Embed Size (px)
Citation preview

Plain Abdominal Plain Abdominal RadiographRadiographIn patients presenting with acute abdominal In patients presenting with acute abdominal
pain ,plain film remain one of the most pain ,plain film remain one of the most valuable initial investigations.valuable initial investigations.
The main purpose of the plain radiograph is The main purpose of the plain radiograph is to :to :establish a diagnosis establish a diagnosis
Decide : Decide : whether or not a patient with acute whether or not a patient with acute abdominal pain needs an operationabdominal pain needs an operation
Should be performed immediately or Should be performed immediately or whether time can be spent resuscitating or whether time can be spent resuscitating or performing other investigations to confirm performing other investigations to confirm the diagnosis .the diagnosis .

INTERPRETATION OF THE PFA
There are some basic rules regarding interpretation of the PFA
NameIt is always important to ensure that the correct radiograph for the correct patient is being viewed.
SexSome pathological processes may be commoner in either one of the sexes. Obviously the genitourinary tracts also differ.
AgeOld or young? Different pathological processes may vary between those of different ages.

Date of investigation
Many radiographs may be present in the patients ‘X-ray bag’ and it is important that the appropriate radiograph is being viewed. Previous radiographs are helpful for comparison.
MarkerThe right or left side should be labeled on the plain abdominal film.
PositionA supine AP (anteroposterior) film is usually obtained. suspected bowel obstruction an erect abdominal film can be helpful Occasionally LT lateral decubitus views may be performed to showintraperitoneal free air.
Having completed these steps, it is now possible to systematically interpret the abdominal film.

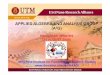
1 Gas in caecum2 Gas in descending colon 3 Gas in stomach4 Gastric rugal folds5 Twelfth rib6 Right kidney 7 L2 vertebra 8 Liver 9 Transverse process of L110 Right psoas muscle 11 Left psoas muscle 12 Head of femur 13 Pubic symphysis14 Right sacro-iliac joint

The formation of a radiographic The formation of a radiographic image depends on the structure & image depends on the structure & size of the organs within the size of the organs within the abdomen.abdomen.
Gas which absorbs least X-rays Gas which absorbs least X-rays appears black or dark grey.appears black or dark grey.
Fat is usually seen as dark grey lines.Fat is usually seen as dark grey lines. Soft tissues appear very light grey Soft tissues appear very light grey
with large soft tissue masses with large soft tissue masses appearing almost white.appearing almost white.
Calcification which absorbs most X-Calcification which absorbs most X-rays appears white.rays appears white.

Main purpose of horizontal beam is to detect Main purpose of horizontal beam is to detect air fluid air fluid levels & free intraperitoneal gas.levels & free intraperitoneal gas.
Relatively large amounts of gas normally Relatively large amounts of gas normally present in the stomach & colon; only a present in the stomach & colon; only a small amount is usually seen in the SI.small amount is usually seen in the SI.
Short air fluid levels in the SI & LI are Short air fluid levels in the SI & LI are normal.normal.
Abnormal AFL when they are numerous/ Abnormal AFL when they are numerous/ bowel is dilatedbowel is dilated

Stomach is identified by gastric rugae & Stomach is identified by gastric rugae & relatively long AFL.relatively long AFL.
Look for extraluminal gas.Look for extraluminal gas.
Look for Ascites & soft tissue masses.Look for Ascites & soft tissue masses.
Detect & localize calcification.Detect & localize calcification.
Identify liver & spleenIdentify liver & spleen
Look for Renal, psoas & bladder outlines.Look for Renal, psoas & bladder outlines.




The outlines of the kidneys The outlines of the kidneys psoas muscles bladder and the psoas muscles bladder and the posterior borders of the liver and posterior borders of the liver and spleen can often be identified by spleen can often be identified by the fat which surrounds them. the fat which surrounds them.

Distinction between small & large bowel Distinction between small & large bowel dilatation can be difficult.dilatation can be difficult.
Three to five fluid levels < 2.5 cm in length may Three to five fluid levels < 2.5 cm in length may be seen particularly in the right lower quadrant be seen particularly in the right lower quadrant without any evidence of intestinal without any evidence of intestinal obstruction/paralytic ileus.obstruction/paralytic ileus.
>2AFL in dilated small bowel >2AFL in dilated small bowel << 2.5 cm is 2.5 cm is abnormal & usually indicates paralytic abnormal & usually indicates paralytic ileus/intestinal obstruction but may also be ileus/intestinal obstruction but may also be seen in normal radiographs.seen in normal radiographs.
When sever pain or when respiration is labored When sever pain or when respiration is labored
such as in pneumonia or asthma more air is such as in pneumonia or asthma more air is swallowed. swallowed.

No. of AFL.No. of AFL. Position.Position. caliber.caliber. Radius of curvatureRadius of curvature Solid faeces.Solid faeces. Haustra(Always asc. & Tr Haustra(Always asc. & Tr
colon).colon). Valvulae conniventes(<distal Valvulae conniventes(<distal
ileum)ileum)

Small bowelSmall bowel Large bowelLarge bowel
HaustraHaustra AbsentAbsent PresentPresent
Vavulae Vavulae connventesconnventes
Present in Present in jejunumjejunum
Absent Absent
Number of loopsNumber of loops Many Many Few Few
Distribution of Distribution of loopsloops
Central Central Peripheral Peripheral
Radius of Radius of curvature of curvature of loops loops
Small Small Large Large
Diameter of loopDiameter of loop 30-50 mm.30-50 mm. 50 mm+50 mm+
Solid faecesSolid faeces Absent Absent May be presentMay be present



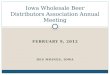
Small bowel obstructionSmall bowel obstruction




String of beads signString of beads sign

CAUSES OF BOWEL CAUSES OF BOWEL DILATATAIONDILATATAION
Mechanical obstructionMechanical obstruction P ileusP ileus Acute ischemiaAcute ischemia Inflammatory bowel diseaseInflammatory bowel disease Local peritonitis.Local peritonitis. GastroenteritisGastroenteritis Closed loop obstructionClosed loop obstruction

Extraluminal GasExtraluminal GasPneumperitoneumPneumperitoneum
Almost always: GIT perforation or after Almost always: GIT perforation or after surgical interventionsurgical intervention
Most common cause Perforated PU-2/3 Most common cause Perforated PU-2/3 recognized radiologicallyrecognized radiologically
Largest amount LILargest amount LI
Smallest amount SISmallest amount SI

PneumperitoneumPneumperitoneum
A Appendictis very rareA Appendictis very rare
Normal after laprotomy 7d adults; 1d childrenNormal after laprotomy 7d adults; 1d children
CXR better than plain AXRCXR better than plain AXR
doubtful-RT lat. decubitusdoubtful-RT lat. decubitus
Easier diagnosis of Air under RT>LT Easier diagnosis of Air under RT>LT hemidiaphragmhemidiaphragm

Extraluminal GasExtraluminal GasAbscess Abscess
bubbles or AFLbubbles or AFL
Mass effectMass effect
Pleural/pulmonary shadowsPleural/pulmonary shadows
Intramural gasIntramural gas
Linear/ovalLinear/oval
PneumobiliaPneumobilia




PneumobiliaPneumobilia Fistula between gallbladder & bowel Fistula between gallbladder & bowel
from passage of gallstone.from passage of gallstone.
Following biliary surgery or endoscopic Following biliary surgery or endoscopic sphincterotomy.sphincterotomy.
Following percutaneous or endoscopic Following percutaneous or endoscopic cholangiography.cholangiography.

Perforated peptic ulcer [ into bile ducts ].Perforated peptic ulcer [ into bile ducts ].
Emphysematous cholangitis [gallbladder Emphysematous cholangitis [gallbladder usually enlarged].usually enlarged].
Physiological – owing to lax sphincter.Physiological – owing to lax sphincter.

ABDOMINAL ABDOMINAL CALCIFICATIONCALCIFICATION
The commonest types of abdominal The commonest types of abdominal calcification are non-visceral and often calcification are non-visceral and often unrelated to the presenting clinical unrelated to the presenting clinical problem:problem:
CommonCommon
1.1. AtherosclerosisAtherosclerosis
2.2. Mesenteric lymph nodesMesenteric lymph nodes
3.3. PhlebolithsPhleboliths
4.4. Rib cartilage (normal)Rib cartilage (normal)
5.5. Injection in the buttocksInjection in the buttocks

MESENTERIC LN calcification
TBMOBILE DENSE

Fibroid Malignant ovarian massBenign-Dermoid
PhlebolithCentral lucency

Adrenal calcificationMAJORITY ASYMPTOMATICHemorrhageTBTUMORS

Vascular calcification
No useful correlation with
hemodynamic severity of vascular dis
Aortic aneurysm best on lat. view

Chronic pancreatitis-calculiPosition diagnostic

FecolithAppendicolith10% of appendicitis
Increased possibility of gangrene –perforation

GALLSTONES
Up to 20%

Hepatic calcification
HepatomaHydatid cystAbscesses&TB
GALLSTONES
RENAL STONES Project over liver shadow
COST. Cart.
Splenic calcification
MAJORITY insignificantHematomacystTBInfarction

Staghorn STONE

Gall & renal stones

FetusContraindicated

PhlebolithCentral lucency


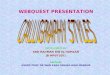
Cocaine‘Body Packer’Calcifications are not the only densities seen on PFA. Swallowed substances such astablets and smuggled capsules Of cocaine may also beseen.

Plain film signs of hepatomegalyPlain film signs of hepatomegaly
Plain film signs of splenomegalyPlain film signs of splenomegaly
Splenic traumaSplenic trauma



Any QuestionsAny Questions??
CommentsComments??

Thank youThank you