Embed Size (px)
Citation preview
Volume 185, Number 6 AmJ Obstet Gynecol
669 DOPPLER ULTRASONOGRAPHY OF THE MIDDLE CEREBRAL ARTERY PEAK SYSTOLIC VELOCITY IN THE FETUS: REPRODUCIBILITY OF MEASUREMENT GIANCARLO MAR11, ALFRED ABUHAMAD~, JONATHAN BRUMFIELD 1, .]AMES E. FERGUSON II1; JUniversity of Virginia, Obstetrics and Gynecology, Charlottesville, VA; 2Eastern Virginia Medical School, Obstetrics and Gynecology, Norfolk, VA
OBJECTIVE: Measurement of the Middle Cerebral Artery Peak Systolic Velocity (MCA-PSV) in the fetus has been shown to predict fetal anemia in pregnancies at risk because of red blood cell alloimmunization and decrease the need for invasive procedures in such pregnancies. The objective of this investigation was to study the reproducibility of MCA-PSV measm'ements in two different institutions.
STUDY DESIGN: This study was performed on 25 normal fetuses. In each tetus, PSV was assessed at 3 different locations of the MCA proximal to the transducer: A) 2 mm after its origin from the internal carotid artery; B) in its mid-length between origin and division; C) 2 mm dose to its division. PSV was also assessed in the contralateral MCA 2 mm after its origin. With each measurement, care was taken to ensure that the ultrasound beam was parallel to the artery for its entire length. The reliability of an angle corrector was also assessed. The technical error of mea.surement and coefficient of variation (CV) were analyzed. The coefficient correlation (r) was also measured. A P < .05 indicated statistical significance.
RESULTS: Gestational age at study entry ranged from 14 to 36 weeks (Median = 23.6 weeks). The proximal MCA 2 nun after its origin from the internal carotid artery (A) had the best intra- (mean 3.77%; SD: 0.899; Min 2.81%; Max: 4.64%; r: 0.99) and interobsmwer variability in both institutions (4.03%, r: 0.98; and 5.48%, r: 0.98, respectively) (P< .05)i No difference in the assessment of the MCA-PSV was noted when different equipment were evaluated (CV = 4.03%; r: 0.98).
CONCLUSION: Our data confirm that fetal MCA-PSV is optimally measured in the proximal MCA 2ram after its origin t-urn the internal carotid artery. Given the importance of clinical decision based on this measurement, each sonographer and sonologist interested in the nmasurement of the MCA- PSV should test his /her intra- and inter-observer variability.
SMFM Abstracts $261
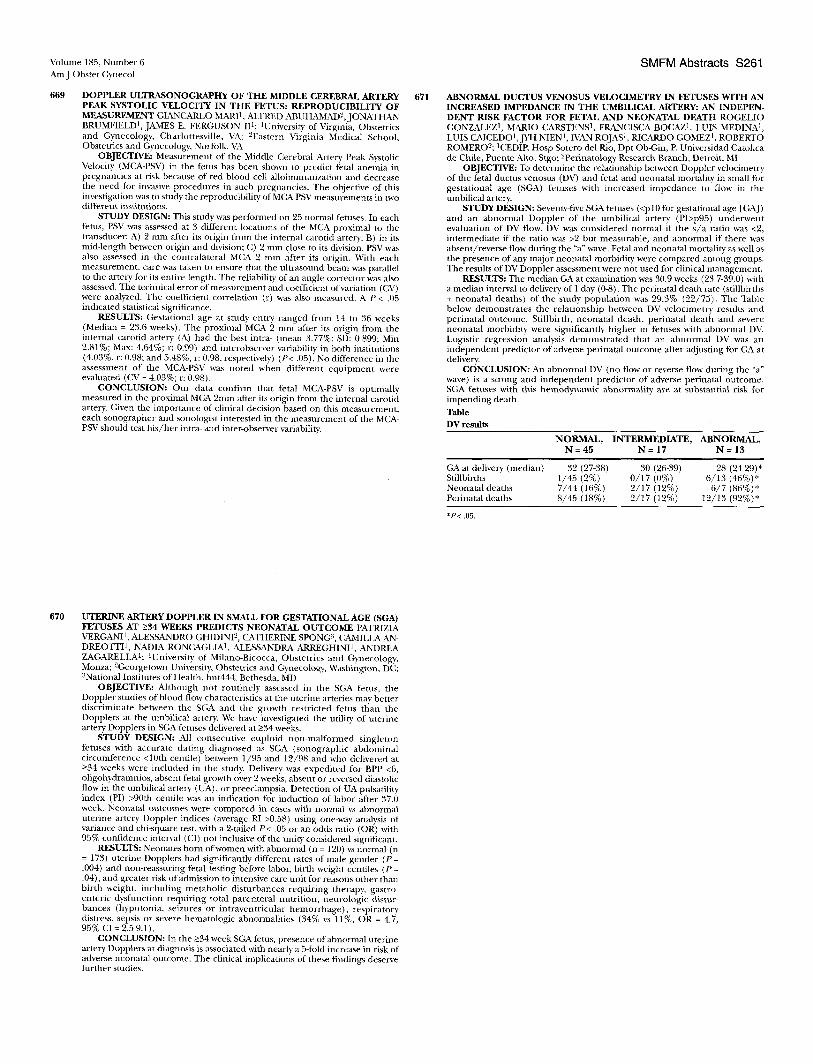
671 ABNORMAL DUCTUS VENOSUS VELOCIMETRY IN FETUSES WITH AN INCREASED IMPEDANCE IN THE UMBILICAL ARTERY: AN INDEPEN- DENT RISK FACTOR FOR FETAL AND NEONATAL DEATH ROGELIO GONZALEZ 1, MARIO CARSTENS 1, FRANCISCA BOCAZ 1, LUIS MEDINA 1, LUIS CAICEDO1, JYH NIEN ~, ]VAN ROJAS l, RICARDO GOMEZ I, ROBERTO ROMERO'-'; 1CEDIE Hosp Sotero del Rio, Dpt Ob-Gin, P. Universidad Catolica de Chile, Puente Alto, Stgo; 2perinatology Research Branch, Detroit, MI
OBJECTIVE: To determine the relationship between Doppler velocimetry of the fetal ductus venosus (DV) and fetal and neonatal mortality in small for gestational age (SGA) fetuses with increased impedance to flow in the umbilical artery.
STUDY DESIGN: Seventy-five SGA fetuses (<pl0 for gestational age [GA]) and an abnormal Doppler of the umbilical artery (Pl>p95) underwent evaluation of DV flow. DV was considered normal if the s /a ratio was <2, intermediate if the ratio was >2 but measurable, and abnormal if there was absent/reverse flow during the "a" wave, Fetal and neonatal mortality as well as the presence of any major neonatal morbidity were compared anmng groups. The results of DV Doppler assessment were not used for clinical management.
RESULTS: The median GA at examination was 30.9 weeks (23.7-39.0) with a median interval to delivery of 1 day (0-8). The perinatal death rate (stillbirths + neonatal deaths) of the study population was 29.3% (22/75). The Table below demonstrates the relationship between DV velocimetry results and perinatal outcome. Stillbirth, neonatal death, perinatal death and severe neonatal morbidity were significantly higher in fetuses with abnormal DV. Logistic regression analysis demonstrated that an abnormal DV was an independent predictor of adverse perinatal outcome "after adjusting for GA at delivery.
CONCLUSION: An abnormal DV (no flow or reverse flow during the "a" wave) is a strong and independent predictor of adverse perinatal outcome. SGA fetuses with this hemodynamie abnormality are at substantial risk for impending death.
Table DV results
NORMAL, INTERMEDIATE, ABNORMAL, N = 4 5 N = 17 N = 13
GA at delivery (median) 32 (27-38) 30 (26-39) 28 (24-29)* Stillbirths 1/45 (2%) 0/17 (0%) 6/13 (46%)* Neonatal deaths 7/44 (16%) 2/17 (12%) 6/7 (86%)* Perinatal deaths 8/45 (18%) 2/17 (12%) 12/13 (92%)*
*P< .05.
670 UTERINE ARTERY DOPPLER IN SMALL FOR GESTATIONAL AGE (SGA) FETUSES AT _>34 WEEKS PREDICTS NEONATAL OUTCOME PATRIZIA VERGANI 1, ALESSANDRO GHIDINI 2, CATHERINE SPONG 3, CAMILLA AN- DREOTTI I, NADIA RONCAGLIA I, ALESSANDRA ARREGHINI 1 , ANDREA ZAGARELLA1; 1University of Milano-gicocca, Obstetrics m,d Gynecology, Monza; 2Georgetown University, Obstetrics and Gynecology, Washington, DC; ~National Institutes of Health, hnt444, Bethesda, MD
OBJECTIVE: Although not routinely assessed in the SGA fetus, tbe Doppler studies of blood flow characteristics at the uterine arteries may better discriminate between the SGA and the growth restricted fetus than the Dopplers at the umbilical artery. We have investigated the utility of uterine artery Dopplers in SGA tetuses delivered at ->34 weeks.
STUDY DESIGN: All consecutive euploid non-malformed singleton fetuses with accurate dating diagnosed as SGA (sonograpbic abdominal circumference <10th centile) between 1/95 and 12/98 and who delivered at ->34 weeks were included in the study. Delivery was expedited for BPP <6, oligohydramnios, absent fetal growth over 2 weeks, absent or reversed diastolic flow in the umbilical artery (UA), or preeclampsia. Detection o fUA pulsatility index (PI) >90th centile was an indication for induction of labor after 37.0 week. Neonatal outcomes were compared in cases with normal vs abnormal uterine artery Doppler indices (average RI >0.58) using one-way analysis of variance and chi-square lest, with a 2-tailed P< .05 or an odds ratio (OR) with 95% confidence interval (CI) not inclusive of the unity considered significant.
RESULTS: Neonates born ofwolnen with abnormal (n - 120) vs normal (n = 173) uterine Dopplers had significantly different rates of male gender ( P - .004) and non-reassuring fetal testing before labor, birth weight centiles (P = .04), and greater risk of admission to intensive care unit for reasons other than birth weight, including metabolic disturbances requiring therapy, gastro- enteric dysfunction requiring total parenteral nutrition, neurologic distur- bances (hypotonia, seizures or intraventricular hemorrhage) , respiratory distress, sepsis or severe hematologic abnormalities (34% vs 11%, OR = 4.7, 95% CI = 2.5-9.1).
CONCLUSION: In the ->34 week SGA fetus, presence of abnormal uterine artery Dopplers at diagnosis is associated with nearly a 5-fold increase in risk of adverse neonatal outcome. The clinical implications of these findings deserve further studies.