Embed Size (px)
Citation preview

©2014 Executive Health Resources, Inc. All rights reserved.
Documentation Improvement for Medical Necessity
Joydip Roy, MD
Senior Medical Director, Audit, Compliance and Education

©2014 Executive Health Resources, Inc. All rights reserved.
Agenda
• Objectives:
– Get Physician Buy In, Why status matters
– Documentation best practices and common errors
– Documentation examples
• Medical Necessity • 2 Midnight rule
©2014 Executive Health Resources, Inc. All rights reserved.
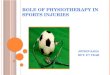
Why is Getting Patient StatusCorrect Such an Important Issue?
• Focus of Recovery Audit Contractors
• Potential False Claims issue if no complaint process is in place
• Potential recoupment of reimbursements during audit and loss of opportunity for appropriate OBS APC and ancillary charge payment
Overuse of Inpatient
• Length of stay artificially elevated
• Mortality data artificially elevated
• Qualified stay impact on patient’s skilled care benefit
• Unexpected patient financial responsibility (self-administered medication charges, inflated co-payments)
Overuse of Observation
It’s about getting it right!

©2014 Executive Health Resources, Inc. All rights reserved.
Patient Deductible and Co-Pays
• Day 1-60: $1216 inpatient deductible per Benefit Period
• Day 61-90: $304/day
• Day 91-151: $608/day
Inpatient (Part A) 2014:
• $147 per year deductible
• 20% coinsurance for all covered outpatient services
• 100% of non-covered outpatient services
Outpatient (Part B) 2014:
Source: http://www.medicare.gov/Pubs/pdf/11579.pdf

©2014 Executive Health Resources, Inc. All rights reserved.
National Exposure• NBC Nightly News/MSNBC March 2014:
– http://www.nbcnews.com/watch/nightly-news/why-going-under-observation-can-cost-you-170444355554– http
://www.nbcnews.com/watch/nightly-news/critical-advice-all-medicare-patients-should-hear-170260035926
• FierceHealthcare, July 15, 2013 – http://www.fiercehealthfinance.com/story/study-hospitals-lose-money-observation-care/2013-07-15?
utm_medium=nl&utm_source=internal
• JAMA: July 8, 2013 - Invited Commentary: Observation Status for Hospitalized Patients/Hospitalized but Not Admitted
• Kaiser News May 3, 2013 – http://www.kaiserhealthnews.org/Stories/2013/May/03/lawsuit-challenges-observation-rules-in-
Medicare.aspx
• Money August 2012; “This could Hurt—a lot” pg 70
• NYTIMES: In the Hospital, but Not Really a Patient; June 22, 2012
• USA Today April 17, 2012– http://www.usatoday.com/money/industries/health/drugs/story/2012-04-30/drugs-can-be-expensive-in-
observation-care/54646378/1
• Washington Post 2010: Patients held for observation can face steep drug bills

©2014 Executive Health Resources, Inc. All rights reserved.
CMS Transmittal 540• Issued on September 4, 2014
– Effective date: September 8, 2014
• MACs and ZPICs may deny “related” claims, either after review or automatically
• Medicare’s example:
– When the Part A Inpatient surgical claim is denied as not reasonable and necessary, the MAC may recoup the surgeon's Part B services. For services where the patient’s history and physical (H&P), physician progress notes or other hospital record documentation does not support the medical necessity for performing the procedure, post payment recoupment may occur for the performing physician’s Part B service.

©2014 Executive Health Resources, Inc. All rights reserved.
Documentation Tips for Medical Necessity

©2014 Executive Health Resources, Inc. All rights reserved.

©2014 Executive Health Resources, Inc. All rights reserved.
What the Auditors Expect

©2014 Executive Health Resources, Inc. All rights reserved.
What typically is Provided

©2014 Executive Health Resources, Inc. All rights reserved.
“Foreign Body Removed
#!”
Name Protected, MD

©2014 Executive Health Resources, Inc. All rights reserved.
Physician Documentation Uses
Before:
•Communication with physician partners and consultants
•Reminder notes for self use
•Possible use by nurses
Now:
•Audit defense
•Billing justification
•Malpractice defense
•Quality of Care Measurement
•Government investigations

©2014 Executive Health Resources, Inc. All rights reserved.
• Limited or no physician documented info (consult, ED note or H & P)– Only information available is a list of symptoms/ lab work– No documentation until several hours after “admission”
• No plan of care or clear impression in the H & P– Common with mid-level providers, medical students and residents
• OP note/H & P for procedures that do not address/include any risk from past medical history
– Frequently occurs from using office notes as history and physical
• Lack of discharge summary for a readmission review and no mention of stability on discharge/return to baseline in the discharge note
• Prolonged stays frequently do not include the current progress note or orders to indicate why the patient requires continued acute care
Common Documentation Problem Areas

©2014 Executive Health Resources, Inc. All rights reserved.
Common Documentation Problem Areas
• Using a symptom rather than a diagnosis for the impression or assessment
─ N/D/V vs. bowel obstruction
─ SOB, chest pain, headache, back pain
─ Listing the diagnosis as an intractable symptom (vertigo, abdominal pain, vomiting) without noting the potential diagnosis
• Using a lab value or treatment plan with no diagnosis
• Documentation for medical necessity is different than for billing level or coding
©2014 Executive Health Resources, Inc. All rights reserved.
General Documentation Takeaways
• 5 key pieces of documentation for Medicare cases and determining medical necessity of Inpatient:
– Medical history
– Current medical needs
– Severity of signs and symptoms
– Facilities available for adequate care
– Predictability of an adverse outcome
Source: CMS Medicare Benefit Policy Manual, Chapter 1, §10

©2014 Executive Health Resources, Inc. All rights reserved.
Key Words
What is your suspicion of what is going on, i.e. impression?SUSPECTS
PREDICTABLERISK
CONCERNS
Given the patient’s history and current presentation, what kind of adverse outcomes are likely and what are the chances
What are your concerns of the situation?

©2014 Executive Health Resources, Inc. All rights reserved.
IP Documentation Review
• Custodial
• Delay
• Convenience
• Any “kill the case” statements?– Can go home from ER but the family cannot take care of the patient
• “The patient was about to be discharged, but apparently she did/does not have much help at home and she is unable to take care of herself…”
– Contradiction of IP order and certification
• IP order and “I anticipate 1 midnight in the hospital and hence she will be admitted under observation.”
– Here for placement
– Home in AM after lab result

©2014 Executive Health Resources, Inc. All rights reserved.
IP Documentation Review
• “Case Killer” statement:
– “The patient was about to be discharged (from ER), but apparently she did/does not have much help at home and she is unable to take care of herself…”
– Instead consider:– 86 y/o female with hx CABG, valve replacement and two hip
replacements, had a ground level trip and fall, resulting in an acute left humerus fx and left sup and inf pubic rami fx. She was treated with IV morphine and had an episode of hypotension. Pt lives by herself and was being worked up as an outpt (for frequent falls). In addition, she is on IV antibiotics for a resistant organism after failing outpt treatment.

©2014 Executive Health Resources, Inc. All rights reserved.
Admission Review – Key Considerations
Physicians Order
Medical Necessity
Expectation of 2-Midnight Stay
Documentation and Certification

©2014 Executive Health Resources, Inc. All rights reserved.
Medical Necessity Example 1
• 76 y/o male with central intermittent chest pain for 2 days which lasts about 20 minutes, few episodes
• Awoke in the morning with left arm tingling that quickly resolved
• Past Hx includes MI, DM2, CABG and prior cardiac stents
• PE BP 90/65 HR 105 RR 24 – Tachycardiac with bilateral crackles
• EKG besides for Sinus Tach is unchanged and cardiac enzymes non-diagnostic, Cr 1.5, Bld Glc 220 g/dL
• Pain is relieved by NTG, then recurs and feels just like his prior MI
Chest Pain
THIS PATIENT PROBABLY DOES NOT MEET INPATIENT CRITERIA

©2014 Executive Health Resources, Inc. All rights reserved.
Documentation Keys: Chest Pain• The common term "chest pain" does not necessarily refer to cardiac disease
and is often misunderstood• Documentation of your clinical judgment (e.g., cardiac ischemia, recurrent or
worsening angina, chest wall pain, non-cardiac, GERD) is important– What is the rationale or factors you considered in your judgment?
• “Atypical chest pain” does not exclude ischemic disease – document
suspected cause regardless of typical or “atypical” pattern• Acute Coronary Syndrome encompasses UA, NSTEMI, or STEMI
– UA - rest angina (usually lasting >20min), new onset (<2months) duration of angina, or crescendo pattern
of occurrence
• Symptoms similar to past events?• EKG baseline vs. current if known and Cardiac Enzymes • Hypotension, Diaphoresis, CHF, Pulmonary Edema?

©2014 Executive Health Resources, Inc. All rights reserved.
Medical Necessity Example 2
• 72 y/o male sudden onset of slurred speech and right arm weakness witnessed by wife
• Past History: HTN, DM2
• BP 170/95 by EMS, in ED BP 135/85
• Symptoms present on EMS arrival
• PE in ED HR 120 – irreg irreg
• EKG by EMS showed Atrial Fibrillation
• Normal neuro exam (back to baseline) in ED
TIA
THIS PATIENT PROBABLY DOES NOT MEET INPATIENT SCREENING CRITERIA

©2014 Executive Health Resources, Inc. All rights reserved.
Documentation Keys: TIA/CVA• Similar previous episodes?
• Atrial Fibrillation/other source for potential cardio embolism?
• ABCD2 score (0 -7 score)─ Age over 60
─ Blood pressure (systolic > 140 or diastolic > 90)
─ Clinical features of TIA (1 or 2 points)─ Unilateral weakness with/without speech impairment
─ Duration (1 or 2 points)─ 10-59 min or over 60 min
─ Diabetes
• ABCD2 score and 2-day stroke risk─ Score of 0-3 = 1% risk of stroke in 2 days
─ Score of 4-5 = 4.1% risk of stroke in 2 days
─ Score of 6-7 = 8.1% risk of stroke in 2 days

©2014 Executive Health Resources, Inc. All rights reserved.
2 Midnight Example 1
Symptoms: 80 year old female admitted with chest pain, positive biomarkers and EKG changes in the emergency room, urgently taken to catheterization lab
Order • Admit as inpatient
Expectationof LOS
• “I expect this patient to remain in the hospital for a time greater than 2 midnights”
Medical Necessity • Documentation present to support inpatient admission
Certification • All elements of certification present per document review
Follow up necessary
• Patient does not remain for 2 MN⁻ Was (presumption not met) due to: death, transfer, AMA, inpatient-
only procedure or “recovery faster than anticipated”?⁻ Evaluate based on start of service to see if benchmark met

©2014 Executive Health Resources, Inc. All rights reserved.
2 Midnight Example 2
Symptoms:
65 year old male, no previous cardiac history, presents with shoulder pain after exertion, physician suspects musculoskeletal, biomarkers below detection threshold, no EKG changes. Monitor overnight if telemetry, enzymes and EKG’s remainnegative, anticipate discharge in am. No planned stress test or further evaluationduring hospitalization.
Order • Admit as inpatient
Expectation of LOS
• 23 hour monitoring
Medical Necessity • Documentation does not support inpatient admission – observation
Certification • Order and physician expectation of 2 midnights are in conflict• Order and medical necessity are in conflict
Follow up necessary
• Consider Condition Code 44 if requirements are met• If patient remains in hospital or new information available, re-review for
medical necessity at inpatient level• If patient discharged – cannot do Condition Code 44, if within rebilling
timeframe, consider for Part B rebilling
©2014 Executive Health Resources, Inc. All rights reserved.
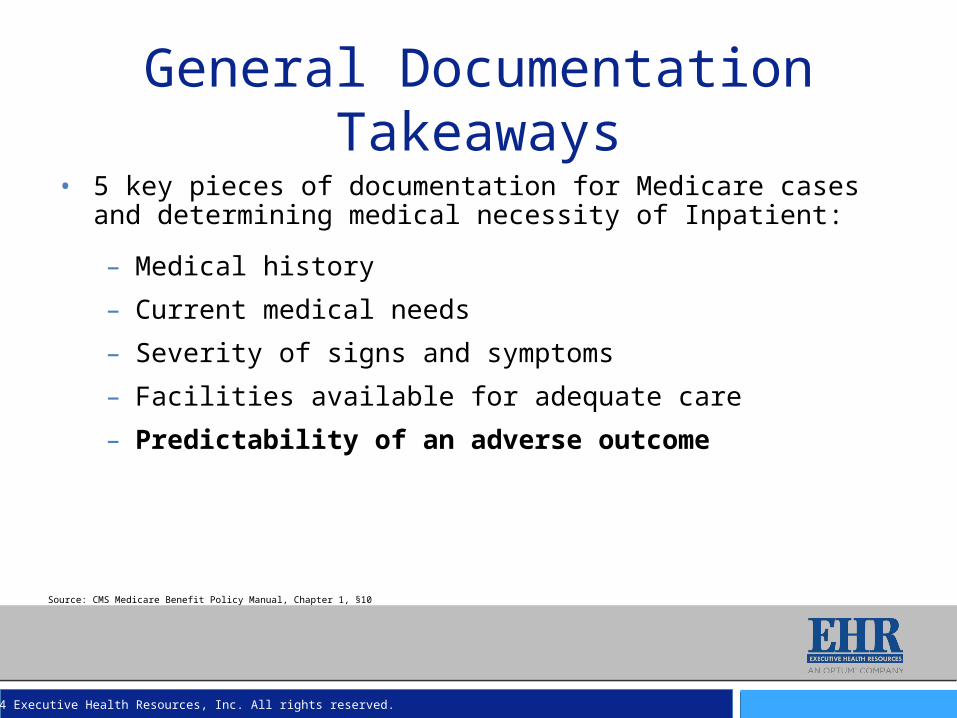
2 Midnight Example 3
Symptoms:78 year old female admitted for atrial flutter, stabilized in Emergency Room. Although expected to be discharged after medication adjustments, patient developed heart block requiring additional adjustments and possible pacemaker
Order • Place in observation
Expectation of LOS • Anticipate short stay, 23 hour monitoring
Medical Necessity • Delayed review suggests that inpatient may be appropriate
Certification • All elements of certification would need to be completed prior to discharge
Follow up necessary
• EHR would recommend inpatient level of service• Call with physician to discuss medical necessity in light of order change
requirement• Call with case manager to discuss order change and expectation
documentation with regard to certification requirements• Inpatient order, documentation of expectation and all other elements of
certification would need to be addressed prior to discharge

©2014 Executive Health Resources, Inc. All rights reserved.
2 Midnight Example 4
Symptoms:76 year old woman with UTI, treated with intravenous antibiotics. Fevers continue with tachycardia and hypotension requiring fluid support. Immunosuppressed due to post kidney transplant status.
Order • Admit for inpatient services
Expectation of LOS
• Admission orders include order for “discharge in am”
Medical Necessity
• Would meet for inpatient by criteria, but documentation clearly violates 2 midnight expectation
Certification • Depending on follow-up activity, if inpatient supported confirm all
elements of certification prior to discharge
Follow up necessary
• Although historically inpatient medical necessity would be met, the documentation does not support 2 MN expectation
• Resolve conflict between order/medical necessity and expectation• Update documentation if patient not discharged as planned• Consider Condition Code 44 if expectation of discharge remains

©2014 Executive Health Resources, Inc. All rights reserved.
2 Midnight Example 5
Symptoms:68 year old male, with a history of stroke, known carotid stenosis, and previous neck irradiation making carotid end-arterectomy high risk. Patient scheduled for carotid angiography and stent placement.
Order • Observation
Expectation of LOS
• Less than 2 midnights
Medical Necessity
• Procedure appropriate for inpatient based on inpatient-only status
Certification • All elements of certification except the 2 MN expectation would be
required to be documented prior to discharge to support inpatient claim
Follow up necessary
• Order should be corrected for procedure on CMS inpatient-only procedure list
• For procedures on the inpatient-only list, order must be present on the medical record prior to the initiation of the procedure
• Inpatient-only procedures are exempted from the 2 midnight expectation, but all other certification requirements remain

©2014 Executive Health Resources, Inc. All rights reserved.
Summary • Excellent patient care is top priority
• Regardless of the payer:– Admission order– Expected LOS– History and Physical/Procedure note– Progress note each hospital day– Discharge summary and plan– Above signed prior to discharge
• Make the obvious, obvious

©2014 Executive Health Resources, Inc. All rights reserved.
Questions?
Joydip Roy, MD
Senior Medical Director, Audit, Compliance and Education

©2014 Executive Health Resources, Inc. All rights reserved.
EHR has been awarded the exclusive endorsement of the American Hospital Association for its leading suite of Clinical Denials Management and Medical Necessity Compliance Solutions Services.
EHR received the elite Peer Reviewed designation from the Healthcare Financial Management Association (HFMA) for its suite of medical necessity compliance solutions, including: Medicare and Medicaid Medical Necessity Compliance Management; Medicare and Medicaid DRG Coding and Medical Necessity Denials and Appeals Management; Managed Care/Commercial Payer Admission Review and Denials Management; and Expert Advisory Services.
EHR was recognized as one of the “Best Places to Work” in the Philadelphia region by Philadelphia Business Journal for the past six consecutive years. The award recognizes EHR’s achievements in creating a positive work environment that attracts and retains employees through a combination of benefits, working conditions, and company culture.
AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance in marketing endorsed products and services. By agreement, pricing of endorsed products and services may not be increased by the providers to reflect fees paid to the AHA.
* HFMA staff and volunteers determined that this product has met specific criteria developed under the HFMA Peer Review Process. HFMA does not endorse or guarantee the use of this product.
About Executive Health Resources

©2014 Executive Health Resources, Inc. All rights reserved.
©2014 Executive Health Resources, Inc. All rights reserved.
No part of this presentation may be reproduced or distributed.Permission to reproduce or transmit in any form or by any meanselectronic or mechanical, including presenting, photocopying,recording and broadcasting, or by any information storage andretrieval system must be obtained in writing from Executive Health Resources. Requests for permission should be directed to [email protected].