Embed Size (px)
Citation preview

AG
AA
bst
ract
s954
Prevalence of Colorectal Adenomas in Blacks, Whites and Hispanics HavingScreening Colonoscopy in a Patient Navigation Program: A ProspectiveMulticenter StudyRobin B. Mendelsohn, Delia Calo, Ann G. Zauber, Mari Carlesimo, Samantha De Leon,Jason J. Wang, Deborah Kuk, Sidney J. Winawer
Background: Colorectal cancer (CRC) is the third most commonly diagnosed cancer andthe third most common cause of cancer deaths in both men and women in the UnitedStates. Blacks have been reported to have a higher incidence and mortality and a moreproximal anatomic distribution of CRC compared to whites and Hispanics. However, it isunclear whether this is due to biological differences in the pathology of adenomatous polypsor lower screening rates. Existing data consisting of retrospective studies and one singlecenter prospective study indicate that factors such as access to health care and modifiablerisk factors may be responsible for these racial disparities as opposed to biological differences.Methods: In 2003, the New York City Department of Health and Mental Hygiene (NYCDOHMH) implemented the Colonoscopy Patient Navigator Program (CPNP). Ten New YorkCity Hospital Sites, five public and five private, participated in the study. Through a oneto one relationship, PN helped to bridge disparities by scheduling appointments, educatingregarding bowel preparation and addressing obstacles. Data were prospectively collectedfrom 2005 through the first quarter of 2012 from centers with at least three consecutiveyears of reporting while using PN. Patient information including name, contact information,gender, date of birth, ethnicity and insurance information was collected by each PN duringthe initial contact after the patient was referred for screening colonoscopy (sCo). Adenomaand cancer detection rates, pathology and location were recorded and stratified by patientdemographic characteristics including age, gender, and race. Results: With the assistance ofPN, 29,711 individuals ages 50 and older underwent complete sCo. A total of 6226 adenomasand 35 cancers were found. The prevalence of adenomas was higher among white patientsthan black patients (27.45% versus 19.35%, p value < 0.05) (See tables 1 and 2). With theexception of the hepatic flexure, whites had a statistically significant higher prevalence ofadenomas, segment by segment, than blacks and Hispanics. Conclusion: This is a prospectivemulticenter center study of a large urban cohort investigating the prevalence of adenomasin blacks versus whites and Hispanics using a PN program. Preliminary data do not showthat blacks have an increased risk of adenomas compared to whites and Hispanics. Thissuggests that the higher incidence and mortality from CRC in blacks that was reported inother studies are more likely a function of access to colonoscopy as opposed to biologic factors.Table 1: Results of completed screening colonoscopy exams cross-tabulated by patient race(age ≥ 50)
* p-value ≤ 0.05 for chi-squared testTable 2: Types of adenomas detected by race for screening colonoscopies (age ≥ 50)
* p-value ≤ 0.05 for chi-squared test
955
Racial and Geographical Disparities in the Outcome of HepatocellularCarcinoma Within a High Prevalence Birth Cohort for Chronic Viral HepatitisSandeep Samuel, Adrienne Groman, Renuka Iyer
BACKGROUND: Chronic viral hepatitis is the most important risk factor for hepatocellularcarcinoma (HCC) in the United States. New guidelines recommend birth cohort basedscreening for hepatitis C in people born between 1945 and 1965 (also known as babyboomers). The aim of this study was to evaluate the population attributes and outcome ofHCC in the high prevalence birth cohort for chronic viral hepatitis. METHODS: We did a
S-168AGA Abstracts
retrospective cohort study using Surveillance, Epidemiology and End Result data (SEER)from 18 geographically different cancer registries in the USA. Patients born between 1945and 1965 who got diagnosed with primary HCC from 2000 to 2010 were included. Fibrolamellar, intrahepatic cholangiocarcinoma and neuroendocrine histologies were excluded.Clinicopathologic variables and geographical location were analyzed and compared usingWilcoxon Rank Sum test for ordinal variable and Chi-Square test for categorical variables.Disease specific survival (DSS) was the primary endpoint. Univariate and Multivariate Coxproportional hazards modeling were used to assess the effect of co-variates on DSS. TheDSS was compared using Kaplan-Meier method. All associations were considered statisticallysignificant at an alpha error <0.01 (p value < 0.01). RESULTS: We identified 19,889 patientswith HCC; of which there were 66.7% Caucasians, 16.9% African Americans (AA), 15%Asians and 1.4 % Native Indians. The median age at diagnosis was higher (55 yrs.) in AAcases compared to the overall group (p<0.001). Metastatic disease was more prevalent inAA (19.7%) compared to Caucasians (14.6%, p<0.001). Tumor size of >5cm was more inAsians (42.3%) than AA (36.5%) and Caucasians (31%). In the multivariate DSS model,worse tumor grade and male gender predicted poor DSS. Also, AA- HCC cases had theworst outcomes (HR=1.23, 95% CI: 1.17-1.30, p<0.001). In areas with highest proportionof AA-HCC cases out of the 18 locations studied, southern location predicted poor outcome;Louisiana (HR=1.20, 95% CI: 1.10-1.31, p<.001), Greater Georgia (HR=1.17, 95%CI: 1.06-1.28, p=0.001). Urbanized AA-HCC case predominant regions did not show statisticallyworse outcomes in survival; Metropolitan Detroit (HR= 1.03, 95% CI: 0.94 -1.13, P=0.52)and Metropolitan Atlanta (HR= 1.13, 95% CI: 1.02-1.27, p=0.026). The median DSS (inmonths) was 8 in AA, 13 in Native Indians, 14 in Caucasians and 16 in Asians. CONCLU-SION: Geographical and racial disparities in HCC survival outcome is seen in the highprevalence birth cohort for chronic viral hepatitis. African American race and southern ruralareas in USA predicted the worst survival for HCC inside the birth cohort. Therefore, whenformulating new screening practices for early diagnosis of chronic viral hepatitis and HCC,due importance should be given to this subset of population, to improve survival.
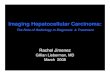
Unadjusted Kaplan-Meier survival estimates for hepatocellular carcinoma based on race
956
The Effect of an Organized Screening Program on Racial and EthnicDisparities and Choice of Colorectal Cancer Screening TestShivan J. Mehta, Christopher D. Jensen, Nirupa R. Ghai, Virginia P. Quinn, Theodore R.Levin, Joanne E. Schottinger, Alexander T. Lee, Wei Zhao, Ann G. Zauber, Marjolein vanBallegooijen, Adeyinka O. Laiyemo, Michael Goodman, Robert H. Fletcher, Douglas A.Corley, Chyke A. Doubeni
Background: Organized colorectal cancer (CRC) screening programs aim to uniformly deliverservices to defined populations, and are effective at increasing screening rates, but it is notknown if their effectiveness differs by race/ethnicity. In 2007, Kaiser Permanente NorthernCalifornia (KPNC) implemented an organized CRC screening program using mailed fecalimmunochemical test (FIT). We examined the association between race/ethnicity and theuse of CRC screening in the period before and after implementation of KPNC's program.Methods: This was a retrospective cohort study of screening-eligible patients in KPNC whowere 50-75 years old and had ≥2 years of enrollment in the 2000-2009 period. Patientswere followed until disenrollment, or December 31, 2011, whichever came first. Our primaryoutcome was whether a patient was up-to-date on CRC screening for each study year usingHealthcare Effectiveness Data and Information Set (HEDIS) criteria (colonoscopy within 10years, sigmoidoscopy within 5 years, or fecal occult blood test/FIT within 1 year). We alsoexamined use of each CRC test, separately. This report focused on non-Hispanic whites,non-Hispanic blacks, Hispanics, Asian/Pacific Islanders (API), and Native Americans. Weused multivariable regression to estimate CRC screening use for each racial/ethnic grouprelative to whites, adjusted for covariates. Analyses were performed separately for the periodsbefore (2000-2006) and during (2007-2011) program implementation. Results: There were870,687 eligible patients included in the analysis. Overall, the proportion of the populationscreened for CRC increased from 12% in 2000 to 77% in 2011. Yearly increases wereobserved in all racial/ethnic groups, but screening rates were lowest among Hispanics andNative Americans and highest among APIs, both before and during program implementation(Table 1). Blacks had slightly higher screening rates than whites before program implementa-tion (odds ratio (OR)= 1.07, CI 1.05-1.08), but proportion screened among blacks fell belowthose among whites (OR=0.81, CI 0.80-0.83) during implementation, due to a lower initialannual increase (Figure 1), particularly among patients who received a mailed FIT. Amongthose who received a mailed FIT, blacks had a lower probability of undergoing screening(55%) than whites (63%). The black-white difference appeared in the first year of programimplementation, but narrowed over time. Conclusions: The rate of CRC screening increased