Embed Size (px)
Citation preview

Endocrinol Japon 1992, 39 (3), 251-257
A Child with Pituitary Gigantism and PrecociousAdrenarche: Does GH and/or PRL Advance the Onset ofAdrenarche?
NORITAKA IWATANI, MIHOKO KODAMA, AND HIROSHI SETO*
Departments of Child Development and *Neurosurgery,Kumamoto University Medical School, Kumamoto 860, Japan
Abstract. We describe a female child with pituitary gigantism and precocious adrenarche. From two
years of age she showed unusual overgrowth, and at 5 years old she was 133.5 cm (+ 5.5 SD) tall andweighed 40.5 kg. Her precocious manifestations were pubic hair, acne vulgaris, hirsutism, and advancedbone age. Endocrinological examination revealed markedly increased serum growth hormone (GH) and
prolactin (PRL), which responded paradoxically to a TRH test. In addition, the concentrations of serumdehydroepiandrosterone (DHA) and its sulfate (DHAS) were increased to adult levels, moving inaccordance with changes in ACTH, which suggested that these androgens were secreted from theadrenal glands functionally. These androgens seemed to be responsible for her partial precocity. Priorreports have suggested that GH and/or PRL overproduction might have played a role in the induction ofadrenarche. Also, in previous reports of 9 gigantism patients under 10 years old, the manifestation of
precocious adrenarche was suggested in 8. Further investigation of the influence of GH and PRL onadrenal androgen production in children with pituitary gigantism is required. On the other hand, inshort children with normal GH secretion, attention should be paid to whether or not the GH therapy inearly childhood induces precocious adrenarche.
Key words: Pituitary gigantism, Precocious adrenarche, GH, PRL, Dehydroepiandrosterone (DHA),DHA sulfate (DHAS). (Endocrinol Japon 39: 251-257, 1992)
LITTLE IS known about the mechanism of theactivation of adrenal androgen secretion in child-hood, referred to as adrenarche. Although the
production of these androgens is stimulated byACTH, ACTH may not be the sole factor regulat-ing adrenarche. Several investigators have sug-
gested that factors other than ACTH are involvedin the control of adrenal androgen production.However, the nature of these agents remains amatter of controversy.
The gigantism child presented here, with pituit-ary adenoma secreting both GH and PRL, wasassociated with precocious adrenarche. GH is amajor hormone promoting linear growth in child-
hood; however, it also has various other biological
effects in vivo. Again, the physiological significanceof PRL is not fully known. Although gigantism
due to pituitary adenoma in childhood is a raredisorder, the patient provides much significant
information for elucidating the biological effectsof GH and/or PRL in childhood. In this report, we
describe in detail the results of endocrinologicalstudies in this gigantism case. Further, we review
previous reports of pituitary gigantism children[1-8], and discuss the still unknown mechanism ofadrenarchal onset.
Subject and Methods
Subject (Case Report)
The subject was a 12.6-year-old girl who was
Received: December 11, 1991Accepted: April 17, 1992Correspondence to: Dr. Noritaka IWATANI, Department ofChild Development, Kumamoto University Medical School,1-1-1 Honjo, Kumamoto 860, Japan.

252 IWATANI et al.
born after 35 gestational weeks of an uncompli-cated pregnancy with a birth weight and length of
2650 g and 46 cm, respectively. Her parents
became aware of her accelerated physical growthat around 2 years of age. At 3.5 years old herheight was 111.0 cm (+4.0 SD) and weight 28 kg
(obesity rate according to height, 49%). She wasfirst admitted to our hospital at 5.4 years old
because of excessive growth. Her physical man-ifestations at that time were: height 133.5 cm (+
5.5 SD); weight 40.5 kg (obesity rate according toheight 36%); a large head (circumference 56.2
cm); a prominent forehead and mandible; a widenasal bridge; thick lips; disproportionately largehands and feet (palm-middle finger length 16.0
cm, and foot length 24.5 cm); and acanthosisnigricans of the axillae. Her heel pad thickness was
27 mm. Other findings at the time were sparse
pubic hair (Tanner grade II) without other exter-nal genital abnormalities, acne on the forehead,hirsutism on the legs, and advanced bone age (7.4
years old); no breast budding or galactorrhea wasobserved. CT scanning of the head revealed anintrasellar tumor extending to the suprasella.
At 5.5 years old, she underwent removal of thetumor under the diagnosis of a GH- and PRL-
secreting adenoma. The pathological diagnosiswas an eosinophilic and chromophobic mixedadenoma. The pituitary tumor, however, was not
resected completely; subsequently 30 Gy irradia-tion and two more surgical operations were
needed at the ages of 6.2 and 9.2 years to remove
the residual tumor. Bromocriptine administrationwas started after the second operation. In spite of
the administration of large doses of bromocrip-tine, serum GH and PRL continued to be abnor-
mally high (Table 1). After the third operationbasal GH decreased to a level slightly higher than
normal, while IGF-I and PRL remained abnormal-ly high (Table 1). She continued to grow excessive-ly tall and heavy.
At the age of 12.6 years, she reached 176.8 cm inheight (+ 4.2 SD) and 86.0 kg in weight, and had
long extremities (upper to lower segment ratio,0.78). Her pubertal signs corresponded to Tanner
grade III for breast and IV for pubic hair, but nomenstruation or galactorrhea was observed. Her
bone age was 13.5 years old at the time.
Methods
To evaluate the pituitary function, provocative
tests were performed during fasting with in-travenous administration of 0.1 U of insulin perkilogram of body weight, 500 ,,cg of TRH and 100
μg of LH-RH. Blood samples were drawn before
and 15, 30, 60, 90 and 120 min after injection. Anoral glucose tolerance test (OGTT) was performedduring fasting with 1.75 g of glucose per kilogramof body weight or 75 g as the maximum dose.Blood samples were drawn before and every 30min after glucose was given, for 180 min. A single
Table 1. Therapy and baseline hormone levels
GH and PRL values indicate means•}1SD (n=number of measured samples). Dose of bromocriptine was
increased from 2.5 to 35 mg/day successively until the third surgery. a, range in adulthood; 1), range in
childhood.

PITUITARY GIGANTISM AND ADRENARCHE 253
dose of 2.5 mg of bromocriptine was administered
orally to assess its influence on serum GH and
PRL, and 7.5 mg of bromocriptine was adminis-
tered for 5 days to assess its influence on
androgens. Dexamethasone was administered in 2,
4, and 8 mg doses for 2 days each to achieve
sufficient suppression of ACTH. An ACTH test
was performed with 250 eug of ACTH-(1-24)
administered intravenously. To assess the changes
in the serum baselines of GH and PRL, serum
samples were obtained at random. Every blood
hormone was measured by means of a specific
RIA: serum GH was measured by a double-
antibody technique (HGH-I kit, Eiken), serum
PRL by an IRMA using monoclonal antibody (Ab
Bead PRL kit, Eiken), serum LH and FSH by a
double-antibody technique (HLH and HFSH kits,
Eiken, respectively), serum cortisol by a solid
phase method (Amerlex-Cortisol kit, Amersham),
TSH by an IRMA with monoclonal antibody
(Amerwell-TSH kit, Amersham), and serum in-
sulin by a solid phase method (Ab Bead Insulin kit,
Eiken). Serum IGF-I was measured by the pre-
viously reported method with an acid-ethanol
extracted sample [9] (SM-C kit, Nichols Institute
Diagnostics), and recombinant IGF-I (Fujisawa
Pharmaceuticals, Japan) was used as the kit's
standard reference. Estradiol, DHA, DHAS, and
etiocholanolone were measured at the Special
Reference Laboratory (Tokyo, Japan). Serum
samples were stored at -20•Ž until use. Adrenal
scintigraphy was performed with 131I-adosterol.
Bone age was estimated by the Tanner-
Whitehouse II method.
Results
During her first and second admissions to our
hospital at 5.4 and 6.0 years of age, detailed
endocrinological evaluations were performed.
Complete blood count, routine blood chemistry,
and thyroid hormone levels were normal, except
for increased alkaline-phosphatase.
The baselines of GH and PRL concentrations in
her serum were markedly increased and the serum
IGF-I level was also very high (Table 1). In
pituitary function studies, serum GH and PRL did
not respond to either insulin-induced hypo-
glycemia or to an LH-RH test. In response to
TRH, however, the GH level rose paradoxically
from 208 to 2513 ng/ml, and PRL increased from
1052 to 1640 ng/ml. A single oral dose of 2.5 mg
bromocriptine resulted in an apparent reduction
in the serum levels of both GH and PRL (from 207
and 858 ng/ml to 39 and 182 ng/ml, respectively).
Serum GH was not suppressed after oral adminis-
tration of glucose. The ACTH-cortisol axis re-
sponded normally to insulin-induced hypo-
glycemia (peak cortisol, 15.3 ƒÊg/dl at 15 min).
Other noticeable findings were increased serum
DHA and DHAS concentrations, already at adult
levels (Table 1), and increased urinary 17-
ketosteroids (17 KS) and urinary etiocholanolone,
one of the metabolites of these androgens. To
determine the origin and nature of these
androgens, an ACTH test, a dexamethasone sup-
pression test, bromocriptine loading, and adrenal
scintigraphy were performed at age 6. In response
to the ACTH and dexamethasone suppression
tests, DHA, DHAS, and etiocholanolone seemed
to move in accordance with changes in ACTH
(Figs. 1 and 2), and the adrenal scintillation
examination showed radioisotope accumulation in
identical positions in bilateral adrenal glands with
a normal image and intensity. These findings
indicated the origin of the androgens to be the
adrenal glands.
In a loading test with 7.5 mg bromocriptine for
5 days, the serum GH and PRL concentrations
remained at abnormally high levels even at the 5th
day (GH: from 82 to 114 ng/ml, PRL: from 519 to
117 ng/m/), and the serum level of DHAS and the
urinary excretion of etiocholanolone were un-
affected (DHAS: from 1072 to 1160 ng/ml,
etiocholanolone: from 2.4 to 2.1 mg/day).
The LH and FSH responses to an LH-RH test
performed at age 5.4 years showed prepubertal
increases (Table 2A). The serum estradiol concen-
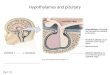
Fig.1. Adrenal androgen response to ACTH test. Tested
at age 6. 250 ,ug of ACTH-(1-24) was administered
intravenously.

254 IWATANI et al.
Fig. 2. Dexamethasone suppression test. Tested at age 6.
Dexamethasone was administered orally in doses of
2, 4, and 8 mg for 2 days each. Serum cortisol,DHAS, and urinary etiocholanolone were mea-
sured for 7 days.
Table 2. Pituitary function studies
Examination A was performed at the age of 5.4 years,
and B and C at 12.6 years. Values in parentheses indicate
peak times in minutes.
tration also remained at a prepubertal level (Table1).
At 12.6 years of age, we evaluated her pituitary
function again. Although basal GH had decreasedto a level slightly higher than normal, the serum
GH still showed a paradoxical response to TRHadministration (Table 2C). Furthermore, in an
OGTT, the GH level was not suppressed signi-ficantly, but maintained a slightly higher than
normal level. LH and FSH responded to anLH-RH test better than previously (Table 2B), but
the pituitary-gonadal function did not develop tothe pubertal level because the serum estradiol levelremained below 10 pg/ml (Table 1).
Discussion
The adrenarche, an increase in adrenal
androgens, does not occur in early childhood
[10-12]; however, serum DHA and DHAS of this
patient had already increased to adult levels at 6
years of age. By means of ACTH and dexametha-sone suppression tests performed at 6 years of age,we confirmed that the origin of the androgens,DHA and DHAS, was the adrenal glands, because
the movement of these steroids was dependent onchanges in ACTH (Figs. 1 and 2). Furthermore,
the results of adrenal scintigraphy also indicatedthat the origin of these androgens was the
adrenals.Although DHAS is the most abundant steroid
circulating in the plasma of normal human adults,its biological role is not fully known. Some reportshave suggested that DHAS may possess weak
androgenic and estrogenic activities [13], and that
the adrenarche may be related to the pubic hair
growth [14, 15]. Our patient exhibited the follow-ing noticeable manifestations at 5 and 6 years of
age: pubic hair, acne vulgaris, hirsutism of thelegs, and advanced bone age, which can be
considered a reflection of androgenic and/orestrogenic effects. It seems unlikely that thesefindings resulted from the effects of pituitary-
gonadal axis activation, because gonadotropinresponse to an LH-RH test remained at a pre-
pubertal level and the serum estradiol concentra-tion also remained low (Tables 1 and 2A). There-
fore, increased adrenal androgens should be re-sponsible for her partial precocity and bone age
acceleration.The onset mechanism of adrenarche remains
uncertain. The existence of a pituitary adrenalandrogen-stimulating hormone (AASH), which
acts in the presence of ACTH to stimulate andcontrol the secretion of adrenal androgens, has
been postulated [16-18]. On the other hand, someresearchers do not agree that there is such a factor
and have suggested that adrenarche results from ashift in the pathway of steroid synthesis in re-sponse to the ACTH stimulation that follows the
development of the zona reticularis [19]. However,it is still not known what factor develops the zona
reticularis and causes adrenarche.Does pituitary gigantism associated with preco-
cious adrenarche, as observed in our patient,suggest a relationship between GH and/or PRL

PITUITARY GIGANTISM AND ADRENARCHE 255
and adrenarchal onset? Pituitary gigantism inearly childhood is exceedingly rare, and most
patients show overproduction of both GH andPRL. In our review of the literature, we could findas case reports only nine cases under 10 years oldwho were not associated with McCune-Albrightsyndrome, and eight of the nine reports included adescription of pubertal signs and evaluations of
gonadotropins or steroid hormones [1-8]. Eightout of nine cases, including our patient, exhibited
pubic hair or increased urinary 17-KS withoutother pubertal signs or any gonadotropin or sexhormone increase (Table 3). Unfortunately, ex-cept for our patient, none of their DHA or DHASwas measured, so there was no direct evidence ofadrenarche. However, the findings of pubic hairand urinary 17-KS do not seem to be due to
gonadal activation, and therefore suggest in-creased adrenal androgens. Hence, these clinicalfindings associated with pituitary gigantism indi-cate a possible relationship between GH and/orPRL and the induction of adrenarche.
This possibility is suggested by the following
evidence. Carter et al. [20] and Schiebinger et al.
[21] suggested that hyperprolactinemia was re-sponsible for the stimulation of adrenal androgen
production. They reported that bromocriptineinduced significant decreases in the serum PRL,
DHA, and DHAS concentrations in hyperprolac-tinemic patients. The following observations also
suggest the influence of PRL on adrenal function:adrenal tissue contains PRL receptors [22, 23], and
cultured human adrenal cortical cells exposed toPRL secrete more DHAS than do control cells [24].
GH may also stimulate the growth of the adrenal
glands. Skottner et al. [25] observed augmentationof adrenal weight following their treatment of
experimental rats with GH. Pillion et al. [26] andShigematsu et al. [27] reported that IGF-I receptor
is present in the human adrenal cortex, especiallyin the zona reticularis [26]. Further, in isolated GH
deficient children, adrenarche does occur; howev-er, a lower serum DHAS was observed than in the
control group [28]. These results indicate that PRL
Table 3. Pituitary gigantism under 10 years of age: review of reported cases*
*One case was omitted since it lacked a pubertal evaluation.
Eight out of 9 cases exhibited pubic hair or increased urinary 17-KS without other pubertal signs or any gonadotropin or
sex hormone increase.
u. 17 KS, urinary 17-ketosteroids; E2, estradiol; ND, not described; Ref. no., reference number.a,b, Normal ranges in childhood before adrenarche are below 1-2 mg/day and 3.5 ,u,mol/day, respectively.

256 IWATANI et al.
and also GH, probably mediated by IGF-I, maycontribute to the regulation of adrenal growth andfunction, and as a consequence play a role inadrenarchal onset.
In our patient, to determine the influence of GHand PRL on adrenal androgen secretion, bromoc-riptine was administered for 5 days. It failed,however, to suppress the serum DHAS level oretiocholanolone excretion in the urine probablybecause serum GH and PRL concentrations werenot reduced enough to influence DHAS secretion.As shown in Table 1, despite the reduction in theGH baseline level after the third operation, theblood IGF-I and also the PRL concentrations werestill abnormally high. These findings indicate thatthe residual pituitary adenoma was still active
(Table 2C), and this must be the cause of still highDHA and DHAS levels.
The mechanism of precocious adrenarcheobserved in the gigantism child appears complex.ACTH seems to be necessary to control adrenalandrogen production. Further, the possibility ofthe participation of GH or PRL, or the synergicaction of both, should be considered. Again, it isunclear whether or not GH/IGF-I and/or PRL
contribute to the natural onset of adrenarche.However, the fact that child gigantism with GH-
and PRL-producing adenoma was associated with
precocious adrenarche suggests that GH and/orPRL should be considered a possible causativefactor(s) in adrenarchal onset. Our findings also
invite attention to the GH treatment of shortchildren. The recent unlimited supply of GH
preparation derived from recombinant DNA tech-nology makes possible studies to assess the efficacy
of exogenous GH for height gain in non-GH-deficient short children [29-31], but such a treat-ment may induce precocious adrenarche. Further
investigation of the influence of GH and PRL onadrenal androgen production in children is re-
quired.
Acknowledgments
We thank Dr. Teruhisa Miike, professor of the
Department of Child Development, Kumamoto
University Medical School, for review of the
manuscript and helpful discussion.
References
1. Todd RM (1958) Acromegaly in a girl of 8 years.Arch Dis Child 33: 49-54.
2. Hurxthal LM (1961) Pituitary gigantism in a childfive years of age: effect of X-radiation, estrogentherapy and self-imposed starvation diet during aneleven-year period. J Clin Endocrinol Metab 21:343-353.
3. Spence HJ, Trias EP, Raiti S (1972) Acromegaly ina 9 1/2-year-old boy. Amer J Dis Child 123: 504-506.
4. Guyda H, Robert F, Colle E, Hardy J (1973)Histrogic, ultrastructural, and hormonal charac-terization of a pituitary tumor secreting both hGHand prolactin. J Clin Endocrinol Metab 36: 531-546.
5. Yamada Y, Okada M, Nohara Y, Fujita J, Endo M,Matsuura N, Nakayama K, Okuno T (1977) A casewith pituitary gigantism. Horumon To Rinsyo 25:941-948 (in Japanese).
6. Oikawa H, Yamasaki M, Machida Y, Kusunoki T(1977) A case of child gigantism. Horumon ToRinsyo 25: 1326-1328. (In Japanese).
7. Espiner EA, Carter TAH, Abbott GD, Wrightson P(1981). Pituitary gigantism in a 31-month-old girl:endocrine studies and successful response tohypophysectomy. J Endocrinol Invest 4: 445-450.
8. Ritzen EM, Wettrell G, Davies G, Grant DB (1985)
Management of pituitary gigantism; the role ofbromocriptine and radiotherapy. Acta Pediatr Scand74: 807-814.
9. Suwa S, Katsumata N, Maesaka H, Tokuhiro E,Yokoya S (1988) Serum insulin-like growth factor I(somatomedin-C) level in normal subjects frominfancy to adulthood, pituitary dwarfs and normalvariant short children. Endocrinol Japon 35:857-864.
10. Peretti E, Forest M (1976) Unconjugated plasmadehydroepiandrosterone plasma levels in normalsubjects from birth to adolescence in human; theuse of a sensitive radioimmunoassay.J Clin Endocri-nol Metab 43: 982-991.
11. Peretti E, Forest M (1978) Pattern of plasmadehydroepiandrosterone sulfate levels in humansfrom birth to adulthood: evidence for testicularproduction. J Clin Endocrinol Metab 47: 572-577.
12. Collu R, Ducharme JR (1978) Role of adrenalsteroids in the initiation of pubertal mechanisms.In: James VHT, Serio M, Giusti G, Martini L (eds)The Endocrine Function of the Human AdrenalCortex. Academic Press, London, New York, SanFrancisco: 547-559.
13. Drucker WD, Blumberg JM, Gandy HM, David

PITUITARY GIGANTISM AND ADRENARCHE 257
RR, Verde AL (1972) Biologic Activity of dehyd-roepiandrosterone sulfate in man. J Clin EndocrinolMetab 35: 48-54.
14. Rosenfield RL (1971) Plasma 17-ketosteroids and17 beta-hydroxysteroids in girls with prematuredevelopment of sexual hair. J Pediatr 79: 260-266.
15. Korth-Schutz S, Levine LS, New MI (1976) Serumandrogens in normal prepubertal and pubertalchildren and in children with precocious adrenar-che. J Clin Endocrinol Metab 42: 117-124.
16. Parker LN, Odell WD (1979) Evidence for exist-ence of cortical androgen-stimulating hormone.Am J Physiol 236: E616-620.
17. Cutler Jr GB, Davis SE, Johnsonbaugh RE,Loriaux DL (1979) Dissociation of cortisol andadrenal androgen secretion in patients with secon-dary adrenal insufficiency. j Clin Endocrinol Metab49: 604-609.
18. Sklar CA, Kaplan SL, Grumbach MM (1980)Evidence for dissociation between adrenarche and
gonadarche: studies in patients with idiopathicprecocious puberty, gonadal dysgenesis, isolatedgonadotropin deficiency, and constitutionally de-layed growth and adolescence. J Clin EndocrinolMetab 51: 548-556.
19. Rich BH, Rosenfield RL, Lucky AW, Helke JC,Otto P (1981) Adrenarche: changing adrenal re-sponse to adrenocorticotropin. J Clin EndocrinolMetab 52: 1129-1136.
20. Carter JN, Tyson JE, Warne GL, McNeilly AS,Faiman C, Friesen HG (1977) Adrenocorticalfunction in hyperprolactinemic women. J ClinEndocrinol Metab 45: 973-980.
21. Schiebinger RJ, Chrousos GP, Cutler GB, LoriauxDL (1986) The effect of serum prolactin on plasmaadrenal androgens and the production and meta-bolic clearance rate of dehydroepiandrosteronesulfate in normal and hyperprolactinemic subjects.
J Clin Endocrinol Metab 62: 202-209.22. Posner BI, Kelly PA, Shiu RPC, Friesen HG (1974)
Studies of insulin, growth hormone and prolactinbinding: tissue distribution, species variation andchracterization. Endocrinology 95 : 521-531.
23. Calvo JC, Finocchiaro L, Lathy I, Charreau EH,Calandra RS, EngstrOm B, Hansson V (1981)
Specific prolactin binding in the rat adrenal gland:its characterization and hormonal regulation. JEndocrinol 89: 317-325.
24. Higuchi K, Nawata H, Maki T, Higashizima M,Kato K, Ibayashi H (1984) Prolactin has a directeffect on adrenal androgen secretion. J Clin Endoc-rinol Metab 59: 714-718.
25. Skottner A, Clark RG, Fryklund L, Robinson ICAF(1989) Growth responses in a mutant dwarf rat tohuman growth hormone and recombinant humaninsulin-like growth factor I. Endocrinology 124:2519-2526.
26. Pillion DJ, Arnold P, Yang M, Stockard CR, GrizzleWE (1989) Receptors for insulin and insulin-like
growth factor-I in the human adrenal gland.Biochem Biophys Res Commun 165: 204-211.
27. Shigematsu K, Niwa M, Kurihara M, Yamasita K,Kawai K, Tsuchiyama H (1989) Receptor auto-radiographic localization of insulin-like growthfactor-I (IGF-I) binding sites in human fetal andadult adrenal glands. Life Sciences 45: 383-389.
28. Tokuhiro E, Suwa S (1981) The study of serumdehydroepiandrosterone sulfate levels in normalchildren and children with pituitary dwarfism.Folia Endocrinol Jap 57: 1186-1198 (In Japanese).
29. Rosenfeld RG, Hintz RL, Johanson AJ, ShermanB, Brasel JA, Burstein S, Chernausek S, ComptonP, Frane J, Gotlin RW, Kuntze J, Lippe BM,Mahoney PC, Moore WV, New MI, Saenger P,Sybert V (1988) Three-year results of a rando-mized prospective trial of methionyl human
growth hormone and oxandrolone in Turnersyndrome. J Pediatr 113: 393-400.
30. Takano K, Shizume K, Hibi I, the members of thecommittee for treatment of Turner syndrome
(1989) Treatment of 94 patients with Turner'ssyndrome with recombinant human growth hor-mone (SM-9500) for two years-the results of amulticentric study in Japan. Endocrinol Japon 36:569-578.
31. Genentech Collaborative Study Group (1989)Idiopathic short stature: Results of a one-yearcontrolled study of human growth hormone treat-ment. J Pediatr 115: 713-719.