Embed Size (px)
Citation preview
Important benefits information
2015 benefits enrollment booklet for new
hires and newly eligible team members
Action required Enroll before your enrollment period deadline
Welcome to Wells Fargo
Congratulations on your new position We value and
support our people as a competitive advantage We
strive to attract develop retain and motivate the most
talented people we can find These people become our
team members and are a treasured resource in whom
we invest
As part of that investment Wells Fargo is proud
to offer you a competitive benefits package with a
comprehensive selection of benefits
Our aim is to support you so you can learn about your
plans gain confidence when making benefits choices
plan for your future and reach your personal health
well-being and retirement goals
Using the booklet
Some benefits are provided at no additional cost to you
mdash and you are automatically enrolled when you become
eligible for benefits These benefits are noted in this
booklet by this symbol PAID FOR
You and Wells Fargo share the cost for most benefits
There are optional benefits in which you pay the
total cost if you elect them designated by this
symbol YOUR CHOICE
Use the Enrollment Worksheet on page 8 to keep track
of the coverage yoursquore interested in for you and your
eligible dependents
Keep in mind that this booklet is intended to provide
only an overview and does not contain all the
provisions of the Wells Fargo-sponsored benefits plans
It is very important that you refer to the Benefi ts Book
available on Teamworks which contains the provisions
of the Wells Fargo-sponsored benefit plans
3
Inside the booklet
Donrsquot miss your benefits enrollment period 4
How to enroll 5
Enrollment worksheet mdash optional 8
Medical coverage 10
Account-based medical plans overview 11
The HRA-Based Medical Plan 12
The HSA-based medical plans 14
Health and wellness dollars 17
Prescription drug coverage
under the account-based plans 18
Comparing the account-based medical plans 20
How does your account get funded 23
The Kaiser HMO and HDHP Kaiser medical plan 24
Health and well-being 28
Your medical plan resources 29
Flexible spending accounts 30
Dental and vision coverage 31
Financial protection Long-Term Care Plan 33
Financial protection Disability coverage 35
Financial protection Life insurance coverage 37
Financial protection Business Travel Accident
and Accidental Death and Dismemberment 39
Naming a beneficiary 40
Financial protection Legal Services Plan 41
Other benefits Commuter Benefit Program 42
Claims administrators contact info 43
Tools and resources 45
Important information and disclosures 46
4
Donrsquot miss your benefits enrollment period
If you want to elect certain benefits you must enroll
during your designated enrollment period
If you are hired rehired or become newly eligible from
You must enroll by Your benefits take effect on
January 2 to February 1 February 14 March 1
February 2 to March 1 March 14 April 1
March 2 to April 1 April 14 May 1
April 2 to May 1 May 14 June 1
May 2 to June 1 June 14 July 1
June 2 to July 1 July 14 August 1
July 2 to August 1 August 14 September 1
August 2 to September 1 September 14 October 1
September 2 to October 1 October 14 November 1
October 2 to November 1 November 14 December 1
November 2 to December 1 December 14 January 1
December 2 to January 1 January 14 February 1
Note Your designated enrollment period ends
at 1159 pm Central Time on the last day of the
enrollment period Please note that online enrollment
is unavailable on certain nights after 845 pm
Central Time
Why is electing your benefits during your enrollment period so important
Some benefits such as medical dental vision
Accidental Death and Dismemberment legal services
and flexible spending accounts may be elected only
during your designated enrollment period If you do
not enroll during your designated enrollment period
you must generally wait until the next Annual Benefits
Enrollment period to enroll yourself and your eligible
dependents unless you experience a Qualified Event
Other benefits such as life insurance optional long-
term disability and long-term care may be elected
without proof of good health only during this fi rst
designated enrollment period Changes to your life
insurance coverage optional long-term disability or
long-term care after your initial designated enrollment
period (or Qualified Event for life insurance) must be
approved under the applicable proof of good health or
evidence of insurability process
For additional details see the section titled Making
Changes after Your Designated Enrollment Period on
page 7 and the Benefits Book
5
How to enroll
Online
To enroll go to the Your Benefits tool on Teamworks or
Teamworks at Home (teamworkswellsfargocom) Sign
on to the Your Benefits tool using your Wells Fargo
username and password Click the help links if you
have ID or password questions For more detailed
help with the steps listed below click the Help Center
button in the Your Benefits tool at any time
Use the Enrollment Worksheet beginning on page 8 to
choose and keep track of your benefit elections
Enroll early for the best possible response time in the
online Your Benefits tool Delays or disruptions might
occur during evening hours when payroll functions are
running
Go to teamworkswellsfargo com
From work Click Pay amp Benefits then Benefits
Tools then Your Benefits
From home Click Your Benefits
1 On the Your Benefits tool home page click
Benefits Enrollment This link is active during your
enrollment and change periods only
2 Click Review Personal Information Check your
address and other information and update it if
necessary (You must do this only the first time you
view this site during a new enrollment period)
3 After reviewing your personal information you must
agree to the terms of the benefits enrollment before
you can proceed
4 When finished click Return to Benefits Enrollment
at the bottom of the page
Choose and save your plan elections
5 In the Enrollment Events table click Select The
Enrollment Summary page lists each benefit and
shows your current and new selections To make
changes to a benefits selection or to see all of that
benefit planrsquos choices and costs click Choose
6 On the enrollment page for each benefit click
one choice to elect a plan or waive coverage Add
dependent information if necessary (see If You Have
Eligible Dependents on page 6)
Note You can change elections at any time until your
designated enrollment period ends Any elections you
save will display when you return so you can verify or
make more changes
7 To save your election click Next review the
Confirmation page and click Save Yoursquoll return to
the Enrollment Summary page
Repeat steps 5 to 7 until you have selected all the plans
in which you want to enroll If you need to end your
session before completing all your benefits elections
complete step 7 and return later to finish enrolling
8 When yoursquove completed your benefits elections click
Finish The last page provides timing information for
the enrollment and change periods and a link to your
Benefi ts Confirmation Statement which you should
review for accuracy To exit the Your Benefits tool
click Sign Off at the top of the page
By phone
If you do not have online access from a computer or
have trouble signing on call the HR Service Center at
1-877-HRWELLS (1-877-479-3557) option 2 Monday
through Friday from 800 am to 500 pm in your time
zone The HR Service Center accepts relay service calls
TDDTTY users may call 1-800-988-0161
Confirm or correct your benefits elections
After you make your benefits elections you will receive
an email containing a link to access your Benefits
Confirmation Statement to review and print a copy for
your records This statement is also available from the
Your Benefits tool
Review your Benefits Confirmation Statement carefully
If you need to make changes to your benefits elections
follow the instructions on the statement If you make
corrections during your change period your benefits
administrators might not have a record of the changes
by the date on which your benefits become effective
your updated ID cards could be delayed as a result
Note If you receive your Benefits Confirmation
Statement by email (or similar electronic delivery)
you may request to have a paper copy sent to
you at no cost either by sending an email to
hrsddistributionfulfillmentwellsfargocom or by
calling the HR Service Center at 1-877-HRWELLS
(1-877-479-3557) option 2 The HR Service Center
accepts relay service calls TDDTTY users may call
1-800-988-0161
6
This paper copy will be the same version that you can
print from the Your Benefits tool If you donrsquot have
a valid Wells Fargo email address you will receive a
paper Benefi ts Confirmation Statement through the
US mail If you donrsquot have at-home or at-work access to
the Your Benefits tool call the HR Service Center with
your changes or corrections
If you have eligible dependents
You are eligible for benefits described in this booklet if
you are classified as either a regular team member who is
scheduled with standard hours of 30 or more hours per
week or a part-time team member who is scheduled with
standard hours of between 175 and 29 hours per week
In general your eligible dependents include
bull Your spouse or domestic partner
bull Your or your spouse or domestic partnerrsquos natural-
born or legally adopted child until his or her 26th
birthday
bull A child for whom you your spouse or your domestic
partner is the agency- or court-appointed legal
guardian or foster parent
See the Benefits Book on Teamworks and Teamworks
at Home (teamworkswellsfargocom) for complete
dependent eligibility requirements
Note Enrolling a dependent who does not meet
Wells Fargorsquos eligibility criteria is a violation of the
Code of Ethics and may result in disciplinary action
including termination of your employment with
Wells Fargo Wells Fargo reserves the right to conduct
audits and reviews of all dependent eligibility
To add eligible dependents
1 Click Add Dependent Details on the enrollment
page for any benefit that allows dependent
enrollment Note that you must enroll in the plan
yourself fi rst
2 On the DependentBeneficiary Personal Information
page enter the required information
3 Review the information carefully mdash you wonrsquot be
able to update it online later (except for a spouse or
domestic partnerrsquos smoker status) Click Save
4 The new dependent will be shown on the enrollment
page for any benefit that allows dependent
enrollment Repeat steps 1 to 3 to list more
dependents
5 Any dependents you listed will now appear with
checkboxes that allow you to add them to your
benefi ts coverage
6 Check the Enroll checkboxes next to the names of
the dependents you want to enroll
7 Click Next Follow the certification instructions
To certify newly enrolled eligible dependents
If you enroll an eligible dependent in coverage
yoursquore required to complete a brief certifi cation of
benefits eligibility Certification is triggered for these
dependents after you select the Enroll checkbox and
click Next on the benefits enrollment page
1 Read the overview page and click Continue
2 The certification page includes the eligible
dependentrsquos name and the benefits eligibility
requirements specific to the eligible dependentrsquos
relationship to you Read it and enter any required
information If your dependent qualifi es click I
Certify For any who donrsquot qualify click I Do Not
Certify You will not be able to enroll an uncertified
dependent
bullensp If you have several eligible dependents to certify
yoursquoll see a page for each one
bullensp When certifying an eligible dependent child of
a domestic partner you may need to certify the
domestic partner first even if you arenrsquot enrolling
the domestic partner in benefits coverage
3 When you finish certifying yoursquoll see the enrollment
confirmation page Review it and click Save
Yoursquoll return to the Enrollment Summary page After
you certify an eligible dependent in one plan you
may enroll him or her in any additional benefits plans
without repeating the certification steps
Certification is not the same as enrollment mdash you will
still need to select the enrollment checkboxes for your
eligible dependents on every plan in which you want
them enrolled
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
Welcome to Wells Fargo
Congratulations on your new position We value and
support our people as a competitive advantage We
strive to attract develop retain and motivate the most
talented people we can find These people become our
team members and are a treasured resource in whom
we invest
As part of that investment Wells Fargo is proud
to offer you a competitive benefits package with a
comprehensive selection of benefits
Our aim is to support you so you can learn about your
plans gain confidence when making benefits choices
plan for your future and reach your personal health
well-being and retirement goals
Using the booklet
Some benefits are provided at no additional cost to you
mdash and you are automatically enrolled when you become
eligible for benefits These benefits are noted in this
booklet by this symbol PAID FOR
You and Wells Fargo share the cost for most benefits
There are optional benefits in which you pay the
total cost if you elect them designated by this
symbol YOUR CHOICE
Use the Enrollment Worksheet on page 8 to keep track
of the coverage yoursquore interested in for you and your
eligible dependents
Keep in mind that this booklet is intended to provide
only an overview and does not contain all the
provisions of the Wells Fargo-sponsored benefits plans
It is very important that you refer to the Benefi ts Book
available on Teamworks which contains the provisions
of the Wells Fargo-sponsored benefit plans
3
Inside the booklet
Donrsquot miss your benefits enrollment period 4
How to enroll 5
Enrollment worksheet mdash optional 8
Medical coverage 10
Account-based medical plans overview 11
The HRA-Based Medical Plan 12
The HSA-based medical plans 14
Health and wellness dollars 17
Prescription drug coverage
under the account-based plans 18
Comparing the account-based medical plans 20
How does your account get funded 23
The Kaiser HMO and HDHP Kaiser medical plan 24
Health and well-being 28
Your medical plan resources 29
Flexible spending accounts 30
Dental and vision coverage 31
Financial protection Long-Term Care Plan 33
Financial protection Disability coverage 35
Financial protection Life insurance coverage 37
Financial protection Business Travel Accident
and Accidental Death and Dismemberment 39
Naming a beneficiary 40
Financial protection Legal Services Plan 41
Other benefits Commuter Benefit Program 42
Claims administrators contact info 43
Tools and resources 45
Important information and disclosures 46
4
Donrsquot miss your benefits enrollment period
If you want to elect certain benefits you must enroll
during your designated enrollment period
If you are hired rehired or become newly eligible from
You must enroll by Your benefits take effect on
January 2 to February 1 February 14 March 1
February 2 to March 1 March 14 April 1
March 2 to April 1 April 14 May 1
April 2 to May 1 May 14 June 1
May 2 to June 1 June 14 July 1
June 2 to July 1 July 14 August 1
July 2 to August 1 August 14 September 1
August 2 to September 1 September 14 October 1
September 2 to October 1 October 14 November 1
October 2 to November 1 November 14 December 1
November 2 to December 1 December 14 January 1
December 2 to January 1 January 14 February 1
Note Your designated enrollment period ends
at 1159 pm Central Time on the last day of the
enrollment period Please note that online enrollment
is unavailable on certain nights after 845 pm
Central Time
Why is electing your benefits during your enrollment period so important
Some benefits such as medical dental vision
Accidental Death and Dismemberment legal services
and flexible spending accounts may be elected only
during your designated enrollment period If you do
not enroll during your designated enrollment period
you must generally wait until the next Annual Benefits
Enrollment period to enroll yourself and your eligible
dependents unless you experience a Qualified Event
Other benefits such as life insurance optional long-
term disability and long-term care may be elected
without proof of good health only during this fi rst
designated enrollment period Changes to your life
insurance coverage optional long-term disability or
long-term care after your initial designated enrollment
period (or Qualified Event for life insurance) must be
approved under the applicable proof of good health or
evidence of insurability process
For additional details see the section titled Making
Changes after Your Designated Enrollment Period on
page 7 and the Benefits Book
5
How to enroll
Online
To enroll go to the Your Benefits tool on Teamworks or
Teamworks at Home (teamworkswellsfargocom) Sign
on to the Your Benefits tool using your Wells Fargo
username and password Click the help links if you
have ID or password questions For more detailed
help with the steps listed below click the Help Center
button in the Your Benefits tool at any time
Use the Enrollment Worksheet beginning on page 8 to
choose and keep track of your benefit elections
Enroll early for the best possible response time in the
online Your Benefits tool Delays or disruptions might
occur during evening hours when payroll functions are
running
Go to teamworkswellsfargo com
From work Click Pay amp Benefits then Benefits
Tools then Your Benefits
From home Click Your Benefits
1 On the Your Benefits tool home page click
Benefits Enrollment This link is active during your
enrollment and change periods only
2 Click Review Personal Information Check your
address and other information and update it if
necessary (You must do this only the first time you
view this site during a new enrollment period)
3 After reviewing your personal information you must
agree to the terms of the benefits enrollment before
you can proceed
4 When finished click Return to Benefits Enrollment
at the bottom of the page
Choose and save your plan elections
5 In the Enrollment Events table click Select The
Enrollment Summary page lists each benefit and
shows your current and new selections To make
changes to a benefits selection or to see all of that
benefit planrsquos choices and costs click Choose
6 On the enrollment page for each benefit click
one choice to elect a plan or waive coverage Add
dependent information if necessary (see If You Have
Eligible Dependents on page 6)
Note You can change elections at any time until your
designated enrollment period ends Any elections you
save will display when you return so you can verify or
make more changes
7 To save your election click Next review the
Confirmation page and click Save Yoursquoll return to
the Enrollment Summary page
Repeat steps 5 to 7 until you have selected all the plans
in which you want to enroll If you need to end your
session before completing all your benefits elections
complete step 7 and return later to finish enrolling
8 When yoursquove completed your benefits elections click
Finish The last page provides timing information for
the enrollment and change periods and a link to your
Benefi ts Confirmation Statement which you should
review for accuracy To exit the Your Benefits tool
click Sign Off at the top of the page
By phone
If you do not have online access from a computer or
have trouble signing on call the HR Service Center at
1-877-HRWELLS (1-877-479-3557) option 2 Monday
through Friday from 800 am to 500 pm in your time
zone The HR Service Center accepts relay service calls
TDDTTY users may call 1-800-988-0161
Confirm or correct your benefits elections
After you make your benefits elections you will receive
an email containing a link to access your Benefits
Confirmation Statement to review and print a copy for
your records This statement is also available from the
Your Benefits tool
Review your Benefits Confirmation Statement carefully
If you need to make changes to your benefits elections
follow the instructions on the statement If you make
corrections during your change period your benefits
administrators might not have a record of the changes
by the date on which your benefits become effective
your updated ID cards could be delayed as a result
Note If you receive your Benefits Confirmation
Statement by email (or similar electronic delivery)
you may request to have a paper copy sent to
you at no cost either by sending an email to
hrsddistributionfulfillmentwellsfargocom or by
calling the HR Service Center at 1-877-HRWELLS
(1-877-479-3557) option 2 The HR Service Center
accepts relay service calls TDDTTY users may call
1-800-988-0161
6
This paper copy will be the same version that you can
print from the Your Benefits tool If you donrsquot have
a valid Wells Fargo email address you will receive a
paper Benefi ts Confirmation Statement through the
US mail If you donrsquot have at-home or at-work access to
the Your Benefits tool call the HR Service Center with
your changes or corrections
If you have eligible dependents
You are eligible for benefits described in this booklet if
you are classified as either a regular team member who is
scheduled with standard hours of 30 or more hours per
week or a part-time team member who is scheduled with
standard hours of between 175 and 29 hours per week
In general your eligible dependents include
bull Your spouse or domestic partner
bull Your or your spouse or domestic partnerrsquos natural-
born or legally adopted child until his or her 26th
birthday
bull A child for whom you your spouse or your domestic
partner is the agency- or court-appointed legal
guardian or foster parent
See the Benefits Book on Teamworks and Teamworks
at Home (teamworkswellsfargocom) for complete
dependent eligibility requirements
Note Enrolling a dependent who does not meet
Wells Fargorsquos eligibility criteria is a violation of the
Code of Ethics and may result in disciplinary action
including termination of your employment with
Wells Fargo Wells Fargo reserves the right to conduct
audits and reviews of all dependent eligibility
To add eligible dependents
1 Click Add Dependent Details on the enrollment
page for any benefit that allows dependent
enrollment Note that you must enroll in the plan
yourself fi rst
2 On the DependentBeneficiary Personal Information
page enter the required information
3 Review the information carefully mdash you wonrsquot be
able to update it online later (except for a spouse or
domestic partnerrsquos smoker status) Click Save
4 The new dependent will be shown on the enrollment
page for any benefit that allows dependent
enrollment Repeat steps 1 to 3 to list more
dependents
5 Any dependents you listed will now appear with
checkboxes that allow you to add them to your
benefi ts coverage
6 Check the Enroll checkboxes next to the names of
the dependents you want to enroll
7 Click Next Follow the certification instructions
To certify newly enrolled eligible dependents
If you enroll an eligible dependent in coverage
yoursquore required to complete a brief certifi cation of
benefits eligibility Certification is triggered for these
dependents after you select the Enroll checkbox and
click Next on the benefits enrollment page
1 Read the overview page and click Continue
2 The certification page includes the eligible
dependentrsquos name and the benefits eligibility
requirements specific to the eligible dependentrsquos
relationship to you Read it and enter any required
information If your dependent qualifi es click I
Certify For any who donrsquot qualify click I Do Not
Certify You will not be able to enroll an uncertified
dependent
bullensp If you have several eligible dependents to certify
yoursquoll see a page for each one
bullensp When certifying an eligible dependent child of
a domestic partner you may need to certify the
domestic partner first even if you arenrsquot enrolling
the domestic partner in benefits coverage
3 When you finish certifying yoursquoll see the enrollment
confirmation page Review it and click Save
Yoursquoll return to the Enrollment Summary page After
you certify an eligible dependent in one plan you
may enroll him or her in any additional benefits plans
without repeating the certification steps
Certification is not the same as enrollment mdash you will
still need to select the enrollment checkboxes for your
eligible dependents on every plan in which you want
them enrolled
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

3
Inside the booklet
Donrsquot miss your benefits enrollment period 4
How to enroll 5
Enrollment worksheet mdash optional 8
Medical coverage 10
Account-based medical plans overview 11
The HRA-Based Medical Plan 12
The HSA-based medical plans 14
Health and wellness dollars 17
Prescription drug coverage
under the account-based plans 18
Comparing the account-based medical plans 20
How does your account get funded 23
The Kaiser HMO and HDHP Kaiser medical plan 24
Health and well-being 28
Your medical plan resources 29
Flexible spending accounts 30
Dental and vision coverage 31
Financial protection Long-Term Care Plan 33
Financial protection Disability coverage 35
Financial protection Life insurance coverage 37
Financial protection Business Travel Accident
and Accidental Death and Dismemberment 39
Naming a beneficiary 40
Financial protection Legal Services Plan 41
Other benefits Commuter Benefit Program 42
Claims administrators contact info 43
Tools and resources 45
Important information and disclosures 46
4
Donrsquot miss your benefits enrollment period
If you want to elect certain benefits you must enroll
during your designated enrollment period
If you are hired rehired or become newly eligible from
You must enroll by Your benefits take effect on
January 2 to February 1 February 14 March 1
February 2 to March 1 March 14 April 1
March 2 to April 1 April 14 May 1
April 2 to May 1 May 14 June 1
May 2 to June 1 June 14 July 1
June 2 to July 1 July 14 August 1
July 2 to August 1 August 14 September 1
August 2 to September 1 September 14 October 1
September 2 to October 1 October 14 November 1
October 2 to November 1 November 14 December 1
November 2 to December 1 December 14 January 1
December 2 to January 1 January 14 February 1
Note Your designated enrollment period ends
at 1159 pm Central Time on the last day of the
enrollment period Please note that online enrollment
is unavailable on certain nights after 845 pm
Central Time
Why is electing your benefits during your enrollment period so important
Some benefits such as medical dental vision
Accidental Death and Dismemberment legal services
and flexible spending accounts may be elected only
during your designated enrollment period If you do
not enroll during your designated enrollment period
you must generally wait until the next Annual Benefits
Enrollment period to enroll yourself and your eligible
dependents unless you experience a Qualified Event
Other benefits such as life insurance optional long-
term disability and long-term care may be elected
without proof of good health only during this fi rst
designated enrollment period Changes to your life
insurance coverage optional long-term disability or
long-term care after your initial designated enrollment
period (or Qualified Event for life insurance) must be
approved under the applicable proof of good health or
evidence of insurability process
For additional details see the section titled Making
Changes after Your Designated Enrollment Period on
page 7 and the Benefits Book
5
How to enroll
Online
To enroll go to the Your Benefits tool on Teamworks or
Teamworks at Home (teamworkswellsfargocom) Sign
on to the Your Benefits tool using your Wells Fargo
username and password Click the help links if you
have ID or password questions For more detailed
help with the steps listed below click the Help Center
button in the Your Benefits tool at any time
Use the Enrollment Worksheet beginning on page 8 to
choose and keep track of your benefit elections
Enroll early for the best possible response time in the
online Your Benefits tool Delays or disruptions might
occur during evening hours when payroll functions are
running
Go to teamworkswellsfargo com
From work Click Pay amp Benefits then Benefits
Tools then Your Benefits
From home Click Your Benefits
1 On the Your Benefits tool home page click
Benefits Enrollment This link is active during your
enrollment and change periods only
2 Click Review Personal Information Check your
address and other information and update it if
necessary (You must do this only the first time you
view this site during a new enrollment period)
3 After reviewing your personal information you must
agree to the terms of the benefits enrollment before
you can proceed
4 When finished click Return to Benefits Enrollment
at the bottom of the page
Choose and save your plan elections
5 In the Enrollment Events table click Select The
Enrollment Summary page lists each benefit and
shows your current and new selections To make
changes to a benefits selection or to see all of that
benefit planrsquos choices and costs click Choose
6 On the enrollment page for each benefit click
one choice to elect a plan or waive coverage Add
dependent information if necessary (see If You Have
Eligible Dependents on page 6)
Note You can change elections at any time until your
designated enrollment period ends Any elections you
save will display when you return so you can verify or
make more changes
7 To save your election click Next review the
Confirmation page and click Save Yoursquoll return to
the Enrollment Summary page
Repeat steps 5 to 7 until you have selected all the plans
in which you want to enroll If you need to end your
session before completing all your benefits elections
complete step 7 and return later to finish enrolling
8 When yoursquove completed your benefits elections click
Finish The last page provides timing information for
the enrollment and change periods and a link to your
Benefi ts Confirmation Statement which you should
review for accuracy To exit the Your Benefits tool
click Sign Off at the top of the page
By phone
If you do not have online access from a computer or
have trouble signing on call the HR Service Center at
1-877-HRWELLS (1-877-479-3557) option 2 Monday
through Friday from 800 am to 500 pm in your time
zone The HR Service Center accepts relay service calls
TDDTTY users may call 1-800-988-0161
Confirm or correct your benefits elections
After you make your benefits elections you will receive
an email containing a link to access your Benefits
Confirmation Statement to review and print a copy for
your records This statement is also available from the
Your Benefits tool
Review your Benefits Confirmation Statement carefully
If you need to make changes to your benefits elections
follow the instructions on the statement If you make
corrections during your change period your benefits
administrators might not have a record of the changes
by the date on which your benefits become effective
your updated ID cards could be delayed as a result
Note If you receive your Benefits Confirmation
Statement by email (or similar electronic delivery)
you may request to have a paper copy sent to
you at no cost either by sending an email to
hrsddistributionfulfillmentwellsfargocom or by
calling the HR Service Center at 1-877-HRWELLS
(1-877-479-3557) option 2 The HR Service Center
accepts relay service calls TDDTTY users may call
1-800-988-0161
6
This paper copy will be the same version that you can
print from the Your Benefits tool If you donrsquot have
a valid Wells Fargo email address you will receive a
paper Benefi ts Confirmation Statement through the
US mail If you donrsquot have at-home or at-work access to
the Your Benefits tool call the HR Service Center with
your changes or corrections
If you have eligible dependents
You are eligible for benefits described in this booklet if
you are classified as either a regular team member who is
scheduled with standard hours of 30 or more hours per
week or a part-time team member who is scheduled with
standard hours of between 175 and 29 hours per week
In general your eligible dependents include
bull Your spouse or domestic partner
bull Your or your spouse or domestic partnerrsquos natural-
born or legally adopted child until his or her 26th
birthday
bull A child for whom you your spouse or your domestic
partner is the agency- or court-appointed legal
guardian or foster parent
See the Benefits Book on Teamworks and Teamworks
at Home (teamworkswellsfargocom) for complete
dependent eligibility requirements
Note Enrolling a dependent who does not meet
Wells Fargorsquos eligibility criteria is a violation of the
Code of Ethics and may result in disciplinary action
including termination of your employment with
Wells Fargo Wells Fargo reserves the right to conduct
audits and reviews of all dependent eligibility
To add eligible dependents
1 Click Add Dependent Details on the enrollment
page for any benefit that allows dependent
enrollment Note that you must enroll in the plan
yourself fi rst
2 On the DependentBeneficiary Personal Information
page enter the required information
3 Review the information carefully mdash you wonrsquot be
able to update it online later (except for a spouse or
domestic partnerrsquos smoker status) Click Save
4 The new dependent will be shown on the enrollment
page for any benefit that allows dependent
enrollment Repeat steps 1 to 3 to list more
dependents
5 Any dependents you listed will now appear with
checkboxes that allow you to add them to your
benefi ts coverage
6 Check the Enroll checkboxes next to the names of
the dependents you want to enroll
7 Click Next Follow the certification instructions
To certify newly enrolled eligible dependents
If you enroll an eligible dependent in coverage
yoursquore required to complete a brief certifi cation of
benefits eligibility Certification is triggered for these
dependents after you select the Enroll checkbox and
click Next on the benefits enrollment page
1 Read the overview page and click Continue
2 The certification page includes the eligible
dependentrsquos name and the benefits eligibility
requirements specific to the eligible dependentrsquos
relationship to you Read it and enter any required
information If your dependent qualifi es click I
Certify For any who donrsquot qualify click I Do Not
Certify You will not be able to enroll an uncertified
dependent
bullensp If you have several eligible dependents to certify
yoursquoll see a page for each one
bullensp When certifying an eligible dependent child of
a domestic partner you may need to certify the
domestic partner first even if you arenrsquot enrolling
the domestic partner in benefits coverage
3 When you finish certifying yoursquoll see the enrollment
confirmation page Review it and click Save
Yoursquoll return to the Enrollment Summary page After
you certify an eligible dependent in one plan you
may enroll him or her in any additional benefits plans
without repeating the certification steps
Certification is not the same as enrollment mdash you will
still need to select the enrollment checkboxes for your
eligible dependents on every plan in which you want
them enrolled
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
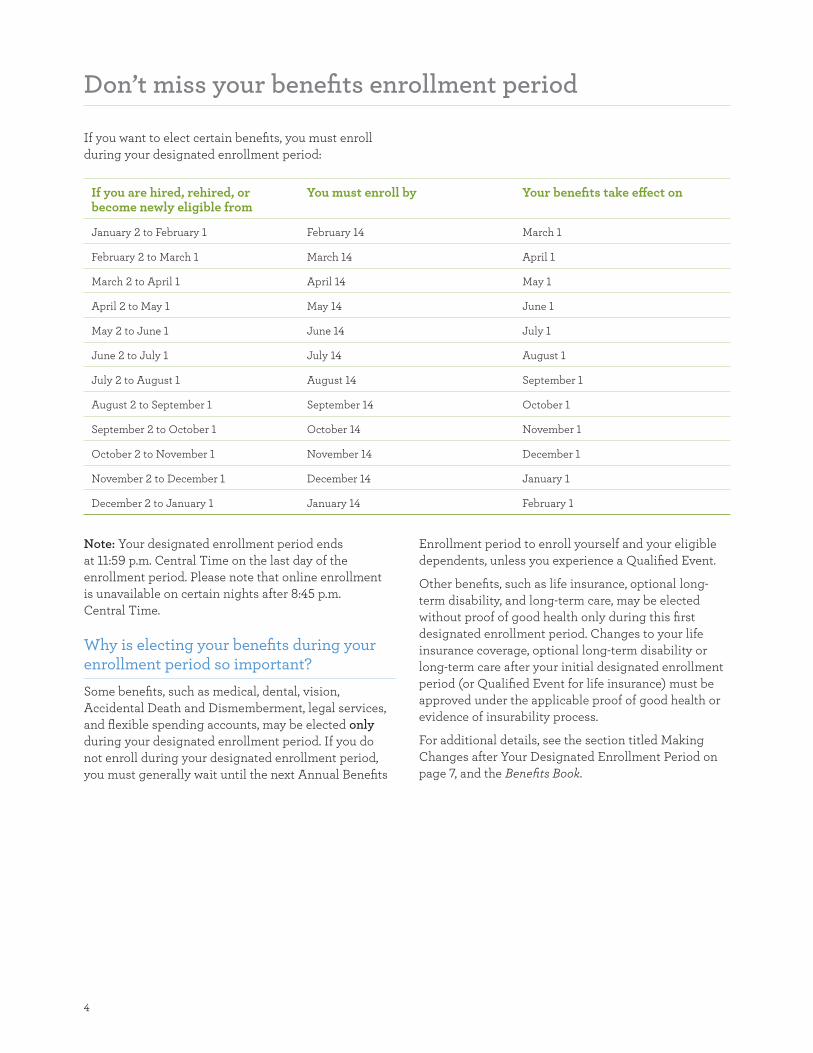
4
Donrsquot miss your benefits enrollment period
If you want to elect certain benefits you must enroll
during your designated enrollment period
If you are hired rehired or become newly eligible from
You must enroll by Your benefits take effect on
January 2 to February 1 February 14 March 1
February 2 to March 1 March 14 April 1
March 2 to April 1 April 14 May 1
April 2 to May 1 May 14 June 1
May 2 to June 1 June 14 July 1
June 2 to July 1 July 14 August 1
July 2 to August 1 August 14 September 1
August 2 to September 1 September 14 October 1
September 2 to October 1 October 14 November 1
October 2 to November 1 November 14 December 1
November 2 to December 1 December 14 January 1
December 2 to January 1 January 14 February 1
Note Your designated enrollment period ends
at 1159 pm Central Time on the last day of the
enrollment period Please note that online enrollment
is unavailable on certain nights after 845 pm
Central Time
Why is electing your benefits during your enrollment period so important
Some benefits such as medical dental vision
Accidental Death and Dismemberment legal services
and flexible spending accounts may be elected only
during your designated enrollment period If you do
not enroll during your designated enrollment period
you must generally wait until the next Annual Benefits
Enrollment period to enroll yourself and your eligible
dependents unless you experience a Qualified Event
Other benefits such as life insurance optional long-
term disability and long-term care may be elected
without proof of good health only during this fi rst
designated enrollment period Changes to your life
insurance coverage optional long-term disability or
long-term care after your initial designated enrollment
period (or Qualified Event for life insurance) must be
approved under the applicable proof of good health or
evidence of insurability process
For additional details see the section titled Making
Changes after Your Designated Enrollment Period on
page 7 and the Benefits Book
5
How to enroll
Online
To enroll go to the Your Benefits tool on Teamworks or
Teamworks at Home (teamworkswellsfargocom) Sign
on to the Your Benefits tool using your Wells Fargo
username and password Click the help links if you
have ID or password questions For more detailed
help with the steps listed below click the Help Center
button in the Your Benefits tool at any time
Use the Enrollment Worksheet beginning on page 8 to
choose and keep track of your benefit elections
Enroll early for the best possible response time in the
online Your Benefits tool Delays or disruptions might
occur during evening hours when payroll functions are
running
Go to teamworkswellsfargo com
From work Click Pay amp Benefits then Benefits
Tools then Your Benefits
From home Click Your Benefits
1 On the Your Benefits tool home page click
Benefits Enrollment This link is active during your
enrollment and change periods only
2 Click Review Personal Information Check your
address and other information and update it if
necessary (You must do this only the first time you
view this site during a new enrollment period)
3 After reviewing your personal information you must
agree to the terms of the benefits enrollment before
you can proceed
4 When finished click Return to Benefits Enrollment
at the bottom of the page
Choose and save your plan elections
5 In the Enrollment Events table click Select The
Enrollment Summary page lists each benefit and
shows your current and new selections To make
changes to a benefits selection or to see all of that
benefit planrsquos choices and costs click Choose
6 On the enrollment page for each benefit click
one choice to elect a plan or waive coverage Add
dependent information if necessary (see If You Have
Eligible Dependents on page 6)
Note You can change elections at any time until your
designated enrollment period ends Any elections you
save will display when you return so you can verify or
make more changes
7 To save your election click Next review the
Confirmation page and click Save Yoursquoll return to
the Enrollment Summary page
Repeat steps 5 to 7 until you have selected all the plans
in which you want to enroll If you need to end your
session before completing all your benefits elections
complete step 7 and return later to finish enrolling
8 When yoursquove completed your benefits elections click
Finish The last page provides timing information for
the enrollment and change periods and a link to your
Benefi ts Confirmation Statement which you should
review for accuracy To exit the Your Benefits tool
click Sign Off at the top of the page
By phone
If you do not have online access from a computer or
have trouble signing on call the HR Service Center at
1-877-HRWELLS (1-877-479-3557) option 2 Monday
through Friday from 800 am to 500 pm in your time
zone The HR Service Center accepts relay service calls
TDDTTY users may call 1-800-988-0161
Confirm or correct your benefits elections
After you make your benefits elections you will receive
an email containing a link to access your Benefits
Confirmation Statement to review and print a copy for
your records This statement is also available from the
Your Benefits tool
Review your Benefits Confirmation Statement carefully
If you need to make changes to your benefits elections
follow the instructions on the statement If you make
corrections during your change period your benefits
administrators might not have a record of the changes
by the date on which your benefits become effective
your updated ID cards could be delayed as a result
Note If you receive your Benefits Confirmation
Statement by email (or similar electronic delivery)
you may request to have a paper copy sent to
you at no cost either by sending an email to
hrsddistributionfulfillmentwellsfargocom or by
calling the HR Service Center at 1-877-HRWELLS
(1-877-479-3557) option 2 The HR Service Center
accepts relay service calls TDDTTY users may call
1-800-988-0161
6
This paper copy will be the same version that you can
print from the Your Benefits tool If you donrsquot have
a valid Wells Fargo email address you will receive a
paper Benefi ts Confirmation Statement through the
US mail If you donrsquot have at-home or at-work access to
the Your Benefits tool call the HR Service Center with
your changes or corrections
If you have eligible dependents
You are eligible for benefits described in this booklet if
you are classified as either a regular team member who is
scheduled with standard hours of 30 or more hours per
week or a part-time team member who is scheduled with
standard hours of between 175 and 29 hours per week
In general your eligible dependents include
bull Your spouse or domestic partner
bull Your or your spouse or domestic partnerrsquos natural-
born or legally adopted child until his or her 26th
birthday
bull A child for whom you your spouse or your domestic
partner is the agency- or court-appointed legal
guardian or foster parent
See the Benefits Book on Teamworks and Teamworks
at Home (teamworkswellsfargocom) for complete
dependent eligibility requirements
Note Enrolling a dependent who does not meet
Wells Fargorsquos eligibility criteria is a violation of the
Code of Ethics and may result in disciplinary action
including termination of your employment with
Wells Fargo Wells Fargo reserves the right to conduct
audits and reviews of all dependent eligibility
To add eligible dependents
1 Click Add Dependent Details on the enrollment
page for any benefit that allows dependent
enrollment Note that you must enroll in the plan
yourself fi rst
2 On the DependentBeneficiary Personal Information
page enter the required information
3 Review the information carefully mdash you wonrsquot be
able to update it online later (except for a spouse or
domestic partnerrsquos smoker status) Click Save
4 The new dependent will be shown on the enrollment
page for any benefit that allows dependent
enrollment Repeat steps 1 to 3 to list more
dependents
5 Any dependents you listed will now appear with
checkboxes that allow you to add them to your
benefi ts coverage
6 Check the Enroll checkboxes next to the names of
the dependents you want to enroll
7 Click Next Follow the certification instructions
To certify newly enrolled eligible dependents
If you enroll an eligible dependent in coverage
yoursquore required to complete a brief certifi cation of
benefits eligibility Certification is triggered for these
dependents after you select the Enroll checkbox and
click Next on the benefits enrollment page
1 Read the overview page and click Continue
2 The certification page includes the eligible
dependentrsquos name and the benefits eligibility
requirements specific to the eligible dependentrsquos
relationship to you Read it and enter any required
information If your dependent qualifi es click I
Certify For any who donrsquot qualify click I Do Not
Certify You will not be able to enroll an uncertified
dependent
bullensp If you have several eligible dependents to certify
yoursquoll see a page for each one
bullensp When certifying an eligible dependent child of
a domestic partner you may need to certify the
domestic partner first even if you arenrsquot enrolling
the domestic partner in benefits coverage
3 When you finish certifying yoursquoll see the enrollment
confirmation page Review it and click Save
Yoursquoll return to the Enrollment Summary page After
you certify an eligible dependent in one plan you
may enroll him or her in any additional benefits plans
without repeating the certification steps
Certification is not the same as enrollment mdash you will
still need to select the enrollment checkboxes for your
eligible dependents on every plan in which you want
them enrolled
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

5
How to enroll
Online
To enroll go to the Your Benefits tool on Teamworks or
Teamworks at Home (teamworkswellsfargocom) Sign
on to the Your Benefits tool using your Wells Fargo
username and password Click the help links if you
have ID or password questions For more detailed
help with the steps listed below click the Help Center
button in the Your Benefits tool at any time
Use the Enrollment Worksheet beginning on page 8 to
choose and keep track of your benefit elections
Enroll early for the best possible response time in the
online Your Benefits tool Delays or disruptions might
occur during evening hours when payroll functions are
running
Go to teamworkswellsfargo com
From work Click Pay amp Benefits then Benefits
Tools then Your Benefits
From home Click Your Benefits
1 On the Your Benefits tool home page click
Benefits Enrollment This link is active during your
enrollment and change periods only
2 Click Review Personal Information Check your
address and other information and update it if
necessary (You must do this only the first time you
view this site during a new enrollment period)
3 After reviewing your personal information you must
agree to the terms of the benefits enrollment before
you can proceed
4 When finished click Return to Benefits Enrollment
at the bottom of the page
Choose and save your plan elections
5 In the Enrollment Events table click Select The
Enrollment Summary page lists each benefit and
shows your current and new selections To make
changes to a benefits selection or to see all of that
benefit planrsquos choices and costs click Choose
6 On the enrollment page for each benefit click
one choice to elect a plan or waive coverage Add
dependent information if necessary (see If You Have
Eligible Dependents on page 6)
Note You can change elections at any time until your
designated enrollment period ends Any elections you
save will display when you return so you can verify or
make more changes
7 To save your election click Next review the
Confirmation page and click Save Yoursquoll return to
the Enrollment Summary page
Repeat steps 5 to 7 until you have selected all the plans
in which you want to enroll If you need to end your
session before completing all your benefits elections
complete step 7 and return later to finish enrolling
8 When yoursquove completed your benefits elections click
Finish The last page provides timing information for
the enrollment and change periods and a link to your
Benefi ts Confirmation Statement which you should
review for accuracy To exit the Your Benefits tool
click Sign Off at the top of the page
By phone
If you do not have online access from a computer or
have trouble signing on call the HR Service Center at
1-877-HRWELLS (1-877-479-3557) option 2 Monday
through Friday from 800 am to 500 pm in your time
zone The HR Service Center accepts relay service calls
TDDTTY users may call 1-800-988-0161
Confirm or correct your benefits elections
After you make your benefits elections you will receive
an email containing a link to access your Benefits
Confirmation Statement to review and print a copy for
your records This statement is also available from the
Your Benefits tool
Review your Benefits Confirmation Statement carefully
If you need to make changes to your benefits elections
follow the instructions on the statement If you make
corrections during your change period your benefits
administrators might not have a record of the changes
by the date on which your benefits become effective
your updated ID cards could be delayed as a result
Note If you receive your Benefits Confirmation
Statement by email (or similar electronic delivery)
you may request to have a paper copy sent to
you at no cost either by sending an email to
hrsddistributionfulfillmentwellsfargocom or by
calling the HR Service Center at 1-877-HRWELLS
(1-877-479-3557) option 2 The HR Service Center
accepts relay service calls TDDTTY users may call
1-800-988-0161
6
This paper copy will be the same version that you can
print from the Your Benefits tool If you donrsquot have
a valid Wells Fargo email address you will receive a
paper Benefi ts Confirmation Statement through the
US mail If you donrsquot have at-home or at-work access to
the Your Benefits tool call the HR Service Center with
your changes or corrections
If you have eligible dependents
You are eligible for benefits described in this booklet if
you are classified as either a regular team member who is
scheduled with standard hours of 30 or more hours per
week or a part-time team member who is scheduled with
standard hours of between 175 and 29 hours per week
In general your eligible dependents include
bull Your spouse or domestic partner
bull Your or your spouse or domestic partnerrsquos natural-
born or legally adopted child until his or her 26th
birthday
bull A child for whom you your spouse or your domestic
partner is the agency- or court-appointed legal
guardian or foster parent
See the Benefits Book on Teamworks and Teamworks
at Home (teamworkswellsfargocom) for complete
dependent eligibility requirements
Note Enrolling a dependent who does not meet
Wells Fargorsquos eligibility criteria is a violation of the
Code of Ethics and may result in disciplinary action
including termination of your employment with
Wells Fargo Wells Fargo reserves the right to conduct
audits and reviews of all dependent eligibility
To add eligible dependents
1 Click Add Dependent Details on the enrollment
page for any benefit that allows dependent
enrollment Note that you must enroll in the plan
yourself fi rst
2 On the DependentBeneficiary Personal Information
page enter the required information
3 Review the information carefully mdash you wonrsquot be
able to update it online later (except for a spouse or
domestic partnerrsquos smoker status) Click Save
4 The new dependent will be shown on the enrollment
page for any benefit that allows dependent
enrollment Repeat steps 1 to 3 to list more
dependents
5 Any dependents you listed will now appear with
checkboxes that allow you to add them to your
benefi ts coverage
6 Check the Enroll checkboxes next to the names of
the dependents you want to enroll
7 Click Next Follow the certification instructions
To certify newly enrolled eligible dependents
If you enroll an eligible dependent in coverage
yoursquore required to complete a brief certifi cation of
benefits eligibility Certification is triggered for these
dependents after you select the Enroll checkbox and
click Next on the benefits enrollment page
1 Read the overview page and click Continue
2 The certification page includes the eligible
dependentrsquos name and the benefits eligibility
requirements specific to the eligible dependentrsquos
relationship to you Read it and enter any required
information If your dependent qualifi es click I
Certify For any who donrsquot qualify click I Do Not
Certify You will not be able to enroll an uncertified
dependent
bullensp If you have several eligible dependents to certify
yoursquoll see a page for each one
bullensp When certifying an eligible dependent child of
a domestic partner you may need to certify the
domestic partner first even if you arenrsquot enrolling
the domestic partner in benefits coverage
3 When you finish certifying yoursquoll see the enrollment
confirmation page Review it and click Save
Yoursquoll return to the Enrollment Summary page After
you certify an eligible dependent in one plan you
may enroll him or her in any additional benefits plans
without repeating the certification steps
Certification is not the same as enrollment mdash you will
still need to select the enrollment checkboxes for your
eligible dependents on every plan in which you want
them enrolled
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

6
This paper copy will be the same version that you can
print from the Your Benefits tool If you donrsquot have
a valid Wells Fargo email address you will receive a
paper Benefi ts Confirmation Statement through the
US mail If you donrsquot have at-home or at-work access to
the Your Benefits tool call the HR Service Center with
your changes or corrections
If you have eligible dependents
You are eligible for benefits described in this booklet if
you are classified as either a regular team member who is
scheduled with standard hours of 30 or more hours per
week or a part-time team member who is scheduled with
standard hours of between 175 and 29 hours per week
In general your eligible dependents include
bull Your spouse or domestic partner
bull Your or your spouse or domestic partnerrsquos natural-
born or legally adopted child until his or her 26th
birthday
bull A child for whom you your spouse or your domestic
partner is the agency- or court-appointed legal
guardian or foster parent
See the Benefits Book on Teamworks and Teamworks
at Home (teamworkswellsfargocom) for complete
dependent eligibility requirements
Note Enrolling a dependent who does not meet
Wells Fargorsquos eligibility criteria is a violation of the
Code of Ethics and may result in disciplinary action
including termination of your employment with
Wells Fargo Wells Fargo reserves the right to conduct
audits and reviews of all dependent eligibility
To add eligible dependents
1 Click Add Dependent Details on the enrollment
page for any benefit that allows dependent
enrollment Note that you must enroll in the plan
yourself fi rst
2 On the DependentBeneficiary Personal Information
page enter the required information
3 Review the information carefully mdash you wonrsquot be
able to update it online later (except for a spouse or
domestic partnerrsquos smoker status) Click Save
4 The new dependent will be shown on the enrollment
page for any benefit that allows dependent
enrollment Repeat steps 1 to 3 to list more
dependents
5 Any dependents you listed will now appear with
checkboxes that allow you to add them to your
benefi ts coverage
6 Check the Enroll checkboxes next to the names of
the dependents you want to enroll
7 Click Next Follow the certification instructions
To certify newly enrolled eligible dependents
If you enroll an eligible dependent in coverage
yoursquore required to complete a brief certifi cation of
benefits eligibility Certification is triggered for these
dependents after you select the Enroll checkbox and
click Next on the benefits enrollment page
1 Read the overview page and click Continue
2 The certification page includes the eligible
dependentrsquos name and the benefits eligibility
requirements specific to the eligible dependentrsquos
relationship to you Read it and enter any required
information If your dependent qualifi es click I
Certify For any who donrsquot qualify click I Do Not
Certify You will not be able to enroll an uncertified
dependent
bullensp If you have several eligible dependents to certify
yoursquoll see a page for each one
bullensp When certifying an eligible dependent child of
a domestic partner you may need to certify the
domestic partner first even if you arenrsquot enrolling
the domestic partner in benefits coverage
3 When you finish certifying yoursquoll see the enrollment
confirmation page Review it and click Save
Yoursquoll return to the Enrollment Summary page After
you certify an eligible dependent in one plan you
may enroll him or her in any additional benefits plans
without repeating the certification steps
Certification is not the same as enrollment mdash you will
still need to select the enrollment checkboxes for your
eligible dependents on every plan in which you want
them enrolled
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
7
Making changes after your designated enrollment period
If you experience a Qualified Event mdash such as a
change of marital or employment status or the birth or
adoption of a child mdash you may be able to change certain
benefits elections by calling the HR Service Center
within 60 days of the Qualified Event to update your
coverage
See the Benefits Book for more information about
Qualified Events If you donrsquot contact the HR Service
Center within 60 days of your Qualified Event yoursquoll
have to wait until the next Annual Benefits Enrollment
period to change your benefi ts elections
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
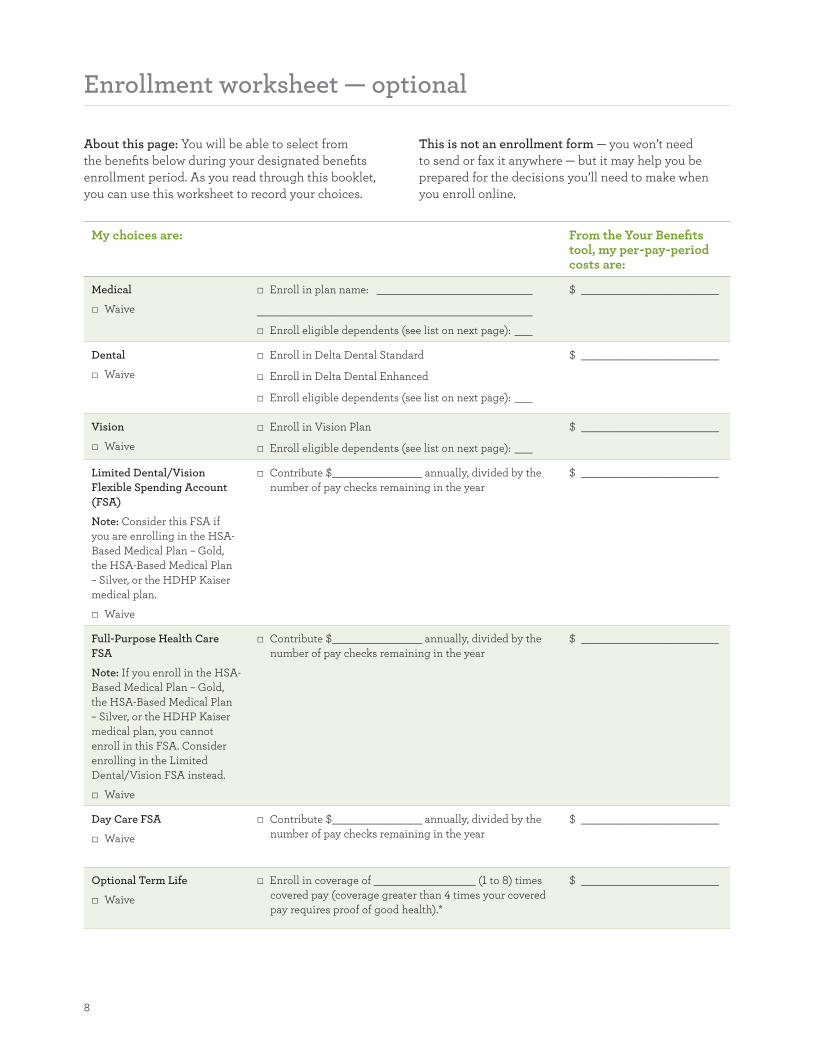
8
__________________________
______________________________________________
ensp ___
_______________________
___
_______________________
___
_______________________
_______________________
________________________________________
_______________
_______________ _______________________
_______________ _______________________
Enrollment worksheet mdash optional
About this page You will be able to select from
the benefits below during your designated benefi ts
enrollment period As you read through this booklet
you can use this worksheet to record your choices
This is not an enrollment form mdash you wonrsquot need
to send or fax it anywhere mdash but it may help you be
prepared for the decisions yoursquoll need to make when
you enroll online
My choices are From the Your Benefits tool my per-pay-period costs are
Medical
Waive
Enroll in plan name
Enroll eligible dependents (see list on next page)
$
Dental
Waive
Enroll in Delta Dental Standard
Enroll in Delta Dental Enhanced
Enroll eligible dependents (see list on next page)
$
Vision
Waive
Enroll in Vision Plan
Enroll eligible dependents (see list on next page)
$
Limited DentalVision
Flexible Spending Account
(FSA)
Note Consider this FSA if
you are enrolling in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Full-Purpose Health Care
FSA
Note If you enroll in the HSA-
Based Medical Plan ndash Gold
the HSA-Based Medical Plan
ndash Silver or the HDHP Kaiser
medical plan you cannot
enroll in this FSA Consider
enrolling in the Limited
DentalVision FSA instead
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Day Care FSA
Waive
Contribute $ annually divided by the
number of pay checks remaining in the year
$
Optional Term Life
Waive
Enroll in coverage of (1 to 8) times
covered pay (coverage greater than 4 times your covered
pay requires proof of good health)
$
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
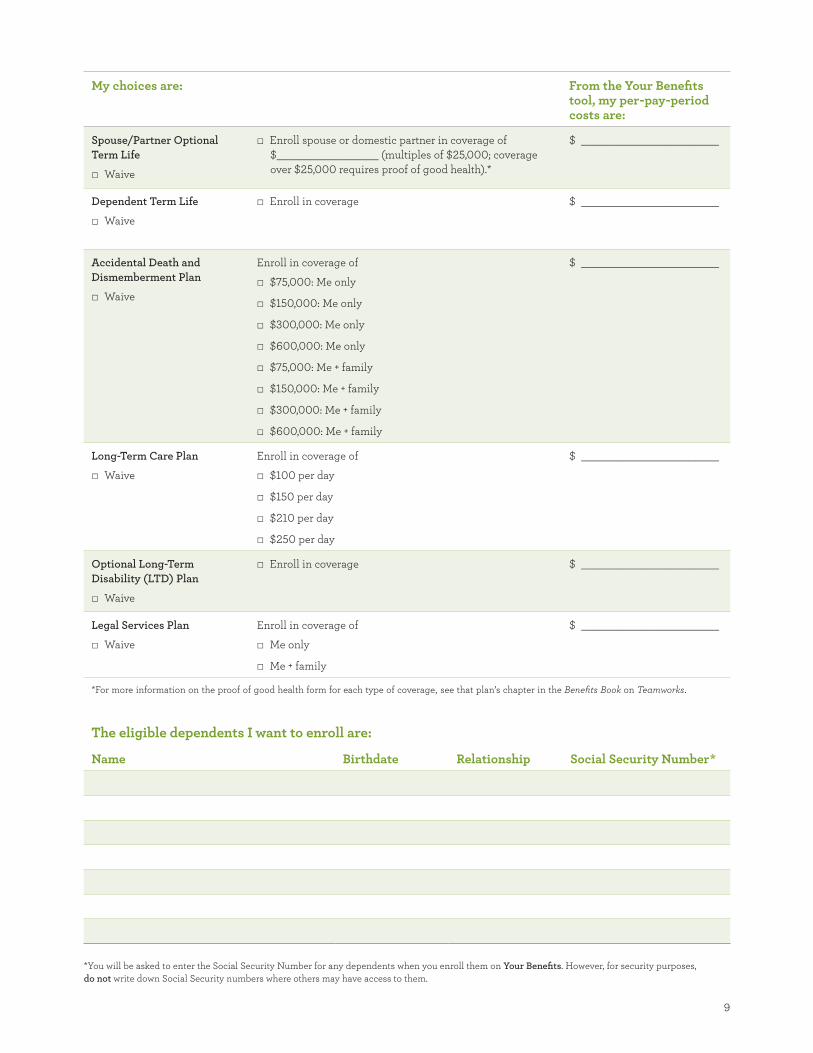
9
My choices are From the Your Benefi ts tool my per-pay-period costs are
ensp
_________________
_______________________
ensp
ensp _______________________
ensp
_______________________
ensp
ensp ensp
ensp
ensp
ensp
ensp
ensp
ensp
_______________________
ensp ensp
ensp
ensp
ensp
ensp _______________________
ensp
_______________________
ensp ensp
ensp
SpousePartner Optional
Term Life
Waive
Enroll spouse or domestic partner in coverage of
$ (multiples of $25000 coverage
over $25000 requires proof of good health)
$
Dependent Term Life
Waive
Enroll in coverage $
Accidental Death and
Dismemberment Plan
Waive
Enroll in coverage of
$75000 Me only
$150000 Me only
$300000 Me only
$600000 Me only
$75000 Me + family
$150000 Me + family
$300000 Me + family
$600000 Me + family
$
Long-Term Care Plan
Waive
Enroll in coverage of
$100 per day
$150 per day
$210 per day
$250 per day
$
Optional Long-Term
Disability (LTD) Plan
Waive
Enroll in coverage $
Legal Services Plan
Waive
Enroll in coverage of
Me only
Me + family
$
For more information on the proof of good health form for each type of coverage see that planrsquos chapter in the Benefits Book on Teamworks
The eligible dependents I want to enroll are
Name Birthdate Relationship Social Security Number
You will be asked to enter the Social Security Number for any dependents when you enroll them on Your Benefits However for security purposes
do not write down Social Security numbers where others may have access to them
10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

10
Medical coverage YOUR CHOICE
All our medical plans offer
bull Eligible preventive care services covered at 100
when you use in-network providers
bull Comprehensive medical coverage that includes
routine care emergency care and mental health and
substance abuse services
bull Comprehensive prescription drug benefits
bull Annual limits on what you might pay to provide
fi nancial protection
bull A large network of doctors hospitals and other
providers that offer services at negotiated rates
bull Personalized one-on-one programs to help you and your
covered dependents improve or maintain your health
and well-being
Wells Fargo gives you a choice of three medical plans
that come with accounts mdash the Health Reimbursement
Account (HRA)-Based Medical Plan and two health
savings account (HSA)-based medical plans the
HSA-Based Medical Plan ndash Gold and the HSA-Based
Medical Plan ndash Silver Another account-based plan the
High-Deductible Health Plan (HDHP) Kaiser medical
plan is also available in select locations
If you live in These plans are available to you
Any state
except Hawaii
bullensp HRA-Based Medical Plan
bullensp HSA-Based Medical Plan ndash Gold
bullensp HSA-Based Medical Plan ndash Silver
Kaiser available in
the following service
areas within California
Colorado (Denver
and Colorado Springs
areas) Oregon
(Portland and Salem
areas) or Washington
(Vancouver Longview
and Kelso areas)
bullensp HDHP Kaiser medical plan
bullensp Kaiser HMO medical plan
Hawaii bullensp POS Kaiser Added Choice
Each medical planrsquos claims networks and provider fees are handled by a claims administrator For contact
information for the administrators see page 43
Medical Plan Claims administrator State or territory
HRA-Based
Medical Plan
HSA-Based
Medical Plan
UnitedHealthcare Alabama Arizona Arkansas Colorado District of Columbia Florida
Illinois Iowa Louisiana Maine Maryland Massachusetts Mississippi
Missouri Nebraska Nevada New Hampshire New Jersey New Mexico
Oregon Utah Wisconsin Wyoming
Anthem BCBS Alaska California Connecticut Delaware Georgia Idaho Indiana Kansas
Kentucky Michigan Montana New York North Carolina North Dakota
Ohio Oklahoma Pennsylvania Rhode Island South Carolina South
Dakota Tennessee Texas Vermont Virginia Washington West Virginia
HealthPartners Minnesota
Indemnity Medical
Plan mdash Anthem BCBS
Anthem BCBS Puerto Rico Guam and the Northern Mariana Islands (Saipan) Not
available in the 50 United States or in the District of Columbia
CVScaremark is the prescription drug administrator for all the medical plans listed above
Kaiser medical
plans
Kaiser Permanente Residents of Kaiser service areas within California Colorado (Denver
and Colorado Springs areas) Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added
Choice mdash Hawaii
Kaiser Permanente Hawaii
The Kaiser HMO HDHP Kaiser medical plan and the POS Kaiser Added Choice are fully insured medical plans under the Wells Fargo amp
Company Health Plan The benefits described in this booklet do not apply The descriptions of plan benefits for the various Kaiser medical
plans are provided in separate documentation that will be sent to you by Kaiser if you enroll in the applicable plan The information that
comprises the complete Summary Plan Description for the applicable Kaiser plan is noted in Chapter 1 of the Benefits Book
Note If you live in Puerto Rico Guam or the Northern Mariana Islands (Saipan) or are an expatriate view the plan
options shown on the Your Benefits tool
11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

11
Account-based medical plans overview
Wells Fargo sponsors a choice of three national account-
based health plans in the continental United States
bull The HRA-Based Medical Plan
bull The HSA-Based Medical Plan ndash Gold
bull The HSA-Based Medical Plan ndash Silver
Our medical plans help you manage your health
care expenses with comprehensive medical and
prescription drug coverage and the advantages of a
health reimbursement or health savings account These
account-based medical plans allow you to use a health
reimbursement account (HRA) or a health savings
account (HSA) to plan and pay for qualifi ed medical
expenses
You are responsible for understanding how your plans
work how they pay for services and how your account
supports your benefi ts throughout the year
Check out the Quick Comparison Chart on page 20
for more information For additional details about the
medical plans see Chapter 2 of the Benefi ts Book
Thinking and acting like a health care consumer
Understand how your medical plan works you and
your plan share the responsibility of paying for eligible
medical services Wells Fargo pays the majority of your
costs for coverage mdash on average 75 of your medical
premiums mdash and you are responsible for the rest
Knowing what your plan covers and your share of the
cost can help you make informed decisions throughout
the year
bull Research each plan yoursquore considering to understand
all covered services and costs
bull Use the Medical Plan Comparison Tool and the CVS
caremark website to help guide your decisions
bull Take control of your important health care decisions
from choosing a plan to knowing where to go for care
when you need it
bull Save money and time by making sure that all your
providers are in your planrsquos network
bull Once yoursquove selected a plan use your claims
administratorrsquos online tools to research the cost of
any service you may need
bull Work closely with your doctor by following care
regimens seeking guidance on maintaining your
health and asking questions
bull Never avoid getting care when you need it
You can further manage your costs by considering the
fl exible spending account (FSA) options available to
you depending on the plan in which you enroll Also
if you complete the health and wellness activities you
and your covered spouse or domestic partner may
each be able to earn up to $800 in health and wellness
dollars for your HRA or HSA
Eligible preventive care benefi ts are covered at 100 in network
The Wells Fargo-sponsored medical plans cover 100
of the cost of eligible in-network preventive care
services such as the types of services listed in the
charts below To be covered at 100 your provider
must code the eligible service as preventive care
Read more about preventive care coverage in Chapter 2
of the Benefits Book
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
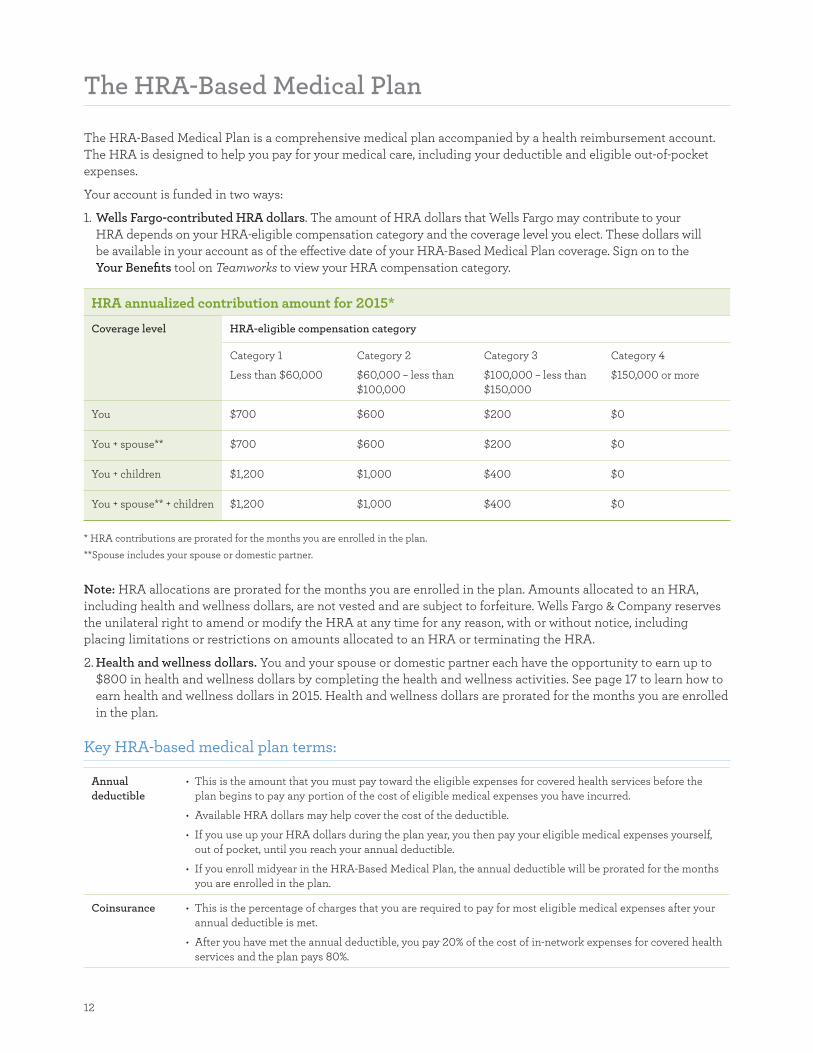
12
The HRA-Based Medical Plan
The HRA-Based Medical Plan is a comprehensive medical plan accompanied by a health reimbursement account
The HRA is designed to help you pay for your medical care including your deductible and eligible out-of-pocket
expenses
Your account is funded in two ways
1 Wells Fargo-contributed HRA dollars The amount of HRA dollars that Wells Fargo may contribute to your
HRA depends on your HRA-eligible compensation category and the coverage level you elect These dollars will
be available in your account as of the effective date of your HRA-Based Medical Plan coverage Sign on to the
Your Benefits tool on Teamworks to view your HRA compensation category
HRA annualized contribution amount for 2015
Coverage level HRA-eligible compensation category
Category 1
Less than $60000
Category 2
$60000 ndash less than
$100000
Category 3
$100000 ndash less than
$150000
Category 4
$150000 or more
You $700 $600 $200 $0
You + spouse $700 $600 $200 $0
You + children $1200 $1000 $400 $0
You + spouse + children $1200 $1000 $400 $0
HRA contributions are prorated for the months you are enrolled in the plan
Spouse includes your spouse or domestic partner
Note HRA allocations are prorated for the months you are enrolled in the plan Amounts allocated to an HRA
including health and wellness dollars are not vested and are subject to forfeiture Wells Fargo amp Company reserves
the unilateral right to amend or modify the HRA at any time for any reason with or without notice including
placing limitations or restrictions on amounts allocated to an HRA or terminating the HRA
2 Health and wellness dollars You and your spouse or domestic partner each have the opportunity to earn up to
$800 in health and wellness dollars by completing the health and wellness activities See page 17 to learn how to
earn health and wellness dollars in 2015 Health and wellness dollars are prorated for the months you are enrolled
in the plan
Key HRA-based medical plan terms
Annual
deductible
bullensp This is the amount that you must pay toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses you have incurred
bullensp Available HRA dollars may help cover the cost of the deductible
bullensp If you use up your HRA dollars during the plan year you then pay your eligible medical expenses yourself
out of pocket until you reach your annual deductible
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual deductible will be prorated for the months
you are enrolled in the plan
Coinsurance bullensp This is the percentage of charges that you are required to pay for most eligible medical expenses after your
annual deductible is met
bullensp After you have met the annual deductible you pay 20 of the cost of in-network expenses for covered health
services and the plan pays 80
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
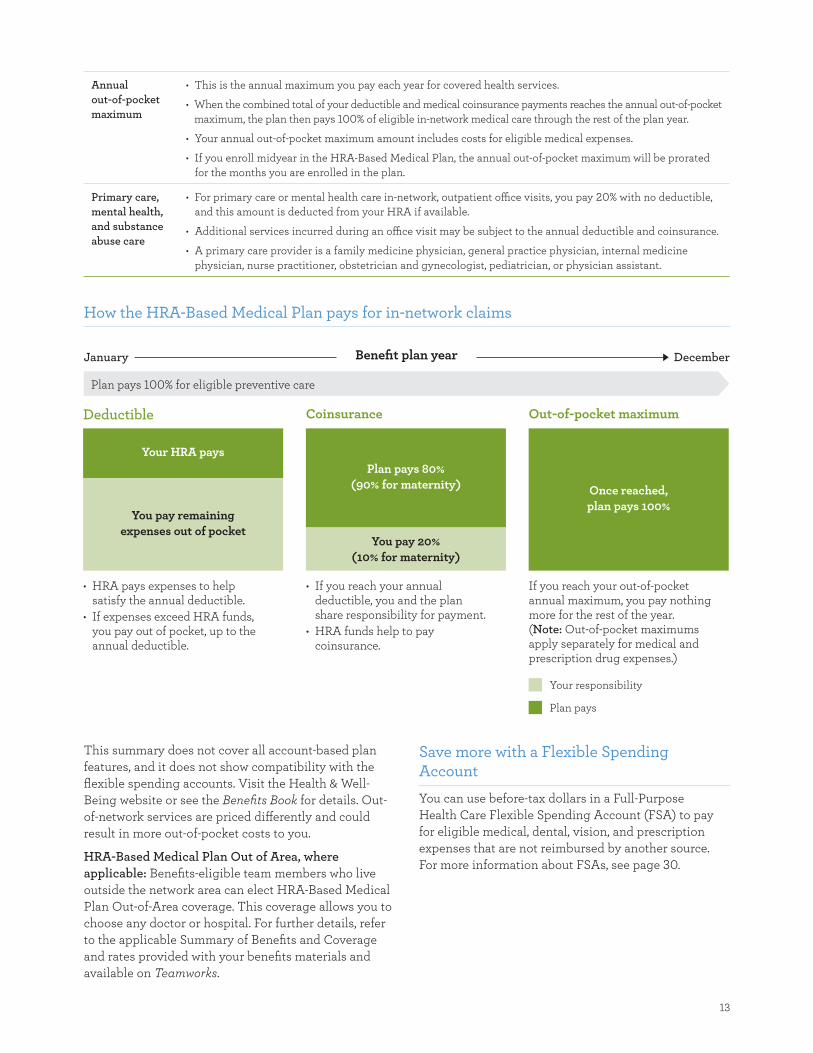
13
Your responsibility
Plan pays
Annual
out-of-pocket
maximum
bullensp This is the annual maximum you pay each year for covered health services
bullensp When the combined total of your deductible and medical coinsurance payments reaches the annual out-of-pocket
maximum the plan then pays 100 of eligible in-network medical care through the rest of the plan year
bullensp Your annual out-of-pocket maximum amount includes costs for eligible medical expenses
bullensp If you enroll midyear in the HRA-Based Medical Plan the annual out-of-pocket maximum will be prorated
for the months you are enrolled in the plan
Primary care
mental health
and substance
abuse care
bullensp For primary care or mental health care in-network outpatient offi ce visits you pay 20 with no deductible
and this amount is deducted from your HRA if available
bullensp Additional services incurred during an offi ce visit may be subject to the annual deductible and coinsurance
bullensp A primary care provider is a family medicine physician general practice physician internal medicine
physician nurse practitioner obstetrician and gynecologist pediatrician or physician assistant
How the HRA-Based Medical Plan pays for in-network claims
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
Your HRA pays
You pay remaining
expenses out of pocket
bull HRA pays expenses to help satisfy the annual deductible
bull If expenses exceed HRA funds you pay out of pocket up to the annual deductible
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20
(10 for maternity)
bull If you reach your annual deductible you and the plan share responsibility for payment
bull HRA funds help to pay coinsurance
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket annual maximum you pay nothing more for the rest of the year (Note Out-of-pocket maximums apply separately for medical and prescription drug expenses)
This summary does not cover all account-based plan
features and it does not show compatibility with the
flexible spending accounts Visit the Health amp Well-
Being website or see the Benefits Book for details Out-
of-network services are priced differently and could
result in more out-of-pocket costs to you
HRA-Based Medical Plan Out of Area where
applicable Benefits-eligible team members who live
outside the network area can elect HRA-Based Medical
Plan Out-of-Area coverage This coverage allows you to
choose any doctor or hospital For further details refer
to the applicable Summary of Benefits and Coverage
and rates provided with your benefits materials and
available on Teamworks
Save more with a Flexible Spending Account
You can use before-tax dollars in a Full-Purpose
Health Care Flexible Spending Account (FSA) to pay
for eligible medical dental vision and prescription
expenses that are not reimbursed by another source
For more information about FSAs see page 30
14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

14
HSA-Based Medical Plans (Gold and Silver)
The HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver are comprehensive high-
deductible health plans that are compatible with health
savings accounts and are designed to help you save and
pay for your medical care mental health and substance
abuse services and prescription expenses You decide
when to use your available HSA balance to pay for
eligible services
Key HSA-based medical plan terms
Annual
deductible
bullensp This is the amount you pay each year toward the eligible expenses for covered health services before the
plan begins to pay any portion of the cost of eligible medical expenses
bullensp You pay 100 of health care costs including prescription drugs that are not on the preventive therapy
drug list from your HSA or out of pocket until you meet the annual deductible
Coinsurance bullensp The percentage of charges you are required to pay for most eligible medical expenses after your annual
deductible is met
bullensp The plan pays the rest for covered health services
Annual out-of-
pocket maximum
bullensp This is the annual maximum you would ever pay each year for covered health services
bullensp If your coinsurance payments reach the annual out-of-pocket maximum the plan then covers eligible
in-network medical care at 100 through the rest of the plan year
bullensp Your annual out-of-pocket maximum includes costs for eligible medical mental health and prescription drugs
Both the HSA-Based Medical Plan ndash Gold and the HSA-
Based Medical Plan ndash Silver
bull Cover 100 of your eligible in-network preventive
care subject to certain limitations
bull Cover 80 of costs for prescription drugs on the
Preventive Therapy Drug List purchased at in-
network pharmacies or from the CVScaremark Mail
Service pharmacy you pay only 20 and have no
deductible
The HSA-Based Medical Plan ndash Silver pays 80
(you pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
The HSA-Based Medical Plan ndash Gold pays 80 (you
pay only 20) of the cost of in-network medical
services and prescription drugs after you meet the in-
network deductible
While still a high-deductible plan the HSA-Based
Medical Plan ndash Gold offers a lower annual deductible
and lower annual out-of-pocket maximum than the
HSA-Based Medical Plan ndash Silver
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
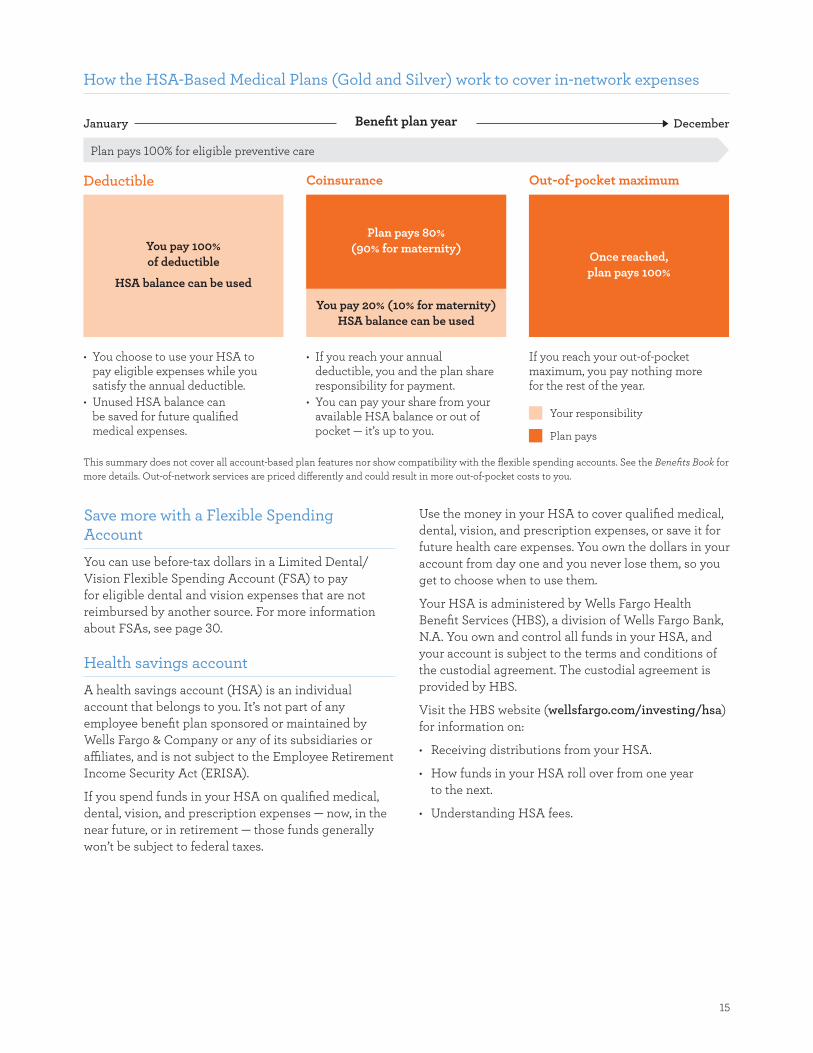
15
Your responsibility
Plan pays
How the HSA-Based Medical Plans (Gold and Silver) work to cover in-network expenses
January Benefit plan year December
Plan pays 100 for eligible preventive care
Deductible
You pay 100
of deductible
HSA balance can be used
bull You choose to use your HSA to pay eligible expenses while you satisfy the annual deductible
bull Unused HSA balance can be saved for future qualified medical expenses
Coinsurance
Plan pays 80
(90 for maternity)
You pay 20 (10 for maternity)
HSA balance can be used
bull If you reach your annual deductible you and the plan share responsibility for payment
bull You can pay your share from your available HSA balance or out of pocket mdash itrsquos up to you
Out-of-pocket maximum
Once reached
plan pays 100
If you reach your out-of-pocket maximum you pay nothing more for the rest of the year
This summary does not cover all account-based plan features nor show compatibility with the flexible spending accounts See the Benefits Book for
more details Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Save more with a Flexible Spending Account
You can use before-tax dollars in a Limited Dental
Vision Flexible Spending Account (FSA) to pay
for eligible dental and vision expenses that are not
reimbursed by another source For more information
about FSAs see page 30
Health savings account
A health savings account (HSA) is an individual
account that belongs to you Itrsquos not part of any
employee benefit plan sponsored or maintained by
Wells Fargo amp Company or any of its subsidiaries or
affi liates and is not subject to the Employee Retirement
Income Security Act (ERISA)
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualifi ed medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Your HSA is administered by Wells Fargo Health
Benefit Services (HBS) a division of Wells Fargo Bank
NA You own and control all funds in your HSA and
your account is subject to the terms and conditions of
the custodial agreement The custodial agreement is
provided by HBS
Visit the HBS website (wellsfargocominvestinghsa)
for information on
bull Receiving distributions from your HSA
bull How funds in your HSA roll over from one year
to the next
bull Understanding HSA fees
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
16
HSA eligibility
You must be enrolled in an HSA-based medical plan to
make payroll contributions to the HSA
In general you cannot contribute to an HSA if you
bull Are covered under any nonndashhigh-deductible health plan
bull Are entitled to benefits under Medicare (that is you
are enrolled in Medicare)
bull Are eligible to be claimed as a dependent on another
personrsquos tax return Please note that a spouse or
domestic partner is not considered a dependent for
this purpose
bull Have received medical benefits from the US
Department of Veterans Affairs at any time during
the preceding three months
bull Are enrolled in the Full-Purpose Health Care FSA
through Wells Fargo or your spouse or domestic
partnerrsquos employer
In addition individuals covered as dependents under a
parentrsquos Full-Purpose Health Care FSA are not eligible
to contribute to an HSA You must be enrolled in an
HSA-based medical plan in order to make payroll
contributions to your HSA Consult your tax advisor if
you have questions
Contributing to your HSA
Using the Your Benefits tool on Teamworks you choose
how often and how much you want to contribute to
your HSA per pay period You can make updates at
any time You can allocate certain dollar amounts on
specific paydays or adjust the timing of your annual
deductions You may also establish an annual HSA
payroll contribution by contacting the HR Service
Center at 1-877-HRWELLS (1-877-479-3557) option 2
Any contributions made by Wells Fargo count toward
your maximum annual contribution limit as set by
the IRS Because you have the opportunity to earn
health and wellness dollars the annual maximum HSA
contributions through Wells Fargo payroll for 2015 are
less than the IRS maximum
You only $3350
You + spouse $6650
You + children $6650
You + spouse + children $6650
Team member age 55+ catch-up $1000
Includes eligible spouse or domestic partner
Includes spousersquos or domestic partnerrsquos eligible children
Domestic Partner HSA information
When you enroll in any of the medical plans that are
compatible with an HSA your domestic partner will
have benefits coverage under the medical portion of
the plan In that case you will have a shared deductible
and out-of-pocket maximum for the medical plan when
you select employee plus spouse or domestic partner
coverage
Whether you can pay your domestic partnerrsquos medical
expenses with your HSA depends on whether your
domestic partner qualifies as a tax dependent If you
can claim your domestic partner as a dependent on
your federal income tax return distributions for his or
her medical expenses are tax-free
bull Any individual you can claim as a tax dependent as
defined by Internal Revenue Code is not eligible to
open or contribute to his or her own HSA
bull If your domestic partner is not a tax dependent
distributions from your HSA for his or her medical
expenses are not tax-free
ndash Wells Fargo offers an annual special wage payment
for team members who cover a same-sex domestic
partner (andor his or her children) designated as
after-tax dependents in Wells Fargo-sponsored
medical dental or vision coverage
bull A domestic partner whom you cannot claim as your
dependent may open and contribute to his or her own
HSA
Your covered domestic partner is eligible to open an
HSA through Wells Fargo Health Benefit Services
(HBS) or any other HSA administrator as long as
he or she is enrolled in a qualifying high-deductible
health plan If your domestic partner has his or her own
HSA you might need to divide the maximum HSA
contribution limit between the two of you If you have
questions about allocating contribution limits between
domestic partners consult a tax advisor
17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

17
Health and wellness dollars
When you enroll in an account-based medical plan
(the HRA-Based Medical Plan one of the HSA-based
medical plans or the HDHP Kaiser medical plan) you
can earn health and wellness dollars for your HRA or
HSA by completing health and wellness activities and
educational programs
Depending on the activities completed you and your
covered spouse or domestic partner if he or she is also
enrolled could each earn up to $800 for your HRA or
HSA If you enroll midyear the amount of health and
wellness dollars that you can earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account
As you complete the activities health and wellness
dollars will be deposited to your HRA or HSA in
approximately 30 days Health and wellness dollars
cannot be deposited either in the Full-Purpose Health
Care FSA or the Limited DentalVision FSA
Activities that allow you to earn health and wellness dollars
Before you can earn health and wellness dollars you
must register on the Optum website Optum is the
Wells Fargo provider for health and wellness activities
Registration takes only a few minutes and once yoursquore
registered you can use this same account for all of
the activities Note You and your spouse or domestic
partner may complete the health and wellness activities
only after your medical coverage effective date It may
take up to two weeks after your coverage effective date
before you are able to register on the Optum website
Visit the Health amp Well-Being website on Teamworks for
detailed registration instructions and helpful links or go
to the Optum website (wellnessmyoptumhealthcom)
and click Register in the upper right corner of the page
If you are unable to register online contact Optum at
1-877-543-4294
Health and wellness activity
Maximum health and wellness dollars for you
Maximum health and wellness dollars for your covered spouse or domestic partner
Time to complete activity How to complete the activity
Health
assessment
$150 $150 About 15 minutes Sign on to the Optum website
and fi ll out the confi dential
questionnaire
Biometric
screening
$250 $250 About 30 minutes at either an
event on site at a Wells Fargo
location or an appointment with
your doctor preferably at the time
of your annual preventive exam
Sign on to the Optum website
and register for an on-site
event or print a personalized
Health Provider Screening
Form for your personal doctor
to complete
Online
wellness
education
programs or
telephonic
wellness
coaching
program
$400 $400 6 to 8 weeks to complete one of
the following
bullensp Online Wellness Education
Program Complete 12 activities
and five weekly tracker entries
bullensp Telephonic Wellness Coaching
Program Complete two
outbound coaching calls
Online Wellness Education
Program Sign on to the
Optum website and complete
the program requirements
Telephonic Wellness
Coaching Program
Call Optum at
1-877-440-9402 to register
Summary $800 $800 30 days to deposit funds in
your HRA or HSA
Important dates for earning health and wellness dollars
Complete the health and wellness activities between your medical plan coverage effective date and November 15
2015 to earn health and wellness dollars in 2015
18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

18
Prescription drug coverage under
the account-based plans
Comprehensive prescription drug benefits for the
account-based medical plans are administered by
CVScaremark The nationwide network of more than
64000 pharmacies includes most retail chains and
many independent pharmacies in addition to the CVS
caremark Mail Service Pharmacy
About 90 of team members in account-based plans
are already saving money by choosing generic versions
of their drugs You can cut your costs further by
switching to a 90-day supply of the prescriptions you
take regularly Call CVScaremark at 1-855-673-6197
and they will take care of switching to 90-day supplies
for you You can have your prescriptions mailed to you
or you can pick them up at a CVSpharmacy store
Visit the CVScaremark Prescription Benefits Preview
website at caremarkcomwf to
bull Check drug costs
bull See if your drug requires prior authorization requires
you to first try an alternative drug or has quantity
limits
bull View the Advance Formulary drug list
bull View the Preventive Therapy Drug List Drugs on this
list are not subject to the deductible for the HSA-
based medical plans
bull Learn how you can save time and money by
switching to 90-day supply prescriptions
Comparing the account-based plans (in network)
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Is there a copay
for generic
prescription
drugs
Yes $7 retail (up to a 30-day supply)
$14 mail service (up to a 90-day supply)
or CVSpharmacy stores
(84- to 90-day supplies only)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
No coinsurance applies
You pay 20 after annual
deductible (or 20 with no
deductible for drugs on the
preventive therapy drug list)
Are prescription
drugs part of
the medical
out-of-pocket
maximum
No There is a separate annual out-of-
pocket maximum for prescriptions you
purchase at
bullensp CVScaremark Mail Service Pharmacy
(up to a 90-day supply)
bullensp CVSpharmacy stores
(84- to 90-day supplies only)
bullensp Other in-network retail pharmacies
(up to 30-day supply)
bullensp CVScaremark Specialty Pharmacy
(up to a 90-day supply)
Yes Yes
Benefits are determined using the plansrsquo allowed amounts for eligible covered expenses If you buy a brand-name drug when generic is available you also
pay the cost difference which is not applied to your deductible (HSA-based medical plans only) or out-of-pocket maximum Out-of-network prescriptions
are covered differently they have separate deductibles and out-of-pocket maximums and could result in more out-of-pocket costs to you
19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

19
Additional requirements for some prescription drugs
Some drugs have additional requirements that must be
met before the plan will cover your prescription
bull Certain medications require prior authorization by
CVScaremark before your prescription can be fi lled
bull Some plans require step therapy This means that if
you are prescribed a drug you might be required to
first try a generic drug or other therapy before the
plan will cover certain drugs
bull Most specialty medications mdash typically medications
that are self-injectable or require special handling
mdash are available only through the CVScaremark
Specialty Pharmacy not through retail pharmacies
bull Some drugs are covered only for certain limited
quantities based on manufacturer and clinical
guidelines
For more information about additional requirements
visit the CVScaremark Prescription Benefits Preview
website (caremarkcomwf) and see Chapter 2 of the
Benefits Book
Save more with a Flexible Spending Account
If you enroll in the HRA-based medical plan you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
prescription expenses that are not reimbursed by
another source For more information about FSAs see
page 30
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
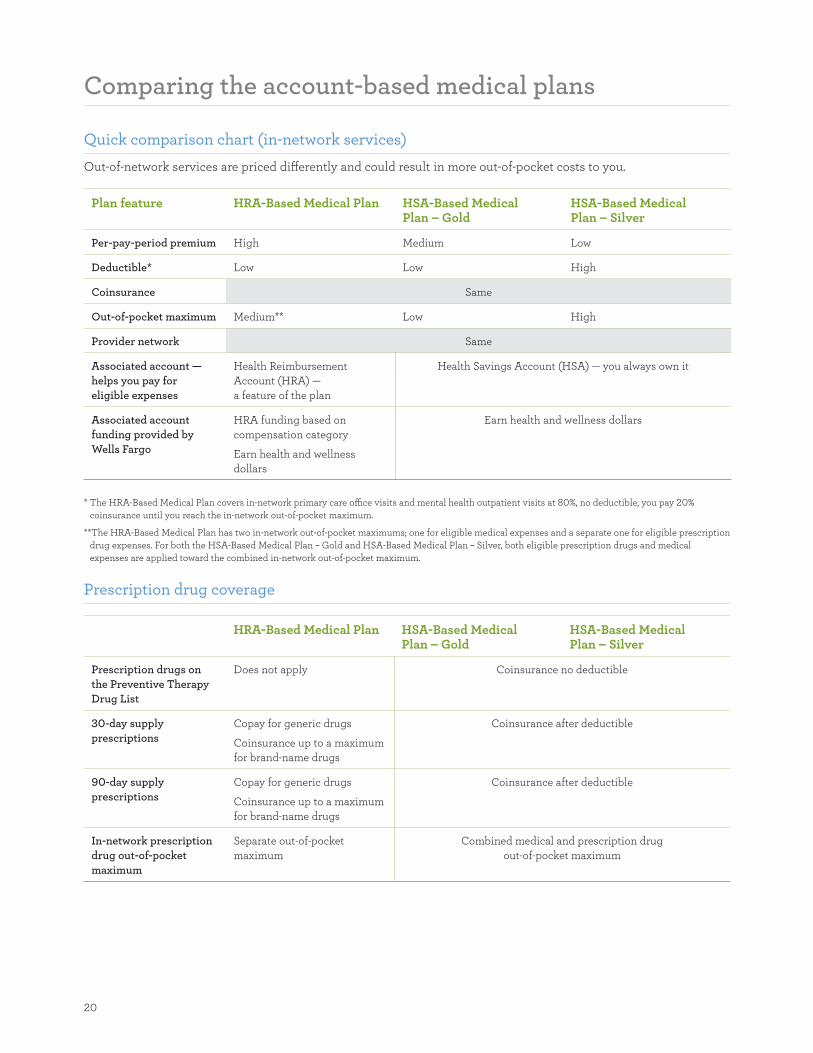
20
Comparing the account-based medical plans
Quick comparison chart (in-network services)
Out-of-network services are priced differently and could result in more out-of-pocket costs to you
Plan feature HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Per-pay-period premium High Medium Low
Deductible Low Low High
Coinsurance Same
Out-of-pocket maximum Medium Low High
Provider network Same
Associated account mdash
helps you pay for
eligible expenses
Health Reimbursement
Account (HRA) mdash
a feature of the plan
Health Savings Account (HSA) mdash you always own it
Associated account
funding provided by
Wells Fargo
HRA funding based on
compensation category
Earn health and wellness
dollars
Earn health and wellness dollars
The HRA-Based Medical Plan covers in-network primary care office visits and mental health outpatient visits at 80 no deductible you pay 20
coinsurance until you reach the in-network out-of-pocket maximum
The HRA-Based Medical Plan has two in-network out-of-pocket maximums one for eligible medical expenses and a separate one for eligible prescription
drug expenses For both the HSA-Based Medical Plan ndash Gold and HSA-Based Medical Plan ndash Silver both eligible prescription drugs and medical
expenses are applied toward the combined in-network out-of-pocket maximum
Prescription drug coverage
HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Prescription drugs on
the Preventive Therapy
Drug List
Does not apply Coinsurance no deductible
30-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
90-day supply
prescriptions
Copay for generic drugs
Coinsurance up to a maximum
for brand-name drugs
Coinsurance after deductible
In-network prescription
drug out-of-pocket
maximum
Separate out-of-pocket
maximum
Combined medical and prescription drug
out-of-pocket maximum
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
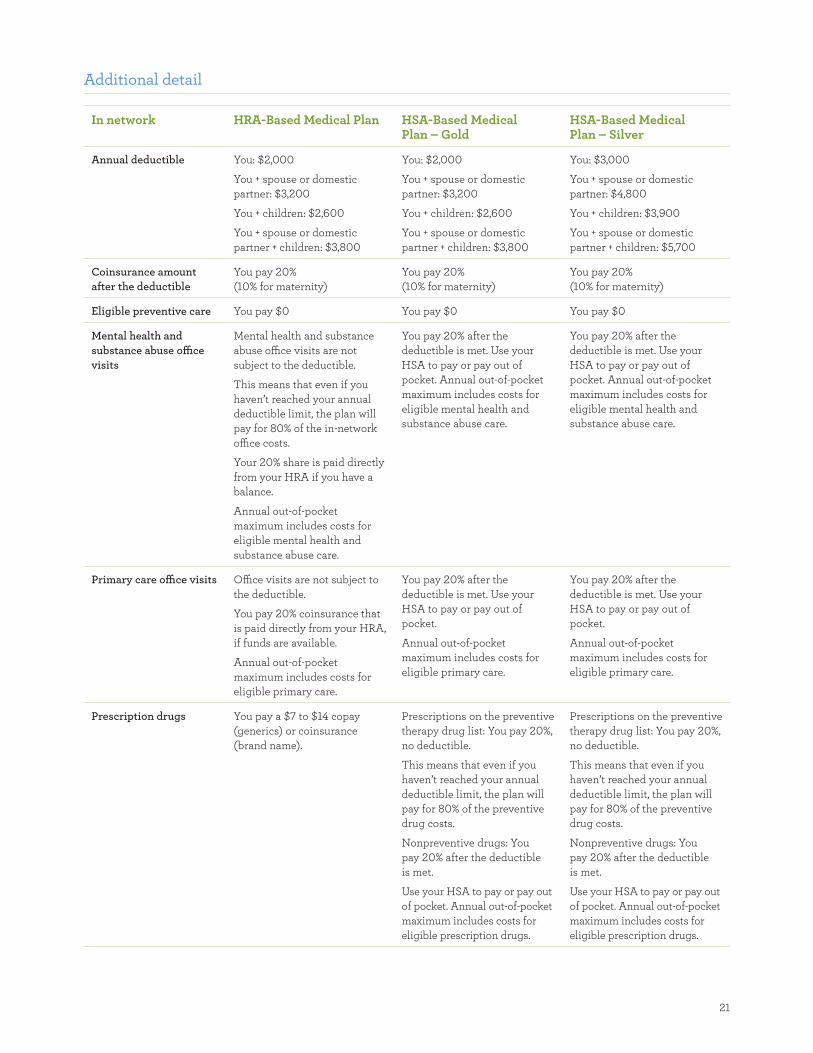
21
Additional detail
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Annual deductible You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $2000
You + spouse or domestic
partner $3200
You + children $2600
You + spouse or domestic
partner + children $3800
You $3000
You + spouse or domestic
partner $4800
You + children $3900
You + spouse or domestic
partner + children $5700
Coinsurance amount
after the deductible
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
You pay 20
(10 for maternity)
Eligible preventive care You pay $0 You pay $0 You pay $0
Mental health and
substance abuse office
visits
Mental health and substance
abuse office visits are not
subject to the deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the in-network
office costs
Your 20 share is paid directly
from your HRA if you have a
balance
Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
pocket Annual out-of-pocket
maximum includes costs for
eligible mental health and
substance abuse care
Primary care office visits Office visits are not subject to
the deductible
You pay 20 coinsurance that
is paid directly from your HRA
if funds are available
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum includes costs for
eligible primary care
Prescription drugs You pay a $7 to $14 copay
(generics) or coinsurance
(brand name)
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
Prescriptions on the preventive
therapy drug list You pay 20
no deductible
This means that even if you
havenrsquot reached your annual
deductible limit the plan will
pay for 80 of the preventive
drug costs
Nonpreventive drugs You
pay 20 after the deductible
is met
Use your HSA to pay or pay out
of pocket Annual out-of-pocket
maximum includes costs for
eligible prescription drugs
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
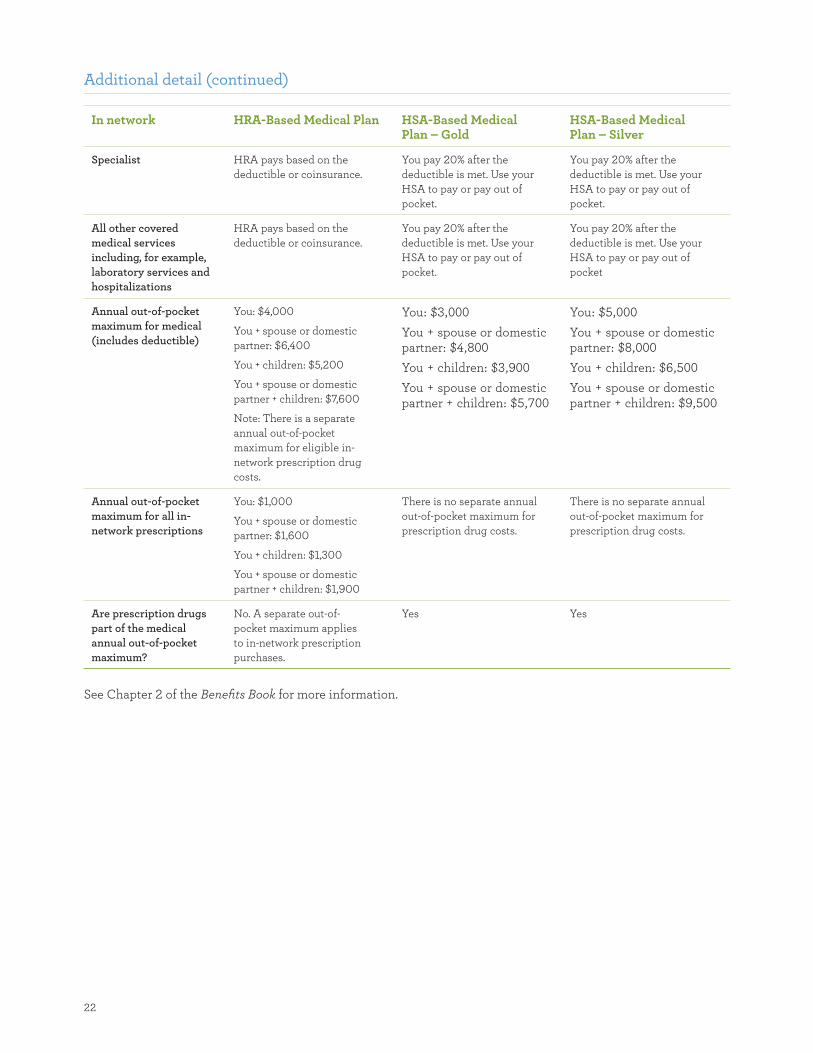
22
Additional detail (continued)
In network HRA-Based Medical Plan HSA-Based Medical Plan ndash Gold
HSA-Based Medical Plan ndash Silver
Specialist HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
All other covered
medical services
including for example
laboratory services and
hospitalizations
HRA pays based on the
deductible or coinsurance
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
You pay 20 after the
deductible is met Use your
HSA to pay or pay out of
Annual out-of-pocket
maximum for medical
(includes deductible)
You $4000
You + spouse or domestic
partner $6400
You + children $5200
You + spouse or domestic
partner + children $7600
Note There is a separate
annual out-of-pocket
maximum for eligible in-
network prescription drug
costs
You $3000
You + spouse or domestic partner $4800
You + children $3900
You + spouse or domestic partner + children $5700
You $5000
You + spouse or domestic partner $8000
You + children $6500
You + spouse or domestic partner + children $9500
Annual out-of-pocket
maximum for all in-
network prescriptions
You $1000
You + spouse or domestic
partner $1600
You + children $1300
You + spouse or domestic
partner + children $1900
There is no separate annual
out-of-pocket maximum for
prescription drug costs
There is no separate annual
out-of-pocket maximum for
prescription drug costs
Are prescription drugs
part of the medical
annual out-of-pocket
maximum
No A separate out-of-
pocket maximum applies
to in-network prescription
purchases
Yes Yes
See Chapter 2 of the Benefits Book for more information
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
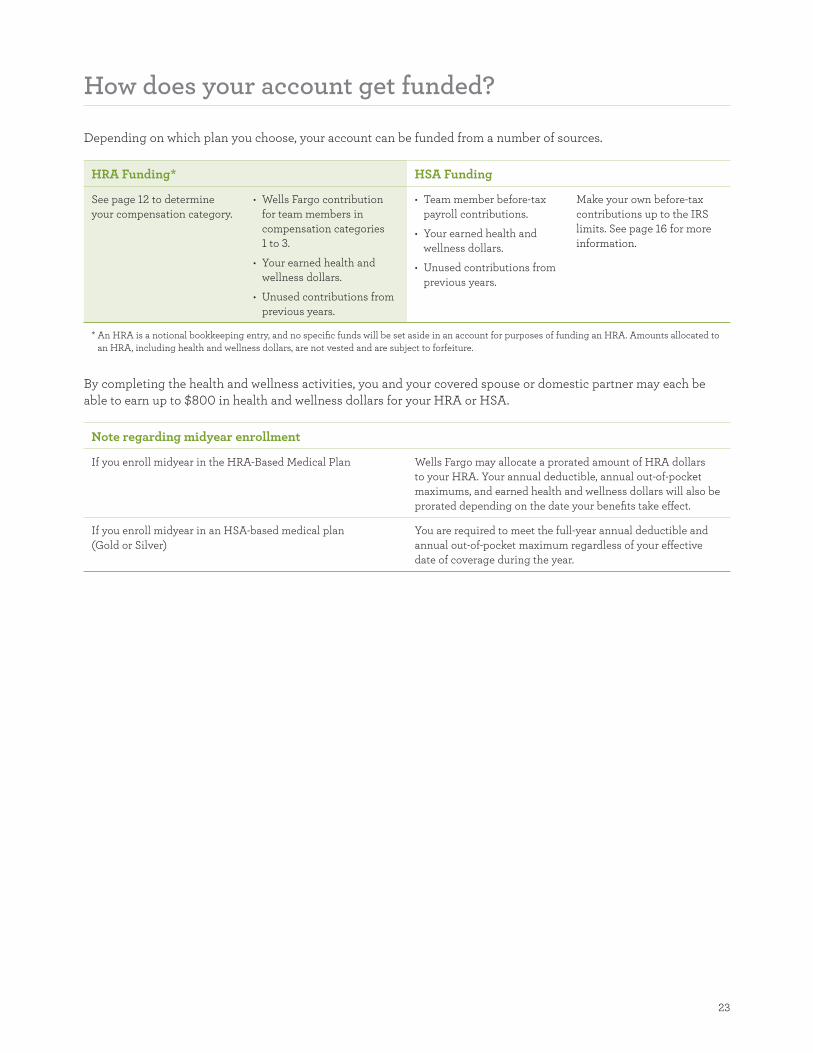
23
How does your account get funded
Depending on which plan you choose your account can be funded from a number of sources
HRA Funding HSA Funding
See page 12 to determine
your compensation category
bullensp Wells Fargo contribution
for team members in
compensation categories
1 to 3
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
bullensp Team member before-tax
payroll contributions
bullensp Your earned health and
wellness dollars
bullensp Unused contributions from
previous years
Make your own before-tax
contributions up to the IRS
limits See page 16 for more
information
An HRA is a notional bookkeeping entry and no specific funds will be set aside in an account for purposes of funding an HRA Amounts allocated to
an HRA including health and wellness dollars are not vested and are subject to forfeiture
By completing the health and wellness activities you and your covered spouse or domestic partner may each be
able to earn up to $800 in health and wellness dollars for your HRA or HSA
Note regarding midyear enrollment
If you enroll midyear in the HRA-Based Medical Plan Wells Fargo may allocate a prorated amount of HRA dollars
to your HRA Your annual deductible annual out-of-pocket
maximums and earned health and wellness dollars will also be
prorated depending on the date your benefits take effect
If you enroll midyear in an HSA-based medical plan
(Gold or Silver)
You are required to meet the full-year annual deductible and
annual out-of-pocket maximum regardless of your effective
date of coverage during the year
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
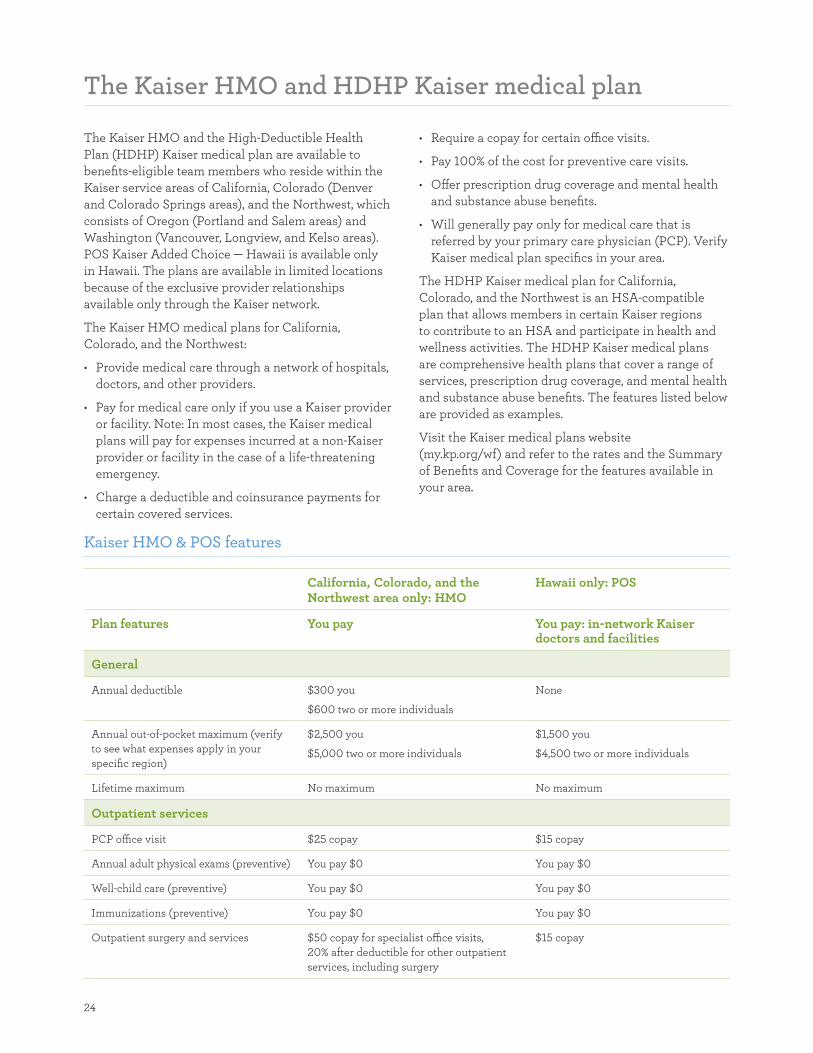
24
The Kaiser HMO and HDHP Kaiser medical plan
The Kaiser HMO and the High-Deductible Health
Plan (HDHP) Kaiser medical plan are available to
benefits-eligible team members who reside within the
Kaiser service areas of California Colorado (Denver
and Colorado Springs areas) and the Northwest which
consists of Oregon (Portland and Salem areas) and
Washington (Vancouver Longview and Kelso areas)
POS Kaiser Added Choice mdash Hawaii is available only
in Hawaii The plans are available in limited locations
because of the exclusive provider relationships
available only through the Kaiser network
The Kaiser HMO medical plans for California
Colorado and the Northwest
bull Provide medical care through a network of hospitals
doctors and other providers
bull Pay for medical care only if you use a Kaiser provider
or facility Note In most cases the Kaiser medical
plans will pay for expenses incurred at a non-Kaiser
provider or facility in the case of a life-threatening
emergency
bull Charge a deductible and coinsurance payments for
certain covered services
bull Require a copay for certain office visits
bull Pay 100 of the cost for preventive care visits
bull Offer prescription drug coverage and mental health
and substance abuse benefits
bull Will generally pay only for medical care that is
referred by your primary care physician (PCP) Verify
Kaiser medical plan specifics in your area
The HDHP Kaiser medical plan for California
Colorado and the Northwest is an HSA-compatible
plan that allows members in certain Kaiser regions
to contribute to an HSA and participate in health and
wellness activities The HDHP Kaiser medical plans
are comprehensive health plans that cover a range of
services prescription drug coverage and mental health
and substance abuse benefits The features listed below
are provided as examples
Visit the Kaiser medical plans website
(mykporgwf) and refer to the rates and the Summary
of Benefits and Coverage for the features available in
your area
Kaiser HMO amp POS features
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
General
Annual deductible $300 you
$600 two or more individuals
None
Annual out-of-pocket maximum (verify
to see what expenses apply in your
specific region)
$2500 you
$5000 two or more individuals
$1500 you
$4500 two or more individuals
Lifetime maximum No maximum No maximum
Outpatient services
PCP office visit $25 copay $15 copay
Annual adult physical exams (preventive) You pay $0 You pay $0
Well-child care (preventive) You pay $0 You pay $0
Immunizations (preventive) You pay $0 You pay $0
Outpatient surgery and services $50 copay for specialist office visits
20 after deductible for other outpatient
services including surgery
$15 copay
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
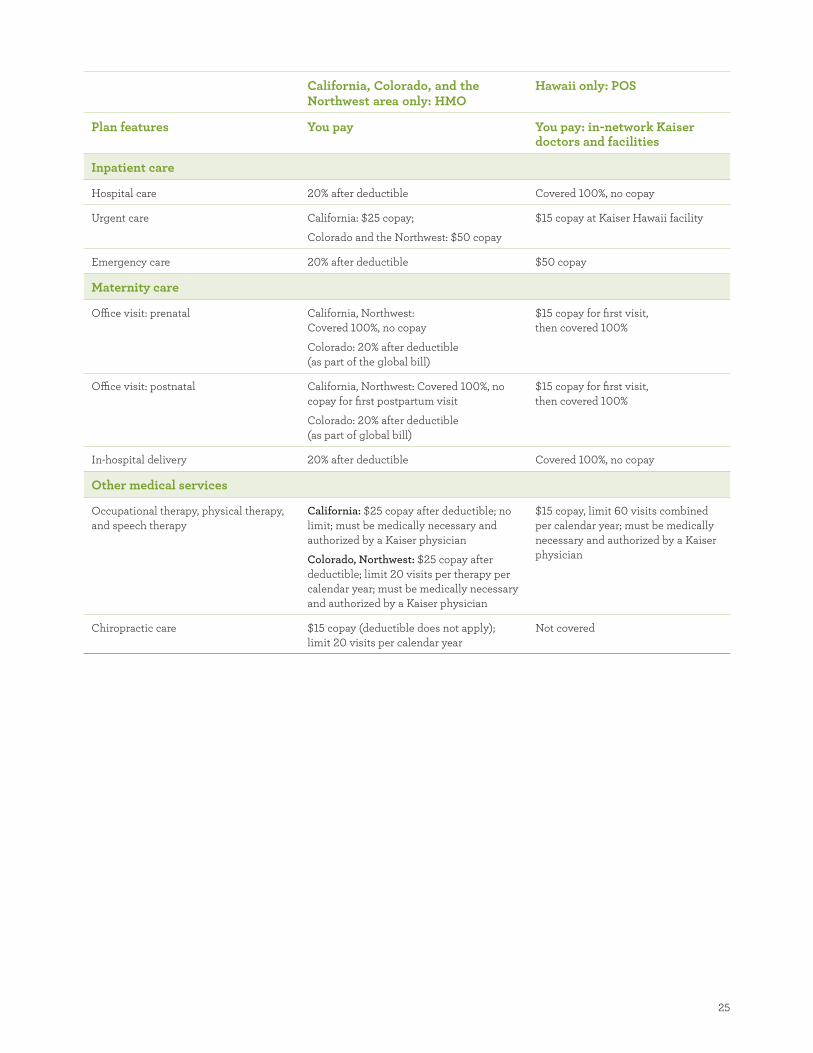
25
California Colorado and the Northwest area only HMO
Hawaii only POS
Plan features You pay You pay in-network Kaiser doctors and facilities
Inpatient care
Hospital care 20 after deductible Covered 100 no copay
Urgent care California $25 copay
Colorado and the Northwest $50 copay
$15 copay at Kaiser Hawaii facility
Emergency care 20 after deductible $50 copay
Maternity care
Office visit prenatal California Northwest
Covered 100 no copay
Colorado 20 after deductible
(as part of the global bill)
$15 copay for first visit
then covered 100
Office visit postnatal California Northwest Covered 100 no
copay for first postpartum visit
Colorado 20 after deductible
(as part of global bill)
$15 copay for first visit
then covered 100
In-hospital delivery 20 after deductible Covered 100 no copay
Other medical services
Occupational therapy physical therapy
and speech therapy
California $25 copay after deductible no
limit must be medically necessary and
authorized by a Kaiser physician
Colorado Northwest $25 copay after
deductible limit 20 visits per therapy per
calendar year must be medically necessary
and authorized by a Kaiser physician
$15 copay limit 60 visits combined
per calendar year must be medically
necessary and authorized by a Kaiser
physician
Chiropractic care $15 copay (deductible does not apply)
limit 20 visits per calendar year
Not covered
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
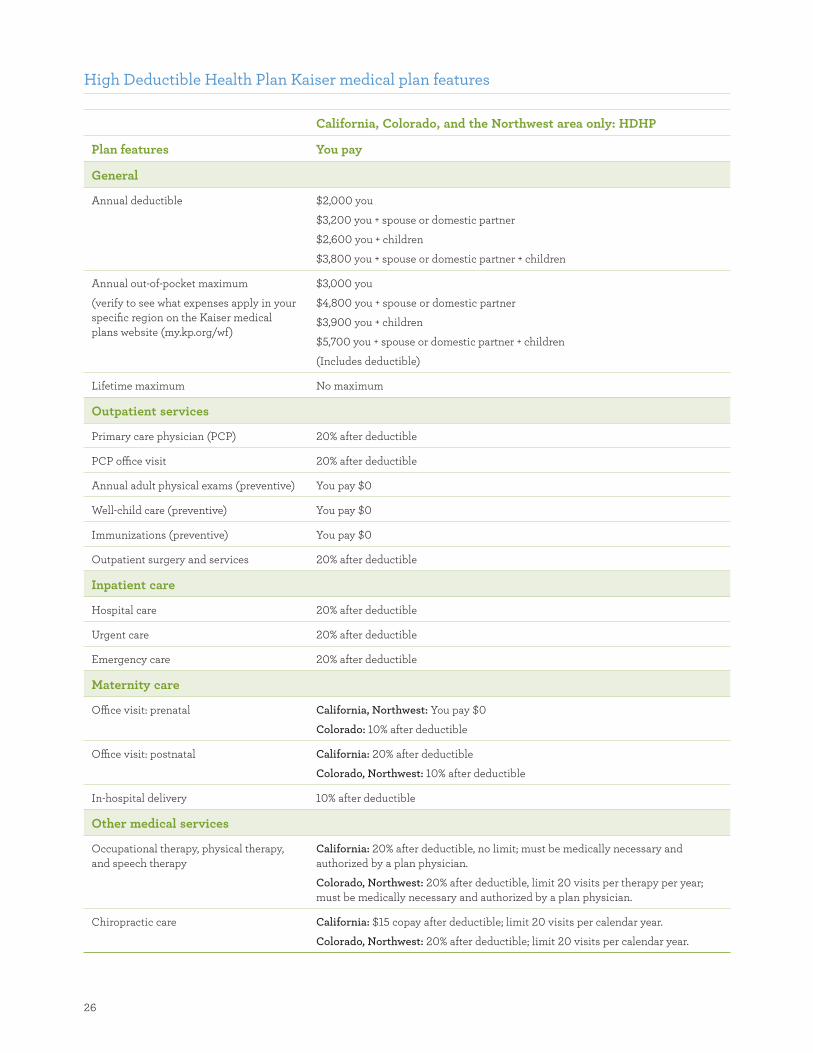
26
High Deductible Health Plan Kaiser medical plan features
California Colorado and the Northwest area only HDHP
Plan features You pay
General
Annual deductible $2000 you
$3200 you + spouse or domestic partner
$2600 you + children
$3800 you + spouse or domestic partner + children
Annual out-of-pocket maximum
(verify to see what expenses apply in your
specific region on the Kaiser medical
plans website (mykporgwf)
$3000 you
$4800 you + spouse or domestic partner
$3900 you + children
$5700 you + spouse or domestic partner + children
(Includes deductible)
Lifetime maximum No maximum
Outpatient services
Primary care physician (PCP) 20 after deductible
PCP office visit 20 after deductible
Annual adult physical exams (preventive) You pay $0
Well-child care (preventive) You pay $0
Immunizations (preventive) You pay $0
Outpatient surgery and services 20 after deductible
Inpatient care
Hospital care 20 after deductible
Urgent care 20 after deductible
Emergency care 20 after deductible
Maternity care
Office visit prenatal California Northwest You pay $0
Colorado 10 after deductible
Office visit postnatal California 20 after deductible
Colorado Northwest 10 after deductible
In-hospital delivery 10 after deductible
Other medical services
Occupational therapy physical therapy
and speech therapy
California 20 after deductible no limit must be medically necessary and
authorized by a plan physician
Colorado Northwest 20 after deductible limit 20 visits per therapy per year
must be medically necessary and authorized by a plan physician
Chiropractic care California $15 copay after deductible limit 20 visits per calendar year
Colorado Northwest 20 after deductible limit 20 visits per calendar year
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
27
Using a health savings account
The HDHP Kaiser medical plan is a comprehensive
medical plan that is compatible with a health savings
account designed to help you save money to pay for
future qualified medical dental vision and prescription
expenses You decide when to use your available HSA
balance to pay for eligible services
If you spend funds in your HSA on qualified medical
dental vision and prescription expenses mdash now in the
near future or in retirement mdash those funds generally
wonrsquot be subject to federal taxes
Use the money in your HSA to cover qualified medical
dental vision and prescription expenses or save it for
future health care expenses You own the dollars in your
account from day one and you never lose them so you
get to choose when to use them
Health and wellness dollars
With the HDHP Kaiser medical plan you are eligible
to earn health and wellness dollars for your HSA
by completing health and wellness activities and
educational programs Depending on the activities
completed you and your covered spouse or domestic
partner if he or she is also enrolled could each earn
up to $800 for your HSA If you enroll midyear the
amount of health and wellness dollars that you can
earn will be prorated
Note Only specified activities allow you to earn health
and wellness dollars for your account See page 17 for
more information about health and wellness activities
Save more with a flexible spending account
If you enroll in a Kaiser HMO or POS option or if you
waive Wells Fargo medical plan coverage you can
use before-tax dollars in a Full-Purpose Health Care
Flexible Spending Account (FSA) to pay for eligible
medical dental vision and prescription expenses that
are not reimbursed by another source
If you enroll in the HDHP Kaiser medical plan you
can use before-tax dollars in a Limited DentalVision
Flexible Spending Account (FSA) to pay for eligible
dental and vision expenses that are not reimbursed by
another source
For more information about FSAs see page 30
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
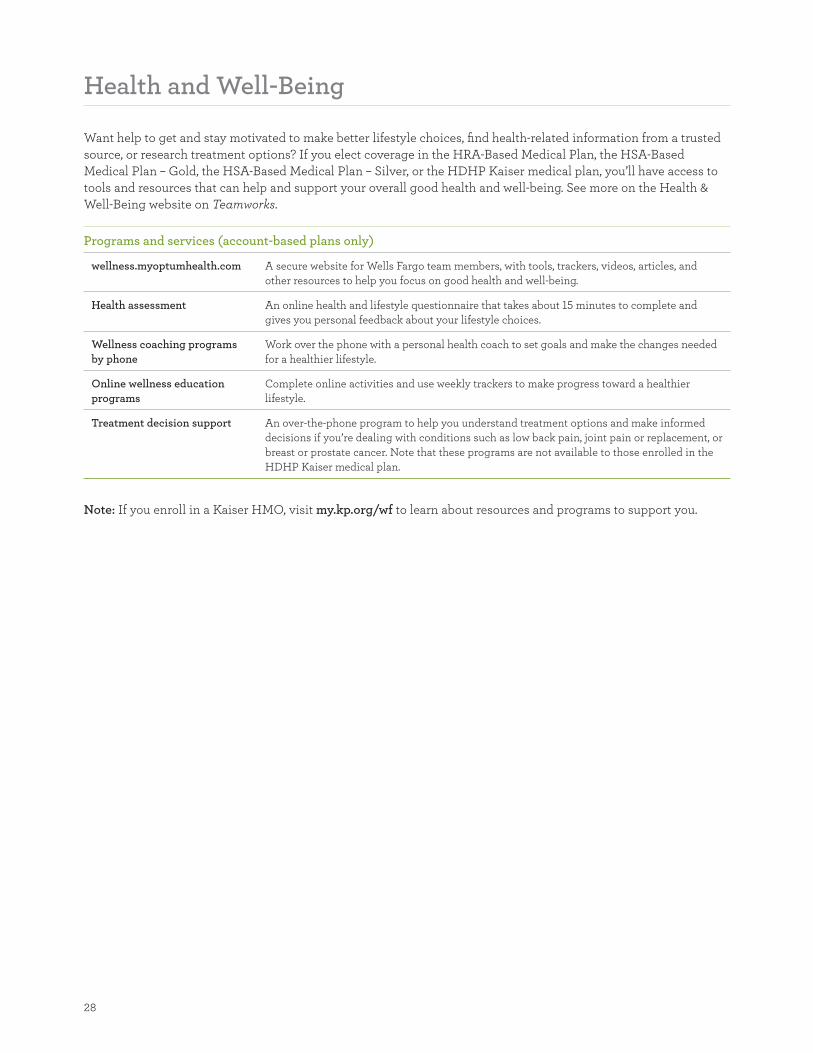
28
Health and Well-Being
Want help to get and stay motivated to make better lifestyle choices fi nd health-related information from a trusted
source or research treatment options If you elect coverage in the HRA-Based Medical Plan the HSA-Based
Medical Plan ndash Gold the HSA-Based Medical Plan ndash Silver or the HDHP Kaiser medical plan yoursquoll have access to
tools and resources that can help and support your overall good health and well-being See more on the Health amp
Well-Being website on Teamworks
Programs and services (account-based plans only)
wellnessmyoptumhealthcom A secure website for Wells Fargo team members with tools trackers videos articles and
other resources to help you focus on good health and well-being
Health assessment An online health and lifestyle questionnaire that takes about 15 minutes to complete and
gives you personal feedback about your lifestyle choices
Wellness coaching programs
by phone
Work over the phone with a personal health coach to set goals and make the changes needed
for a healthier lifestyle
Online wellness education
programs
Complete online activities and use weekly trackers to make progress toward a healthier
lifestyle
Treatment decision support An over-the-phone program to help you understand treatment options and make informed
decisions if yoursquore dealing with conditions such as low back pain joint pain or replacement or
breast or prostate cancer Note that these programs are not available to those enrolled in the
HDHP Kaiser medical plan
Note If you enroll in a Kaiser HMO visit mykporgwf to learn about resources and programs to support you
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
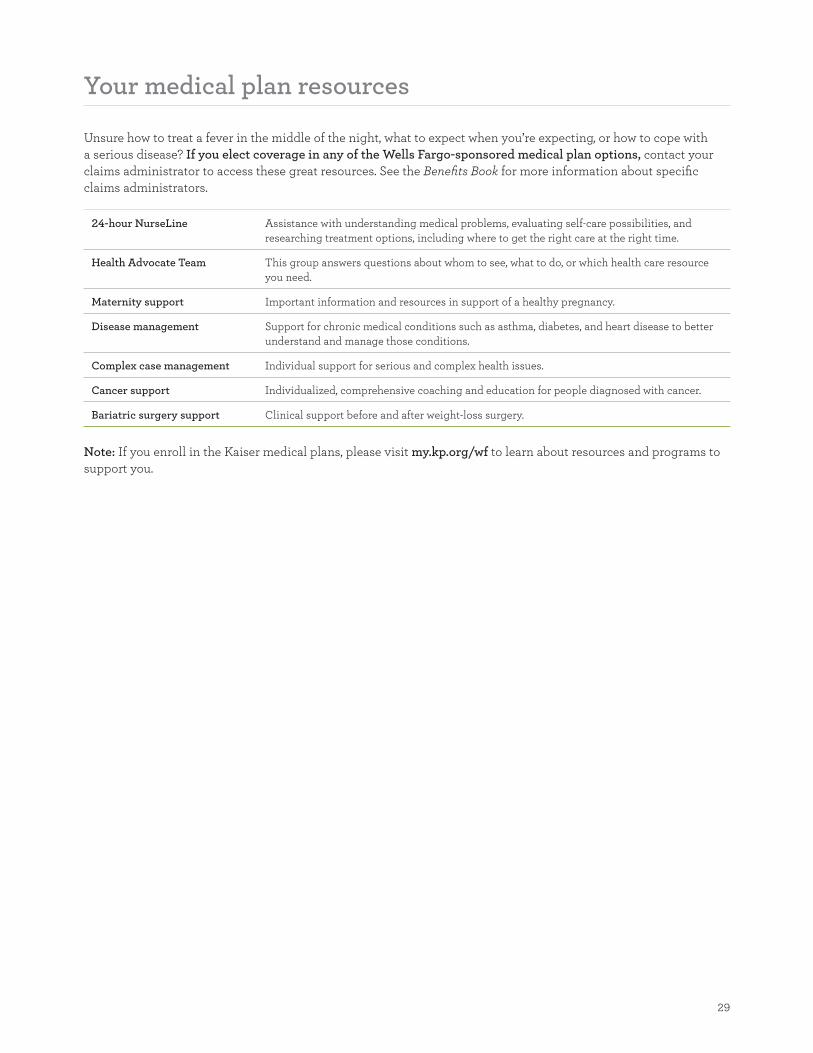
29
Your medical plan resources
Unsure how to treat a fever in the middle of the night what to expect when yoursquore expecting or how to cope with
a serious disease If you elect coverage in any of the Wells Fargo-sponsored medical plan options contact your
claims administrator to access these great resources See the Benefits Book for more information about specifi c
claims administrators
24-hour NurseLine Assistance with understanding medical problems evaluating self-care possibilities and
researching treatment options including where to get the right care at the right time
Health Advocate Team This group answers questions about whom to see what to do or which health care resource
you need
Maternity support Important information and resources in support of a healthy pregnancy
Disease management Support for chronic medical conditions such as asthma diabetes and heart disease to better
understand and manage those conditions
Complex case management Individual support for serious and complex health issues
Cancer support Individualized comprehensive coaching and education for people diagnosed with cancer
Bariatric surgery support Clinical support before and after weight-loss surgery
Note If you enroll in the Kaiser medical plans please visit mykporgwf to learn about resources and programs to
support you
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
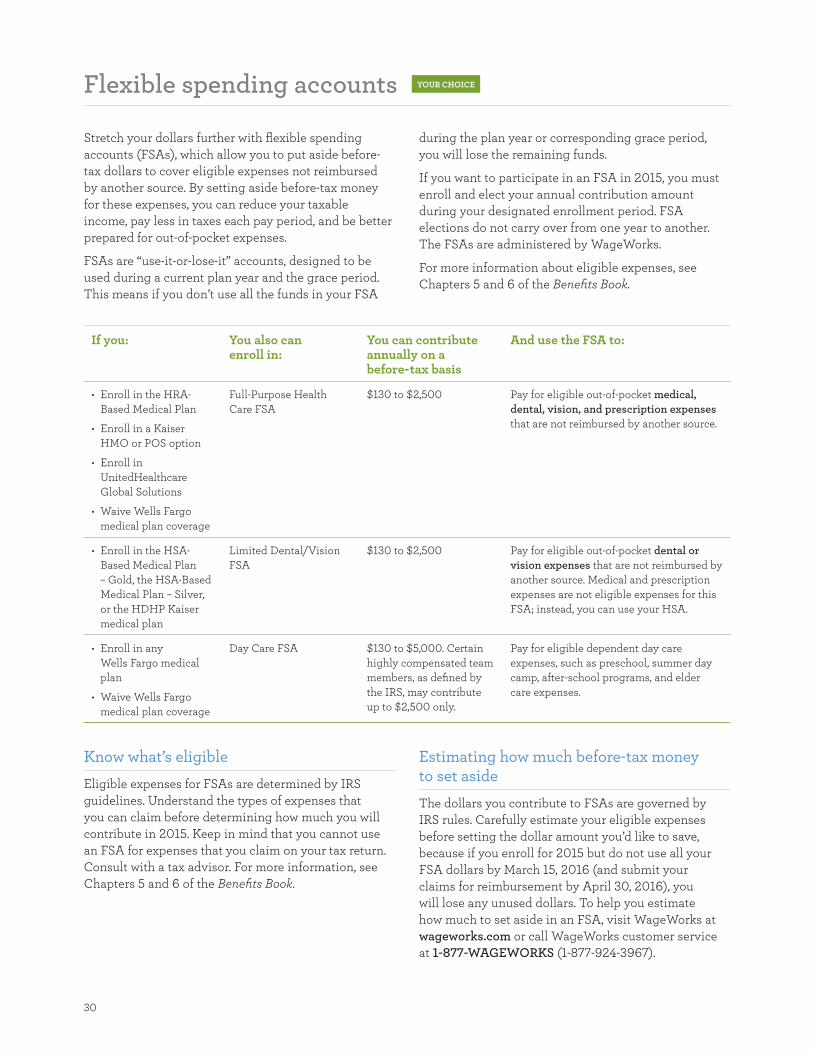
30
Flexible spending accounts YOUR CHOICE
Stretch your dollars further with flexible spending
accounts (FSAs) which allow you to put aside before-
tax dollars to cover eligible expenses not reimbursed
by another source By setting aside before-tax money
for these expenses you can reduce your taxable
income pay less in taxes each pay period and be better
prepared for out-of-pocket expenses
FSAs are ldquouse-it-or-lose-itrdquo accounts designed to be
used during a current plan year and the grace period
This means if you donrsquot use all the funds in your FSA
during the plan year or corresponding grace period
you will lose the remaining funds
If you want to participate in an FSA in 2015 you must
enroll and elect your annual contribution amount
during your designated enrollment period FSA
elections do not carry over from one year to another
The FSAs are administered by WageWorks
For more information about eligible expenses see
Chapters 5 and 6 of the Benefits Book
If you You also can enroll in
You can contribute annually on a before-tax basis
And use the FSA to
bullensp Enroll in the HRA-
Based Medical Plan
bullensp Enroll in a Kaiser
HMO or POS option
bullensp Enroll in
UnitedHealthcare
Global Solutions
bullensp Waive Wells Fargo
medical plan coverage
Full-Purpose Health
Care FSA
$130 to $2500 Pay for eligible out-of-pocket medical
dental vision and prescription expenses
that are not reimbursed by another source
bullensp Enroll in the HSA-
Based Medical Plan
ndash Gold the HSA-Based
Medical Plan ndash Silver
or the HDHP Kaiser
medical plan
Limited DentalVision
FSA
$130 to $2500 Pay for eligible out-of-pocket dental or
vision expenses that are not reimbursed by
another source Medical and prescription
expenses are not eligible expenses for this
FSA instead you can use your HSA
bullensp Enroll in any
Wells Fargo medical
plan
bullensp Waive Wells Fargo
medical plan coverage
Day Care FSA $130 to $5000 Certain
highly compensated team
members as defined by
the IRS may contribute
up to $2500 only
Pay for eligible dependent day care
expenses such as preschool summer day
camp after-school programs and elder
care expenses
Know whatrsquos eligible
Eligible expenses for FSAs are determined by IRS
guidelines Understand the types of expenses that
you can claim before determining how much you will
contribute in 2015 Keep in mind that you cannot use
an FSA for expenses that you claim on your tax return
Consult with a tax advisor For more information see
Chapters 5 and 6 of the Benefits Book
Estimating how much before-tax money to set aside
The dollars you contribute to FSAs are governed by
IRS rules Carefully estimate your eligible expenses
before setting the dollar amount yoursquod like to save
because if you enroll for 2015 but do not use all your
FSA dollars by March 15 2016 (and submit your
claims for reimbursement by April 30 2016) you
will lose any unused dollars To help you estimate
how much to set aside in an FSA visit WageWorks at
wageworkscom or call WageWorks customer service
at 1-877-WAGEWORKS (1-877-924-3967)
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
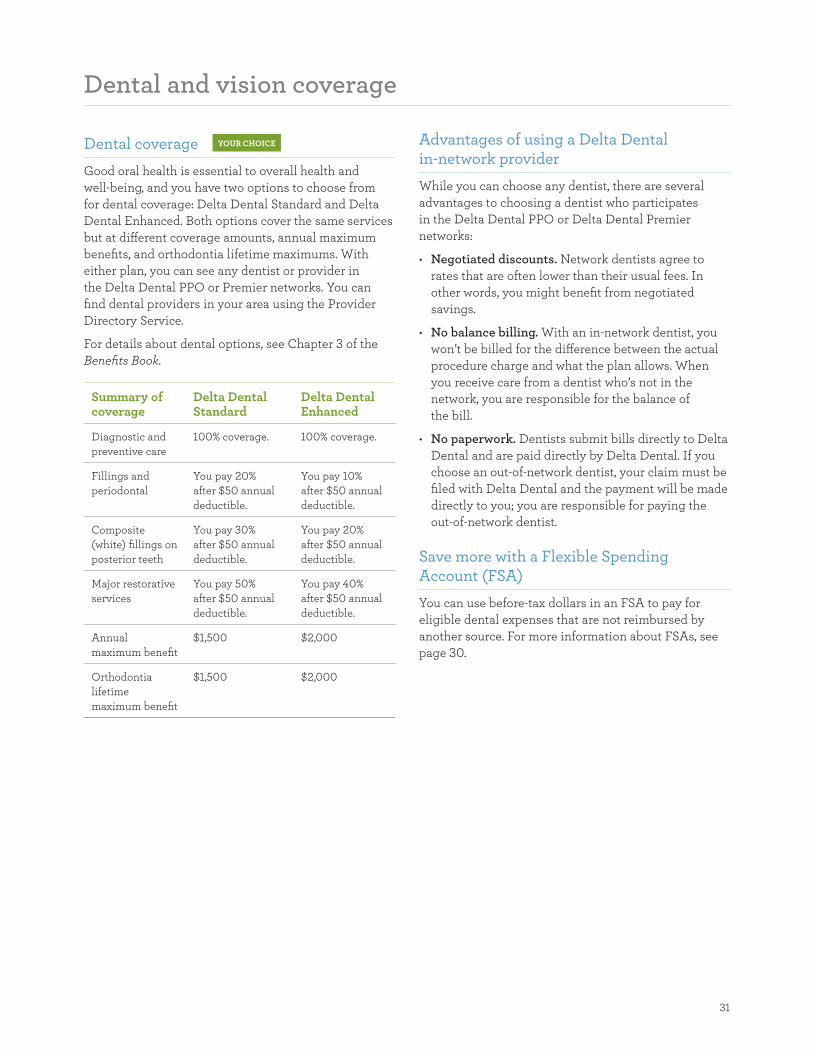
31
Dental and vision coverage
Dental coverage YOUR CHOICE
Good oral health is essential to overall health and
well-being and you have two options to choose from
for dental coverage Delta Dental Standard and Delta
Dental Enhanced Both options cover the same services
but at different coverage amounts annual maximum
benefits and orthodontia lifetime maximums With
either plan you can see any dentist or provider in
the Delta Dental PPO or Premier networks You can
find dental providers in your area using the Provider
Directory Service
For details about dental options see Chapter 3 of the
Benefits Book
Summary of coverage
Delta Dental Standard
Delta Dental Enhanced
Diagnostic and
preventive care
100 coverage 100 coverage
Fillings and
periodontal
You pay 20
after $50 annual
deductible
You pay 10
after $50 annual
deductible
Composite
(white) fillings on
posterior teeth
You pay 30
after $50 annual
deductible
You pay 20
after $50 annual
deductible
Major restorative
services
You pay 50
after $50 annual
deductible
You pay 40
after $50 annual
deductible
Annual
maximum benefit
$1500 $2000
Orthodontia
lifetime
maximum benefit
$1500 $2000
Advantages of using a Delta Dental in-network provider
While you can choose any dentist there are several
advantages to choosing a dentist who participates
in the Delta Dental PPO or Delta Dental Premier
networks
bull Negotiated discounts Network dentists agree to
rates that are often lower than their usual fees In
other words you might benefit from negotiated
savings
bull No balance billing With an in-network dentist you
wonrsquot be billed for the difference between the actual
procedure charge and what the plan allows When
you receive care from a dentist whorsquos not in the
network you are responsible for the balance of
the bill
bull No paperwork Dentists submit bills directly to Delta
Dental and are paid directly by Delta Dental If you
choose an out-of-network dentist your claim must be
fi led with Delta Dental and the payment will be made
directly to you you are responsible for paying the
out-of-network dentist
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in an FSA to pay for
eligible dental expenses that are not reimbursed by
another source For more information about FSAs see
page 30
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
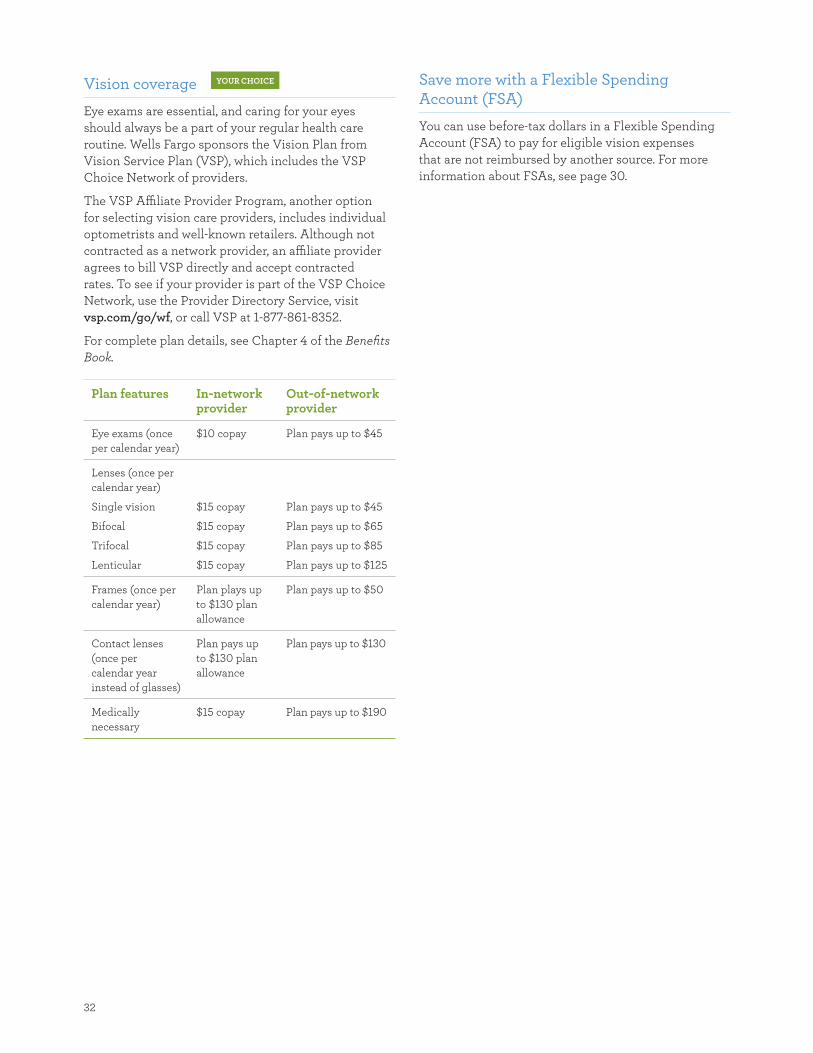
32
Vision coverage YOUR CHOICE
Eye exams are essential and caring for your eyes
should always be a part of your regular health care
routine Wells Fargo sponsors the Vision Plan from
Vision Service Plan (VSP) which includes the VSP
Choice Network of providers
The VSP Affiliate Provider Program another option
for selecting vision care providers includes individual
optometrists and well-known retailers Although not
contracted as a network provider an affiliate provider
agrees to bill VSP directly and accept contracted
rates To see if your provider is part of the VSP Choice
Network use the Provider Directory Service visit
vspcomgowf or call VSP at 1-877-861-8352
For complete plan details see Chapter 4 of the Benefits
Book
Plan features In-network provider
Out-of-network provider
Eye exams (once
per calendar year)
$10 copay Plan pays up to $45
Lenses (once per
calendar year)
Single vision $15 copay Plan pays up to $45
Bifocal $15 copay Plan pays up to $65
Trifocal $15 copay Plan pays up to $85
Lenticular $15 copay Plan pays up to $125
Frames (once per
calendar year)
Plan plays up
to $130 plan
allowance
Plan pays up to $50
Contact lenses
(once per
calendar year
instead of glasses)
Plan pays up
to $130 plan
allowance
Plan pays up to $130
Medically
necessary
$15 copay Plan pays up to $190
Save more with a Flexible Spending Account (FSA)
You can use before-tax dollars in a Flexible Spending
Account (FSA) to pay for eligible vision expenses
that are not reimbursed by another source For more
information about FSAs see page 30
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
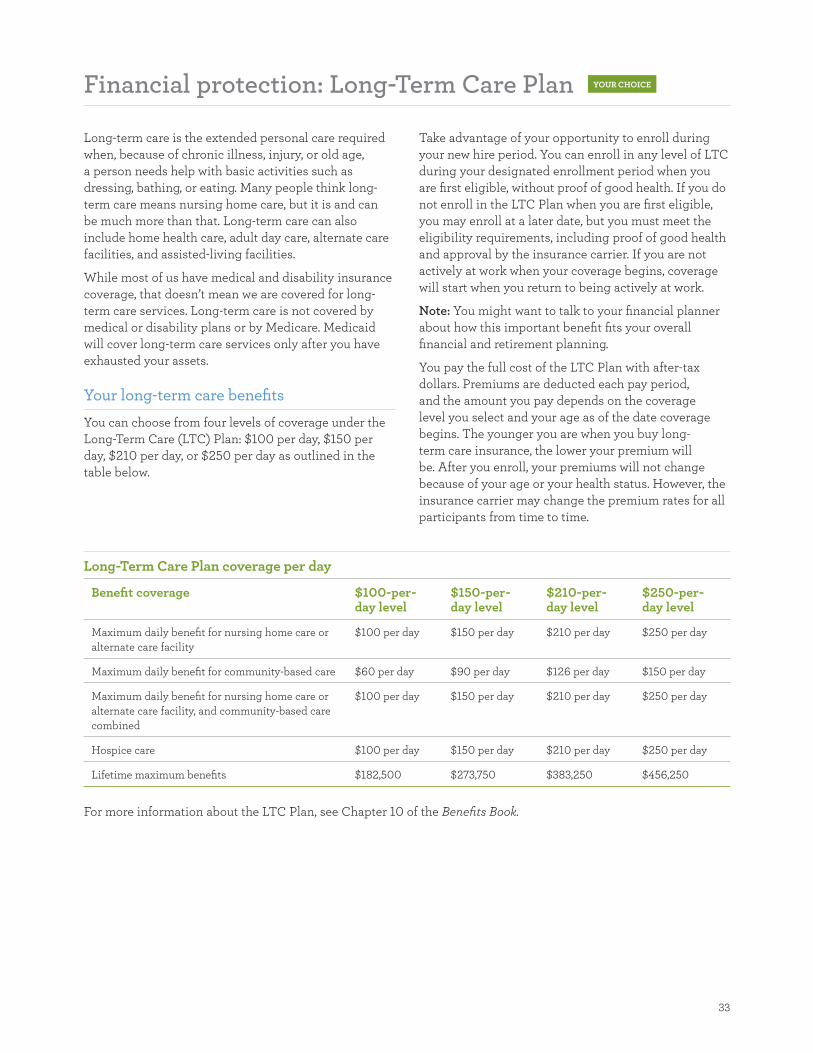
33
Financial protection Long-Term Care Plan YOUR CHOICE
Long-term care is the extended personal care required
when because of chronic illness injury or old age
a person needs help with basic activities such as
dressing bathing or eating Many people think long-
term care means nursing home care but it is and can
be much more than that Long-term care can also
include home health care adult day care alternate care
facilities and assisted-living facilities
While most of us have medical and disability insurance
coverage that doesnrsquot mean we are covered for long-
term care services Long-term care is not covered by
medical or disability plans or by Medicare Medicaid
will cover long-term care services only after you have
exhausted your assets
Your long-term care benefits
You can choose from four levels of coverage under the
Long-Term Care (LTC) Plan $100 per day $150 per
day $210 per day or $250 per day as outlined in the
table below
Take advantage of your opportunity to enroll during
your new hire period You can enroll in any level of LTC
during your designated enrollment period when you
are first eligible without proof of good health If you do
not enroll in the LTC Plan when you are first eligible
you may enroll at a later date but you must meet the
eligibility requirements including proof of good health
and approval by the insurance carrier If you are not
actively at work when your coverage begins coverage
will start when you return to being actively at work
Note You might want to talk to your financial planner
about how this important benefit fits your overall
financial and retirement planning
You pay the full cost of the LTC Plan with after-tax
dollars Premiums are deducted each pay period
and the amount you pay depends on the coverage
level you select and your age as of the date coverage
begins The younger you are when you buy long-
term care insurance the lower your premium will
be After you enroll your premiums will not change
because of your age or your health status However the
insurance carrier may change the premium rates for all
participants from time to time
Long-Term Care Plan coverage per day
Benefi t coverage $100-per-day level
$150-per-day level
$210-per-day level
$250-per-day level
Maximum daily benefit for nursing home care or
alternate care facility
$100 per day $150 per day $210 per day $250 per day
Maximum daily benefit for community-based care $60 per day $90 per day $126 per day $150 per day
Maximum daily benefit for nursing home care or
alternate care facility and community-based care
combined
$100 per day $150 per day $210 per day $250 per day
Hospice care $100 per day $150 per day $210 per day $250 per day
Lifetime maximum benefi ts $182500 $273750 $383250 $456250
For more information about the LTC Plan see Chapter 10 of the Benefits Book
34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

34
Return of premium benefit and portability
If you die before age 75 while covered by the LTC Plan
your designated beneficiary may receive a refund of
some or all of the premiums paid up to the date of
death The amount will be reduced by any plan benefits
that you have been paid or are payable at the time of
death You can designate only one primary beneficiary
for the LTC Plan
If you enroll in the benefit remember to designate a
beneficiary
In addition the LTC Plan is portable If you leave
Wells Fargo and wish to continue coverage you may do
so at the same rate directly with the insurance carrier
Coverage for eligible dependents
Your spouse or domestic partner parents or the
parents of your spouse or domestic partner may apply
for individual long-term care coverage at the group rate
by contacting CNA at 1-800-932-1132 Proof of good
health is required before they can purchase coverage
CNA will provide the necessary application forms and
will bill them directly after they enroll
A Proof of Good Health form for your spouse or
domestic partner is available on Teamworks and
Teamworks at Home (teamworkswellsfargocom)
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
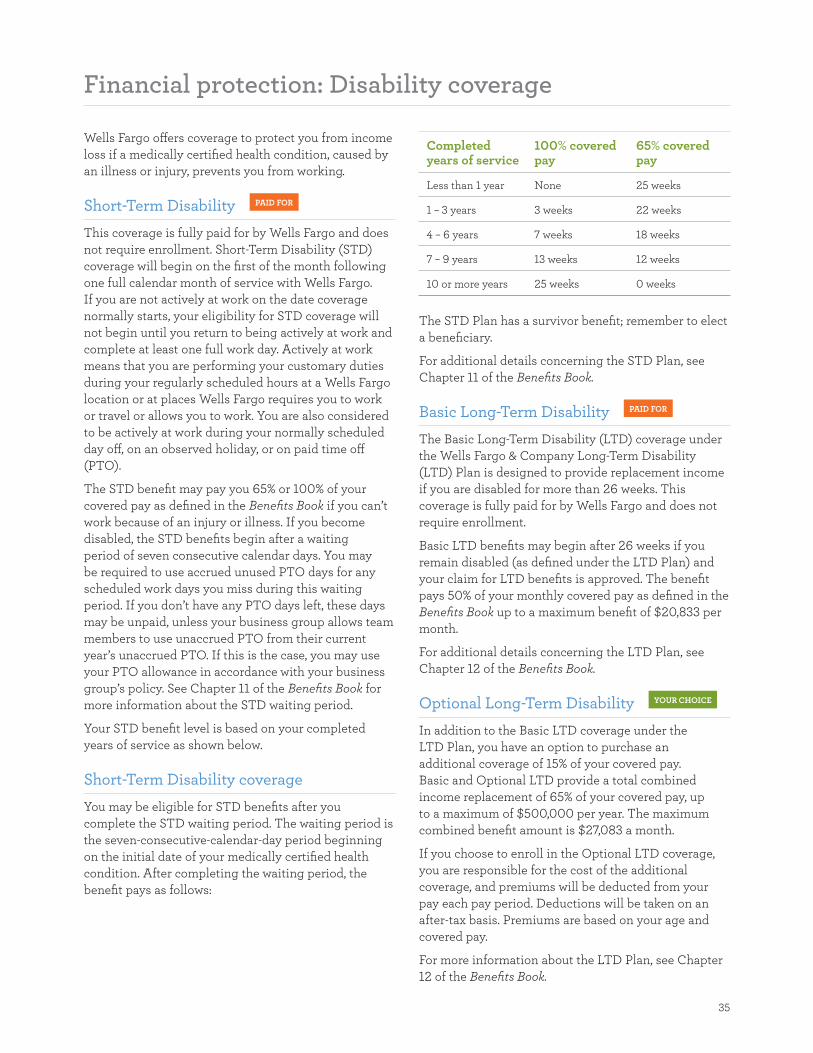
35
Financial protection Disability coverage
Wells Fargo offers coverage to protect you from income
loss if a medically certified health condition caused by
an illness or injury prevents you from working
Short-Term Disability PAID FOR
This coverage is fully paid for by Wells Fargo and does
not require enrollment Short-Term Disability (STD)
coverage will begin on the first of the month following
one full calendar month of service with Wells Fargo
If you are not actively at work on the date coverage
normally starts your eligibility for STD coverage will
not begin until you return to being actively at work and
complete at least one full work day Actively at work
means that you are performing your customary duties
during your regularly scheduled hours at a Wells Fargo
location or at places Wells Fargo requires you to work
or travel or allows you to work You are also considered
to be actively at work during your normally scheduled
day off on an observed holiday or on paid time off
(PTO)
The STD benefit may pay you 65 or 100 of your
covered pay as defined in the Benefits Book if you canrsquot
work because of an injury or illness If you become
disabled the STD benefits begin after a waiting
period of seven consecutive calendar days You may
be required to use accrued unused PTO days for any
scheduled work days you miss during this waiting
period If you donrsquot have any PTO days left these days
may be unpaid unless your business group allows team
members to use unaccrued PTO from their current
yearrsquos unaccrued PTO If this is the case you may use
your PTO allowance in accordance with your business
grouprsquos policy See Chapter 11 of the Benefits Book for
more information about the STD waiting period
Your STD benefi t level is based on your completed
years of service as shown below
Short-Term Disability coverage
You may be eligible for STD benefits after you
complete the STD waiting period The waiting period is
the seven-consecutive-calendar-day period beginning
on the initial date of your medically certified health
condition After completing the waiting period the
benefit pays as follows
Completed years of service
100 covered pay
65 covered pay
Less than 1 year None 25 weeks
1 ndash 3 years 3 weeks 22 weeks
4 ndash 6 years 7 weeks 18 weeks
7 ndash 9 years 13 weeks 12 weeks
10 or more years 25 weeks 0 weeks
The STD Plan has a survivor benefit remember to elect
a beneficiary
For additional details concerning the STD Plan see
Chapter 11 of the Benefits Book
Basic Long-Term Disability PAID FOR
The Basic Long-Term Disability (LTD) coverage under
the Wells Fargo amp Company Long-Term Disability
(LTD) Plan is designed to provide replacement income
if you are disabled for more than 26 weeks This
coverage is fully paid for by Wells Fargo and does not
require enrollment
Basic LTD benefits may begin after 26 weeks if you
remain disabled (as defined under the LTD Plan) and
your claim for LTD benefits is approved The benefit
pays 50 of your monthly covered pay as defined in the
Benefits Book up to a maximum benefit of $20833 per
month
For additional details concerning the LTD Plan see
Chapter 12 of the Benefits Book
Optional Long-Term Disability YOUR CHOICE
In addition to the Basic LTD coverage under the
LTD Plan you have an option to purchase an
additional coverage of 15 of your covered pay
Basic and Optional LTD provide a total combined
income replacement of 65 of your covered pay up
to a maximum of $500000 per year The maximum
combined benefit amount is $27083 a month
If you choose to enroll in the Optional LTD coverage
you are responsible for the cost of the additional
coverage and premiums will be deducted from your
pay each pay period Deductions will be taken on an
after-tax basis Premiums are based on your age and
covered pay
For more information about the LTD Plan see Chapter
12 of the Benefits Book
36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

36
Preexisting condition
The LTD Plan does not pay benefits for a disability
that contributed to was caused by or resulted from a
preexisting condition You have a preexisting condition
if you meet the following
bull You received medical treatment consultation care
or services took prescription medications or had
medications prescribed during the three months just
before your effective date of coverage
bull The disability begins in the first 12 months after your
effective date of coverage and you have been treated
for the disability during the three months before the
eff ective date However even though your condition
meets the definition of a preexisting condition under
the LTD Plan you might be eligible for LTD benefi ts
if you were previously covered under the LTD Plan
of a company acquired by Wells Fargo (a ldquoprior LTD
planrdquo)
For more information about the pre-existing limitation
see Chapter 12 of the Benefits Book
37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

37
Financial protection Life insurance coverage
Wells Fargo provides several types of term life
insurance coverage to help give you peace of mind and
protect your family fi nancially if something were to
happen to you or to a covered dependent
Basic Term Life Plan PAID FOR
Wells Fargo provides all eligible team members
with the Basic Term Life Plan You are automatically
enrolled for this benefi t The Basic Term Life Plan
provides benefits to your beneficiary if you die The
amount of the benefit is one time your annual covered
pay as defined in the Benefits Book with a coverage
minimum amount of $10000 and a maximum of
$50000
Remember to elect a beneficiary for the Basic Term Life
Plan For additional details concerning Basic Term Life
insurance benefits and coverage under the Wells Fargo
amp Company Life Insurance Plan see Chapter 7 of the
Benefits Book for more information
Optional Term Life Plan YOUR CHOICE
The Optional Term Life Plan allows you to choose
additional life insurance coverage You can choose from
one to eight times your annual covered pay as defined
in Chapter 7 of the Benefits Book for your coverage
level up to a maximum of $3000000 subject to plan
provisions
Take advantage of your opportunity to enroll You
can enroll for one to four times your annual covered
pay as defined in the Benefits Book during your
designated enrollment period without proof of good
health Enrollment for fi ve to eight times your annual
covered pay as defined in Chapter 7 of the Benefits
Book requires proof of good health and is subject to
approval by the insurance carrier If you are not actively
at work on the day coverage begins Optional Term Life
coverage will begin when you are actively at work
Important You can sign up for the Optional Term Life
Plan at a later date but you must meet the eligibility
requirements including proof of good health and
approval by the insurance carrier unless you have
a Qualified Event such as birth of a child adoption
or placement for adoption of a child marriage or
creation of a domestic partnership death of a spouse
legal separation divorce or dissolution of a domestic
partnership
If you enroll in the Optional Term Life Insurance Plan
remember to elect a beneficiary
SpousePartner Optional Term Life Plan YOUR CHOICE
You can enroll in the SpousePartner Optional Term
Life Plan to provide financial protection if your spouse
or domestic partner dies You can enroll for benefits in
$25000 increments up to a total coverage of $250000
during your designated enrollment period subject to
plan provisions Important Enrollment at the $25000
level does not require proof of good health during your
designated enrollment period To enroll in this optional
plan you cannot be legally separated or divorced from
your spouse Enrollment in coverage amounts greater
than $25000 during your designated enrollment
period requires your spouse or domestic partner to
provide proof of good health and is subject to approval
by the insurance carrier
You are automatically the beneficiary for your Spouse
Partner Optional Term Life Plan
Optional Term Life premiums and nicotine use status
Premiums for the Optional Term Life Plan and the
SpousePartner Optional Term Life Plan are based
on the level of coverage you select and the insured
personrsquos age and nicotine use status You or your
spouse or domestic partner are considered a nicotine
user if you used tobacco andor nicotine in any form
including cigarettes electronic cigarettes cigars pipes
chewing tobacco nicotine gum or nicotine patches in
the 12 months before enrollment
For more information about the Optional Term Life
Plan under the Wells Fargo amp Company Life Insurance
Plan see Chapter 7 of the Benefits Book for more
information
Dependent Term Life YOUR CHOICE
You can also enroll in the Dependent Term Life Plan
during your designated enrollment period to help ease
the burden if your child (or children) dies Enrollment
in the Dependent Term Life Plan automatically covers
all of your eligible dependents and any future newly
eligible dependents Important Take advantage of
your opportunity to enroll If you enroll during your
designated enrollment period you do not need to
submit a proof of good health form You do not need
to enroll each individual dependent Your dependentrsquos
eligibility will be verified at the time the claim is fi led
and the claim will be denied if your dependent is
38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

38
ineligible The coverage amount is $20000 per eligible
covered dependent
Make sure your child (or children) is eligible See
Chapter 1 of the Benefits Book for complete dependent
eligibility requirements
Note See the section titled If You Have Eligible
Dependents on page 6 for details on certification for
newly enrolled dependents
You are automatically the beneficiary of the Dependent
Term Life Plan
For more information about the Dependent Term Life
Plan see Chapter 7 of the Benefits Book
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
39
Financial protection Business Travel Accident and
Accidental Death and Dismemberment
Wells Fargo also offers two plans that provide insurance
coverage if you are in a covered accident and die
become paralyzed or suffer the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while eligible under the plans
Business Travel Accident Plan PAID FOR
All eligible regular and part-time team members are
automatically enrolled in the Business Travel Accident
(BTA) Plan You become eligible as soon as you begin
working for Wells Fargo You are covered while you are
traveling on Wells Fargo business
You are automatically covered in this plan Remember
to elect a beneficiary
For more information about the BTA Plan see Chapter
8 of the Benefits Book
Accidental Death and Dismemberment Plan YOUR CHOICE
The Accidental Death and Dismemberment (ADampD)
Plan is an optional plan that helps provide fi nancial
protection for you or your family if you or a covered
family member are in a covered accident and die
become paralyzed or suff er the loss of a limb speech
hearing or sight or if a coma commences within 365
days of the date of a covered accident that occurred
while you were covered under the ADampD Plan You
pay the full cost for coverage through after-tax payroll
deductions if you enroll in the ADampD Plan If you are
not actively at work on the day coverage begins your
ADampD coverage will begin when you are actively at
work
If you enroll in the ADampD plan remember to elect a
benefi ciary
For more information about the ADampD Plan see
Chapter 9 of the Benefi ts Book
Business Travel Accident Plan and Accidental Death and Dismemberment Plan benefi ts
Your BTA Plan benefi t is fi ve times your covered pay
as defi ned in Chapter 8 of the Benefi ts Book up to a
maximum of $2000000
For the ADampD Plan you can enroll in individual or
family coverage based on the following individual
coverage levels $75000 $150000 $300000 and
$600000 If you elect family coverage the spouse
benefi t (the amount you get if your spouse dies) is
50 of your elected coverage amount (not to exceed
$300000) and your child benefi t is 15 of that amount
(not to exceed $45000)
For more information about benefi ts and coverage
under the BTA Plan or the ADampD Plan see Chapters 8
and 9 of the Benefi ts Book
40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

40
Naming a beneficiary
A beneficiary is the person persons trust charitable
institution or estate that you choose to receive benefi ts if
you die At any time you can designate your benefi ciary
(or beneficiaries) for these plans using the Your Benefi ts
tool in Teamworks for the following plans
bull Company-paid plans Basic Term Life BTA and
Short-Term Disability
bull Voluntary plans Optional Term Life ADampD and LTC
For SpousePartner Optional Term Life and Dependent
Term Life you are automatically the designated
benefi ciary of your spouse or domestic partner and
dependent
Default beneficiary
If you do not designate a beneficiary or if the
designated beneficiary dies before you do and no
contingent beneficiary is named the benefit is paid
after death in the following order
1 Your surviving spouse or domestic partner
2 Equally among your surviving biological and
adopted children
3 Equally between your surviving parents
4 Equally among your surviving brothers and sisters
5 Your estate
If you are not the biological or adoptive parent of your
spousersquos or domestic partnerrsquos child but would like that
child to receive benefits in the event of your death you
must properly designate the child as your beneficiary
Your estate is the default beneficiary for the Long-Term
Care Plan
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
41
Financial protection Legal Services Plan YOUR CHOICE
Through the Legal Services Plan insured by
ARAGreg you can receive professional legal advice
representation and assistance for personal legal
matters During your designated enrollment period
you can enroll in individual or family coverage
ARAG manages a nationwide network of attorneys to
provide you with professional legal assistance As a
Legal Services Plan member yoursquore guaranteed access
to a Network Attorney within 30 miles of your home If
a Network Attorney is not available in your area ARAG
will provide you with a non-Network Attorney who will
provide you with in-network benefi ts
Network Attorney fees for the services provided are
100 paid in full unless otherwise stated in Chapter 14
in the Benefi ts Book
Visit the ARAG Legal Center at ARAGLegalCentercom
If you have questions contact the ARAG Customer
Care Center at 1-800-299-2345
Representation available through the Legal Services Plan
Legal advice available by telephone
Tools and resources accessible online
bullensp Consumer protection Contract
disputes or warranty issues
bullensp Court adoption proceedings contested
and uncontested
bullensp Divorce Contested and uncontested
(up to 20 hours is paid in full)
bullensp IRS audit protection and collection
defense
bullensp Juvenile court proceedings
bullensp Legal name change
bullensp Personal property protection
bullensp Property transfer
bullensp Real estate
bullensp Renterrsquos rights
bullensp Will preparation and estate planning
bullensp Document preparation and review
bullensp Follow-up calls and letters
bullensp General legal advice
bullensp Small claims assistance
bullensp Attorney Finder
bullensp DIYtrade Do-it-yourself legal documents
bullensp Education Center Access to
guidebooks and videos a law guide
the LawExpressoreg e-newsletter
Personal Information Organizer
and other educational resources that
off er tips and tools for dealing with
everyday legal issues
42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

42
Other benefits Commuter Benefi t Program YOUR CHOICE
The Wells Fargo Commuter Benefit Program provides
tax savings to team members who commute by
qualified mass transit or pay to park Off ered through
WageWorks the program lets you pay for parking and
transit on a before-tax basis
You can
bull Purchase your transit pass online or by telephone
and have the pass delivered directly to your home
bull Pay your transit provider by using a WageWorks
Commuter Card
bull Elect to have your parking vendor paid directly
bull Pay your parking vendor by using a WageWorks
Parking Card
bull Designate the amount you will pay for daily parking
and get reimbursed after you submit a claim with
WageWorks
The amount you elect for these services will be
deducted from your paycheck on a before-tax basis up
to IRS limits (and on an after-tax basis thereafter)
Itrsquos not necessary to wait until your benefits-effective
date to enroll in the Commuter Benefit Program
However only active team members who are
commuting are able to participate
Unlike the flexible spending accounts you can enroll
change or cancel participation at any time during
the year subject to the monthly enrollment and
disenrollment date requirements To begin using
services for commuter expenses in the following
month generally you must enroll by the 10th of the
current month Some transit agencies might impose
an earlier deadline Go to wageworkscom to see if the
transit agency in your area is one of them
You cannot elect this benefit using the Your Benefi ts
tool To elect this benefit you can enroll any time
directly with WageWorks
To enroll
bull Go to Teamworks and enter ldquocommuter benefitrdquo in
the Search field
bull On the Commuter Benefit page click the
WageWorks Sign-On button
You can also call WageWorks at 1-877-WAGEWORKS
(1-877-924-3967) Additional information regarding
the Wells Fargo Commuter Benefit Program is available
on Teamworks
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
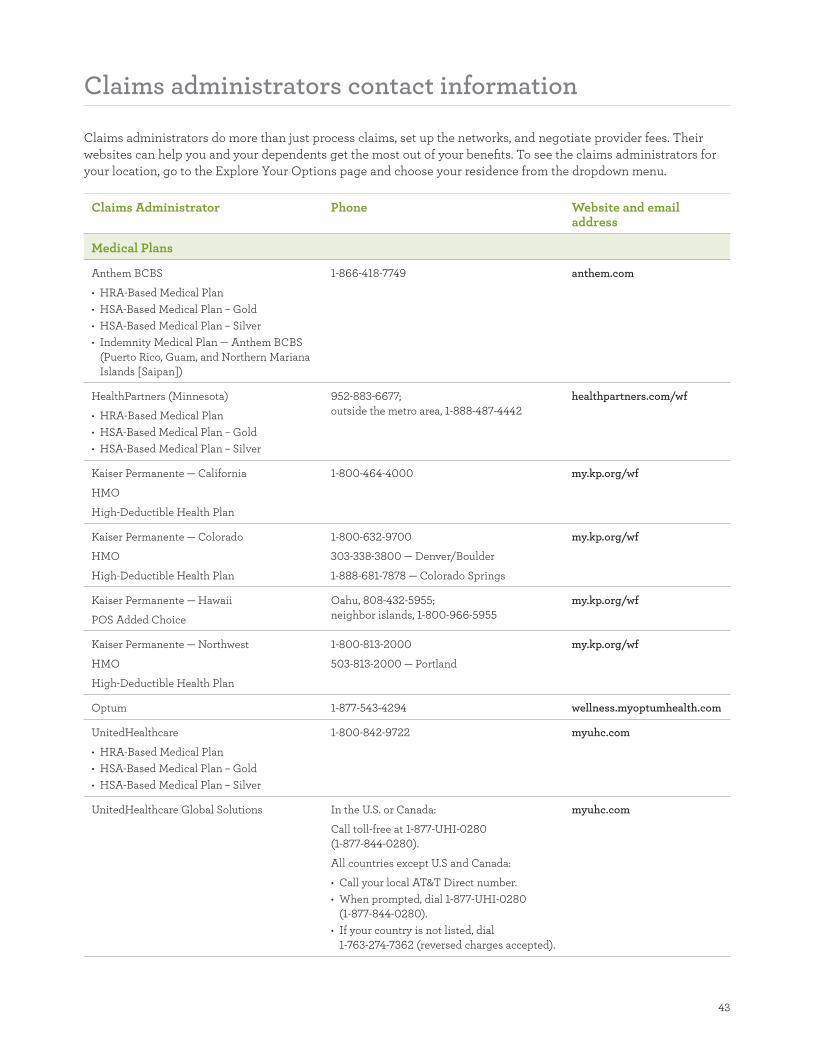
43
Claims administrators contact information
Claims administrators do more than just process claims set up the networks and negotiate provider fees Their
websites can help you and your dependents get the most out of your benefits To see the claims administrators for
your location go to the Explore Your Options page and choose your residence from the dropdown menu
Claims Administrator Phone Website and email address
Medical Plans
Anthem BCBS
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
bull Indemnity Medical Plan mdash Anthem BCBS
(Puerto Rico Guam and Northern Mariana
Islands [Saipan])
1-866-418-7749 anthemcom
HealthPartners (Minnesota)
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
952-883-6677
outside the metro area 1-888-487-4442
healthpartners comwf
Kaiser Permanente mdash California
HMO
High-Deductible Health Plan
1-800-464-4000 mykporgwf
Kaiser Permanente mdash Colorado
HMO
High-Deductible Health Plan
1-800-632-9700
303-338-3800 mdash DenverBoulder
1-888-681-7878 mdash Colorado Springs
mykporgwf
Kaiser Permanente mdash Hawaii
POS Added Choice
Oahu 808-432-5955
neighbor islands 1-800-966-5955
mykporgwf
Kaiser Permanente mdash Northwest
HMO
High-Deductible Health Plan
1-800-813-2000
503-813-2000 mdash Portland
mykporgwf
Optum 1-877-543-4294 wellnessmyoptumhealth com
UnitedHealthcare
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Gold
bull HSA-Based Medical Plan ndash Silver
1-800-842-9722 myuhc com
UnitedHealthcare Global Solutions In the US or Canada
Call toll-free at 1-877-UHI-0280
(1-877-844-0280)
All countries except US and Canada
bull Call your local ATampT Direct number
bull When prompted dial 1-877-UHI-0280
(1-877-844-0280)
bull If your country is not listed dial
1-763-274-7362 (reversed charges accepted)
myuhc com
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
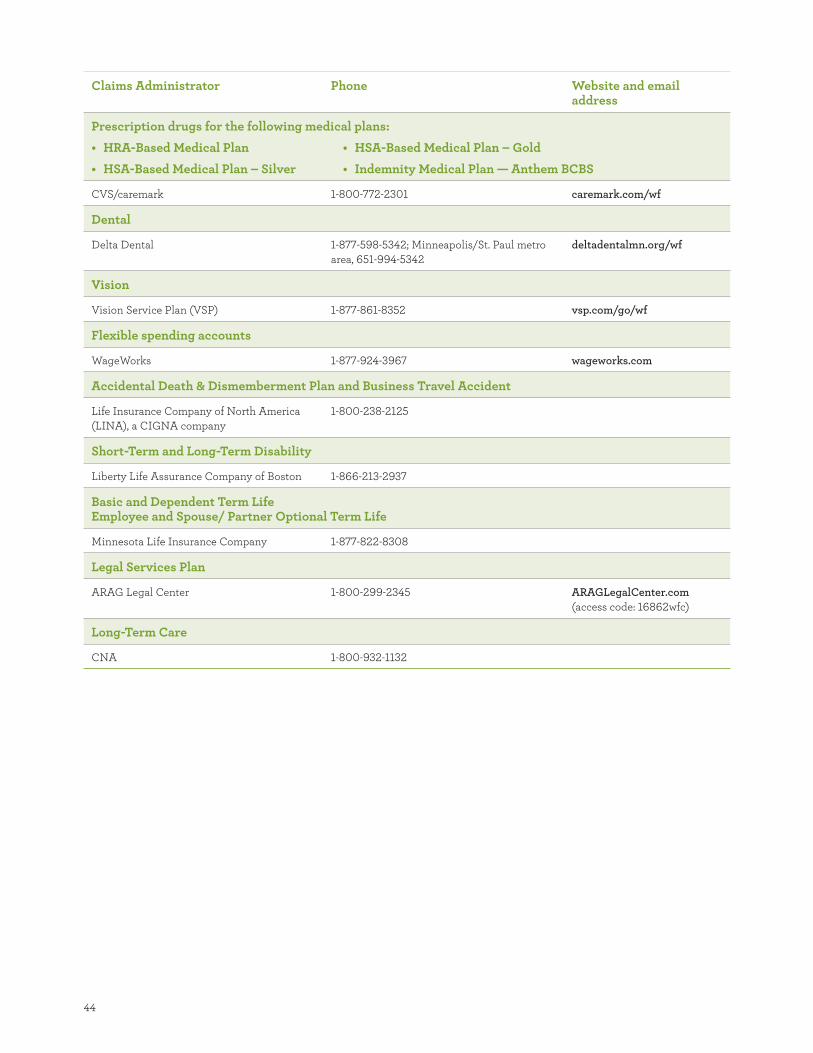
44
Claims Administrator Phone Website and email address
Prescription drugs for the following medical plans
bull HRA-Based Medical Plan
bull HSA-Based Medical Plan ndash Silver
bull HSA-Based Medical Plan ndash Gold
bull Indemnity Medical Plan mdash Anthem BCBS
CVScaremark 1-800-772-2301 caremark comwf
Dental
Delta Dental 1-877-598-5342 MinneapolisSt Paul metro
area 651-994-5342
deltadentalmnorgwf
Vision
Vision Service Plan (VSP) 1-877-861-8352 vsp comgowf
Flexible spending accounts
WageWorks 1-877-924-3967 wageworks com
Accidental Death amp Dismemberment Plan and Business Travel Accident
Life Insurance Company of North America
(LINA) a CIGNA company
1-800-238-2125
Short-Term and Long-Term Disability
Liberty Life Assurance Company of Boston 1-866-213-2937
Basic and Dependent Term Life Employee and Spouse Partner Optional Term Life
Minnesota Life Insurance Company 1-877-822-8308
Legal Services Plan
ARAG Legal Center 1-800-299-2345 ARAGLegalCenter com
(access code 16862wfc)
Long-Term Care
CNA 1-800-932-1132
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483
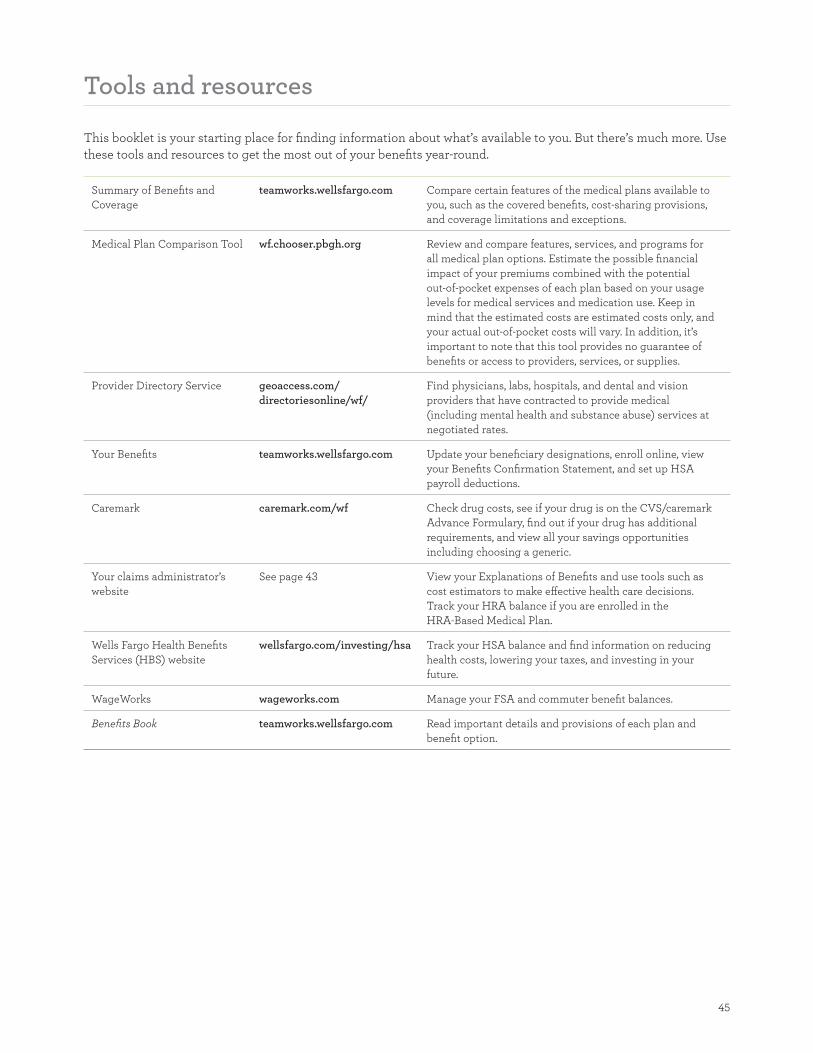
45
Tools and resources
This booklet is your starting place for finding information about whatrsquos available to you But therersquos much more Use
these tools and resources to get the most out of your benefits year-round
Summary of Benefits and
Coverage
teamworkswellsfargocom Compare certain features of the medical plans available to
you such as the covered benefits cost-sharing provisions
and coverage limitations and exceptions
Medical Plan Comparison Tool wfchooserpbghorg Review and compare features services and programs for
all medical plan options Estimate the possible financial
impact of your premiums combined with the potential
out-of-pocket expenses of each plan based on your usage
levels for medical services and medication use Keep in
mind that the estimated costs are estimated costs only and
your actual out-of-pocket costs will vary In addition itrsquos
important to note that this tool provides no guarantee of
benefits or access to providers services or supplies
Provider Directory Service geoaccesscom
directoriesonlinewf
Find physicians labs hospitals and dental and vision
providers that have contracted to provide medical
(including mental health and substance abuse) services at
negotiated rates
Your Benefits teamworkswellsfargocom Update your beneficiary designations enroll online view
your Benefi ts Confirmation Statement and set up HSA
payroll deductions
Caremark caremarkcomwf Check drug costs see if your drug is on the CVScaremark
Advance Formulary find out if your drug has additional
requirements and view all your savings opportunities
including choosing a generic
Your claims administratorrsquos
website
See page 43 View your Explanations of Benefits and use tools such as
cost estimators to make eff ective health care decisions
Track your HRA balance if you are enrolled in the
HRA-Based Medical Plan
Wells Fargo Health Benefi ts
Services (HBS) website
wellsfargocominvestinghsa Track your HSA balance and find information on reducing
health costs lowering your taxes and investing in your
future
WageWorks wageworkscom Manage your FSA and commuter benefi t balances
Benefits Book teamworkswellsfargocom Read important details and provisions of each plan and
benefi t option
46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

46
Important information and disclosures
The disclosures provided here contain important
information about the employee benefi t plans
sponsored by Wells Fargo amp Company We encourage
you to review them in addition to reviewing the other
benefi ts information provided to you
Offi cial plan documents
This guide is intended to provide a high-level
overview of the referenced employee benefi t plans The
information presented in this booklet does not contain
all the terms and provisions of the employee benefi t
plans sponsored by Wells Fargo amp Company Refer to
each planrsquos Summary Plan Description (SPD) contained
in the Benefi ts Book for applicable plan provisions
For fully insured plans or coverage options (including
health maintenance organizations [HMOs]) also refer
to the applicable insurance policy or group contract
provided by the insurer Additional plan details can
be found in the offi cial plan documents If there is a
discrepancy between the statements and information
contained in this benefi ts enrollment booklet and the
offi cial plan documents the offi cial plan documents will
govern
Wells Fargo amp Company reserves the unilateral right to
amend modify or terminate any of its benefi t plans (or
benefi t plan options) programs policies or practices
at any time for any reason with or without notice Any
such amendment modifi cation or termination may
apply to both current and future participants and their
dependents and benefi ciaries
Disclosure about health savings accounts (HSAs)
HSAs are not part of any Employee Retirement Income
Security Act (ERISA)-covered employee benefi t plan
sponsored or maintained by Wells Fargo amp Company
or any of its subsidiaries or affi liates It is Wells Fargo
amp Companyrsquos intention to comply with the US
Department of Labor guidance which specifi es that
an HSA is not subject to ERISA when the employerrsquos
involvement is limited Establishment of an HSA is
completely voluntary on your part
bull Wells Fargo amp Company does not limit your ability to
move your funds to another health savings account
or impose conditions on usage of such funds beyond
those permitted under the Internal Revenue Code
However Wells Fargo will only support payroll
deductions or provide funding of wellness dollars
and other employer contributions if applicable for
HSAs opened at Wells Fargo Health Benefi t Services
a division of Wells Fargo Bank NA
bull Wells Fargo amp Company does not make or infl uence
the investment decisions with respect to funds
contributed to an HSA Available HSA investment
funds are not guaranteed and you could lose money
bull Wells Fargo amp Company does not represent that the
HSA is an ERISA-covered employee benefi t plan
established or maintained by Wells Fargo amp Company
or any of its subsidiaries
An HSA is an individually owned account The HSA
will continue to be your account even if you leave
Wells Fargo or change health plan coverage
Disclosure about health reimbursement accounts (HRAs)
The HRA is a notional bookkeeping entry and no
specifi c funds will be set aside in an account for
purposes of funding an HRA No interest or earnings
will be credited to an HRA Amounts allocated to
an HRA including health and wellness dollars are
not vested and are subject to forfeiture Wells Fargo
amp Company reserves the unilateral right to amend
or modify the HRA at any time for any reason with
or without notice including placing limitations or
restrictions on amounts allocated to an HRA or
terminating the HRA
Optum
Optum administers the health and wellness activities
under the Wells Fargo amp Company Health Plan
including the online health assessment biometric
screenings online wellness education programs
and telephonic wellness coaching programs These
health and wellness activities are not a substitute
for and are not intended to provide medical care or
treatment Additionally the statements made in this
communication regarding biometric screenings are
for general information purposes only and do not
constitute individual medical advice or care You
should discuss specifi c questions about your individual
health care with your personal health care provider
Your participation in the health and wellness programs
administered by Optum is completely voluntary and
the information you share through your participation
will be kept strictly confi dential in accordance with
applicable law Only you Optum partners or affi liates
of Optum your medical planrsquos claims administrator
and your provider have access to your information and
results Wells Fargo will not receive any individually
identifi able information or results Wells Fargo will
receive only aggregate summary results which
47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

47
combine the data of all team members who participate
in health and wellness programs in a de-identifi ed
format Applicable law prohibits Wells Fargo from
using any of this information for employment-related
actions or decisions
Privacy of your protected health information
Your privacy is important We encourage you
to read the Notice of HIPAA Privacy Rights for
the Wells Fargo-sponsored group health plans to
understand how your protected health information
may be used and disclosed by the group health plans
and your rights under HIPAA The Notice is available
to you on Teamworks (search for ldquoNotice of HIPAA
Privacyrdquo) or you can request a copy by contacting the
HR Service Center at 1-877-HRWELLS (1-877-479-
3557) option 2 The HR Service Center accepts relay
service calls TDDTTY users may call 1-800-988-0161
Authorization to deduct premiums from payroll
By making your benefi t elections (including default
elections) for yourself and your dependents as part
of the benefi ts enrollment process you authorize
your employer to deduct from your pay the necessary
contribution and premium amounts for the benefi t
coverage you elected under the various Wells Fargo amp
Company employee benefi t plans including deducting
from your pay any back contributions or premiums for
coverage for which you may be in arrears to the extent
permitted by applicable law
General Information
The information presented in this booklet is not
intended to provide medical advice Consult with
your health care provider to determine the services or
treatments that may be appropriate for your situation
The provisions governing your medical plan control
what if any benefi ts are available for the services
you receive The fact that a health care provider has
performed or prescribed a procedure or treatment
does not mean that it is a covered service under your
medical plan
Eligibility for or participation in the employee benefi t
plans does not constitute a contract or guarantee
of employment with Wells Fargo amp Company or its
subsidiaries or affi liates
C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483

C000000
From well-managed forests
100
HRS9597 (0115)copy 2015 Wells Fargo Bank NA All rights reserved ECG-1230483