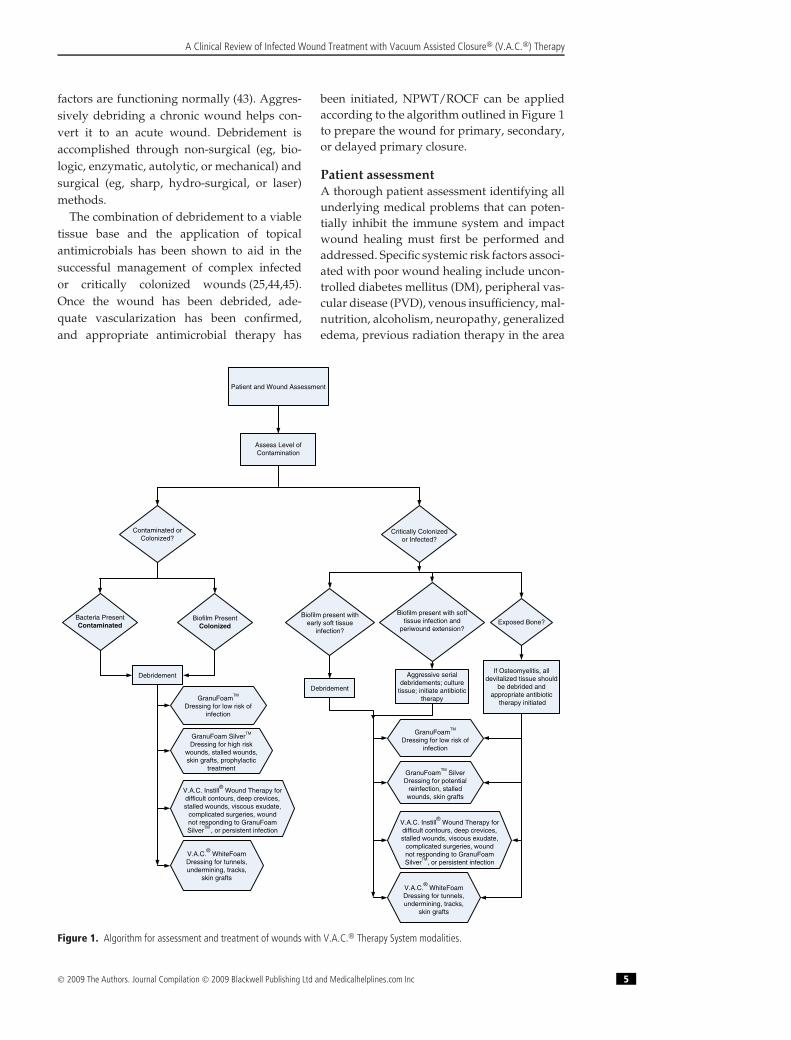
been initiated, NPWT/ROCF can be appliedaccording to the algorithm outlined in Figure 1to prepare the wound for primary, secondary,or delayed primary closure.
Patient assessmentA thorough patient assessment identifying allunderlying medical problems that can poten-tially inhibit the immune system and impactwound healing must first be performed andaddressed. Specific systemic risk factors associ-ated with poor wound healing include uncon-trolled diabetes mellitus (DM), peripheral vas-cular disease (PVD), venous insufficiency, mal-nutrition, alcoholism, neuropathy, generalizededema, previous radiation therapy in the area
Patient and Wound Assessment
Assess Level ofContamination
Contaminated orColonized?
Critically Colonizedor Infected?
Bacteria PresentContaminated
Biofilm PresentColonized
Debridement
GranuFoam SilverTM
Dressing for high riskwounds, stalled wounds,skin grafts, prophylactic
treatment
GranuFoamTM
Dressing for low risk ofinfection
Biofilm present withearly soft tissue
infection?
Biofilm present with softtissue infection and
periwound extension?Exposed Bone?
Debridement
Aggressive serialdebridements; culture
tissue; initiate antibiotictherapy
If Osteomyelitis, alldevitalized tissue should
be debrided andappropriate antibiotic
therapy initiated
GranuFoamTM
SilverDressing for potential
reinfection, stalledwounds, skin grafts
V.A.C.®
WhiteFoamDressing for tunnels,undermining, tracks,
skin grafts
V.A.C. Instill®
Wound Therapy fordifficult contours, deep crevices,stalled wounds, viscous exudate,
complicated surgeries, woundnot responding to GranuFoamSilver
TM, or persistent infection
GranuFoamTM
Dressing for low risk ofinfection
V.A.C.®
WhiteFoamDressing for tunnels,undermining, tracks,
skin grafts
V.A.C. Instill®
Wound Therapy fordifficult contours, deep crevices,stalled wounds, viscous exudate,
complicated surgeries, woundnot responding to GranuFoamSilver
TM , or persistent infection
Figure 1. Algorithm for assessment and treatment of wounds with V.A.C.® Therapy System modalities.
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 5

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
of the wound and long-term corticosteroiduse (41). A combination of these factors mayalso cause a remodeled wound to break down.
Peripheral vascular assessment, especiallyin patients with lower extremity wounds,is imperative. Regardless of the etiology,insufficient blood flow may prevent systemicantibiotics from reaching the wound andmay not allow the body to systemically clearmicroorganisms. If perfusion is inadequate,surgical, endovascular, hyperbaric oxygenand/or pharmacological intervention may benecessary.
Patient age should also be considered amajor factor in the wound healing process,based on the biochemical and cytokine milieuthat is present with aging (46,47). There is anup-regulation of MMP-2 in normal aged skin,and MMP-2 and MMP-9 in acute wounds inaged skin in comparison to that found in skinof young adults (46,47). This alteration in thecytokine profile is similar to that seen in chronicwounds in younger patients and may affect thewound healing process.
Wound assessmentA complete wound assessment, including size(eg, area, volume, depth, etc), base color,amount and type of exudate, odor, and pres-ence of edema, is necessary to determine thestatus of the wound. Specifically, wound colorcan be an initial determinant of infection.Bioburden classification may be made bothclinically and by more quantifiable methods.Tissue biopsy and culture has become the‘‘gold standard’’ for assessing wound bacteriallevels (48,49). However, quantitative culturingis not routinely performed in many institu-tions as it is less convenient and/or acces-sible than swab cultures, requires additionalpractitioner skill, is invasive, takes longer tocollect and process and is more costly. Deepbacterial swabs can be used to provide asemi-quantitative estimate of bacterial growthand may be performed after debridement inthe operating room (48,50). Despite ongoingcontroversy in measuring bacterial bioburden,current diagnoses of infection have remainedlargely based on clinical symptoms and signs(Table 2). Currently, the Infectious DiseasesSociety of America (IDSA) guidelines recom-mend that two signs of inflammation (eg,redness, warmth, or, swelling) or other clinicalsigns (eg, purulence, cellulitis, or, pain) must
Table 2 Clinical and systemic signs of infection
Signs/symptoms ofsystemic infection
Signs/symptoms oflocal infection
• Fever • Pain• Aches • Redness• Chills • Pus• Nausea • Swelling• Vomiting • Drainage with a foul odor• Weakness • Heat to the site
• Fever
be present to indicate infection (51). Althoughit is beneficial to have quantitative results,broad-spectrum antibiotic treatment can beadministered, provided cultures have alreadybeen taken at the onset of secondary clinicalfindings, with clinical improvement noted bythe time culture results are available.
Deep bacterial swabs, tissue biopsies, andwound cultures may be used to guide antimi-crobial therapy. Antibiotics and/or topicalantiseptics should be administered with a clearunderstanding of the treatment goals deter-mined by the clinician. Antibiotics are com-monly administered systemically and havea single pharmacologic target, which makesthem vulnerable to resistance. On the otherhand, antibacterial antiseptics are suitable fortopical administration, have broad-spectrumcoverage, and multiple mechanisms of action,which renders them less likely to trigger resis-tance (52).
WOUND TYPES AND ASSESSMENTALGORITHMFor the purposes of establishing an NPWT/ROCF algorithm for treating infected wounds,wounds were classified according to levelof contamination. The following are detaileddescriptions of each of the classifications in thealgorithm. (Figure 1)
Contaminated woundsWound contamination is defined as the pres-ence of non-replicating microorganisms that donot impair wound healing (3,4). Primary ther-apy goals for contaminated wounds are to pre-vent further wound deterioration and facilitateclosure. Often these wounds are inflamedsubsequent to an acute trauma, which can bedetrimental to wound healing. Debridementcan be performed surgically or non-surgicallyto remove non-replicating microorganisms.
6 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
Colonized woundsWounds that are making progress towardhealing (ie, demonstrating granulation tissue,wound contraction and decreasing wounddepth) are described as colonized. That is, thebioburden is low enough that it does not impairthe wound’s ability to heal. The first step in themanagement of such wounds is surgical orexcisional debridement to restart the inflam-matory phase of the wound healing cycle.Most chronic wounds contain more than threespecies of microorganisms, which increases therisk of infection because they may develop syn-ergies with each other (33,53–55). In woundsthat are infected with multiple species, distin-guishing which is the causative organism maybe difficult. In the absence of true quantitativecultures, immediate broad-spectrum antibioticcoverage and treatment are warranted.
Critically colonized woundsThe term critically colonized was introducedto describe a wound with a level of bacterialburden between the categories of colonizedand infected. Chronic wounds, stalled due tohigh bacterial bioburden, could be consideredcritically colonized. This relatively new classi-fication, first introduced in 1996 by Davis (56),has been the source of critical comment buthas gained increasing acceptance. The termhas become synonymous with locally infected.Both describe wounds that do not heal but maynot display classic local signs of infection (eg,erythema, warmth, pain, etc) (3,4). Althoughthese wounds do not demonstrate the normalhost responses to infection, they still contain amicrobiological impairment to healing.
Critically colonized wounds are at veryhigh risk to become infected. In addition, aconfounding factor in the stalling process maybe the presence of biofilms, which can give thewound a healthy pink appearance even thoughthe wound may be harboring large colonies ofbacteria (38–40,57,58).
Infected woundsInfection occurs when there is a histologicaldemonstration of tissue invasion by organ-isms and a subsequent host response (59,60).Infected wounds may demonstrate any of theclassic clinical signs of infection (Table 2). Thetype and pathogenicity of the organisms maysometimes be as important as the quantity
of organisms in increasing the risk of infec-tion (55,61).
The wound assessment algorithm (Figure 1)defines critically colonized wounds as havingbiofilm present with early local infection ofsoft tissue. Infected wounds, by contrast,have biofilm present with soft tissue infectionand periwound extension. When infectionpenetrates to deeper levels, it is importantto rule out the spread of infection and/ornecrosis along the anatomic planes. Withextensive or persisting infection, a return tothe operating room for repeated thoroughdebridements is warranted until the infectionis controlled in the wound. If osteomyelitis issuspected, devitalized tissue must be debridedand appropriate antibiotic therapy initiated.
PREREQUISITES FOR USINGNPWT/ROCF IN INFECTED WOUNDSThe panel established three important pre-requisites before initiating NPWT/ROCF oncritically colonized or infected wounds: 1) thepatient is free of most systemic signs of grossinfection; 2) all necrotic tissue is debrided andabscesses are drained in the wound; and 3) thewound has adequate perfusion (necrosis canoccur when negative pressure is applied onan ischemic wound). If there is any doubt, re-examine the wound in 12-24 hours before start-ing NPWT/ROCF. Sound clinical judgment isnecessary before placement of NPWT/ROCFand usage should always be in combinationwith good medical and wound care practices.
PRE-TREATING AND MONITORINGINFECTED WOUNDSIn deep wound infection, NPWT/ROCFshould always be used in combination withantibiotics after having obtained a bacterialswab pre- or intraoperatively to avoid theconsequences of bacteremia (62). Immediateinitiation of empiric, broad-spectrum antibiotictreatment at presentation of infection is rec-ommended, followed by antibiotics to whichthe cultured microorganisms are sensitive onceculture results are received (63). A six-weekantibiotic treatment course when treating spinewound infections is commonly reported in theliterature (63,64).
All infected wounds should be debrideduntil only normal, soft, and well-vascularized
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 7

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
Table 3 NPWT/ROCF systems: contraindications, warnings and precautions recommended by the panel*
CONTRAINDICATIONS WARNINGS PRECAUTIONS
Gross infection If bleeding develops, discontinue therapy Exposed blood vessels, nerves or organs must beprotected using overlying fascia, tissue, orother protective barrier
Sepsis Protect vessels and organs (cover withthick layers of natural tissue or meshednon-adherent material)
Extreme care must be taken in the presence ofexisting or potential bleeding problems
Recurrent deep wound infection Use therapy cautiously in presence ofinfected blood vessels
Bone fragments or sharp edges that couldpuncture protective barriers, vessels, or organsshould be managed by debriding sharp edges
Presence of a pseudoaneurysm Smooth and cover any residual sharpedges to decrease risk of serious orfatal injury
Extreme care must be taken to protect vascularanastomoses, including coronary artery bypassgrafts, or weakened, irradiated, or suturedblood vessels or organs
Malignancy Monitor hemostasis, anticoagulants, andplatelet aggregation inhibitors
Lack of local wound hemostasis Monitor infected wounds closely; mayrequire more frequent dressingchanges than non-infected wounds
Untreated osteomyelitis NPWT/ROCF-silver is not intended toreplace use of systemic therapy
Unprotected vascularanastomoses
Foam placement directly overweakened or irradiated vessels
*This table does not necessarily reflect the contraindications, warnings, and precautions provided in the manufacturer’s labeling.
tissue remains. NPWT/ROCF should be imple-mented as early as possible after surgi-cal debridement (62). The wound should beassessed at each dressing change in a closelymonitored health care setting and under thesupervision of an experienced wound care clin-ician. Although manufacturer guidelines rec-ommend dressing changes 48–72 hours (65),reports in the literature cite periods of 1 to4 days between dressing changes, dependingon type and location of infected wound. Permanufacturer’s guidelines, infected woundsshould be monitored closely and may requiremore frequent dressing changes than non-infected wounds (65).
CONTRAINDICATIONS,PRECAUTIONS AND REPORTEDCOMPLICATIONSCaution should be exercised in all cases ofwound infection. Based on literature and panelconsensus, NPWT/ROCF should not be usedin the presence of gross infection, sepsis orrecurrent infection. Contraindications, warn-ings, and precautions for use of NPWT/ROCFas provided by the panel are summarized inTable 3.
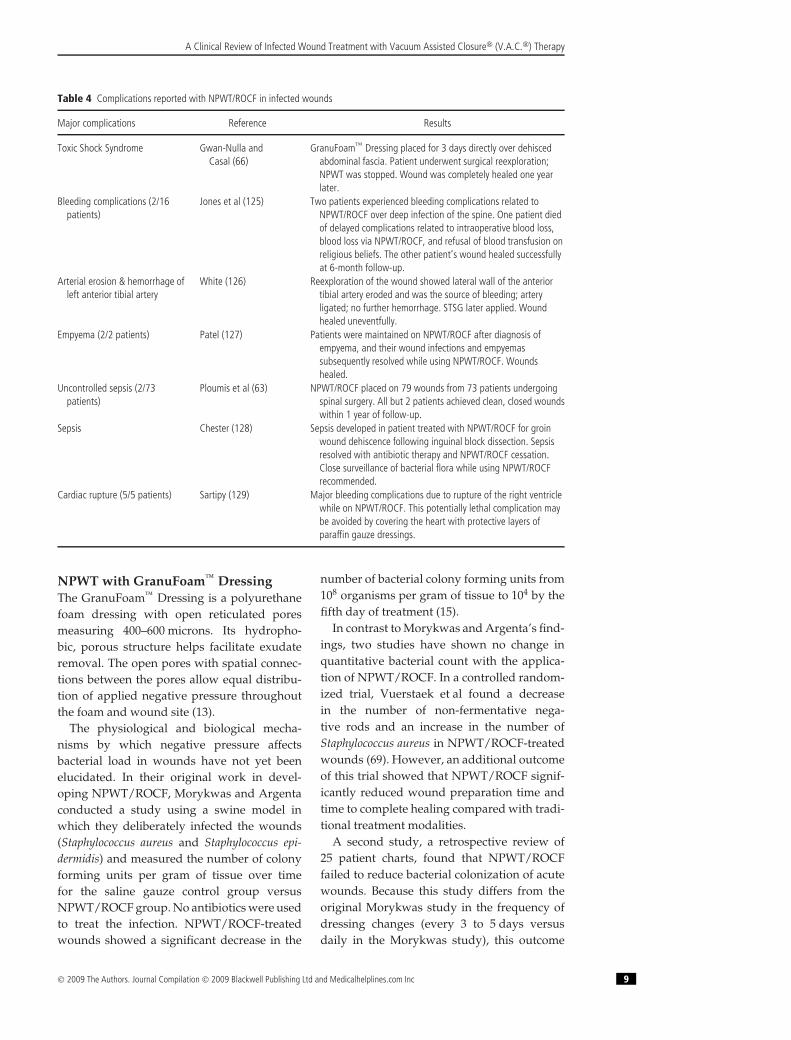
The majority of reported complications(Table 4) reflect inadequate protection ofexposed vital structures. One report docu-ments the use of NPWT/ROCF in an infectedwound that led to toxic shock syndrome (66).This patient was managed with NPWT/ROCFthat had been in place for three days directlyover dehisced abdominal fascia. The authorsstated that the dressing may have providedan environment that enhanced proliferationor elaboration of the toxigenic Staphylococcus.Another contributing factor may have beenthat there was no protective layer betweenthe exposed abdominal structures and thefoam. The importance of protecting all exposedabdominal or neurovascular structures under-neath the foam is detailed in recommendedguidelines for NPWT/ROCF use (44,67,68).
SELECTING AN NPWT/ROCFMODALITYThe following are brief descriptions, literaturereviews and panel recommendations to assistclinicians in using each type of NPWT/ROCFmodality for the management of criticallycolonized or infected wounds (Figure 1).
8 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
Table 4 Complications reported with NPWT/ROCF in infected wounds
Major complications Reference Results
Toxic Shock Syndrome Gwan-Nulla andCasal (66)
GranuFoam™ Dressing placed for 3 days directly over dehiscedabdominal fascia. Patient underwent surgical reexploration;NPWT was stopped. Wound was completely healed one yearlater.
Bleeding complications (2/16patients)
Jones et al (125) Two patients experienced bleeding complications related toNPWT/ROCF over deep infection of the spine. One patient diedof delayed complications related to intraoperative blood loss,blood loss via NPWT/ROCF, and refusal of blood transfusion onreligious beliefs. The other patient’s wound healed successfullyat 6-month follow-up.
Arterial erosion & hemorrhage ofleft anterior tibial artery
White (126) Reexploration of the wound showed lateral wall of the anteriortibial artery eroded and was the source of bleeding; arteryligated; no further hemorrhage. STSG later applied. Woundhealed uneventfully.
Empyema (2/2 patients) Patel (127) Patients were maintained on NPWT/ROCF after diagnosis ofempyema, and their wound infections and empyemassubsequently resolved while using NPWT/ROCF. Woundshealed.
Uncontrolled sepsis (2/73patients)
Ploumis et al (63) NPWT/ROCF placed on 79 wounds from 73 patients undergoingspinal surgery. All but 2 patients achieved clean, closed woundswithin 1 year of follow-up.
Sepsis Chester (128) Sepsis developed in patient treated with NPWT/ROCF for groinwound dehiscence following inguinal block dissection. Sepsisresolved with antibiotic therapy and NPWT/ROCF cessation.Close surveillance of bacterial flora while using NPWT/ROCFrecommended.
Cardiac rupture (5/5 patients) Sartipy (129) Major bleeding complications due to rupture of the right ventriclewhile on NPWT/ROCF. This potentially lethal complication maybe avoided by covering the heart with protective layers ofparaffin gauze dressings.
NPWT with GranuFoam™ DressingThe GranuFoam™ Dressing is a polyurethanefoam dressing with open reticulated poresmeasuring 400–600 microns. Its hydropho-bic, porous structure helps facilitate exudateremoval. The open pores with spatial connec-tions between the pores allow equal distribu-tion of applied negative pressure throughoutthe foam and wound site (13).
The physiological and biological mecha-nisms by which negative pressure affectsbacterial load in wounds have not yet beenelucidated. In their original work in devel-oping NPWT/ROCF, Morykwas and Argentaconducted a study using a swine model inwhich they deliberately infected the wounds(Staphylococcus aureus and Staphylococcus epi-dermidis) and measured the number of colonyforming units per gram of tissue over timefor the saline gauze control group versusNPWT/ROCF group. No antibiotics were usedto treat the infection. NPWT/ROCF-treatedwounds showed a significant decrease in the
number of bacterial colony forming units from108 organisms per gram of tissue to 104 by thefifth day of treatment (15).
In contrast to Morykwas and Argenta’s find-ings, two studies have shown no change inquantitative bacterial count with the applica-tion of NPWT/ROCF. In a controlled random-ized trial, Vuerstaek et al found a decreasein the number of non-fermentative nega-tive rods and an increase in the number ofStaphylococcus aureus in NPWT/ROCF-treatedwounds (69). However, an additional outcomeof this trial showed that NPWT/ROCF signif-icantly reduced wound preparation time andtime to complete healing compared with tradi-tional treatment modalities.
A second study, a retrospective review of25 patient charts, found that NPWT/ROCFfailed to reduce bacterial colonization of acutewounds. Because this study differs from theoriginal Morykwas study in the frequency ofdressing changes (every 3 to 5 days versusdaily in the Morykwas study), this outcome
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 9

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
may be more a reflection of frequency of dress-ing changes than of bioburden reduction (70).Further research is needed in this area. Interest-ingly, all wounds in both studies did progressto complete closure in a significantly acceler-ated time frame, despite the bacteria levels.These findings are further supported by aprospective randomized clinical trial in whichMoues et al found a significant decrease in thenumber of non-fermentative negative rods, yeta significant increase in the number of S. aureusin NPWT/ROCF-treated wounds versus moistgauze therapy. The total quantitative bacte-rial load was generally stable in both groups.However, the study showed a positive effect ofNPWT/ROCF on wound healing, based on sig-nificant reduction of wound surface area (71).
A Medline search using the terms ‘‘infected’’and ‘‘vacuum assisted closure’’ in combinationwith ‘‘sternal wound’’, ‘‘abdominal wound’’,‘‘extremity wound’’, ‘‘groin wound’’, ‘‘spinalwound’’ or ‘‘necrotizing fasciitis’’ yieldedover 100 publications focused on the use ofNPWT/ROCF in infected wounds. The vastmajority of these publications describe theeffective use of NPWT/ROCF within a smallto medium-sized, uncontrolled cohort. Studiesthat describe complications in NPWT/ROCF-treated infected wounds are described inTable 4. Although more prospective random-ized studies are needed to validate hypotheses,the volume of positive anecdotal evidence iscompelling and demonstrates wide use of thistherapy in diverse infected wound types.
Successful management of critically colo-nized and infected lower extremity woundswith NPWT/ROCF has also been documentedin the literature (24,67,72–74). In a series of 77Iraqi patients with 88 NPWT/ROCF-treatedhigh-energy soft tissue combat wounds, theoverall wound complication and infectionrates were 0%, compared to an anecdo-tal infection rate of 80% prior to introduc-tion of NPWT/ROCF treatment. The authorsattributed the results to the closed environ-ment of the NPWT/ROCF, which protects thewound from the ward environment, isolatesthe tissue injury, and keeps the wound cleanand free of exudates (75).
GranuFoam™ Dressing is used by itself inthe majority of the studies, although occa-sionally it is used in tandem with otherantibacterial products. Song et al has reportedon the use of GranuFoam™ Dressing over
a silver coated antimicrobial barrier dress-ing in temporizing complicated mediastinitiswounds (76). Other case reports have docu-mented successful use of silver contact layerdressings between the wound or skin graft andthe GranuFoam™ Dressing (77–80). However,in these cases, microdeformational changeswithin the wound that are expected withNPWT/ROCF could be limited by the lackof direct GranuFoam™ Dressing contact withthe wound surface.
Panel recommendationsThe panel recommended use of the Granu-Foam™ Dressing in contaminated or colonizedshallow wounds with no exposed bone orforeign body. It can also be used either inwounds with low risk of infection or in infectedwounds, which can be seen in the algorithm inFigure 1.
The majority of studies report that NPWT/ROCF is effective in the management of colo-nized or infected wounds. Our review revealedrelatively few major complications (Table 4),given the extensive use of NPWT/ROCF.This is consistent with the experience ofall panel members who noted a reductionin clinical signs of infection with use ofNPWT/ROCF in most colonized and infectedwounds. Although the anecdotal evidence ispositive and encouraging, there is a growingneed for further controlled research in this areaof bioburden reduction using NPWT/ROCF.Because of the complexities of wound heal-ing, measuring bacteria and developing well-designed prospective wound studies, thereremains a paucity of controlled evidencefrom which to draw conclusions regard-ing NPWT/ROCF and bacterial clearance.As applications for the therapy expand intoincreasingly complex wounds at high riskfor deep infection, there is considerably moreto learn and understand about the effect ofNPWT/ROCF on wound bioburden.
NPWT with GranuFoam Silver™
DressingThe GranuFoam Silver™ Dressing has all of theproperties of the original GranuFoam™ Dress-ing, but with the added feature that the foamhas been micro-bonded with metallic silver viaa proprietary metallization process (65). Withthe initiation of NPWT/ROCF-silver, exposureof the silver dressing to wound fluid causes oxi-dation of metallic silver to ionic silver, which
10 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
results in a 99.9% microorganism kill withinthe first thirty minutes in vitro. An in vitro sil-ver elution study showed that the GranuFoamSilver™ Dressing provides sustained releaseof ionic silver up to 72 hours (81). The reticu-lated open-cell structure of this dressing allowsfor compression and conformity to the entirewound surface. Exposure of the dressing towound fluid results in oxidation of metallicsilver to ionic silver, allowing the continuous,sustained release of silver ions that act as aneffective barrier to bacterial penetration (65).
Silver has been widely used in woundcare due to its demonstrated broad-spectrumantibacterial, antifungal and antiviral proper-ties. Its usage has increased during the pastfive years, perhaps because of the increasedlevel of bacterial resistance to traditional antibi-otics. For example, rates of methicillin-resistantStaphylococcus aureus (MRSA) increased fromabout 30% in 1989 to 50–60% in 1999 inmost institutions across the US (82). Althoughcoagulase-negative Staphylococci (CoNS) havebeen methicillin resistant for many years, theincidence of resistance has also increased from70% in 1989 to 90–95% in 2001–2002 (83).
In addition to MRSA and other grampositive cocci, and gram negative bacte-ria, especially Pseudomonas aeruginosa, Serratiamarcescens, Acinetobacter, Enterobacter, and Cit-robacter, are also problematic for cliniciansbecause of their frequent occurrence andtheir resistance patterns (84,85). For years,imipenem has been used to treat infectionscaused by multidrug-resistance organismsbecause of its efficacy and the lack of resis-tance to it. In 1988, the incidence of Pseudomonasresistance to imipenem was approximately 5%.During the last 5 years, resistance has risento approximately 11%. In intensive care unit(ICU) settings where it is used frequently, resis-tance has jumped to approximately 20% (86).
Unlike traditional antibiotics, ionic silver hasmultiple mechanisms of action, such as inhibit-ing cellular respiration, denaturing nucleicacids, and altering cellular membrane perme-ability (87,88). An adequate concentration ofsilver, in addition to its various mechanismsof action, makes it difficult for microorganismsto develop resistance because the numerousmutations they would have to undergo in orderto develop defense mechanisms against silver’svaried attack (5).
However, potential resistance to silverremains an important factor, and the adequatelevel of silver required for bioburden efficacyremains a controversial and complex issue.Some investigators believe that low levels areenough and others support the view that ahigher level of silver is necessary for sufficientbacterial kill. There is no global standardfor elution studies, and the literature variesdrastically, from 1.0 parts per million (ppm) toover 36 ppm, in the suggested requirements forthe proper kill levels (89). A key confoundingfactor is that all pathogens have multiplestrains and different strains require differentlevels of silver for kill. There are also significantdifferences in measurement methodology,which complicate data interpretation of silverlevels among various silver dressings.
The literature supports that silver releasemust be measured and sustained overtime (2,89,90). Research also indicates that theability of a silver-containing dressing to con-form to the contours of a wound is importantto reduce areas of non-contact where bacteriamay proliferate (91).
Some authors have suggested that higherlevels of silver delivered by agents such asnanocrystalline silver can be harmful to viablecells. This toxicity of silver is supported in sev-eral in vitro studies (92–95). However, the tox-icity is generally associated with frequent andhigh levels of silver used, and increasing evi-dence suggests that toxicity results observed inanimal and in vitro studies do not seem to playout in actual wounds.
In a study of silver-containing dressingsand their variable effects on cells, Cochraneet al used a fibroblast-seeded collagen gelmodel to evaluate the effect of seven differ-ent silver-containing antimicrobial dressingson fibroblast contraction and viability. Threeof the seven dressings demonstrated less than20% cell viability after 96 hours, compared toapproximately 70% viability for the remain-ing four dressings. The authors concluded thattoxicity effects of silver are based on numerouscharacteristics of a dressing, including its fluidhandling, antimicrobial, physical and chemicalproperties (95).
Gabriel et al reported on a prospec-tive case series of 5 consecutive patientswith infected wounds managed withNPWT/ROCF-silver (44). The dressing was indirect and complete contact with the wound
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 11

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
bed. The results showed that no complica-tions were experienced during therapy and allwounds progressed to primary or secondaryclosure. Specifically, the times to infectionclearance and wound closure were 7.00 ± 1.58and 19.20 ± 8.7 days, respectively.
In a case of a 4% total body surface area lowerextremity burn, the patient developed a woundinfection underneath a partial-thickness sheetgraft with an eventual 40% graft loss. Antibi-otics were initiated and on postoperative day22, NPWT/ROCF-silver was applied over asoft silicone wound contact layer. The woundwas completely re-epithelialized by day 9 ofNPWT use and re-grafting was avoided (96).
NPWT/ROCF-silver appears to offer suffi-cient antimicrobial effect and promote woundhealing. The positive outcomes are likely due toa combination of factors including lower non-toxic levels of silver release, optimal woundconformability, exudate removal in a non-traumatic fashion and the established bene-fits of NPWT/ROCF. It is important to notethat use of V.A.C GranuFoam Silver® is notintended to replace use of systemic therapy butto complement antibiotic treatment protocols.
Panel recommendationsBased on their experiences, panel memberssuggested that benefits of NPWT/ROCF-silverinclude antiseptic, antimicrobial propertieswithout the requirement of an additionaladjunctive silver layer. The properties of thesilver dressing may minimize tissue adher-ence to the foam, causing less pain duringdressing removal, compared to the originalNPWT/ROCF dressing. Some panel memberssuggested the use of NPWT/ROCF-silver fora broad range of wounds including cases ofcomplex, colonized, or infected wounds post-debridement, as well as in acute traumaticwounds for reduction of bacterial biobur-den. Some panel members preferred usingNPWT/ROCF-silver dressing in patients whohave severe comorbidities and a history ofchronic wound colonization to help reducethe risk of recurrent infection. Some panelmembers recommend that the silver dressingmay be considered for use with the follow-ing wound types or characteristics: partial-thickness burns, chronic wounds, exposedmesh, stalled wounds, exposed hardware,dehisced, diabetic ulcers, pressure ulcers (stageIII and IV), diabetic amputations, and split-thickness skin grafts (STSGs).
Caution should be exercised when usingsilver in wounds that show signs of cellulitis orsystemic infection, wounds that are colonizedwith fungus, patients with leucopoenia orwhen signs of possible side effects arepresent, such as erythema multiforme (97).Silver dressings should also not be used withsaline or papain-urea (which has since beenremoved from the market) debriding ointment.Saline may decrease the amount of silverreleased (97).
Interface layers are generally not recom-mended to be used between the wound and theV.A.C. GranuFoam Silver® Dressing since it isthe direct contact of the foam with the woundbed that induces micromechanical effects atthe dressing-to-tissue interface resulting intissue undulations and cellular microdeforma-tion (13). A non-adherent layer is needed onlyto protect exposed blood vessels, anastomaticsites, organs and nerves.
Judicious use of silver dressings is recom-mended. Duration of NPWT/ROCF-silver hasyet to be clearly defined and varies amongclinicians and with clinical presentation. Thepanel recommends evaluation of the treat-ment goals and reassessment of progressand changes in the wound after initiation oftreatment. Short-term use of silver-containingdressings until wound bioburden is con-trolled and wound healing progress has beenreported (41). Notable secondary signs andsymptoms of healing would include: changein odor, pain, color and quality of granula-tion tissue; reversal of stalling; and coverageof structures. Guidelines for duration are mul-tifaceted and should reflect response to treat-ment. As with any modality, if the wound isnot progressing within 1–2 weeks, reevaluationof treatment is warranted. After completingtreatment with NPWT/ROCF-silver, it maybe appropriate to switch back to NPWT withGranuFoam™ or V.A.C.® WhiteFoam Dress-ings for the duration of treatment.
NPWT with timed, automatedinstillation of fluidsWound irrigation is an integral step in themanagement of soft tissue injuries and openfractures, typically following debridement ofthe injured soft tissues. Several factors, includ-ing fluid type, fluid volume, and deliverymethod, must be considered prior to woundirrigation. While pulsed lavage is perhaps the
12 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
most common type of irrigation, high pressurepulsed lavage has been shown to be deleteriousto bone healing (98). Although the effect of highpressure irrigation systems on some woundsremains controversial, it is well accepted thatintermittent irrigation is a requirement toremove debris and adhered bacteria whendealing with heavily contaminated wounds.
V.A.C. Instill® Wound Therapy (NPWTwith instillation) was introduced to the USacute care market in 2003 as an evolution ofthe standard NPWT/ROCF. The instillationdevice combines the mechanisms of actionof the original NPWT/ROCF with timed,intermittent, gravity-fed delivery of an instilledtopical solution through a second ingresstube applied to the foam. Varying lengths ofsolution infusion and dwell times are set viathe microprocessor. NPWT with instillationis a low-pressure irrigation delivery systemindicated for patients who would benefit fromVacuum Assisted Closure® and controlleddelivery of topical wound treatment solutionsand suspensions over the wound bed (99,100).NPWT with instillation allows contaminatedwounds to be intermittently irrigated in anautomated fashion to help remove particulateand bacterial matter and facilitate closure (101).
Surgeons are familiar with the use of topicalantibiotics for wound irrigation, and most areaware of the controversy surrounding theirefficacy. No single ideal topical solution existsto treat all variations in bacterial colonization,wound types and host factors. An ideal agentwould have a broad spectrum of activity withno systemic absorption; it would be painless,inexpensive, nontoxic with minimal woundhealing interference, and would be approvedfor topical use by the US Food and DrugAdministration (FDA) (101).
Based on the manufacturer’s clinical guide-lines, NPWT with instillation is intended foruse with topical wound treatment solutions.Various topical agents (such as hydrogen per-oxide, which is contraindicated for use withNPWT with instillation) are not intended forextended tissue contact and must not be usedwith NPWT with instillation. If in doubt aboutthe appropriateness of using a particular solu-tion for NPWT with instillation, contact thesolution’s manufacturer about its suitabilityfor saturated topical wound irrigation in con-junction with exposure to polyurethane foam.Solutions should not be delivered in conflict
with solution manufacturer’s Instructions forUse or Prescribing Information (65).
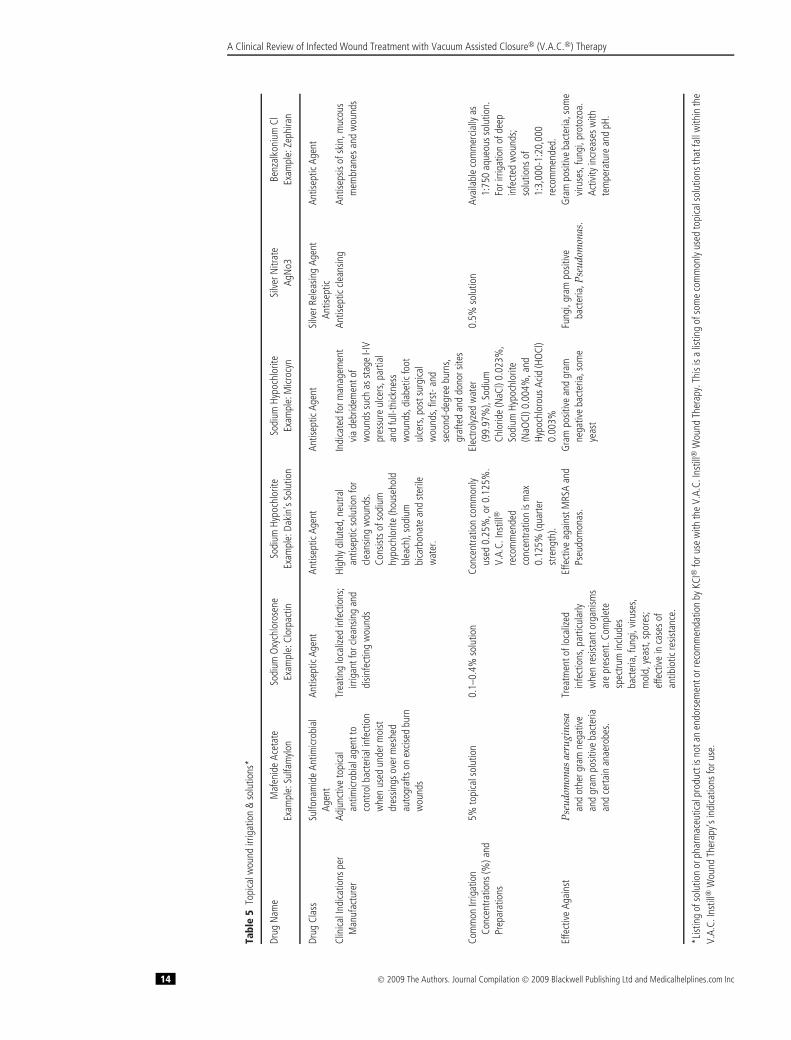
Choices among the short list of antisepticsthat are FDA approved (Table 5) for topicaluse in solution form can have potential draw-backs. Mafenide acetate is FDA approved foruse in a 5% solution form. This agent is broadlybacteriostatic against many gram positive andgram negative bacteria as well as some anaer-obes. However, the solution has been shown tobe systemically absorbed, and complications,such as metabolic acidosis, rare bone marrowdepression, and fatal hemolytic anemia withdisseminated intravascular coagulation, havebeen reported (102–105).
Silver nitrate 0.5% solution has been pro-posed as one solution for use with NPWT withinstillation (45,101). Silver nitrate 0.5% solutionis approved by the FDA and is bactericidalagainst panresistant bacteria. Silver nitrate hasa proven track record at many burn centersthroughout the US for the decolonization ofburn wounds prior to skin grafting (106–108).The solution is painless when applied to thewound and is not absorbed into the bloodstream, which has been demonstrated throughserum level tests (101). This solution does notdamage the components of the negative pres-sure dressing. The silver nitrate solution isprepared from lyophilized powder, which isreconstituted with sterile water. Pharmaceuti-cal grade ready-to-use 0.5% silver nitrate canalso be purchased (45).
Microcyn® Skin and Wound Cleanser (Ocu-lus Innovative Sciences, Petaluma, CA) withpreservatives is an FDA cleared topical woundirrigation solution that has been used success-fully with NPWT with instillation (109,110).It has demonstrated effectiveness by reduc-ing multiple microorganisms including MRSA,VRE, Pseudomonas, and Candida. It is non-irritating and non-cytotoxic with a shelf lifeof 24 months.
Instillation-vacuum techniques in treatinginfection have been described in Europethroughout the past two decades (111–114).Many of these studies have employed the instil-lation vacuum sealing technique, which involvestemporary implantation of the white polyvinylalcohol foam and connection to redon bottlesor an NPWT device and hand-administeredantiseptic or antibiotic instillation at regular,timed intervals. Unfortunately, review of theearlier European literature regarding vacuum
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 13
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
Tabl
e5
Topi
calw
ound
irrig
atio
n&
solu
tions
*
Drug
Nam
eM
afen
ide
Acet
ate
Sodi
umO
xych
loro
sene
Sodi
umHy
poch
lorit
eSo
dium
Hypo
chlo
rite
Silv
erN
itrat
eBe
nzal
koni
umCl
Exam
ple:
Sulfa
mylo
nEx
ampl
e:Cl
orpa
ctin
Exam
ple:
Daki
n’s
Solu
tion
Exam
ple:
Micr
ocyn
AgN
o3Ex
ampl
e:Ze
phira
n
Drug
Clas
sSu
lfona
mid
eAn
timicr
obia
lAg
ent
Antis
eptic
Agen
tAn
tisep
ticAg
ent
Antis
eptic
Agen
tSi
lver
Rele
asin
gAg
ent
Antis
eptic
Antis
eptic
Agen
t
Clin
icalI
ndica
tions
per
Man
ufac
ture
rAd
junc
tive
topi
cal
antim
icrob
iala
gent
toco
ntro
lbac
teria
linf
ectio
nw
hen
used
unde
rmoi
stdr
essin
gsov
erm
eshe
dau
togr
afts
onex
cised
burn
wou
nds
Trea
ting
loca
lized
infe
ctio
ns;
irrig
antf
orcle
ansin
gan
ddi
sinfe
ctin
gw
ound
s
High
lydi
lute
d,ne
utra
lan
tisep
ticso
lutio
nfo
rcle
ansin
gw
ound
s.Co
nsist
sof
sodi
umhy
poch
lorit
e(h
ouse
hold
blea
ch),
sodi
umbi
carb
onat
ean
dst
erile
wat
er.
Indi
cate
dfo
rman
agem
ent
via
debr
idem
ento
fw
ound
ssuc
has
stag
eI-I
Vpr
essu
reul
cers
,par
tial
and
full-
thick
ness
wou
nds,
diab
etic
foot
ulce
rs,p
osts
urgi
cal
wou
nds,
first
-and
seco
nd-d
egre
ebu
rns,
graf
ted
and
dono
rsite
s
Antis
eptic
clean
sing
Antis
epsis
ofsk
in,m
ucou
sm
embr
anes
and
wou
nds
Com
mon
Irrig
atio
nCo
ncen
tratio
ns(%
)and
Prep
arat
ions
5%to
pica
lsol
utio
n0.
1–0.
4%so
lutio
nCo
ncen
tratio
nco
mm
only
used
0.25
%,o
r0.1
25%
.V.
A.C.
Inst
ill®
reco
mm
ende
dco
ncen
tratio
nis
max
0.12
5%(q
uarte
rst
reng
th).
Elec
trolyz
edw
ater
(99.
97%
),So
dium
Chlo
ride
(NaC
l)0.
023%
,So
dium
Hypo
chlo
rite
(NaO
Cl)0
.004
%,a
ndHy
poch
loro
usAc
id(H
OCl
)0.
003%
0.5%
solu
tion
Avai
labl
eco
mm
ercia
llyas
1:75
0aq
ueou
ssol
utio
n.Fo
rirri
gatio
nof
deep
infe
cted
wou
nds;
solu
tions
of1:
3,00
0-1:
20,0
00re
com
men
ded.
Effe
ctiv
eAg
ains
tP
seud
omon
asae
rugi
nosa
and
othe
rgra
mne
gativ
ean
dgr
ampo
sitiv
eba
cter
iaan
dce
rtain
anae
robe
s.
Trea
tmen
tofl
ocal
ized
infe
ctio
ns,p
artic
ular
lyw
hen
resis
tant
orga
nism
sar
epr
esen
t.Co
mpl
ete
spec
trum
inclu
des
bact
eria
,fun
gi,v
iruse
s,m
old,
yeas
t,sp
ores
;ef
fect
ive
inca
ses
ofan
tibio
ticre
sista
nce.
Effe
ctiv
eag
ains
tMRS
Aan
dPs
eudo
mon
as.
Gra
mpo
sitiv
ean
dgr
amne
gativ
eba
cter
ia,s
ome
yeas
t
Fung
i,gr
ampo
sitiv
eba
cter
ia,P
seud
omon
as.
Gra
mpo
sitiv
eba
cter
ia,s
ome
viru
ses,
fung
i,pr
otoz
oa.
Activ
ityin
crea
sesw
ithte
mpe
ratu
rean
dpH
.
*List
ing
ofso
lutio
nor
phar
mac
eutic
alpr
oduc
tisn
otan
endo
rsem
ento
rrec
omm
enda
tion
byKC
I®fo
ruse
with
the
V.A.
C.In
still
®W
ound
Ther
apy.
This
isa
listin
gof
som
eco
mm
only
used
topi
cals
olut
ions
that
fall
with
inth
eV.
A.C.
Inst
ill®
Wou
ndTh
erap
y’si
ndica
tions
foru
se.
14 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
sealing was limited largely to abstracts as manyof the manuscripts were written in German.In a retrospective review of 27 patients withacute infection of bone and soft tissues, chronicosteomyelitis or chronic wounds treated withthis technique for 7 days, only one recurrenceof infection was reported during an average4.2 month follow-up time (115).
In the US, an initial review of the NPWTwith instillation device with case studies waspublished by Wolvos (2004) (99). In a pilotstudy of 5 patients, a variety of complexwounds were treated with NPWT and culture-directed antibiotics. Dilute lidocaine was com-bined with some of the irrigation solutions.All wounds that cultured positive for infectionprior to receiving NPWT with instillation hadfollow-up cultures that showed no growth oronly normal flora. Culture-directed antibioticwound irrigation appeared to decrease the bac-terial burden of infected wounds and changethe appearance to that of clean wounds. Inthe two cases that were being treated withtraditional NPWT, switching to NPWT withinstillation facilitated a clear improvement inwound clinical appearance and culture results.
Gabriel et al reported results of a prospectivecase series of 15 patients treated with NPWT-instillation compared to a retrospective histor-ical control of 15 patients treated with moistgauze wound care. Compared with the stan-dard moist wound care therapy control group,patients in the NPWT with instillation grouprequired fewer days of treatment, cleared ofclinical infection earlier, had wounds closeearlier and had fewer in-hospital stay days.They noted that the addition of an instilled,irrigating fluid to NPWT/ROCF provided aunique autolytic and mechanical debridementeffect that appeared to enhance wound heal-ing over traditional NPWT/ROCF for com-plex, infected wounds. The authors recom-mended NPWT with instillation for woundsthat could benefit from automated intermittenthydro-debridement, such as acute traumaticwounds or acutely debrided wounds becauseof infected soft tissue (45).
In a series of 5 post-surgical diabetic footwounds treated with NPWT with instillation,Bernstein et al noted a decrease in hospital stayand amputation rate with the instillation tech-nique (101). The authors noted the additionof instilled solutions lowered viscosity ofthe wound fluid and allowed more efficient
removal into the canister. The system wasfound to be efficacious in wounds with highlevels of exudate and slough content. Benefitsof the therapy included aiding in withdrawingremaining infectious material from the wound,enhancing granulation tissue formation, main-taining a moist wound environment, andperiodically bathing the wound with antibi-otic solution may help to prevent contiguousosteomyelitis or desiccation of exposed bone.
A recent retrospective, case-control cohortstudy compared outcomes of patients withosteomyelitis of the pelvis or lower extremitytreated with NPWT with instillation (polyhex-anide antiseptic solution) and white polyvinylalcohol foam versus gentamicin polymethyl-methacrylate beads and long-term intravenousantibiotics (116). The rate of recurrence of infec-tion was 3/30 in the Instillation group versus55/93 in the Bead group (p< 0.0001). The dura-tion of hospital stay and number of surgicalprocedures were also less in the Instillationgroup. The authors concluded that in posttrau-matic osteomyelitis, NPWT with instillationreduced the need for repeated surgical inter-ventions compared to implanted gentamicinpolymethylmethacrylate beads (116).
Brem et al reported use of NPWT withinstillation on a polytraumatized patient whosuffered a third-degree open femur defect frac-ture with substantial loss of the lateral femoralmuscles and significant disruption of the softtissue (117). Critical infection was confirmedand NPWT with instillation was initiated as alast resort to salvage the limb. Lavasept (avail-able outside of the US) was instilled for 6 daysand the number of organisms was significantlyreduced. The patient continued with NPWTwithout instillation and was ultimately dis-charged with an intact leg with good function.
Panel recommendationsThe panel-recommended indications forNPWT with instillation are detailed in Table 6.Topical solutions that can be used with NPWTwith instillation include cleansers, antibiotics,antifungals, antiseptics and anesthetics. Thesystem is intended for use with aqueous solu-tions in a physiologic pH range defined as6.0–7.4 (101).
A deeper wound with exposed bone ora foreign body (ie, hardware), or appearinggrossly contaminated, may require surgical
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 15

A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
Table 6 Recommendations for use of NPWT with instillation
• *Diffuse or extensive osteomyelitis is encountered or if large areas of post-debridement bone or joint are present• *Postoperative infection following total joint arthroplasty• *A wound is suspected to be critically colonized and subsequently has become stalled, yet needs continued NPWT• *An alternative to antibiotic-impregnated beads is needed• †Wounds at a high risk for a major amputation due to infection• †Open fracture wounds to prevent wound infections or osteomyelitis• †To decrease the viscosity of wound exudate• †Exposed hardware or foreign bodies including mesh• †Infected wounds that remain infected after a trial of NPWT/ROCF
*Adapted from Bernstein et al (101) †Tom Wolvos, MD, FACS, e-mail communication, July 21, 2009
irrigation. Some of the panel members recom-mend that the wound may benefit from NPWTwith instillation with antiseptic solutions,such as 0.5% silver nitrate, Microcyn® orfrom NPWT/ROCF-silver with regular ster-ile water irrigation. Aggressive brushing ofexposed hardware and continuous irriga-tion with an antiseptic may be effective indecreasing biofilm formation. However, ran-domized, controlled studies are warranted.Once there is appropriate wound progression,NPWT with instillation can be converted toNPWT with GranuFoam Silver™ or regularGranuFoam™ Dressing.
In critically colonized wounds with earlylocal infection, NPWT with instillation of anantiseptic solution is recommended (Figure 1).Some panel members recommended that oncewound exudate and slough levels are min-imized and hydro-debridement is no longernecessary, NPWT with instillation can beconverted to NPWT/ROCF with GranuFoamSilver™ or regular GranuFoam™ Dressing. Fol-lowing short-term treatment, critically colo-nized wounds have a strong probability ofreverting to a chronic state. Therefore, somepanel members suggested that these woundsshould be treated with a broad-spectrum anti-septic, GranuFoam Silver™ Dressings, or regu-lar GranuFoam™ Dressings until full closure isobtained.
Infected wounds may require aggressiveserial debridements and may require multiplereturns to the operating room. Once allnecrotic tissue and abscesses are removedand clinical signs are improving, NPWT withinstillation of an antiseptic may be initiated.Some panel members suggest the use ofNPWT with instillation using a GranuFoamSilver™ Dressing for both superficial anddeep infected wounds to aggressively addressinfection. As with critically colonized wounds,
infected wounds should also be managed witha broad-spectrum antiseptic modality until fullclosure is obtained.
When using a silver nitrate solution for instil-lation, it is important that the pharmacist pre-pare the solution carefully, as solutions greaterthan 0.5% can denature proteins (93,118). Silvernitrate at a concentration of 5% to 10% pro-duces chemical cautery. Minor complicationsof the use of silver nitrate include staining ofbed linens and instability to light. Silver nitrateis hypotonic and not an ideal environment forhealing tissue; it should be used for short-termuse only.
Specifically, NPWT with instillation couldhave a potential role in treating postoperativeinfection following total joint arthroplasty, aserious and devastating complication. Antibi-otic beads have been a mainstay of prac-tice for dead-space management in infectedwounds involving lower and upper extrem-ities (119–122). Newer bio-absorbable carriersof antibiotic-containing hyaluronic acid gel areshowing promise for prophylactic treatment ortreatment of an actual deep infection follow-ing total joint arthroplasty in rabbit and mousemodels (119). To develop an effective treat-ment for this complication, various attemptsat the instillation of antibiotic solution into awound have been made with either passiveegress through the suture line or active suctionvia an exterior pump (123,124).
CONCLUSIONV.A.C.® Therapy, with its newer adjuncts, maybe an optimal initial dressing after debride-ment of infected wounds because of its com-bined effects of V.A.C.® Therapy mechanisms,antibacterial treatment and irrigation. Thecombination therapy has enabled the panelmembers to temporize wounds, which allowthe reconstructive surgeon and the patient time
16 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
before committing to a definite reconstruction.In addition, utilizing the concept of the recon-structive ladder, this therapy has enabled sur-geons to perform less complex reconstructionsof major soft tissue defects. This ultimatelyreduces wound morbidity and decreases anes-thesia time – all of which are better toleratedby the patient.
The important point in the managementof the described wounds is that bacterialcontamination is seen in any open wound,even though low bacterial colony units arereported. All bacteria, whether in an acute orchronic wound, or in a contaminated versusa colonized wound, will produce virulencefactors (eg, exotoxins, endotoxins, and MMPs),all of which have deleterious effects to wound
healing. They decrease the ability of the woundto progress to the next stage and halt itin a chronic inflammatory phase. Thereforethe removal of the cytotoxic cytokines viaV.A.C.® Therapy and the decrease of thebacterial bioburden with the use of antisepticmodalities (eg, V.A.C. Instill®Wound Therapyor GranuFoam Silver™), synergistically help inmanaging these difficult to treat wounds.
ACKNOWLEDGEMENTSWe would like to thank Andrea Adams, KarenBeach, Alice Goodwin, Ricardo R Martinez andJulissa Ramos for their editorial assistance andpreparation of this manuscript.
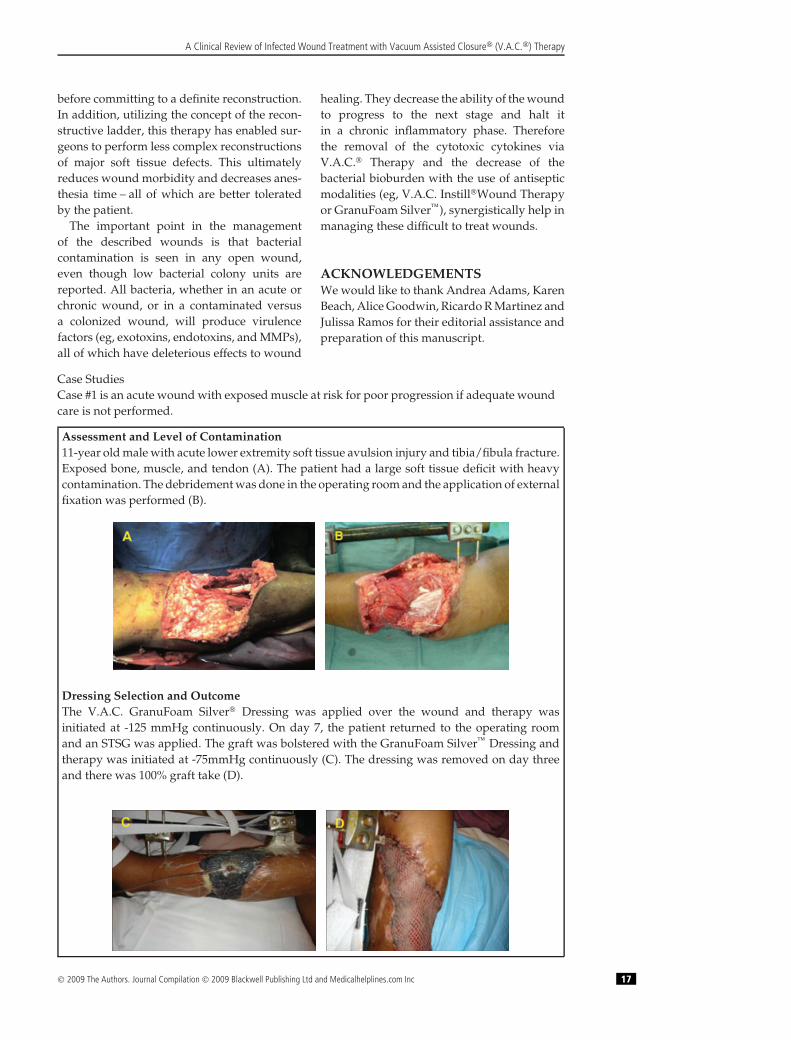
Case StudiesCase #1 is an acute wound with exposed muscle at risk for poor progression if adequate woundcare is not performed.
Assessment and Level of Contamination11-year old male with acute lower extremity soft tissue avulsion injury and tibia/fibula fracture.Exposed bone, muscle, and tendon (A). The patient had a large soft tissue deficit with heavycontamination. The debridement was done in the operating room and the application of externalfixation was performed (B).
Dressing Selection and OutcomeThe V.A.C. GranuFoam Silver® Dressing was applied over the wound and therapy wasinitiated at -125 mmHg continuously. On day 7, the patient returned to the operating roomand an STSG was applied. The graft was bolstered with the GranuFoam Silver™ Dressing andtherapy was initiated at -75mmHg continuously (C). The dressing was removed on day threeand there was 100% graft take (D).
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 17
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
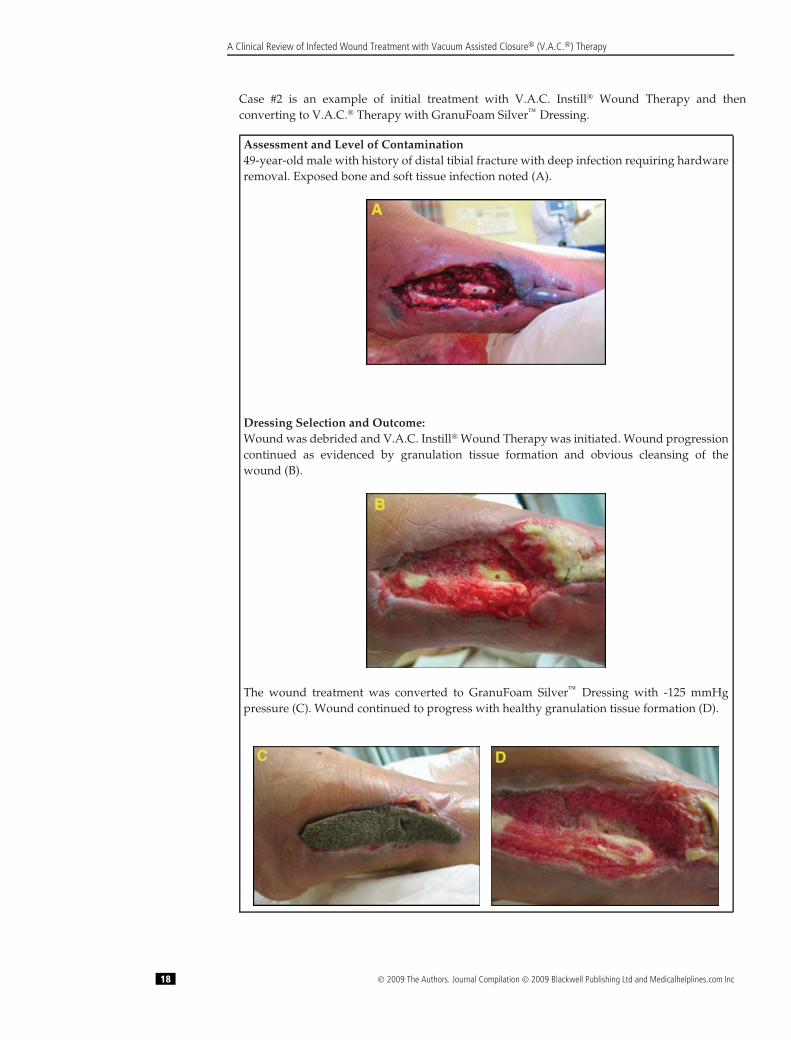
Case #2 is an example of initial treatment with V.A.C. Instill® Wound Therapy and thenconverting to V.A.C.® Therapy with GranuFoam Silver™ Dressing.
Assessment and Level of Contamination49-year-old male with history of distal tibial fracture with deep infection requiring hardwareremoval. Exposed bone and soft tissue infection noted (A).
Dressing Selection and Outcome:Wound was debrided and V.A.C. Instill® Wound Therapy was initiated. Wound progressioncontinued as evidenced by granulation tissue formation and obvious cleansing of thewound (B).
The wound treatment was converted to GranuFoam Silver™ Dressing with -125 mmHgpressure (C). Wound continued to progress with healthy granulation tissue formation (D).
18 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
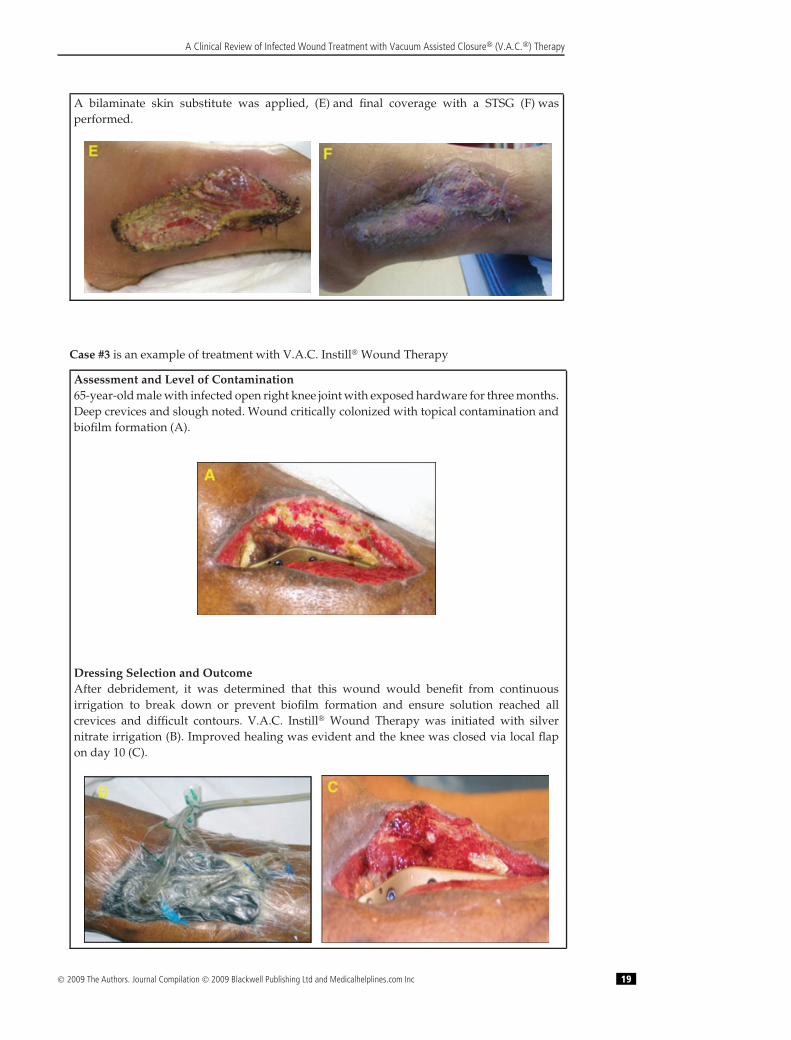
A bilaminate skin substitute was applied, (E) and final coverage with a STSG (F) wasperformed.
Case #3 is an example of treatment with V.A.C. Instill® Wound Therapy
Assessment and Level of Contamination65-year-old male with infected open right knee joint with exposed hardware for three months.Deep crevices and slough noted. Wound critically colonized with topical contamination andbiofilm formation (A).
Dressing Selection and OutcomeAfter debridement, it was determined that this wound would benefit from continuousirrigation to break down or prevent biofilm formation and ensure solution reached allcrevices and difficult contours. V.A.C. Instill® Wound Therapy was initiated with silvernitrate irrigation (B). Improved healing was evident and the knee was closed via local flapon day 10 (C).
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 19
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
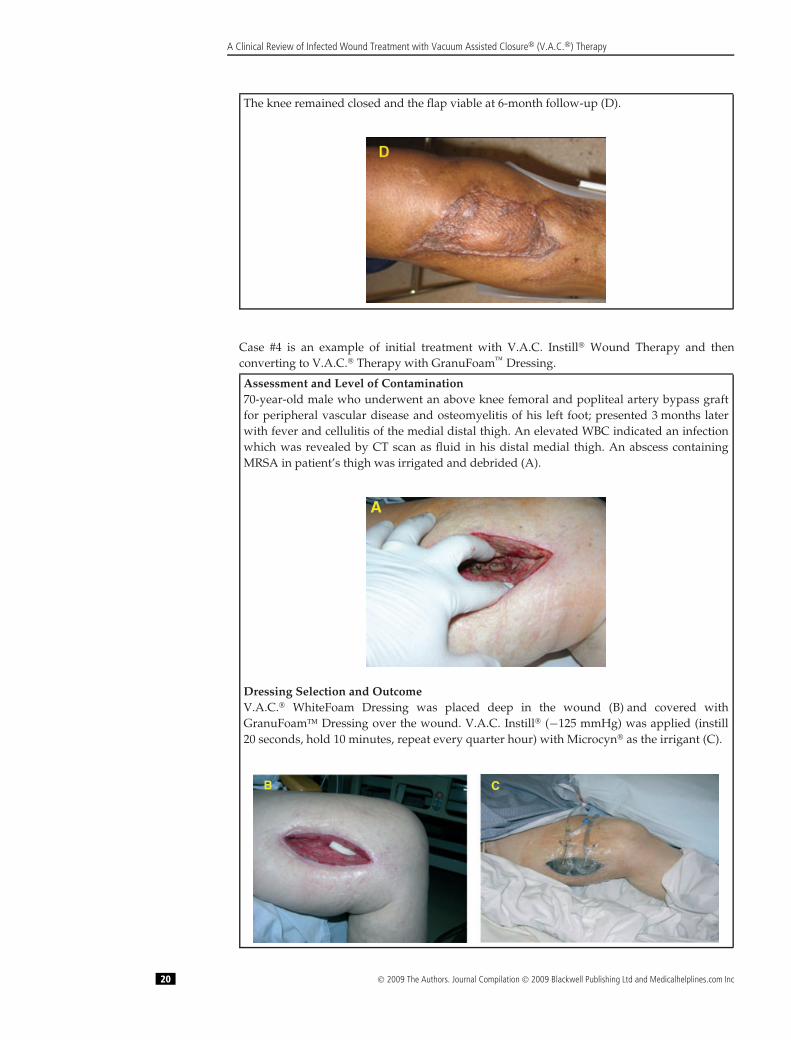
The knee remained closed and the flap viable at 6-month follow-up (D).
Case #4 is an example of initial treatment with V.A.C. Instill® Wound Therapy and thenconverting to V.A.C.® Therapy with GranuFoam™ Dressing.
Assessment and Level of Contamination70-year-old male who underwent an above knee femoral and popliteal artery bypass graftfor peripheral vascular disease and osteomyelitis of his left foot; presented 3 months laterwith fever and cellulitis of the medial distal thigh. An elevated WBC indicated an infectionwhich was revealed by CT scan as fluid in his distal medial thigh. An abscess containingMRSA in patient’s thigh was irrigated and debrided (A).
A
Dressing Selection and OutcomeV.A.C.® WhiteFoam Dressing was placed deep in the wound (B) and covered withGranuFoam™ Dressing over the wound. V.A.C. Instill® (−125 mmHg) was applied (instill20 seconds, hold 10 minutes, repeat every quarter hour) with Microcyn® as the irrigant (C).
C B
20 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
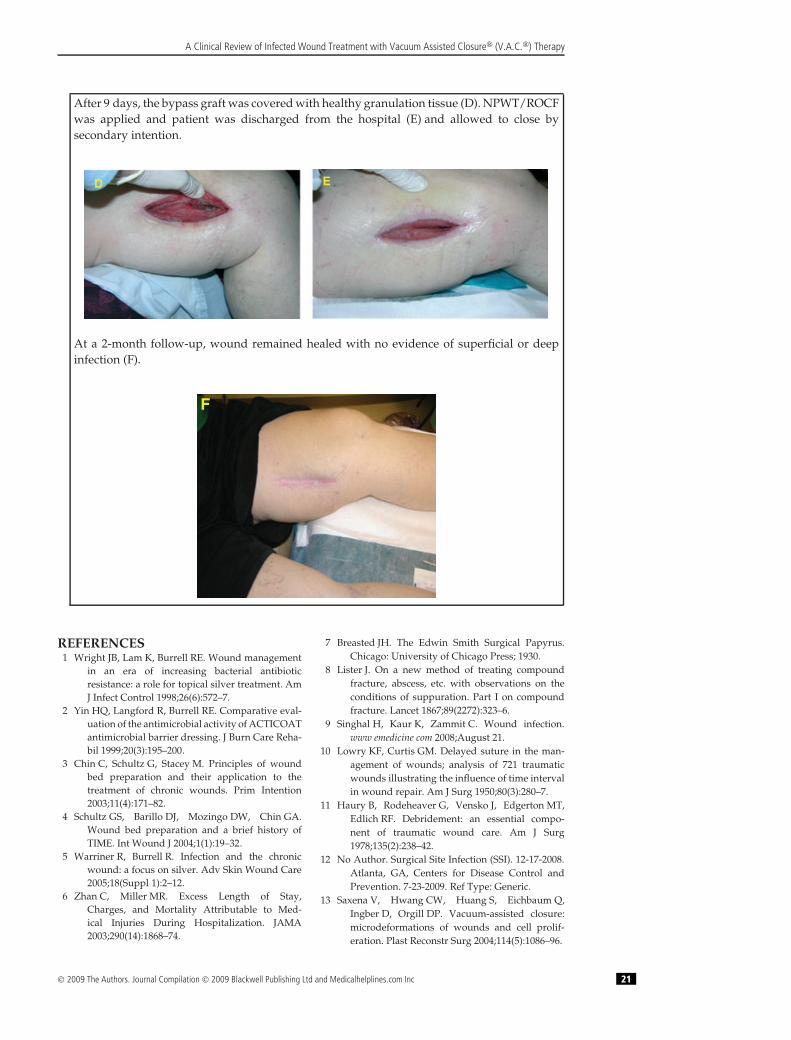
After 9 days, the bypass graft was covered with healthy granulation tissue (D). NPWT/ROCFwas applied and patient was discharged from the hospital (E) and allowed to close bysecondary intention.
D E
At a 2-month follow-up, wound remained healed with no evidence of superficial or deepinfection (F).
F
REFERENCES1 Wright JB, Lam K, Burrell RE. Wound management
in an era of increasing bacterial antibioticresistance: a role for topical silver treatment. AmJ Infect Control 1998;26(6):572–7.
2 Yin HQ, Langford R, Burrell RE. Comparative eval-uation of the antimicrobial activity of ACTICOATantimicrobial barrier dressing. J Burn Care Reha-bil 1999;20(3):195–200.
3 Chin C, Schultz G, Stacey M. Principles of woundbed preparation and their application to thetreatment of chronic wounds. Prim Intention2003;11(4):171–82.
4 Schultz GS, Barillo DJ, Mozingo DW, Chin GA.Wound bed preparation and a brief history ofTIME. Int Wound J 2004;1(1):19–32.
5 Warriner R, Burrell R. Infection and the chronicwound: a focus on silver. Adv Skin Wound Care2005;18(Suppl 1):2–12.
6 Zhan C, Miller MR. Excess Length of Stay,Charges, and Mortality Attributable to Med-ical Injuries During Hospitalization. JAMA2003;290(14):1868–74.
7 Breasted JH. The Edwin Smith Surgical Papyrus.Chicago: University of Chicago Press; 1930.
8 Lister J. On a new method of treating compoundfracture, abscess, etc. with observations on theconditions of suppuration. Part I on compoundfracture. Lancet 1867;89(2272):323–6.
9 Singhal H, Kaur K, Zammit C. Wound infection.www emedicine com 2008;August 21.
10 Lowry KF, Curtis GM. Delayed suture in the man-agement of wounds; analysis of 721 traumaticwounds illustrating the influence of time intervalin wound repair. Am J Surg 1950;80(3):280–7.
11 Haury B, Rodeheaver G, Vensko J, Edgerton MT,Edlich RF. Debridement: an essential compo-nent of traumatic wound care. Am J Surg1978;135(2):238–42.
12 No Author. Surgical Site Infection (SSI). 12-17-2008.Atlanta, GA, Centers for Disease Control andPrevention. 7-23-2009. Ref Type: Generic.
13 Saxena V, Hwang CW, Huang S, Eichbaum Q,Ingber D, Orgill DP. Vacuum-assisted closure:microdeformations of wounds and cell prolif-eration. Plast Reconstr Surg 2004;114(5):1086–96.
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 21
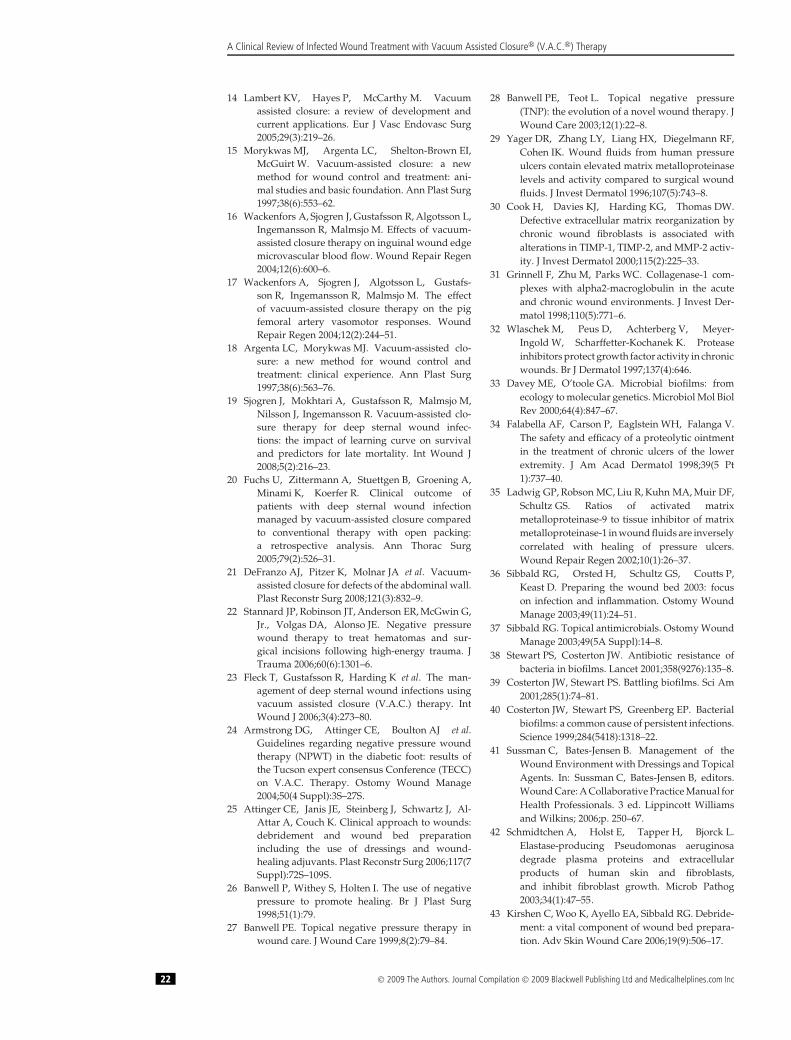
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
14 Lambert KV, Hayes P, McCarthy M. Vacuumassisted closure: a review of development andcurrent applications. Eur J Vasc Endovasc Surg2005;29(3):219–26.
15 Morykwas MJ, Argenta LC, Shelton-Brown EI,McGuirt W. Vacuum-assisted closure: a newmethod for wound control and treatment: ani-mal studies and basic foundation. Ann Plast Surg1997;38(6):553–62.
16 Wackenfors A, Sjogren J, Gustafsson R, Algotsson L,Ingemansson R, Malmsjo M. Effects of vacuum-assisted closure therapy on inguinal wound edgemicrovascular blood flow. Wound Repair Regen2004;12(6):600–6.
17 Wackenfors A, Sjogren J, Algotsson L, Gustafs-son R, Ingemansson R, Malmsjo M. The effectof vacuum-assisted closure therapy on the pigfemoral artery vasomotor responses. WoundRepair Regen 2004;12(2):244–51.
18 Argenta LC, Morykwas MJ. Vacuum-assisted clo-sure: a new method for wound control andtreatment: clinical experience. Ann Plast Surg1997;38(6):563–76.
19 Sjogren J, Mokhtari A, Gustafsson R, Malmsjo M,Nilsson J, Ingemansson R. Vacuum-assisted clo-sure therapy for deep sternal wound infec-tions: the impact of learning curve on survivaland predictors for late mortality. Int Wound J2008;5(2):216–23.
20 Fuchs U, Zittermann A, Stuettgen B, Groening A,Minami K, Koerfer R. Clinical outcome ofpatients with deep sternal wound infectionmanaged by vacuum-assisted closure comparedto conventional therapy with open packing:a retrospective analysis. Ann Thorac Surg2005;79(2):526–31.
21 DeFranzo AJ, Pitzer K, Molnar JA et al. Vacuum-assisted closure for defects of the abdominal wall.Plast Reconstr Surg 2008;121(3):832–9.
22 Stannard JP, Robinson JT, Anderson ER, McGwin G,Jr., Volgas DA, Alonso JE. Negative pressurewound therapy to treat hematomas and sur-gical incisions following high-energy trauma. JTrauma 2006;60(6):1301–6.
23 Fleck T, Gustafsson R, Harding K et al. The man-agement of deep sternal wound infections usingvacuum assisted closure (V.A.C.) therapy. IntWound J 2006;3(4):273–80.
24 Armstrong DG, Attinger CE, Boulton AJ et al.Guidelines regarding negative pressure woundtherapy (NPWT) in the diabetic foot: results ofthe Tucson expert consensus Conference (TECC)on V.A.C. Therapy. Ostomy Wound Manage2004;50(4 Suppl):3S–27S.
25 Attinger CE, Janis JE, Steinberg J, Schwartz J, Al-Attar A, Couch K. Clinical approach to wounds:debridement and wound bed preparationincluding the use of dressings and wound-healing adjuvants. Plast Reconstr Surg 2006;117(7Suppl):72S–109S.
26 Banwell P, Withey S, Holten I. The use of negativepressure to promote healing. Br J Plast Surg1998;51(1):79.
27 Banwell PE. Topical negative pressure therapy inwound care. J Wound Care 1999;8(2):79–84.
28 Banwell PE, Teot L. Topical negative pressure(TNP): the evolution of a novel wound therapy. JWound Care 2003;12(1):22–8.
29 Yager DR, Zhang LY, Liang HX, Diegelmann RF,Cohen IK. Wound fluids from human pressureulcers contain elevated matrix metalloproteinaselevels and activity compared to surgical woundfluids. J Invest Dermatol 1996;107(5):743–8.
30 Cook H, Davies KJ, Harding KG, Thomas DW.Defective extracellular matrix reorganization bychronic wound fibroblasts is associated withalterations in TIMP-1, TIMP-2, and MMP-2 activ-ity. J Invest Dermatol 2000;115(2):225–33.
31 Grinnell F, Zhu M, Parks WC. Collagenase-1 com-plexes with alpha2-macroglobulin in the acuteand chronic wound environments. J Invest Der-matol 1998;110(5):771–6.
32 Wlaschek M, Peus D, Achterberg V, Meyer-Ingold W, Scharffetter-Kochanek K. Proteaseinhibitors protect growth factor activity in chronicwounds. Br J Dermatol 1997;137(4):646.
33 Davey ME, O’toole GA. Microbial biofilms: fromecology to molecular genetics. Microbiol Mol BiolRev 2000;64(4):847–67.
34 Falabella AF, Carson P, Eaglstein WH, Falanga V.The safety and efficacy of a proteolytic ointmentin the treatment of chronic ulcers of the lowerextremity. J Am Acad Dermatol 1998;39(5 Pt1):737–40.
35 Ladwig GP, Robson MC, Liu R, Kuhn MA, Muir DF,Schultz GS. Ratios of activated matrixmetalloproteinase-9 to tissue inhibitor of matrixmetalloproteinase-1 in wound fluids are inverselycorrelated with healing of pressure ulcers.Wound Repair Regen 2002;10(1):26–37.
36 Sibbald RG, Orsted H, Schultz GS, Coutts P,Keast D. Preparing the wound bed 2003: focuson infection and inflammation. Ostomy WoundManage 2003;49(11):24–51.
37 Sibbald RG. Topical antimicrobials. Ostomy WoundManage 2003;49(5A Suppl):14–8.
38 Stewart PS, Costerton JW. Antibiotic resistance ofbacteria in biofilms. Lancet 2001;358(9276):135–8.
39 Costerton JW, Stewart PS. Battling biofilms. Sci Am2001;285(1):74–81.
40 Costerton JW, Stewart PS, Greenberg EP. Bacterialbiofilms: a common cause of persistent infections.Science 1999;284(5418):1318–22.
41 Sussman C, Bates-Jensen B. Management of theWound Environment with Dressings and TopicalAgents. In: Sussman C, Bates-Jensen B, editors.Wound Care: A Collaborative Practice Manual forHealth Professionals. 3 ed. Lippincott Williamsand Wilkins; 2006;p. 250–67.
42 Schmidtchen A, Holst E, Tapper H, Bjorck L.Elastase-producing Pseudomonas aeruginosadegrade plasma proteins and extracellularproducts of human skin and fibroblasts,and inhibit fibroblast growth. Microb Pathog2003;34(1):47–55.
43 Kirshen C, Woo K, Ayello EA, Sibbald RG. Debride-ment: a vital component of wound bed prepara-tion. Adv Skin Wound Care 2006;19(9):506–17.
22 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
44 Gabriel A, Heinrich C, Shores JT, Baqai WK,Rogers FR, Gupta S. Reducing bacterial biobur-den in infected wounds with vacuum assistedclosure and a new silver dressing – a pilot study.Wounds 2006;18(9):245–55.
45 Gabriel A, Shores J., Heinrich C et al. Negativepressure wound therapy with instillation: a pilotstudy describing a new method for treatinginfected wounds. Int Wound J 2008;5(3):399–413.
46 Ashcroft GS, Herrick SE, Tarnuzzer RW,Horan MA, Schultz GS, Ferguson MW. Humanageing impairs injury-induced in vivo expressionof tissue inhibitor of matrix metalloproteinases(TIMP)-1 and -2 proteins and mRNA. J Pathol1997;183(2):169–76.
47 Ashcroft GS, Horan MA, Herrick SE, Tar-nuzzer RW, Schultz GS, Ferguson MW.Age-related differences in the temporal andspatial regulation of matrix metalloproteinases(MMPs) in normal skin and acute cutaneouswounds of healthy humans. Cell Tissue Res1997;290(3):581–91.
48 Sibbald RG, Woo K, Ayello EA. Increased bac-terial burden and infection: the story ofNERDS and STONES. Adv Skin Wound Care2006;19(8):447–61.
49 Tenenhaus M, Bhavsar D, Rennekampff HO. Diag-nosis and Surgical Management in Wound Bacte-rial Burden. In: Granick MS, Gamelli RL, editors.Surgical Wound Healing and Management. 1ed. New York: Informa Healthcare USA, Inc.;2007;p. 29–38.
50 Bill TJ, Ratliff CR, Donovan AM, Knox LK, Mor-gan RF, Rodeheaver GT. Quantitative swab cul-ture versus tissue biopsy: a comparison inchronic wounds. Ostomy Wound Manage2001;47(1):34–7.
51 Lipsky BA, Berendt AR, Deery HG et al. Diagnosisand treatment of diabetic foot infections. ClinInfect Dis 2004;39(7):885–910.
52 Gilbert P. Avoiding the resistance pitfall in infec-tion control. Does the use of antiseptic prod-ucts contribute to the spread of antibiotic resis-tance? Ostomy Wound Manage 2006;52(10ASuppl):1S–3S.
53 Facklam R, Washington J. Streptococcus andelated catalase-negative gram-positive cocci. In:Balows A, Hausler WJ, Jr., Herrmann KL, Isen-berg HD, Shadomy HJ, editors. Manual of Clini-cal Microbiology. 5 ed. Washington, D.C.: Amer-ican Society for Microbiology; 1991;p. 238.
54 Bucknall TE. The effect of local infection uponwound healing: an experimental study. Br J Surg1980;67(12):851–5.
55 Dow G, Browne A, Sibbald RG. Infection in chronicwounds: controversies in diagnosis and treat-ment. Ostomy Wound Manage 1999;45(8):23–40.
56 Davis E. Don’t deny the chance to heal! Presentedat the 2nd Joint Meeting of the Wound HealingSociety and the European Tissue Repair Society,May 15-19, 1996;Boston, MA. 5-15-1996. Ref Type:Abstract.
57 Potera C. Biofilms invade microbiology. Science1996;273(5283):1795–7.
58 Potera C. Forging a link between biofilms anddisease. Science 1999;283(5409):1837–9.
59 Schultz GS, Sibbald RG, Falanga V et al. Wound bedpreparation: a systematic approach to woundmanagement. Wound Repair Regen 2003;11(2Suppl):S1–S28.
60 Orsted H, Sibbald RG. A coordinated approach tochronic wound care. Ostomy Wound Manage2001;47(10):6–8.
61 Robson MC, Duke WF, Krizek TJ. Rapid bacterialscreening in the treatment of civilian wounds. JSurg Res 1973;14(5):426–30.
62 Sumpio BE, Allie DE, Horvath KA et al. Role ofnegative pressure wound therapy in treatingperipheral vascular graft infections. Vascular2008;16(4):194–200.
63 Ploumis A, Mehbod AA, Dressel TD, Dykes DC,Transfeldt EE, Lonstein JE. Therapy of SpinalWound Infections Using Vacuum-assistedWound Closure: Risk Factors Leading to Resis-tance to Treatment. J Spinal Disord Tech2008;21(5):320–3.
64 Mehbod AA, Ogilvie JW, Pinto MR et al. Postoper-ative Deep Wound Infections in Adults AfterSpinal Fusion: Management with Vacuum-Assisted Wound Closure. J Spinal Disord Tech2005;18(1):14–7.
65 V.A.C. Therapy Clinical Guidelines: A referencesource for clinicians. 7-1-2007. Ref Type: Pam-phlet.
66 Gwan-Nulla DN, Casal RS. Toxic shock syndromeassociated with the use of the vacuum-assistedclosure device. Ann Plast Surg 2001;47(5):552–4.
67 DeFranzo AJ, Argenta LC, Marks MW et al. The useof vacuum-assisted closure therapy for the treat-ment of lower-extremity wounds with exposedbone. Plast Reconstr Surg 2001;108(5):1184–91.
68 Gupta S, Gabriel A, Shores J. The perioperative useof negative pressure wound therapy in skingrafting. Ostomy Wound Manage 2004;50(4ASuppl):32–4.
69 Vuerstaek JD, Vainas T, Wuite J, Nelemans P, Neu-mann MH, Veraart JC. State-of-the-art treatmentof chronic leg ulcers: A randomized controlledtrial comparing vacuum-assisted closure (V.A.C.)with modern wound dressings. J Vasc Surg2006;44(5):1029–38.
70 Weed T, Ratliff C, Drake DB. Quantifying bacterialbioburden during negative pressure woundtherapy. Does the wound VAC enhance bacterialclearance? Ann Plast Surg 2004;52(3):276–9.
71 Moues CM, Vos MC, Van Den Bemd GJ, Stijnen T,Hovius SE. Bacterial load in relation to vacuum-assisted closure wound therapy: a prospec-tive randomized trial. Wound Repair Regen2004;12(1):11–7.
72 Armstrong DG, Boulton AJM, Banwell P. Negativepressure wound therapy in treatment of diabeticfoot wounds: a marriage of modalities. OstomyWound Manage 2004;50(4A):9–12.
73 Armstrong DG, Lavery LA, Abu-Rumman P et al.Outcomes of subatmospheric pressure dressingtherapy on wounds of the diabetic foot. OstomyWound Manage 2002;48(4):64–8.
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 23
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
74 Attinger CE, Bulan E, Blume PA. Surgical debride-ment. The key to successful wound healingand reconstruction. Clin Podiatr Med Surg2000;17(4):599–630.
75 Leininger BE, Rasmussen TE, Smith DL, Jenk-ins DH, Coppola C. Experience With WoundVAC and Delayed Primary Closure of Contam-inated Soft Tissue Injuries in Iraq. J Trauma2006;61(5):1207–11.
76 Song DH, Wu LC, Lohman RF, Gottlieb LJ,Franczyk M. Vacuum assisted closure forthe treatment of sternal wounds: the bridgebetween debridement and definitive closure.Plast Reconstr Surg 2003;111(1):92–7.
77 Reeves I, Plourde M, Authier S, Doddridge C. [Com-bined effect of Acticoat and VAC on woundhealing]. Perspect Infirm 2005;2(5):10–5.
78 Melano E, Rodriguez HL, Carillo R, Dillon L. Theeffects of Panafil when using topical negativepressure to heal an infected sternal wound. JWound Care 2004;13(10):425–6.
79 Totaro P, Rambaldini M. Efficacy of antimicrobialactivity of slow release silver nanoparticlesdressing in post-cardiac surgery mediastinitis.Interact Cardiovasc Thorac Surg 2008.
80 Lumenta DB, Kamolz LP, Frey M. Adult BurnPatients With More Than 60% TBSA Involved-Meek and Other Techniques to OvercomeRestricted Skin Harvest Availability-The Vien-nese Concept. J Burn Care Res 2009;30(2):231–42.
81 Ambrosio A, Barton K, Ginther D. VAC GranuFoamSilver dressing - A new antimicrobial silver foamdressing specifically engineered for use with theVAC therapy. White Paper , 1-15. 1-1-2006. SanAntonio, TX, Kinetic Concepts, Inc. Ref Type:Generic.
82 Fridkin SK, Gaynes RP. Antimicrobial resistancein intensive care units. Clin Chest Med1999;20(2):303–16, viii.
83 Wisplinghoff H, Bischoff T, Tallent SM, Seifert H,Wenzel RP, Edmond MB. Nosocomial blood-stream infections in US hospitals: analysisof 24,179 cases from a prospective nation-wide surveillance study. Clin Infect Dis2004;39(3):309–17.
84 Diekema DJ, BootsMiller BJ, Vaughn TE et al.Antimicrobial resistance trends and outbreak fre-quency in United States hospitals. Clin Infect Dis2004;38(1):78–85.
85 McDonald LC. Trends in antimicrobial resistancein health care-associated pathogens and effecton treatment. Clin Infect Dis 2006;42(Suppl2):S65–S71.
86 Gaynes R, Edwards JR, National Nosocomial Infec-tions Surveillance System. Overview of nosoco-mial infections caused by gram-negative bacilli.Clin Infect Dis 2005;41(6):848–54.
87 Ovington LG. The truth about silver. OstomyWound Manage 2004;50(9A Suppl):1S–10S.
88 Driver VR. Silver dressings in clinical prac-tice. Ostomy Wound Manage 2004;50(9ASuppl):11S–5S.
89 Brett DW. A discussion of silver as an antimicrobialagent: alleviating the confusion. Ostomy WoundManage 2006;52(1):34–41.
90 Hall RE, Bender G, Marquis RE. Inhibitory and cidalantimicrobial actions of electrically generated sil-ver ions. J Oral Maxillofac Surg 1987;45(9):779–84.
91 Jones SM, Banwell PE, Shakespeare PG. Interfacedressings influence the delivery of topicalnegative-pressure therapy. Plast Reconstr Surg2005;116(4):1023–8.
92 Ip M, Lui SL, Poon VK, Lung I, Burd A. Antimicro-bial activities of silver dressings: an in vitrocomparison. J Med Microbiol 2006;55(Pt 1):59–63.
93 Poon VK, Burd A. In vitro cytotoxity of silver:implication for clinical wound care. Burns2004;30(2):140–7.
94 Drosou A, Falabella A, Kirsner RS. Antiseptics onwounds: an area of controversy. Wounds2003;15(5):149–66.
95 Cochrane CA, Walker M, Bowler P, Parsons D,Knottenbelt DC. The effect of several silver-containing wound dressings on fibroblast func-tion in vitro using the collagen lattice contractionmodel. Wounds 2006;18(2):29–34.
96 Poulakidas S, Kowal-Vern A. Facilitating residualwound closure after partial graft loss withvacuum assisted closure therapy. J Burn CareRes 2008;29(4):663–5.
97 Swezey L. Antimicrobial wound dressings - silver.Ezine Articles. 7-14-2009. Ref Type: Generic.
98 Bhandari M, Schemitsch EH. High-pressure irriga-tion increases adipocyte-like cells at the expenseof osteoblasts in vitro. J Bone Joint Surg Br2002;84(7):1054–61.
99 Wolvos T. Wound instillation - The next stepin negative pressure wound therapy. Lessonslearned from initial experiences. Ostomy WoundManage 2004;50(11):56–66.
100 Wolvos T. Wound instillation with negative pres-sure wound therapy. Ostomy Wound Manage2005;51(2A Suppl):21S–6S.
101 Bernstein BH, Tam H. Combination of subatmo-spheric pressure dressing and gravity feed antibi-otic instillation in the treatment of post-surgicaldiabetic foot wounds: A case series. Wounds2005;17(2):37–48.
102 Skulan TW, Hoppe JO. Preliminary observationson the toxicity of the hydrochloride and acetatesalts of mafenide (sulfamylon r). Life Sci1966;5(24):2279–82.
103 McCauley RL, Linares HA, Pelligrini V, Hern-don DN, Robson MC, Heggers JP. In vitro toxicityof topical antimicrobial agents to human fibrob-lasts. J Surg Res 1989;46(3):267–74.
104 Cooper ML, Boyce ST, Hansbrough JF, Fore-man TJ, Frank DH. Cytotoxicity to culturedhuman keratinocytes of topical antimicrobialagents. J Surg Res 1990;48(3):190–5.
105 McCauley RL, Li YY, Poole B et al. Differentialinhibition of human basal keratinocyte growth tosilver sulfadiazine and mafenide acetate. J SurgRes 1992;52(3):276–85.
106 Richards RM, Mahlangu GN. Therapy for burnwound infection. J Clin Hosp Pharm1981;6(4):233–43.
107 Klasen HJ. Historical review of the use of silverin the treatment of burns. I. Early uses. Burns2000;26(2):117–30.
24 © 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc
A Clinical Review of Infected Wound Treatment with Vacuum Assisted Closure® (V.A.C.®) Therapy
108 Klasen HJ. A historical review of the use of silverin the treatment of burns. II. Renewed interest forsilver. Burns 2000;26(2):131–8.
109 Wolvos TA. Advanced Wound Care with Stable,Super-Oxidized Water. A look at how combi-nation therapy can optimize wound healing.Wounds 2006;18(Suppl 1):11–3.
110 Wolvos T. Treatment of Diabetic Wounds withNegative Pressure Wound Therapy. In: Nas-san S., editor. Pre- and Post-Operative Servicesfor the Amputee with Diabetes. American Dia-betes Association; 2007;p. 87–93.
111 Labler L, Trentz O. V.A.C. instillation: invitro model. Part 1. Biomed Tech (Berl)2005;50(12):413–8.
112 Labler L, Trentz O. V.A.C. instillation: in vitromodel. Part 2. Biomed Tech (Berl) 2006;51(1):30–7.
113 Moch D, Fleischmann W, Westhauser A. [Instil-lation vacuum sealing–report of initial expe-riences]. Langenbecks Arch Chir Suppl Kon-gressbd 1998;115:1197–9.
114 Kirr R, Wiberg J, Hertlein H. [Clinical experienceand results of using the V.A.C. instill therapyin infected hip- and knee prosthetics]. ZentralblChir 2006;131(Suppl 1):S79–S82.
115 Fleischmann W, Russ M, Westhauser A, Stam-pehl M. [Vacuum sealing as carrier system forcontrolled local drug administration in woundinfection]. Unfallchirurg 1998;101(8):649–54.
116 Timmers MS, Graafland N, Bernards AT, Nelis-sen RG, van Dissel JT, Jukema GN. Negativepressure wound treatment with polyvinylalcohol foam and polyhexanide antisep-tic solution instillation in posttraumaticosteomyelitis. Wound Repair Regen 2009;17(2):278–86.
117 Brem MH, Blanke M, Olk A et al. [The vacuum-assisted closure (V.A.C.) and instillation dressing: Limb salvage after 3 degrees open fracturewith massive bone and soft tissue defectand superinfection.]. Unfallchirurg 2008;111(2):122–5.
118 Lansdown AB. Silver in health care: antimicrobialeffects and safety in use. Curr Probl Dermatol2006;33:17–34.
119 Matsuno H, Yudoh K, Hashimoto M et al. A newantibacterial carrier of hyaluronic acid gel. JOrthop Sci 2006;11(5):497–504.
120 Joseph TN, Chen AL, Di Cesare PE. Use ofantibiotic-impregnated cement in total jointarthroplasty. J Am Acad Orthop Surg2003;11(1):38–47.
121 Neut D, van de Belt H, van Horn JR, vander Mei HC, Busscher HJ. Residual gentamicin-release from antibiotic-loaded polymethyl-methacrylate beads after 5 years of implantation.Biomaterials 2003;24(10):1829–31.
122 Taggart T, Kerry RM, Norman P, Stockley I. Theuse of vancomycin-impregnated cement beads inthe management of infection of prosthetic joints.J Bone Joint Surg Br 2002;84(1):70–2.
123 Rand RP, Cochran RP, Aziz S et al. Prospectivetrial of catheter irrigation and muscle flapsfor sternal wound infection. Ann Thorac Surg1998;65(4):1046–9.
124 Willenegger H. A. die spul-saugdrainage. Indika-tion, wirkungsweise und technik der spul-saugdrainage. Aktuelle Probl Chir Orthop1979;12:68–70.
125 Jones GA, Butler J, Lieberman I, Schlenk R.Negative-pressure wound therapy in the treat-ment of complex postoperative spinal woundinfections: complications and lessons learnedusing vacuum-assisted closure. J NeurosurgSpine 2007;6(5):407–11.
126 White RA, Miki RA, Kazmier P, Anglen JO.Vacuum-assisted closure complicated by erosionand hemorrhage of the anterior tibial artery. JOrthop Trauma 2005;19(1):56–9.
127 Patel NV, Shah RD, Welsh RJ, Chmielewski GW.Empyema–a complication of vacuum-assistedclosure of infected thoracotomy wounds in twoconsecutive cases. Am Surg 2009;75(4):349–50.
128 Chester DL, Waters R. Adverse alteration of woundflora with topical negative-pressure therapy: acase report. Br J Plast Surg 2002;55(6):510–1.
129 Sartipy U, Lockowandt U, Gabel J, Jideus L, Dell-gren G. Cardiac rupture during vacuum-assisted closure therapy. Ann Thorac Surg2006;82(3):1110–1.
DISCLAIMERThe information provided is based on anexpert advisory panel convened to determineappropriate use of the different modalitiesof negative pressure wound therapy (NPWT)as delivered by V.A.C.® Therapy and V.A.C.Instill® with either GranuFoam™ or Granu-Foam Silver™ Dressings for the treatment ofinfected wounds. All NPWT systems do notperform in the same manner, and outcomesusing other systems may not be the same. Rec-ommendations are not intended as a guaranteeof results, outcomes, or performance of theV.A.C.® Therapy Systems. Please note that useof V.A.C.® Therapy does not preclude use ofother surgical techniques or modalities to man-age wounds. As with any application, consultproduct labelling and instructions for use priorto initiating V.A.C.® Therapy.
Microcyn® is the trademark of OculusInnovative Sciences (Petaluma, CA). All othertrademarks designated herein are proprietaryto KCI Licensing, Inc., its affiliates and/orlicensors.
© 2009 The Authors. Journal Compilation © 2009 Blackwell Publishing Ltd and Medicalhelplines.com Inc 25





























