Embed Size (px)
Citation preview
VNSNY CHOICE
2017 ProviderManual
Appendix VI
Medical Management
2017 MA Authorization Requirements
2017 FIDA Authorization Requirements
Continuation of Care form – Transitional Coverage Request Form
Medical Coverage Determination Form

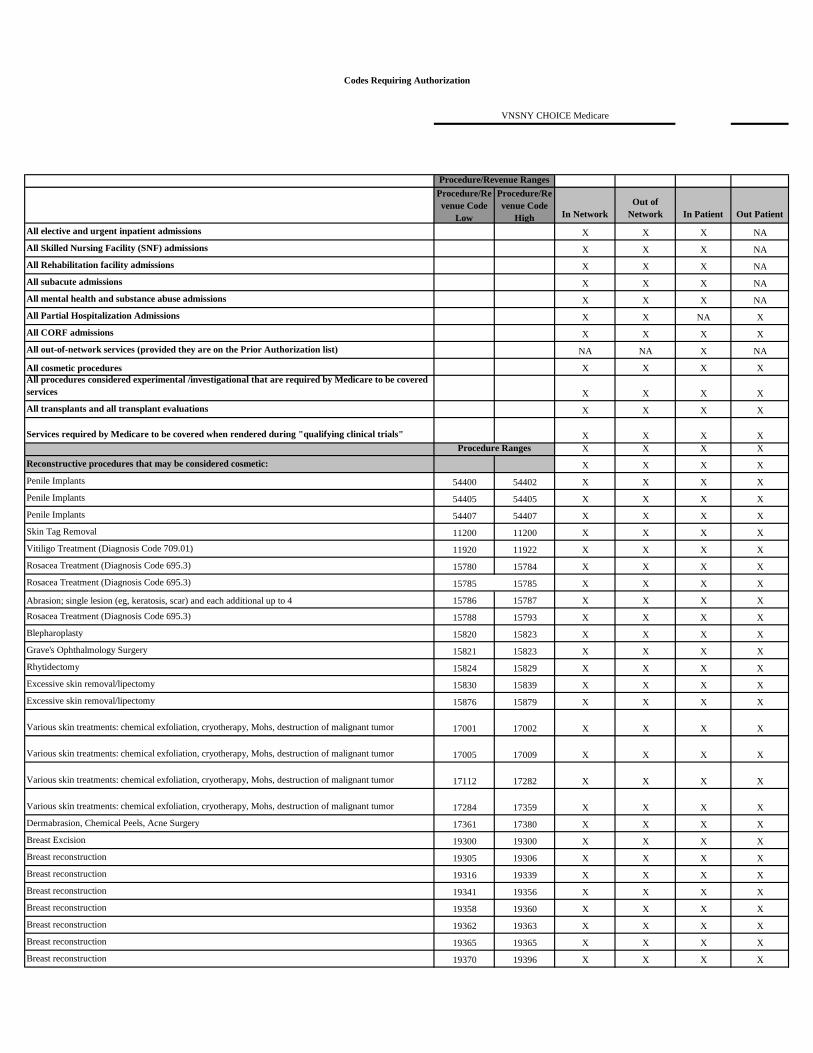
2017 MA Authorization Requirements
Procedure/Re
venue Code
Low
Procedure/Re
venue Code
High In Network
Out of
Network In Patient Out Patient
All elective and urgent inpatient admissions X X X NA
All Skilled Nursing Facility (SNF) admissions X X X NA
All Rehabilitation facility admissions X X X NA
All subacute admissions X X X NA
All mental health and substance abuse admissions X X X NA
All Partial Hospitalization Admissions X X NA X
All CORF admissions X X X X
All out-of-network services (provided they are on the Prior Authorization list) NA NA X NA
All cosmetic procedures X X X X
All procedures considered experimental /investigational that are required by Medicare to be covered
services X X X X
All transplants and all transplant evaluations X X X X
Services required by Medicare to be covered when rendered during "qualifying clinical trials" X X X X
X X X X
Reconstructive procedures that may be considered cosmetic: X X X X
Penile Implants 54400 54402 X X X X
Penile Implants 54405 54405 X X X X
Penile Implants 54407 54407 X X X X
Skin Tag Removal 11200 11200 X X X X
Vitiligo Treatment (Diagnosis Code 709.01) 11920 11922 X X X X
Rosacea Treatment (Diagnosis Code 695.3) 15780 15784 X X X X
Rosacea Treatment (Diagnosis Code 695.3) 15785 15785 X X X X
Abrasion; single lesion (eg, keratosis, scar) and each additional up to 4 15786 15787 X X X X
Rosacea Treatment (Diagnosis Code 695.3) 15788 15793 X X X X
Blepharoplasty 15820 15823 X X X X
Grave's Ophthalmology Surgery 15821 15823 X X X X
Rhytidectomy 15824 15829 X X X X
Excessive skin removal/lipectomy 15830 15839 X X X X
Excessive skin removal/lipectomy 15876 15879 X X X X
Various skin treatments: chemical exfoliation, cryotherapy, Mohs, destruction of malignant tumor 17001 17002 X X X X
Various skin treatments: chemical exfoliation, cryotherapy, Mohs, destruction of malignant tumor 17005 17009 X X X X
Various skin treatments: chemical exfoliation, cryotherapy, Mohs, destruction of malignant tumor 17112 17282 X X X X
Various skin treatments: chemical exfoliation, cryotherapy, Mohs, destruction of malignant tumor 17284 17359 X X X X
Dermabrasion, Chemical Peels, Acne Surgery 17361 17380 X X X X
Breast Excision 19300 19300 X X X X
Breast reconstruction 19305 19306 X X X X
Breast reconstruction 19316 19339 X X X X
Breast reconstruction 19341 19356 X X X X
Breast reconstruction 19358 19360 X X X X
Breast reconstruction 19362 19363 X X X X
Breast reconstruction 19365 19365 X X X X
Breast reconstruction 19370 19396 X X X X
Codes Requiring Authorization
VNSNY CHOICE Medicare
Procedure/Revenue Ranges
Procedure Ranges
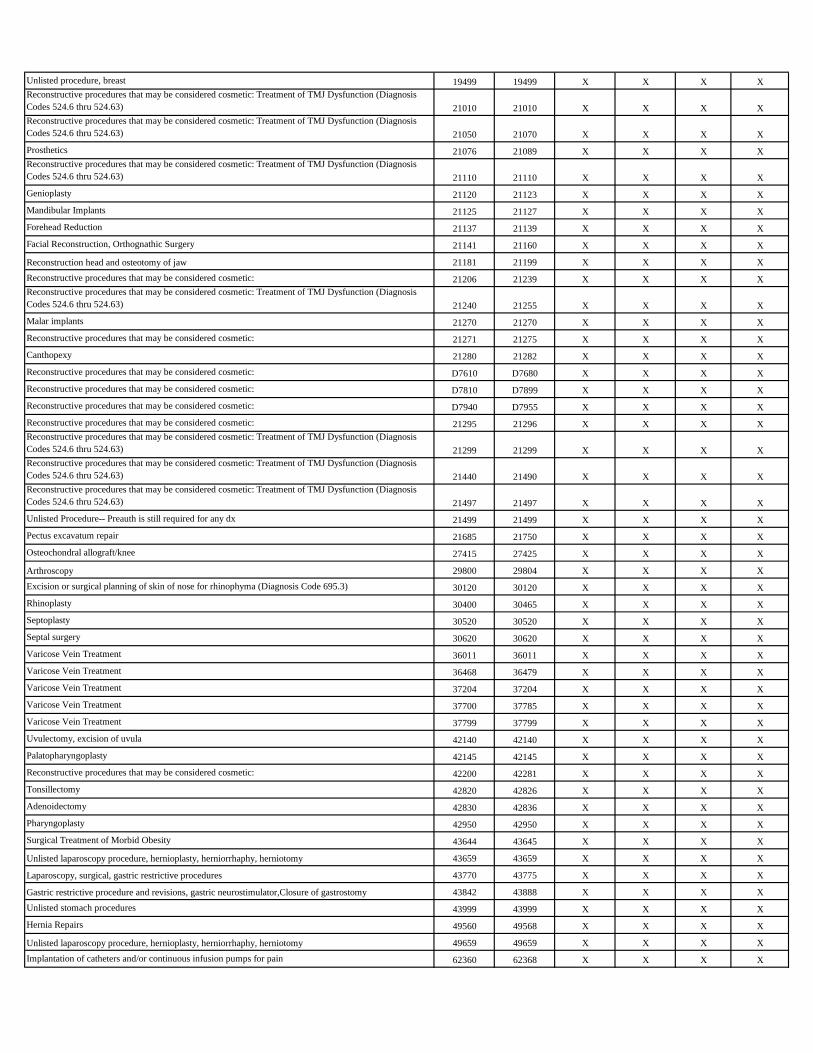
Unlisted procedure, breast 19499 19499 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21010 21010 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21050 21070 X X X X
Prosthetics 21076 21089 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21110 21110 X X X X
Genioplasty 21120 21123 X X X X
Mandibular Implants 21125 21127 X X X X
Forehead Reduction 21137 21139 X X X X
Facial Reconstruction, Orthognathic Surgery 21141 21160 X X X X
Reconstruction head and osteotomy of jaw 21181 21199 X X X X
Reconstructive procedures that may be considered cosmetic: 21206 21239 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21240 21255 X X X X
Malar implants 21270 21270 X X X X
Reconstructive procedures that may be considered cosmetic: 21271 21275 X X X X
Canthopexy 21280 21282 X X X X
Reconstructive procedures that may be considered cosmetic: D7610 D7680 X X X X
Reconstructive procedures that may be considered cosmetic: D7810 D7899 X X X X
Reconstructive procedures that may be considered cosmetic: D7940 D7955 X X X X
Reconstructive procedures that may be considered cosmetic: 21295 21296 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21299 21299 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21440 21490 X X X X
Reconstructive procedures that may be considered cosmetic: Treatment of TMJ Dysfunction (Diagnosis
Codes 524.6 thru 524.63) 21497 21497 X X X X
Unlisted Procedure-- Preauth is still required for any dx 21499 21499 X X X X
Pectus excavatum repair 21685 21750 X X X X
Osteochondral allograft/knee 27415 27425 X X X X
Arthroscopy 29800 29804 X X X X
Excision or surgical planning of skin of nose for rhinophyma (Diagnosis Code 695.3) 30120 30120 X X X X
Rhinoplasty 30400 30465 X X X X
Septoplasty 30520 30520 X X X X
Septal surgery 30620 30620 X X X X
Varicose Vein Treatment 36011 36011 X X X X
Varicose Vein Treatment 36468 36479 X X X X
Varicose Vein Treatment 37204 37204 X X X X
Varicose Vein Treatment 37700 37785 X X X X
Varicose Vein Treatment 37799 37799 X X X X
Uvulectomy, excision of uvula 42140 42140 X X X X
Palatopharyngoplasty 42145 42145 X X X X
Reconstructive procedures that may be considered cosmetic: 42200 42281 X X X X
Tonsillectomy 42820 42826 X X X X
Adenoidectomy 42830 42836 X X X X
Pharyngoplasty 42950 42950 X X X X
Surgical Treatment of Morbid Obesity 43644 43645 X X X X
Unlisted laparoscopy procedure, hernioplasty, herniorrhaphy, herniotomy 43659 43659 X X X X
Laparoscopy, surgical, gastric restrictive procedures 43770 43775 X X X X
Gastric restrictive procedure and revisions, gastric neurostimulator,Closure of gastrostomy 43842 43888 X X X X
Unlisted stomach procedures 43999 43999 X X X X
Hernia Repairs 49560 49568 X X X X
Unlisted laparoscopy procedure, hernioplasty, herniorrhaphy, herniotomy 49659 49659 X X X X
Implantation of catheters and/or continuous infusion pumps for pain 62360 62368 X X X X

Artificial intervertebral disc surgery 63001 63051 X X X X
Percutaneous implant of neuroelectrode array, epidural/Lumbar spinal fusion surgery 63650 63688 X X X X
Lumbar spinal fusion surgery 63700 63710 X X X X
Lumbar spinal fusion surgery 64550 64550 X X X X
Vision Correction surgery 65760 65760 X X X X
Repair of blepharoptosis; Correction of lid retraction/lagophthalmos/ectropion 67900 67924 X X X X
Otoplasty 69300 69320 X X X X
Osseointegrated implant 69700 69799 X X X X
Stereotactic radiosurgery 77371 77373 X X X X
Keloid Removal 77401 77401 X X X X
Varicose Vein Treatment 75894 75894 X X X X
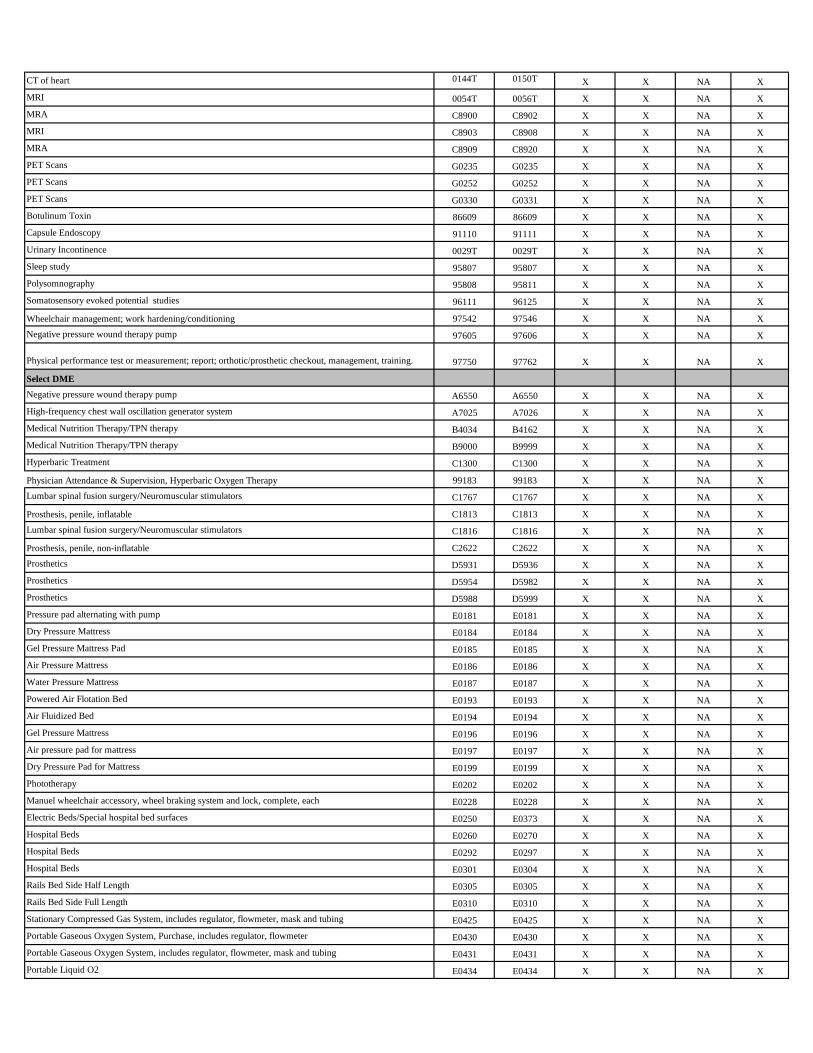
Select Radiology Procedures
MRI 70336 70336 X X NA X
MRI 70540 70543 X X NA X
MRA 70544 70549 X X NA X
MRI 70551 70559 X X NA X
MRI 71550 71552 X X NA X
MRA 71555 71555 X X NA X
MRI 72141 72158 X X NA X
MRA 72159 72159 X X NA X
MRI 72195 72197 X X NA X
MRA 72198 72198 X X NA X
MRI 73218 73223 X X NA X
MRA 73225 73225 X X NA X
MRI 73718 73723 X X NA X
MRA 73725 73725 X X NA X
MRI 74181 74183 X X NA X
MRA 74185 74185 X X NA X
MRI 75552 75556 X X NA X
CT of heart 75571 75574 X X NA X
MRI 75635 75635 X X NA X
MRI 76093 76094 X X NA X
MRI 76376 76377 X X NA X
MRI 76390 76400 X X NA X
MRI 76498 76498 X X NA X
Interstitial radiation source application 77776 77778 X X NA X
SPECT 78205 78206 X X NA X
SPECT 78320 78320 X X NA X
PET Scans 78459 78459 X X NA X
MRA 78473 78481 X X NA X
PET Scans 78491 78492 X X NA X
SPECT 78494 78494 X X NA X
MRA 78496 78496 X X NA X
SPECT 78499 78499 X X NA X
SPECT 78607 78607 X X NA X
PET Scans 78608 78609 X X NA X
SPECT 78647 78647 X X NA X
SPECT 78649 78649 X X NA X
SPECT 78710 78710 X X NA X
SPECT 78803 78803 X X NA X
SPECT 78807 78807 X X NA X
PET Scans 78811 78816 X X NA X
PET Scans 78999 78999 X X NA X
CT of heart 0144T 0150T X X NA X
MRI 0054T 0056T X X NA X
MRA C8900 C8902 X X NA X
MRI C8903 C8908 X X NA X
MRA C8909 C8920 X X NA X
PET Scans G0235 G0235 X X NA X
PET Scans G0252 G0252 X X NA X
PET Scans G0330 G0331 X X NA X
Botulinum Toxin 86609 86609 X X NA X
Capsule Endoscopy 91110 91111 X X NA X
Urinary Incontinence 0029T 0029T X X NA X
Sleep study 95807 95807 X X NA X
Polysomnography 95808 95811 X X NA X
Somatosensory evoked potential studies 96111 96125 X X NA X
Wheelchair management; work hardening/conditioning 97542 97546 X X NA X
Negative pressure wound therapy pump 97605 97606 X X NA X
Physical performance test or measurement; report; orthotic/prosthetic checkout, management, training. 97750 97762 X X NA X
Select DME
Negative pressure wound therapy pump A6550 A6550 X X NA X
High-frequency chest wall oscillation generator system A7025 A7026 X X NA X
Medical Nutrition Therapy/TPN therapy B4034 B4162 X X NA X
Medical Nutrition Therapy/TPN therapy B9000 B9999 X X NA X
Hyperbaric Treatment C1300 C1300 X X NA X
Physician Attendance & Supervision, Hyperbaric Oxygen Therapy 99183 99183 X X NA X
Lumbar spinal fusion surgery/Neuromuscular stimulators C1767 C1767 X X NA X
Prosthesis, penile, inflatable C1813 C1813 X X NA X
Lumbar spinal fusion surgery/Neuromuscular stimulators C1816 C1816 X X NA X
Prosthesis, penile, non-inflatable C2622 C2622 X X NA X
Prosthetics D5931 D5936 X X NA X
Prosthetics D5954 D5982 X X NA X
Prosthetics D5988 D5999 X X NA X
Pressure pad alternating with pump E0181 E0181 X X NA X
Dry Pressure Mattress E0184 E0184 X X NA X
Gel Pressure Mattress Pad E0185 E0185 X X NA X
Air Pressure Mattress E0186 E0186 X X NA X
Water Pressure Mattress E0187 E0187 X X NA X
Powered Air Flotation Bed E0193 E0193 X X NA X
Air Fluidized Bed E0194 E0194 X X NA X
Gel Pressure Mattress E0196 E0196 X X NA X
Air pressure pad for mattress E0197 E0197 X X NA X
Dry Pressure Pad for Mattress E0199 E0199 X X NA X
Phototherapy E0202 E0202 X X NA X
Manuel wheelchair accessory, wheel braking system and lock, complete, each E0228 E0228 X X NA X
Electric Beds/Special hospital bed surfaces E0250 E0373 X X NA X
Hospital Beds E0260 E0270 X X NA X
Hospital Beds E0292 E0297 X X NA X
Hospital Beds E0301 E0304 X X NA X
Rails Bed Side Half Length E0305 E0305 X X NA X
Rails Bed Side Full Length E0310 E0310 X X NA X
Stationary Compressed Gas System, includes regulator, flowmeter, mask and tubing E0425 E0425 X X NA X
Portable Gaseous Oxygen System, Purchase, includes regulator, flowmeter E0430 E0430 X X NA X
Portable Gaseous Oxygen System, includes regulator, flowmeter, mask and tubing E0431 E0431 X X NA X
Portable Liquid O2 E0434 E0434 X X NA X
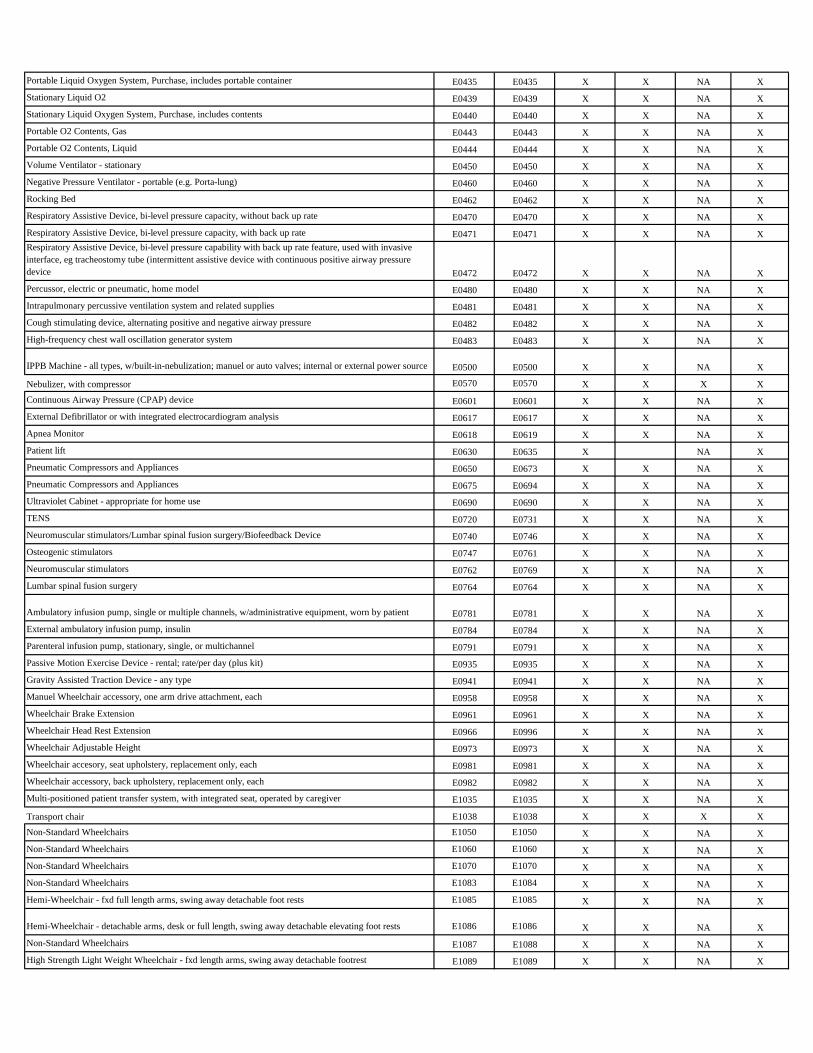
Portable Liquid Oxygen System, Purchase, includes portable container E0435 E0435 X X NA X
Stationary Liquid O2 E0439 E0439 X X NA X
Stationary Liquid Oxygen System, Purchase, includes contents E0440 E0440 X X NA X
Portable O2 Contents, Gas E0443 E0443 X X NA X
Portable O2 Contents, Liquid E0444 E0444 X X NA X
Volume Ventilator - stationary E0450 E0450 X X NA X
Negative Pressure Ventilator - portable (e.g. Porta-lung) E0460 E0460 X X NA X
Rocking Bed E0462 E0462 X X NA X
Respiratory Assistive Device, bi-level pressure capacity, without back up rate E0470 E0470 X X NA X
Respiratory Assistive Device, bi-level pressure capacity, with back up rate E0471 E0471 X X NA X
Respiratory Assistive Device, bi-level pressure capability with back up rate feature, used with invasive
interface, eg tracheostomy tube (intermittent assistive device with continuous positive airway pressure
device E0472 E0472 X X NA X
Percussor, electric or pneumatic, home model E0480 E0480 X X NA X
Intrapulmonary percussive ventilation system and related supplies E0481 E0481 X X NA X
Cough stimulating device, alternating positive and negative airway pressure E0482 E0482 X X NA X
High-frequency chest wall oscillation generator system E0483 E0483 X X NA X
IPPB Machine - all types, w/built-in-nebulization; manuel or auto valves; internal or external power source E0500 E0500 X X NA X
Nebulizer, with compressor E0570 E0570 X X X X
Continuous Airway Pressure (CPAP) device E0601 E0601 X X NA X
External Defibrillator or with integrated electrocardiogram analysis E0617 E0617 X X NA X
Apnea Monitor E0618 E0619 X X NA X
Patient lift E0630 E0635 X NA X
Pneumatic Compressors and Appliances E0650 E0673 X X NA X
Pneumatic Compressors and Appliances E0675 E0694 X X NA X
Ultraviolet Cabinet - appropriate for home use E0690 E0690 X X NA X
TENS E0720 E0731 X X NA X
Neuromuscular stimulators/Lumbar spinal fusion surgery/Biofeedback Device E0740 E0746 X X NA X
Osteogenic stimulators E0747 E0761 X X NA X
Neuromuscular stimulators E0762 E0769 X X NA X
Lumbar spinal fusion surgery E0764 E0764 X X NA X
Ambulatory infusion pump, single or multiple channels, w/administrative equipment, worn by patient E0781 E0781 X X NA X
External ambulatory infusion pump, insulin E0784 E0784 X X NA X
Parenteral infusion pump, stationary, single, or multichannel E0791 E0791 X X NA X
Passive Motion Exercise Device - rental; rate/per day (plus kit) E0935 E0935 X X NA X
Gravity Assisted Traction Device - any type E0941 E0941 X X NA X
Manuel Wheelchair accessory, one arm drive attachment, each E0958 E0958 X X NA X
Wheelchair Brake Extension E0961 E0961 X X NA X
Wheelchair Head Rest Extension E0966 E0996 X X NA X
Wheelchair Adjustable Height E0973 E0973 X X NA X
Wheelchair accesory, seat upholstery, replacement only, each E0981 E0981 X X NA X
Wheelchair accessory, back upholstery, replacement only, each E0982 E0982 X X NA X
Multi-positioned patient transfer system, with integrated seat, operated by caregiver E1035 E1035 X X NA X
Transport chair E1038 E1038 X X X X
Non-Standard Wheelchairs E1050 E1050 X X NA X
Non-Standard Wheelchairs E1060 E1060 X X NA X
Non-Standard Wheelchairs E1070 E1070 X X NA X
Non-Standard Wheelchairs E1083 E1084 X X NA X
Hemi-Wheelchair - fxd full length arms, swing away detachable foot rests E1085 E1085 X X NA X
Hemi-Wheelchair - detachable arms, desk or full length, swing away detachable elevating foot rests E1086 E1086 X X NA X
Non-Standard Wheelchairs E1087 E1088 X X NA X
High Strength Light Weight Wheelchair - fxd length arms, swing away detachable footrest E1089 E1089 X X NA X
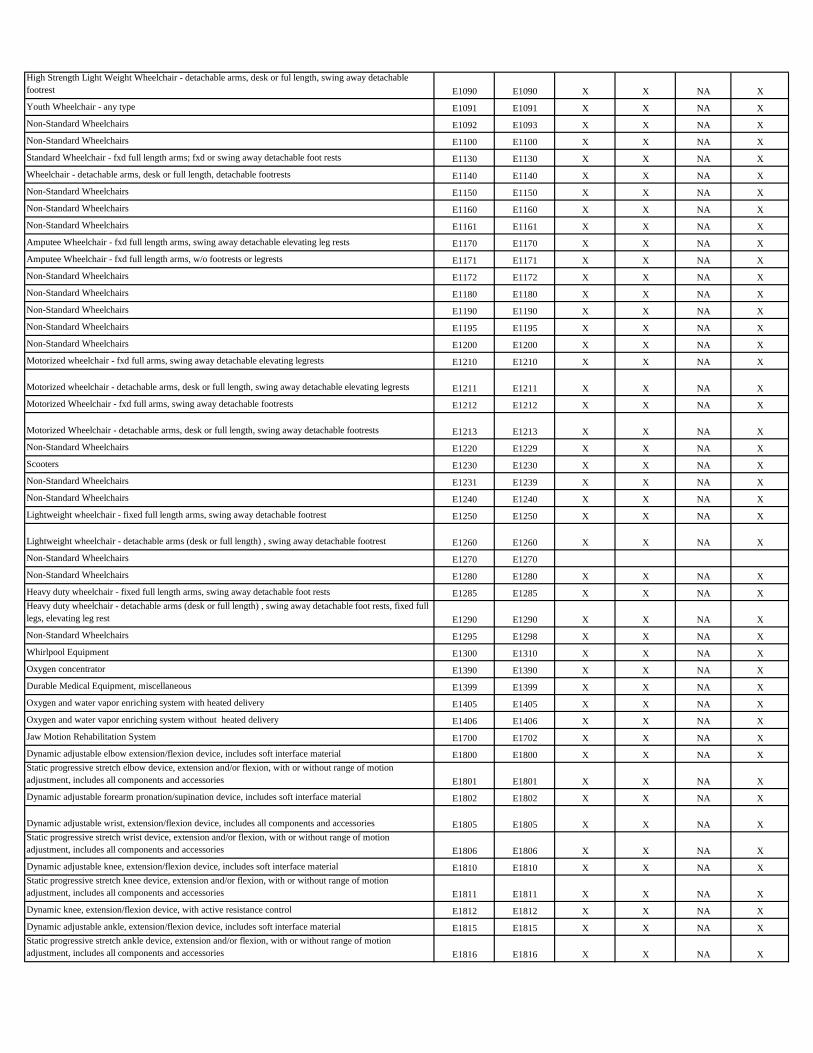
High Strength Light Weight Wheelchair - detachable arms, desk or ful length, swing away detachable
footrest E1090 E1090 X X NA X
Youth Wheelchair - any type E1091 E1091 X X NA X
Non-Standard Wheelchairs E1092 E1093 X X NA X
Non-Standard Wheelchairs E1100 E1100 X X NA X
Standard Wheelchair - fxd full length arms; fxd or swing away detachable foot rests E1130 E1130 X X NA X
Wheelchair - detachable arms, desk or full length, detachable footrests E1140 E1140 X X NA X
Non-Standard Wheelchairs E1150 E1150 X X NA X
Non-Standard Wheelchairs E1160 E1160 X X NA X
Non-Standard Wheelchairs E1161 E1161 X X NA X
Amputee Wheelchair - fxd full length arms, swing away detachable elevating leg rests E1170 E1170 X X NA X
Amputee Wheelchair - fxd full length arms, w/o footrests or legrests E1171 E1171 X X NA X
Non-Standard Wheelchairs E1172 E1172 X X NA X
Non-Standard Wheelchairs E1180 E1180 X X NA X
Non-Standard Wheelchairs E1190 E1190 X X NA X
Non-Standard Wheelchairs E1195 E1195 X X NA X
Non-Standard Wheelchairs E1200 E1200 X X NA X
Motorized wheelchair - fxd full arms, swing away detachable elevating legrests E1210 E1210 X X NA X
Motorized wheelchair - detachable arms, desk or full length, swing away detachable elevating legrests E1211 E1211 X X NA X
Motorized Wheelchair - fxd full arms, swing away detachable footrests E1212 E1212 X X NA X
Motorized Wheelchair - detachable arms, desk or full length, swing away detachable footrests E1213 E1213 X X NA X
Non-Standard Wheelchairs E1220 E1229 X X NA X
Scooters E1230 E1230 X X NA X
Non-Standard Wheelchairs E1231 E1239 X X NA X
Non-Standard Wheelchairs E1240 E1240 X X NA X
Lightweight wheelchair - fixed full length arms, swing away detachable footrest E1250 E1250 X X NA X
Lightweight wheelchair - detachable arms (desk or full length) , swing away detachable footrest E1260 E1260 X X NA X
Non-Standard Wheelchairs E1270 E1270
Non-Standard Wheelchairs E1280 E1280 X X NA X
Heavy duty wheelchair - fixed full length arms, swing away detachable foot rests E1285 E1285 X X NA X
Heavy duty wheelchair - detachable arms (desk or full length) , swing away detachable foot rests, fixed full
legs, elevating leg rest E1290 E1290 X X NA X
Non-Standard Wheelchairs E1295 E1298 X X NA X
Whirlpool Equipment E1300 E1310 X X NA X
Oxygen concentrator E1390 E1390 X X NA X
Durable Medical Equipment, miscellaneous E1399 E1399 X X NA X
Oxygen and water vapor enriching system with heated delivery E1405 E1405 X X NA X
Oxygen and water vapor enriching system without heated delivery E1406 E1406 X X NA X
Jaw Motion Rehabilitation System E1700 E1702 X X NA X
Dynamic adjustable elbow extension/flexion device, includes soft interface material E1800 E1800 X X NA X
Static progressive stretch elbow device, extension and/or flexion, with or without range of motion
adjustment, includes all components and accessories E1801 E1801 X X NA X
Dynamic adjustable forearm pronation/supination device, includes soft interface material E1802 E1802 X X NA X
Dynamic adjustable wrist, extension/flexion device, includes all components and accessories E1805 E1805 X X NA X
Static progressive stretch wrist device, extension and/or flexion, with or without range of motion
adjustment, includes all components and accessories E1806 E1806 X X NA X
Dynamic adjustable knee, extension/flexion device, includes soft interface material E1810 E1810 X X NA X
Static progressive stretch knee device, extension and/or flexion, with or without range of motion
adjustment, includes all components and accessories E1811 E1811 X X NA X
Dynamic knee, extension/flexion device, with active resistance control E1812 E1812 X X NA X
Dynamic adjustable ankle, extension/flexion device, includes soft interface material E1815 E1815 X X NA X
Static progressive stretch ankle device, extension and/or flexion, with or without range of motion
adjustment, includes all components and accessories E1816 E1816 X X NA X
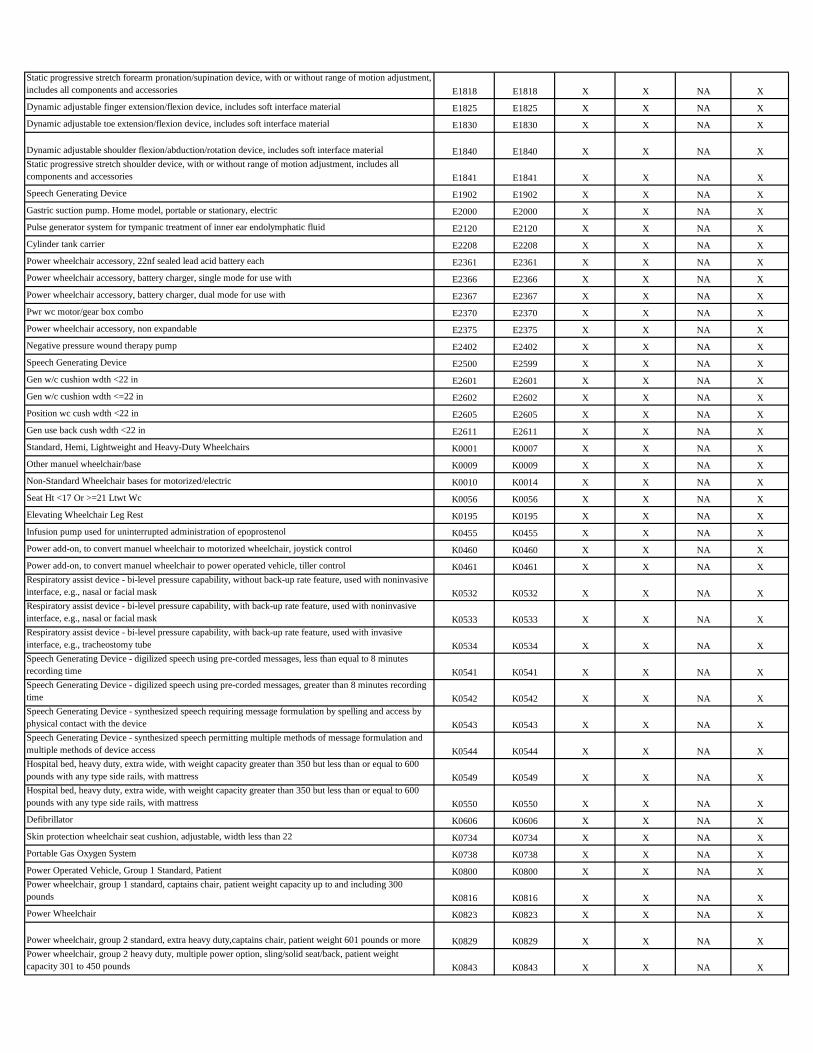
Static progressive stretch forearm pronation/supination device, with or without range of motion adjustment,
includes all components and accessories E1818 E1818 X X NA X
Dynamic adjustable finger extension/flexion device, includes soft interface material E1825 E1825 X X NA X
Dynamic adjustable toe extension/flexion device, includes soft interface material E1830 E1830 X X NA X
Dynamic adjustable shoulder flexion/abduction/rotation device, includes soft interface material E1840 E1840 X X NA X
Static progressive stretch shoulder device, with or without range of motion adjustment, includes all
components and accessories E1841 E1841 X X NA X
Speech Generating Device E1902 E1902 X X NA X
Gastric suction pump. Home model, portable or stationary, electric E2000 E2000 X X NA X
Pulse generator system for tympanic treatment of inner ear endolymphatic fluid E2120 E2120 X X NA X
Cylinder tank carrier E2208 E2208 X X NA X
Power wheelchair accessory, 22nf sealed lead acid battery each E2361 E2361 X X NA X
Power wheelchair accessory, battery charger, single mode for use with E2366 E2366 X X NA X
Power wheelchair accessory, battery charger, dual mode for use with E2367 E2367 X X NA X
Pwr wc motor/gear box combo E2370 E2370 X X NA X
Power wheelchair accessory, non expandable E2375 E2375 X X NA X
Negative pressure wound therapy pump E2402 E2402 X X NA X
Speech Generating Device E2500 E2599 X X NA X
Gen w/c cushion wdth <22 in E2601 E2601 X X NA X
Gen w/c cushion wdth <=22 in E2602 E2602 X X NA X
Position wc cush wdth <22 in E2605 E2605 X X NA X
Gen use back cush wdth <22 in E2611 E2611 X X NA X
Standard, Hemi, Lightweight and Heavy-Duty Wheelchairs K0001 K0007 X X NA X
Other manuel wheelchair/base K0009 K0009 X X NA X
Non-Standard Wheelchair bases for motorized/electric K0010 K0014 X X NA X
Seat Ht <17 Or >=21 Ltwt Wc K0056 K0056 X X NA X
Elevating Wheelchair Leg Rest K0195 K0195 X X NA X
Infusion pump used for uninterrupted administration of epoprostenol K0455 K0455 X X NA X
Power add-on, to convert manuel wheelchair to motorized wheelchair, joystick control K0460 K0460 X X NA X
Power add-on, to convert manuel wheelchair to power operated vehicle, tiller control K0461 K0461 X X NA X
Respiratory assist device - bi-level pressure capability, without back-up rate feature, used with noninvasive
interface, e.g., nasal or facial mask K0532 K0532 X X NA X
Respiratory assist device - bi-level pressure capability, with back-up rate feature, used with noninvasive
interface, e.g., nasal or facial mask K0533 K0533 X X NA X
Respiratory assist device - bi-level pressure capability, with back-up rate feature, used with invasive
interface, e.g., tracheostomy tube K0534 K0534 X X NA X
Speech Generating Device - digilized speech using pre-corded messages, less than equal to 8 minutes
recording time K0541 K0541 X X NA X
Speech Generating Device - digilized speech using pre-corded messages, greater than 8 minutes recording
time K0542 K0542 X X NA X
Speech Generating Device - synthesized speech requiring message formulation by spelling and access by
physical contact with the device K0543 K0543 X X NA X
Speech Generating Device - synthesized speech permitting multiple methods of message formulation and
multiple methods of device access K0544 K0544 X X NA X
Hospital bed, heavy duty, extra wide, with weight capacity greater than 350 but less than or equal to 600
pounds with any type side rails, with mattress K0549 K0549 X X NA X
Hospital bed, heavy duty, extra wide, with weight capacity greater than 350 but less than or equal to 600
pounds with any type side rails, with mattress K0550 K0550 X X NA X
Defibrillator K0606 K0606 X X NA X
Skin protection wheelchair seat cushion, adjustable, width less than 22 K0734 K0734 X X NA X
Portable Gas Oxygen System K0738 K0738 X X NA X
Power Operated Vehicle, Group 1 Standard, Patient K0800 K0800 X X NA X
Power wheelchair, group 1 standard, captains chair, patient weight capacity up to and including 300
pounds K0816 K0816 X X NA X
Power Wheelchair K0823 K0823 X X NA X
Power wheelchair, group 2 standard, extra heavy duty,captains chair, patient weight 601 pounds or more K0829 K0829 X X NA X
Power wheelchair, group 2 heavy duty, multiple power option, sling/solid seat/back, patient weight
capacity 301 to 450 pounds K0843 K0843 X X NA X
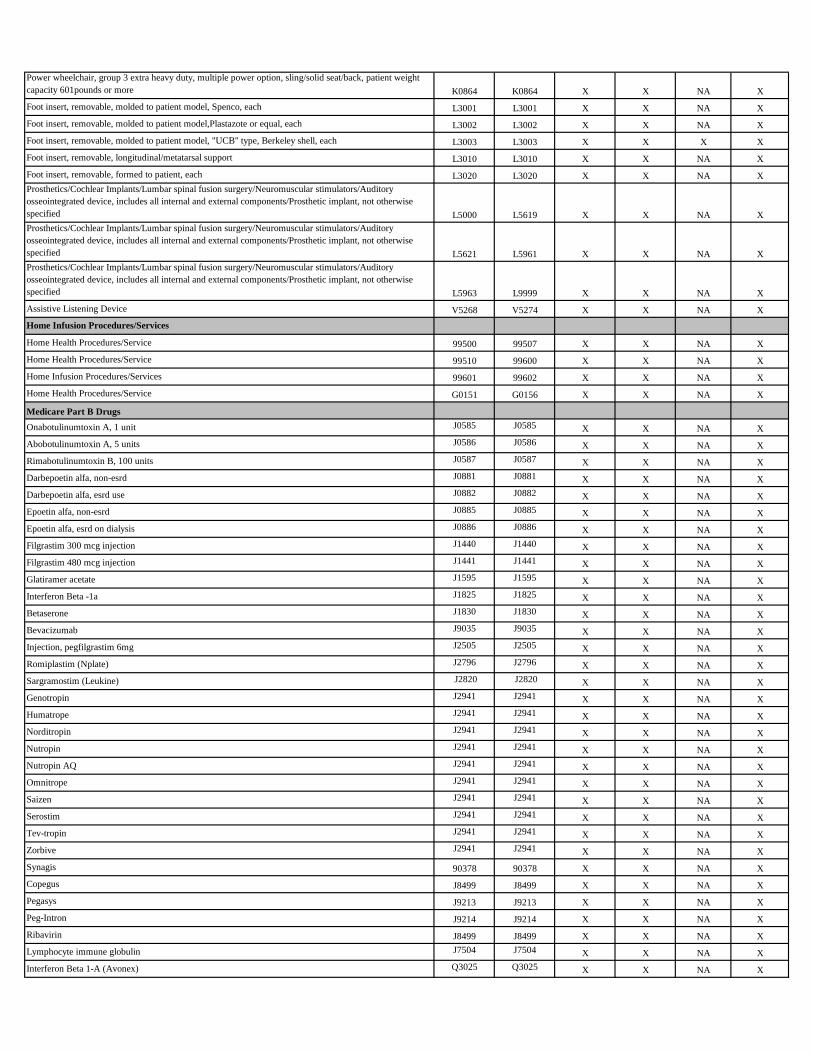
Power wheelchair, group 3 extra heavy duty, multiple power option, sling/solid seat/back, patient weight
capacity 601pounds or more K0864 K0864 X X NA X
Foot insert, removable, molded to patient model, Spenco, each L3001 L3001 X X NA X
Foot insert, removable, molded to patient model,Plastazote or equal, each L3002 L3002 X X NA X
Foot insert, removable, molded to patient model, "UCB" type, Berkeley shell, each L3003 L3003 X X X X
Foot insert, removable, longitudinal/metatarsal support L3010 L3010 X X NA X
Foot insert, removable, formed to patient, each L3020 L3020 X X NA X
Prosthetics/Cochlear Implants/Lumbar spinal fusion surgery/Neuromuscular stimulators/Auditory
osseointegrated device, includes all internal and external components/Prosthetic implant, not otherwise
specified L5000 L5619 X X NA X
Prosthetics/Cochlear Implants/Lumbar spinal fusion surgery/Neuromuscular stimulators/Auditory
osseointegrated device, includes all internal and external components/Prosthetic implant, not otherwise
specified L5621 L5961 X X NA X
Prosthetics/Cochlear Implants/Lumbar spinal fusion surgery/Neuromuscular stimulators/Auditory
osseointegrated device, includes all internal and external components/Prosthetic implant, not otherwise
specified L5963 L9999 X X NA X
Assistive Listening Device V5268 V5274 X X NA X
Home Infusion Procedures/Services
Home Health Procedures/Service 99500 99507 X X NA X
Home Health Procedures/Service 99510 99600 X X NA X
Home Infusion Procedures/Services 99601 99602 X X NA X
Home Health Procedures/Service G0151 G0156 X X NA X
Medicare Part B Drugs
Onabotulinumtoxin A, 1 unit J0585 J0585 X X NA X
Abobotulinumtoxin A, 5 units J0586 J0586 X X NA X
Rimabotulinumtoxin B, 100 units J0587 J0587 X X NA X
Darbepoetin alfa, non-esrd J0881 J0881 X X NA X
Darbepoetin alfa, esrd use J0882 J0882 X X NA X
Epoetin alfa, non-esrd J0885 J0885 X X NA X
Epoetin alfa, esrd on dialysis J0886 J0886 X X NA X
Filgrastim 300 mcg injection J1440 J1440 X X NA X
Filgrastim 480 mcg injection J1441 J1441 X X NA X
Glatiramer acetate J1595 J1595 X X NA X
Interferon Beta -1a J1825 J1825 X X NA X
Betaserone J1830 J1830 X X NA X
Bevacizumab J9035 J9035 X X NA X
Injection, pegfilgrastim 6mg J2505 J2505 X X NA X
Romiplastim (Nplate) J2796 J2796 X X NA X
Sargramostim (Leukine) J2820 J2820 X X NA X
Genotropin J2941 J2941 X X NA X
Humatrope J2941 J2941 X X NA X
Norditropin J2941 J2941 X X NA X
Nutropin J2941 J2941 X X NA X
Nutropin AQ J2941 J2941 X X NA X
Omnitrope J2941 J2941 X X NA X
Saizen J2941 J2941 X X NA X
Serostim J2941 J2941 X X NA X
Tev-tropin J2941 J2941 X X NA X
Zorbive J2941 J2941 X X NA X
Synagis 90378 90378 X X NA X
Copegus J8499 J8499 X X NA X
Pegasys J9213 J9213 X X NA X
Peg-Intron J9214 J9214 X X NA X
Ribavirin J8499 J8499 X X NA X
Lymphocyte immune globulin J7504 J7504 X X NA X
Interferon Beta 1-A (Avonex) Q3025 Q3025 X X NA X
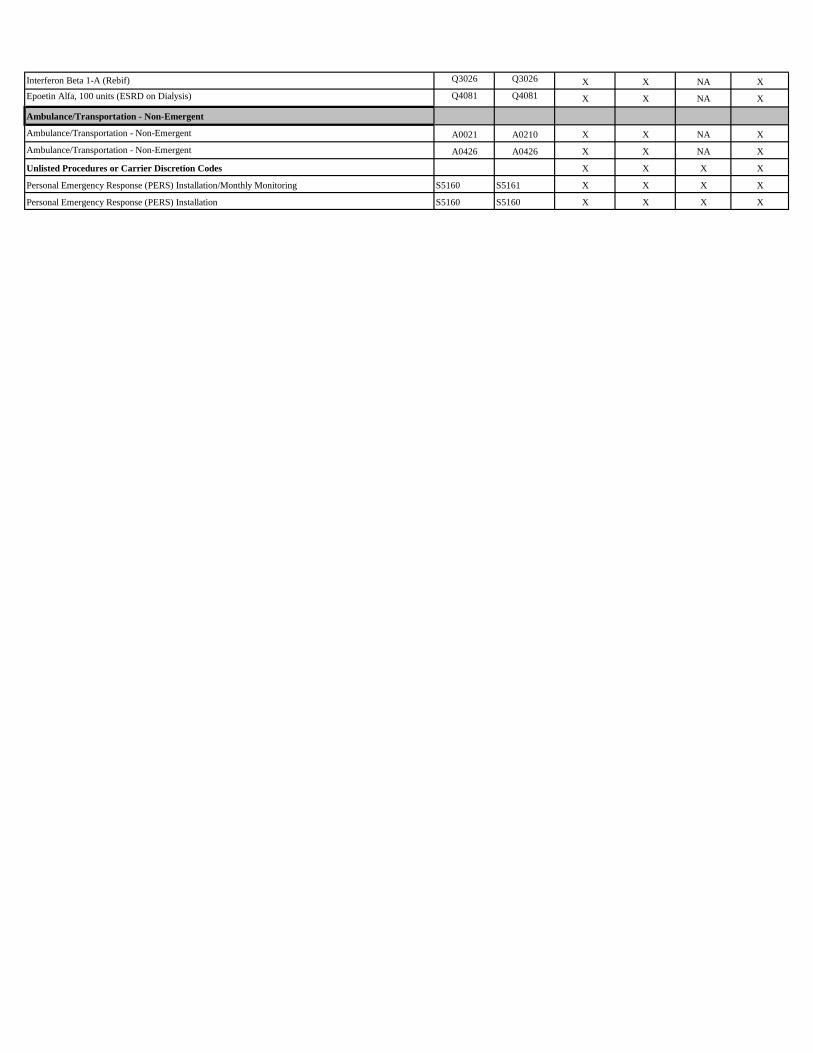
Interferon Beta 1-A (Rebif) Q3026 Q3026 X X NA X
Epoetin Alfa, 100 units (ESRD on Dialysis) Q4081 Q4081 X X NA X
Ambulance/Transportation - Non-Emergent
Ambulance/Transportation - Non-Emergent A0021 A0210 X X NA X
Ambulance/Transportation - Non-Emergent A0426 A0426 X X NA X
Unlisted Procedures or Carrier Discretion Codes X X X X
Personal Emergency Response (PERS) Installation/Monthly Monitoring S5160 S5161 X X X X
Personal Emergency Response (PERS) Installation S5160 S5160 X X X X

2017 FIDA Complete Authorization Requirements
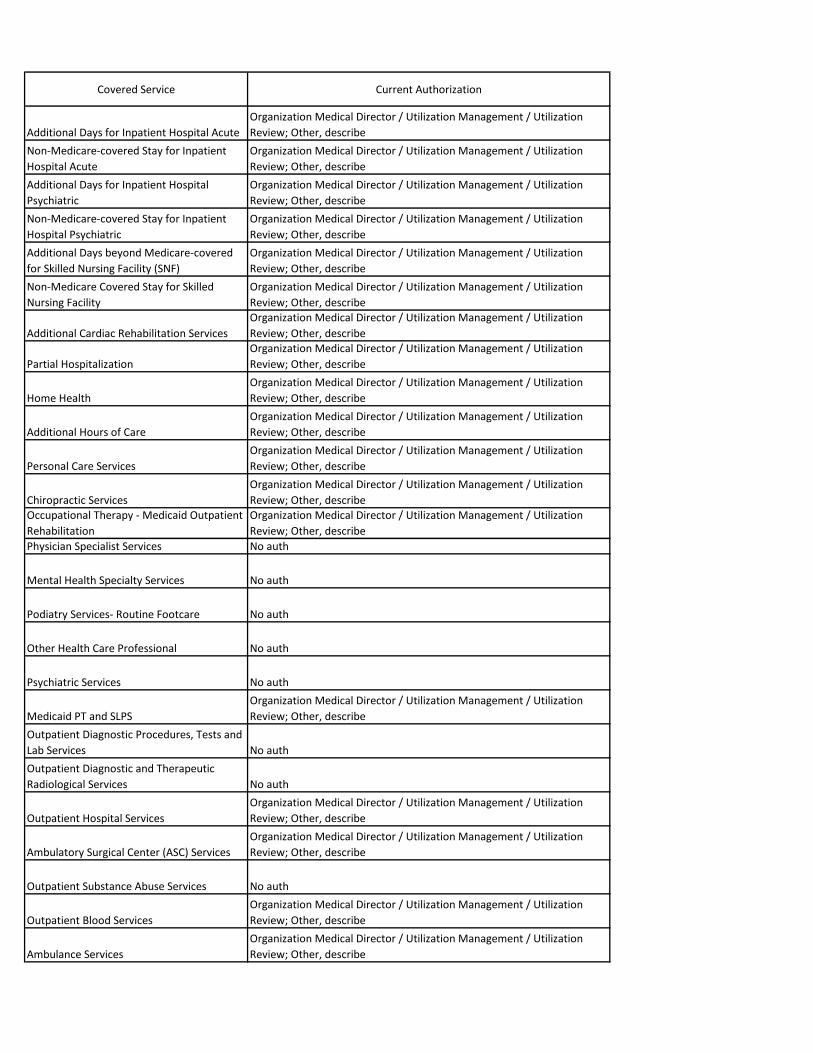
Covered Service Current Authorization
Additional Days for Inpatient Hospital Acute
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Non-Medicare-covered Stay for Inpatient
Hospital Acute
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Additional Days for Inpatient Hospital
Psychiatric
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Non-Medicare-covered Stay for Inpatient
Hospital Psychiatric
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Additional Days beyond Medicare-covered
for Skilled Nursing Facility (SNF)
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Non-Medicare Covered Stay for Skilled
Nursing Facility
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Additional Cardiac Rehabilitation Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Partial Hospitalization
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Home Health
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Additional Hours of Care
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Personal Care Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Chiropractic Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Occupational Therapy - Medicaid Outpatient
Rehabilitation
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Physician Specialist Services No auth
Mental Health Specialty Services No auth
Podiatry Services- Routine Footcare No auth
Other Health Care Professional No auth
Psychiatric Services No auth
Medicaid PT and SLPS
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Outpatient Diagnostic Procedures, Tests and
Lab Services No auth
Outpatient Diagnostic and Therapeutic
Radiological Services No auth
Outpatient Hospital Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Ambulatory Surgical Center (ASC) Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Outpatient Substance Abuse Services No auth
Outpatient Blood Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Ambulance Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe

Transportation Services - any location
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Durable Medical Equipment for use outside
the home
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
DME Other 1 - E-mods, Adaptive Devices
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
DME Other 2 - Assistive Technology
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Prosthetics/Orthotics/Medical - Medicaid
Prosthethics/Medical Supplies
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
End-Stage Renal Disease
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Meal Benefit
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Supplemental Benefits in addition to
Required Covered Benefits
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Supportive Items and Services the IDT finds
necessary
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Palliative Care No auth
Tobacco Cessation Counseling for Pregnant
Women No auth
Respiratory Care Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Family Planning Services No auth
Nursing Home Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Home and Community Based Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Personal Care Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Self-Directed personal Assistance Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Private Duty Nursing Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Case Management (Long Term Care)
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Case Management
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Adult Day Health Care, AIDS Adult Day
Health Care
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Nutrition and Wellness Counseling
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Assertive Community Treatment, Assisted
Living Program
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Outpatient Hospitalization, Outpatient
Surgery
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Community Integ. Counseling and
Community Trans. Svcs.
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Continuing Day Treatment, OMH Licensed
CRs
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
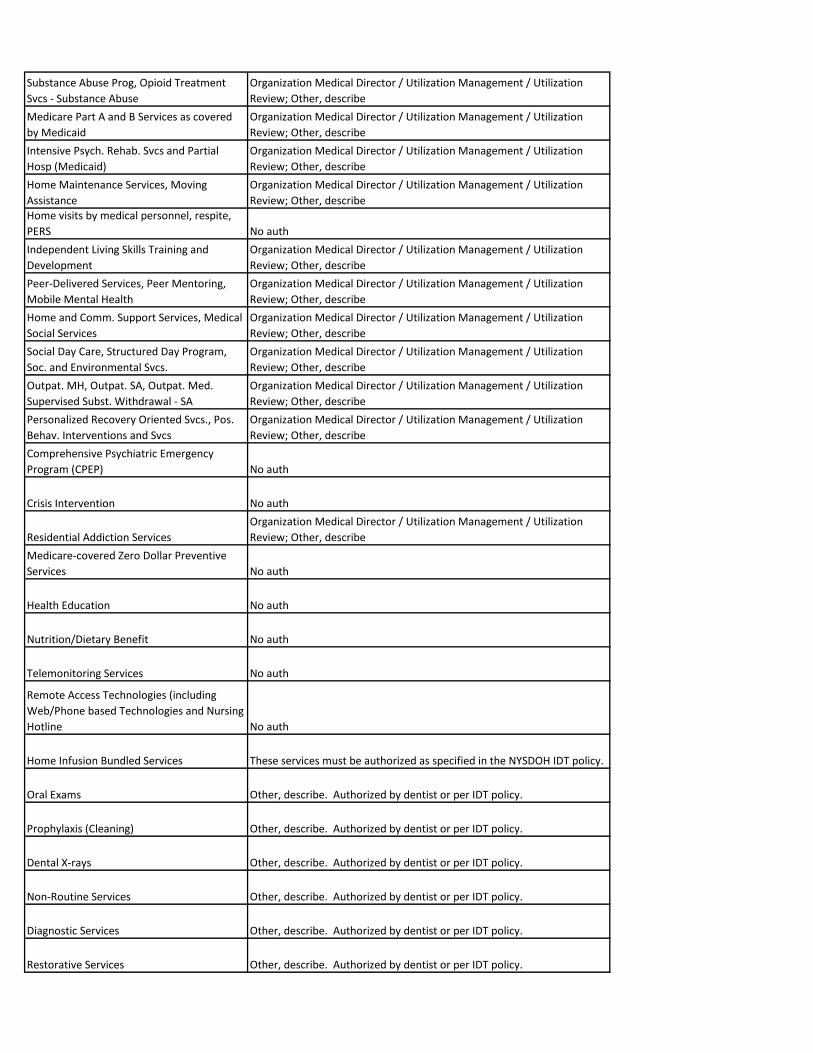
Substance Abuse Prog, Opioid Treatment
Svcs - Substance Abuse
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Medicare Part A and B Services as covered
by Medicaid
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Intensive Psych. Rehab. Svcs and Partial
Hosp (Medicaid)
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Home Maintenance Services, Moving
Assistance
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Home visits by medical personnel, respite,
PERS No auth
Independent Living Skills Training and
Development
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Peer-Delivered Services, Peer Mentoring,
Mobile Mental Health
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Home and Comm. Support Services, Medical
Social Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Social Day Care, Structured Day Program,
Soc. and Environmental Svcs.
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Outpat. MH, Outpat. SA, Outpat. Med.
Supervised Subst. Withdrawal - SA
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Personalized Recovery Oriented Svcs., Pos.
Behav. Interventions and Svcs
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Comprehensive Psychiatric Emergency
Program (CPEP) No auth
Crisis Intervention No auth
Residential Addiction Services
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe
Medicare-covered Zero Dollar Preventive
Services No auth
Health Education No auth
Nutrition/Dietary Benefit No auth
Telemonitoring Services No auth
Remote Access Technologies (including
Web/Phone based Technologies and Nursing
Hotline No auth
Home Infusion Bundled Services These services must be authorized as specified in the NYSDOH IDT policy.
Oral Exams Other, describe. Authorized by dentist or per IDT policy.
Prophylaxis (Cleaning) Other, describe. Authorized by dentist or per IDT policy.
Dental X-rays Other, describe. Authorized by dentist or per IDT policy.
Non-Routine Services Other, describe. Authorized by dentist or per IDT policy.
Diagnostic Services Other, describe. Authorized by dentist or per IDT policy.
Restorative Services Other, describe. Authorized by dentist or per IDT policy.
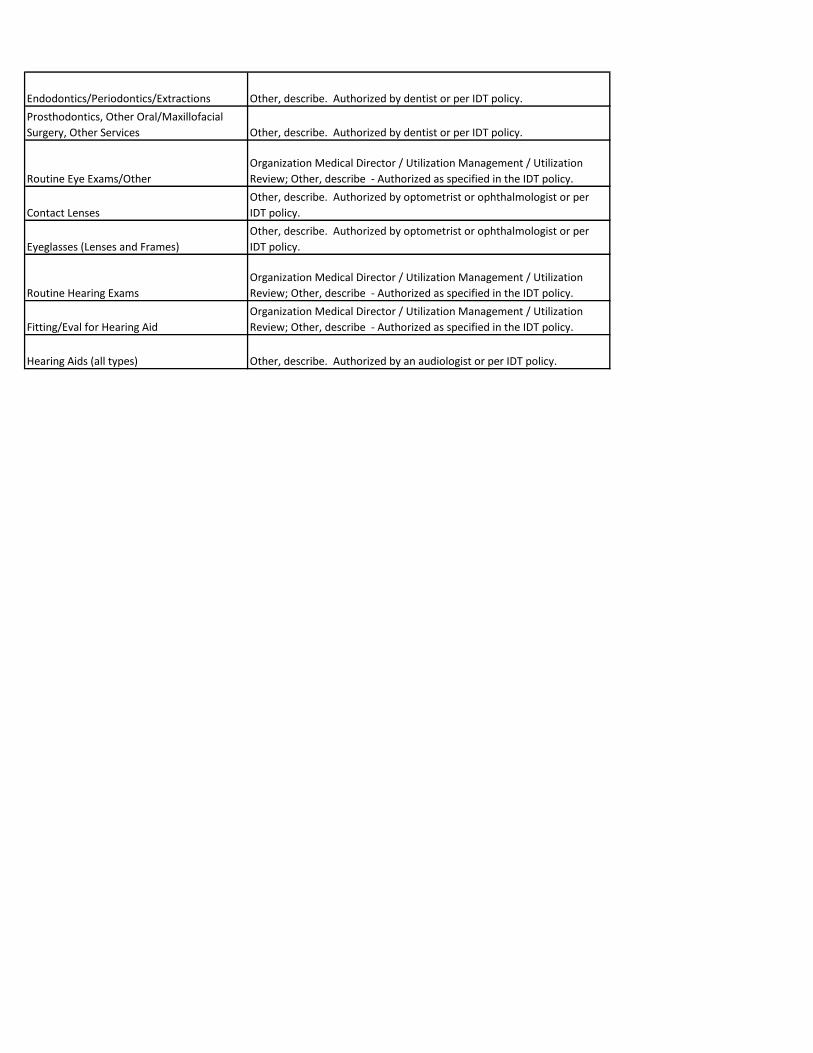
Endodontics/Periodontics/Extractions Other, describe. Authorized by dentist or per IDT policy.
Prosthodontics, Other Oral/Maxillofacial
Surgery, Other Services Other, describe. Authorized by dentist or per IDT policy.
Routine Eye Exams/Other
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe - Authorized as specified in the IDT policy.
Contact Lenses
Other, describe. Authorized by optometrist or ophthalmologist or per
IDT policy.
Eyeglasses (Lenses and Frames)
Other, describe. Authorized by optometrist or ophthalmologist or per
IDT policy.
Routine Hearing Exams
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe - Authorized as specified in the IDT policy.
Fitting/Eval for Hearing Aid
Organization Medical Director / Utilization Management / Utilization
Review; Other, describe - Authorized as specified in the IDT policy.
Hearing Aids (all types) Other, describe. Authorized by an audiologist or per IDT policy.
A-6
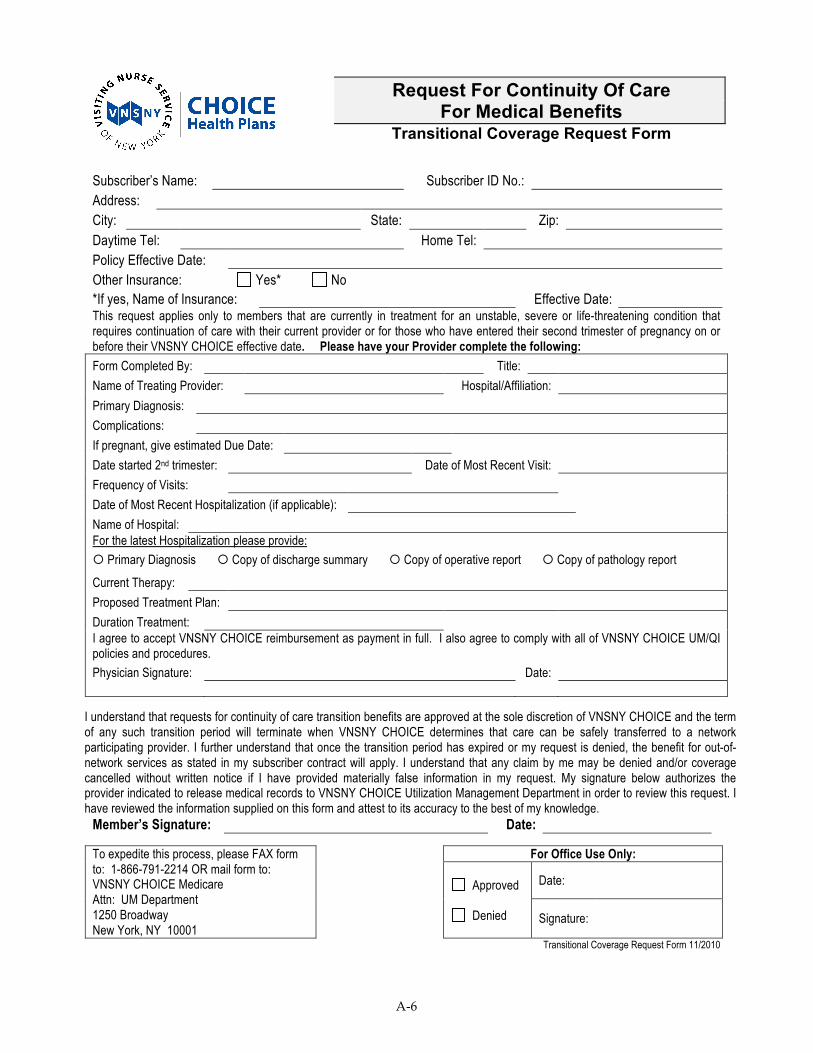
Subscriber’s Name: Subscriber ID No.: Address: City: State: Zip: Daytime Tel: Home Tel: Policy Effective Date: Other Insurance: Yes* No *If yes, Name of Insurance: Effective Date: This request applies only to members that are currently in treatment for an unstable, severe or life-threatening condition that requires continuation of care with their current provider or for those who have entered their second trimester of pregnancy on or before their VNSNY CHOICE effective date. Please have your Provider complete the following: Form Completed By: Title:
Name of Treating Provider: Hospital/Affiliation:
Primary Diagnosis:
Complications:
If pregnant, give estimated Due Date:
Date started 2nd trimester: Date of Most Recent Visit:
Frequency of Visits:
Date of Most Recent Hospitalization (if applicable):
Name of Hospital: For the latest Hospitalization please provide:
Primary Diagnosis Copy of discharge summary Copy of operative report Copy of pathology report
Current Therapy:
Proposed Treatment Plan:
Duration Treatment: I agree to accept VNSNY CHOICE reimbursement as payment in full. I also agree to comply with all of VNSNY CHOICE UM/QI policies and procedures.
Physician Signature: Date:
I understand that requests for continuity of care transition benefits are approved at the sole discretion of VNSNY CHOICE and the term of any such transition period will terminate when VNSNY CHOICE determines that care can be safely transferred to a network participating provider. I further understand that once the transition period has expired or my request is denied, the benefit for out-of-network services as stated in my subscriber contract will apply. I understand that any claim by me may be denied and/or coverage cancelled without written notice if I have provided materially false information in my request. My signature below authorizes the provider indicated to release medical records to VNSNY CHOICE Utilization Management Department in order to review this request. I have reviewed the information supplied on this form and attest to its accuracy to the best of my knowledge.
Member’s Signature: Date:
For Office Use Only:
Date:
To expedite this process, please FAX form to: 1-866-791-2214 OR mail form to: VNSNY CHOICE Medicare Attn: UM Department 1250 Broadway New York, NY 10001
Approved
Denied Signature:
Transitional Coverage Request Form 11/2010
Request For Continuity Of Care For Medical Benefits
Transitional Coverage Request Form
A-2
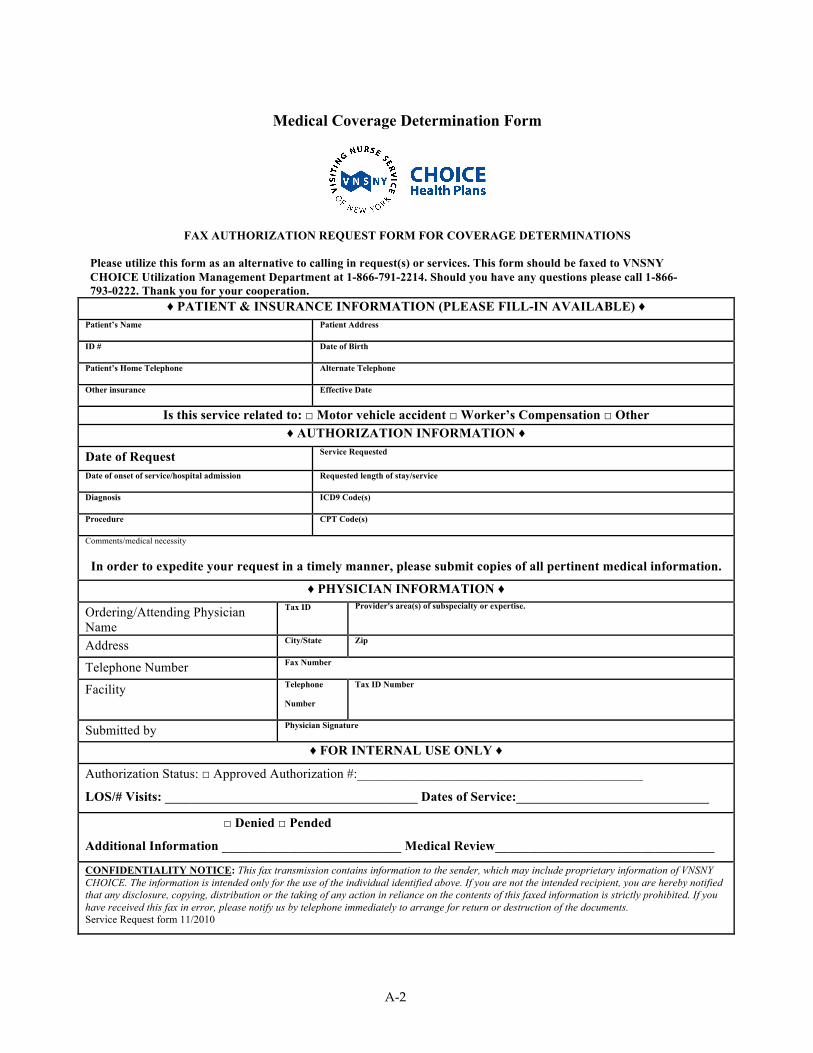
Medical Coverage Determination Form
FAX AUTHORIZATION REQUEST FORM FOR COVERAGE DETERMINATIONS
Please utilize this form as an alternative to calling in request(s) or services. This form should be faxed to VNSNY CHOICE Utilization Management Department at 1-866-791-2214. Should you have any questions please call 1-866-793-0222. Thank you for your cooperation.
♦ PATIENT & INSURANCE INFORMATION (PLEASE FILL-IN AVAILABLE) ♦ Patient’s Name
Patient Address
ID #
Date of Birth
Patient’s Home Telephone
Alternate Telephone
Other insurance
Effective Date
Is this service related to: □ Motor vehicle accident □ Worker’s Compensation □ Other
♦ AUTHORIZATION INFORMATION ♦
Date of Request Service Requested
Date of onset of service/hospital admission
Requested length of stay/service
Diagnosis
ICD9 Code(s)
Procedure
CPT Code(s)
Comments/medical necessity
In order to expedite your request in a timely manner, please submit copies of all pertinent medical information.
♦ PHYSICIAN INFORMATION ♦
Ordering/Attending Physician Name
Tax ID
Provider's area(s) of subspecialty or expertise.
Address City/State
Zip
Telephone Number Fax Number
Facility Telephone
Number
Tax ID Number
Submitted by Physician Signature
♦ FOR INTERNAL USE ONLY ♦
Authorization Status: □ Approved Authorization #:___________________________________________
LOS/# Visits: ______________________________________ Dates of Service:_____________________________
□ Denied □ Pended
Additional Information ___________________________ Medical Review_________________________________
CONFIDENTIALITY NOTICE: This fax transmission contains information to the sender, which may include proprietary information of VNSNY CHOICE. The information is intended only for the use of the individual identified above. If you are not the intended recipient, you are hereby notified that any disclosure, copying, distribution or the taking of any action in reliance on the contents of this faxed information is strictly prohibited. If you have received this fax in error, please notify us by telephone immediately to arrange for return or destruction of the documents. Service Request form 11/2010