-
8/9/2019 4yo Male Abd Pain x 1wk
1/38
Problem RoundsMay 18, 2006
Almost 4 year old male
with abdominal pain for 1 week
-
8/9/2019 4yo Male Abd Pain x 1wk
2/38
CC: abdominal pain x 1 week
HPI: Almost 4 year old Hispanic male was in usual state
of health until one week prior to admission when he
began to have abdominal pain. Patient began on 4/30/06
to complain of diffuse abdominal pain, greatest
immediately after eating. Patients abdomen also was
noted to swell and become taut. Mom would note relief
from pain after the patient had a bowel movement butcontinued
swelling. No fever, vomiting, or diarrhea.
Patient was having regular bowel movements (1/day,
brown, soft, NB but decreased in caliber-pinky size). No
history of constipation. No change in diet. No other
sickcontacts or other family members with similar symptoms.
No recent URI or sore throat symptoms.
instructed parents to bring patient to WCH PER due to
abnormalities in his labs.
-
8/9/2019 4yo Male Abd Pain x 1wk
3/38
HPI Continued: Six days PTA, mom took patient to local
clinic
as patient had an episode of vomiting (NB/NB, looked like
food,
small amt) and continued abdominal pain. He had begun to
have
decrease appetite and only wanted to lay down due to pain
andabdominal swelling. New symptom was the onset of headache
with abdominal pain. At the clinic, a hemacue was checked as
well as urine and mom was told everything was normal and the
abdominal pain was due to gas. The patient continued to
haveabdominal pain and swelling now drinking only milk and
orange juice with some fruit. Patient had another similar
episode of vomiting the following day and at noon on day of
admission.
Four days PTA, patients eyes became swollen and he was
barely
able to open his eyes for 4 days, resolving one day PT coming
to
the ER. No warmth or redness of the eyes, discharge or
tearing,
and no itchiness.
-
8/9/2019 4yo Male Abd Pain x 1wk
4/38
HPI Continued: On day of admission, mom brought
patient to Outside Hospital due increased abdominal
pain, abdominal swelling and now swelling of BLE and R
cheek. Patient developed bilateral lower extremities
(describes as the top of his feet) swelling 2 days PTA and
had stopped walking at home- now spending the entire
day laying on the couch or bed. No redness, warmth or
color change associated with the swelling. On morning
ofadmission mom states patient awoke with swelling of his
right cheek and that both cheeks look red. Swelling does
not appear to be painful to the patient but mom notes he
would intermittently touch his right cheek- puzzled.At Outside
Hospital, mom states blood and urine were
obtained and then the ER physician instructed parents to
bring patient to WCH PER due to abnormalities in his
labs.
-
8/9/2019 4yo Male Abd Pain x 1wk
5/38
Take a moment
to consider your differential diagnosis
-
8/9/2019 4yo Male Abd Pain x 1wk
6/38
ROS:
General: no fevers, no night sweats, no chills, no observed
weight loss
Neuro: + headache with abdominal pain
CVS: no chest pain
Pulm: no SOB or WOB, + dry intermittent cough 1-2
days PTA
Abd: no diarrhea, normal BM 1/day, + vomiting x 3Renal/GU: no
dysuria, hematuria, polyuria
Derm: no rash or bruising
PMD: a clinic, no regular PMD
-
8/9/2019 4yo Male Abd Pain x 1wk
7/38
Birth Hx: FT, NSVD at Outside Hospital, +PNC, no
complications with pregnancy or labor. Spent one day in
the hospital, birth weight 9 lbs, 6 oz.
PMHx: none
PSurgHx: none
Hospitalizations: none
All: NKDA
Meds: Tylenol PRN headache/abdominal pain- giventwice
Diet: Well balance diet. Fast food once/3 weeks. + candy-
lollipops and chocolate.
24oz of milk per day, 16 oz juice, some water. No
vitamins
-
8/9/2019 4yo Male Abd Pain x 1wk
8/38
FH: mom- 24, father 25, mom works at fast food
restaurant, father works as a plumber. There are two
children- patient 31/2 year old male and 2 year old sister.
No family history of asthma, DM, cancer, HTN, CAD,
MI/strokes, GI, kidney or rheumatologic disease
SH: Lives with parents in 2 bedroom house.
No pets, alcohol, tobacco, drugs, violence, guns.
Patient in preschool- no known illnesses/outbreaks,enjoys
school, likes to sing his ABCs.
No sick contacts. No recent travel or foreign visitors, no
exotic foods.
DevHx: walk at 8 months, first words mama at 10
months. Bilingual, speech fully understandable. Dress
himself, rides a tricycle with helmet.
-
8/9/2019 4yo Male Abd Pain x 1wk
9/38
Admission PE:
Temp 97.8F BP 93/61 HR 105 RR 20 Pain 0/10
Wt 22kg (>95th%) Ht- 109 cm (>95th%) BMI- 18.5
(>95th%)
Gen: well-developed, well-nourished male, smiling, cooperative,
NAD
HEENT: NCAT, PERRL, EOM intact, sclera clear, no periorbital
edema, TMclear bilateral, nares turbinates non-erythematous, +
dried discharge, no
polyps, MMM, good dentition, no oral/mucosal lesions, OP clear,
tonsils 2+ no
exudates, no erythema, neck supple, FROM, no palpable thyroid, +
facial
symmetry, fullness to R lower cheek, redness to both cheeks,
NT
Lymph: no LAD- cervical, posterior, axillary or inguinalCV: RRR,
normal S1 and S2, no m/r/g
Pulm: CTA B/L, slightly decreased BS bilateral bases, dullness
to percussion
BL bases, no w/r/r, no retractions
Abd: mildly distended, positive BS, NT, no visible fluid wave,
no HSM, no
massesGU: Tanner 1 male, uncircumcised, testes down B/L, mild
edema scrotum/fat
pad, NT
Ext: no c/c. No edema on B/L feet, no sacral edema, no other
swelling of any
extremities. 2+ distal pulse. CR~ 2 seconds
Neuro: CN II-XII intact, strength 5/5, DTR 2+ bilaterally,
normal gait
Skin: no petechiae/purpura, no ecchymoses, no rash, no jaundice
or pallor
-
8/9/2019 4yo Male Abd Pain x 1wk
10/38
ER course:
Arrived at 1316
Vitals: T- 97 (ax), BP 97/57, HR 119 RR 24
pain 0/10
Cc: abdominal pain x 1 week and mom notes increasing
abdominal girth
Was seen at OSH and referred with lab results:
albumin 1.3, radiology report of small ascites and BL
smallpleural effusions, hemoconcentrated H/H, ua- trace protein
Abdominal girth measured: 65.4 cm
-
8/9/2019 4yo Male Abd Pain x 1wk
11/38
ER PE:
Gen: asleep, arousable, smiling, in NAD
HEENT: NCAT, PERRL, EOM intact, no periorbital edema,
TM clear B/L, dried discharge noted on B/L nares, MMM, OP
clear, no exudates, neck supple, no LAD
Pulm: CTABL, decreased BS at bilateral bases, + dullness to
percussion at bases
CV: tachycardic, RR, no m/r/gAbd: soft, NT, slight distension, +
hyperactive BS, no HSM
GU: Tanner I male, uncircumscribed, testes descended BL,
slight
scrotal edema
Back: no deformities
Ext: no c/c/e, pulses 2+ cap refill
-
8/9/2019 4yo Male Abd Pain x 1wk
12/38
ER Plan:
admission- fluid management
diagnosis-
abdominal pain
hypoalbuminemia
R/O nephrotic syndrome vs protein losing gastroenteropathy,
R/O spontaneous bacterial peritonitis
labs- CBC, TPN panel, PT/PTT, blood culture, C3/C4, urine
dip,micro and culture, repeat CXR, KUB
-
8/9/2019 4yo Male Abd Pain x 1wk
13/38
Admission Plan- spoke with Renal and GI Attendings
Neuro- monitor pain- abdominal, activity bed rest
CVS- HDS
Pulm- CXR, SORA, watch for S/S respiratory distress, O2 sat
Q4
FEN/GI- regular diet, no fluid restriction
Renal- strict I/O, maintain balance
ID- watch fever- SBP, f/u urine and blood culturesHeme- H/H
hemoconcentrated- 3rd spacing
Labs:
total IgA, anti-endomysial IgA and anti-tranglutaminase IgA
upper GI w/contrast- increase gastric folds
CMV and h.pylori
Studies
CXR- reassess pleural effusions
KUB
Upper GI
-
8/9/2019 4yo Male Abd Pain x 1wk
14/38
Take a moment
to consider your differential diagnosis
-
8/9/2019 4yo Male Abd Pain x 1wk
15/38
Labs
-
8/9/2019 4yo Male Abd Pain x 1wk
16/38
Labs Continued
-
8/9/2019 4yo Male Abd Pain x 1wk
17/38
Labs Continued
-
8/9/2019 4yo Male Abd Pain x 1wk
18/38
CXR: Expiratory film, Left pleural effusion,
interstitial prominence suggestive of interstitial edema
-
8/9/2019 4yo Male Abd Pain x 1wk
19/38
KUB: nobg pattern
-
8/9/2019 4yo Male Abd Pain x 1wk
20/38
Take a moment
to consider your differential diagnosis
U GI S
-
8/9/2019 4yo Male Abd Pain x 1wk
21/38
Upper GI Scout
Film
U GI
-
8/9/2019 4yo Male Abd Pain x 1wk
22/38
Upper GI
Continued
U GI
-
8/9/2019 4yo Male Abd Pain x 1wk
23/38
Upper GI
Continued
-
8/9/2019 4yo Male Abd Pain x 1wk
24/38
U GI
-
8/9/2019 4yo Male Abd Pain x 1wk
25/38
Upper GI
Continued
U GI
-
8/9/2019 4yo Male Abd Pain x 1wk
26/38
Upper GI
Continued
-
8/9/2019 4yo Male Abd Pain x 1wk
27/38
Take a moment
to consider your differential diagnosis
-
8/9/2019 4yo Male Abd Pain x 1wk
28/38
Hospital Course
5/9/06 HD#1
GI Consult: acute onset albumin with absence of proteinuria-
most
likely protein losing enteropathy- infantile Menetriers
disease(associated with CMV) Celiac less likely, onset of
malrotation
possible.
UGI: thickened folds consistent with Menetriersdisease
Progress Note: appetite- jello, milk, UOP 1.5 cc/hr, started
highprotein diet
5/10/06 HD#2
Progress Note: headache, + intermittent cough, PO- liquid,
now
solids, nutrition teaching, started on zinc 1 mg/kg (due low alk
phos),
UOP 1.2 cc/hr
Labs: alb- 1.6 (1.8)
-
8/9/2019 4yo Male Abd Pain x 1wk
29/38
Hospital Course
5/11/06 HD#3
Progress Note: abd pain. FROC- abdominal girth and scrotum
size. Abdominal girth- 67 cm (65 cm) PE-2+ tibial edema,
dullnessabdomen, distended, scrotal edema. Later oxygen sat
93-94%,
ordered CXR, started oxygen 0.5L- 98% sats. PE- crackles
B/L.
Increased 1L then down 0.5L. Labs- alb- 1.5 (1.6)
5/12/06 HD#4GI Consult: PE ascites, scrotal edema, consider
single trial albumin
(1gm/kg) and lasix (1 mg/kg). likely to only be transient
benefit but
may be useful in improving mucosal function and subsequent
increase in protein absorption.
Progress Note: UOP 0.9 cc/hr, PE- distended, dullness,
scrotal
edema, 1+ pitting edema sacral, continue oxygen,
albumin/lasix
Resident On Call: abdominal girth- 70cm, comfortable, 96-98%
0.5L NC, pedal and scrotal edema
Labs: alb- 1.7 (1.5)
-
8/9/2019 4yo Male Abd Pain x 1wk
30/38
Hospital Course
5/13/06 HD#5
Progress Note: UOP 4.2 cc/hr, decrease to 67 cm,
frustrations
ID Consult: CMV positive, rec- gancicyclovir x 7days
Labs: alb- 2.0 (1.7)
5/14/06 HD#5
Progress Note: no pain/swelling, girth 65 cm, no scrotal edema,
wean
to RA5/15/06 HD#6
Progress Note: appetite and activity, girth-66 cm, RA, cough,
rales
on exam, UOP 3.4 cc/hr
Labs: alb- 2.2 (2.0)5/16/06 HD#7
Progress Note: Good enery, regular appetite, walking, girth 62
cm
Labs: alb- 2.4 (2.5)
-
8/9/2019 4yo Male Abd Pain x 1wk
31/38
Menetriers Disease
Hyperplastic gastropathy is a rare condition characterized
by
giant gastric folds associated with epithelial hyperplasia.
Two
clinical syndromes have been identified: Mntriers disease anda
variant of it referred to as hyperplastic, hypersecretory
gastropathy, and Zollinger-Ellison syndrome.
Mntriers disease is typically associated with protein-losing
gastropathy and with hypochlorhydria, whereas the
hyperplastic,
hypersecretory variant is associated with increased or
normalacid secretion and parietal and chief cell hyperplasia, with
or
without excessive gastric protein loss.
Other more common conditions can also cause enlarged gastric
folds, including gastric neoplasm (lymphoma,
carcinoma),granulomatous gastritides, gastric varices, infectious
gastritis
(particularlyH. pyloriand CMV), and eosinophilicgastritis.
Resolution ofH. pylorihypertrophic lymphocytic gastritis
with
antibiotics may result in reversal of excess protein loss.
Taken From Feldman: Sleisenger & Fordtran's Gastrointestinal
and Liver Disease, 7th ed.
-
8/9/2019 4yo Male Abd Pain x 1wk
32/38
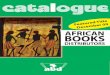
Examples of Hyperplastic gastropathy with giant gastric
folds
Mntriers disease
Zollinger-Ellison syndrome
Taken From Feldman: Sleisenger & Fordtran's Gastrointestinal
and Liver Disease, 7th ed.
-
8/9/2019 4yo Male Abd Pain x 1wk
33/38
In one series, 31 patients with large gastric folds of
uncertain etiology underwent full-thickness gastric mucosal
biopsies. Six patients showed the features of Mntriers
disease,
1 showed the features of hyperplastic,
hypersecretorygastropathy, and 6 showed features of
Zollinger-Ellison
syndrome.The remaining 18 (the majority) had peptic ulcer
disease. (Komorowski R, Caya J: Hyperplastic gastropathy
clinicopathologic correlation. Am J Surg Pathol 15:577, 1991.)
The enlarged gastric folds in Mntriers disease are dueto
foveolar cell hyperplasia, edema, and variable degrees of
inflammation. Patients may present with weight loss,
epigastric
pain, vomiting, anorexia, dyspepsia, hematemesis, and
positive
fecal occult blood tests. The mechanism responsible for the
low
gastric acid secretion is unclear, but it could be related
to
transforming growth factor- (TGF-) or its closely related
peptide, epidermal growth factor (EGF).
Taken From Feldman: Sleisenger & Fordtran's Gastrointestinal
and Liver Disease, 7th ed.
-
8/9/2019 4yo Male Abd Pain x 1wk
34/38
-
8/9/2019 4yo Male Abd Pain x 1wk
35/38
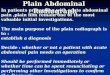
Gastric resections from patients with Mntriers disease
typically show large polypoid gastric folds or large
cerebriform
gastric folds with antral sparing.
Total gastrectomy specimen
in a patient with Mntriers disease
(right, body, with hyperplastic mucosa
and cerebriform rugal folds;
left, antrum, with relative sparing)
Taken From Feldman: Sleisenger & Fordtran's Gastrointestinal
and Liver Disease, 7th ed.
-
8/9/2019 4yo Male Abd Pain x 1wk
36/38
In the absence of a gastrectomy, a full-thickness gastric
mucosal
biopsy is required to adequately assess the gastric histology
in
patients with hyperplastic gastropathy. The predominant
microscopic feature of Mntriers disease and hyperplastic,
hypersecretory gastropathy is foveolar hyperplasia with
cystic
dilation.
The parietal and chief cells may be decreased and replaced
by
mucous glands. Inflammation in hyperplastic gastropathies is
variable and may be absent.
Histology of
Mntriers disease
showing enlarged
folds with foveolar
hyperplasia, cysticallydilated glands, and
minimal gastritis
Taken From Feldman: Sleisenger & Fordtran's Gastrointestinal
and Liver Disease, 7th ed.
-
8/9/2019 4yo Male Abd Pain x 1wk
37/38
Ideal treatment of hyperplastic gastropathy is unclear,
because the condition is rare and controlled trials are
lacking.H.
pyloriinfection should be treated, if present, and the
entire
syndrome may resolve. Symptoms may improve withantisecretory
agents (histamine2 [H2 ] receptor antagonists,
anticholinergic agents, proton pump inhibitors), especially if
the
patient has Zollinger-Ellison syndrome or normogastrinemic
hyperplastic, hypersecretory gastropathy. It has been
suggestedthat H2 blockers and anticholinergics reduce gastric
protein loss
by strengthening intercellular tight junctions. Some patients
with
Mntriers disease have responded to corticosteroids,
octreotide, antifibrinolytic agents, or monoclonal antibody
against the EGF receptor. Partial or total gastric resection
is
reserved for severe complications, such as refractory or
recurrent bleeding, obstruction, severe hypoproteinemia, or
cancer development.
Taken From Feldman: Sleisenger & Fordtran's Gastrointestinal
and Liver Disease, 7th ed.
-
8/9/2019 4yo Male Abd Pain x 1wk
38/38
Eosinophilic gastroenteritis is a disease characterized by
tissue
eosinophilia that can involve any layer or layers of the gut
wall.
Kaijser is credited with the first description of eosinophilic
gastroenteritis in
1937.
A definite diagnosis must fulfill the following criteria:
(1) the presence of GI symptoms
(2) eosinophilic infiltration of one or more areas of GI tract
on biopsy
(3) absence of eosinophilic involvement of multiple organs
outside GI tract
(4) absence of parasitic infestation.
Peripheral blood eosinophilia is absent in at least 20% of
patients and should
not be considered a diagnostic criterion. Furthermore, food
intolerance or
allergy is not required for the diagnosis, because many patients
have no
objective evidence of these problems.
The disease is rare; although increasing numbers of cases have
been reportedin the medical literature, the incidence is difficult
to estimate, because some
patients are probably undiagnosed and surely unreported.
Patients typically
present in the third through fifth decades of life, but the
disease can affect any
age group. An equal gender distribution or a slight male
preponderance has
b t d