Embed Size (px)
Citation preview

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 1/11
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 399, pp. 129–139
© 2002 Lippincott Williams & Wilkins, Inc.
129
Hemiarthroplasty has been the preferred treat-
ment for fractures of the femoral neck in elderly
patients. The objective of the current study was
to assess the outcome of revision of failed hemi-
arthroplasty to total hip arthroplasty in patients
with a primary diagnosis of a femoral neck frac-
ture. One hundred thirty-two conversions were
done in 108 women and 24 men. One hundred
two cemented and 30 uncemented hemiprosthe-
ses were revised to 88 cemented, 17 uncemented,
and 27 hybrid total hip arthroplasties and the
patients were followed up an average of 7.1
years (range, 5.1–15.3 years). Nine hips (6.8%)
were revised for loosening and four additionalhips (3%) were loose at the last followup. Sur-
vivorship free of revision was 96.5% (95% con-
fidence interval, 93%–100%) at 5 years and 92%
(95% confidence interval, 86%–98%) at 10 years.
Major perioperative complications occurred
frequently (45%), including 12 intraoperative
femoral fractures (9%) and 13 dislocations
(9.8%) Three of 12 (25%) of the intraoperative
femoral fractures developed later femoral com-
ponent loosening and all occurred during con-
version of an uncemented Austin-Moore type
hemiprosthesis. Conversion of endoprostheses
to total hip arthroplasties after femoral neck
fractures is fraught with high complication andloosening rates. Careful patient selection for
each type of arthroplasty (hemiarthroplasty
versus total hip arthroplasty) may help amelio-
rate the outcome of arthroplasty for patients
with femoral neck fractures.
Conversion total hip replacement has been de-fined as a total hip replacement done after
failed prior hip surgery.15 This term excludesa prior total hip replacement, and includes
failed hemiarthroplasties, failed hip pinnings,failed hip fractures treated with screw and sideplates, failed osteotomies, failed surface and
cup arthroplasties, and failed hip arthrodeses.One of the most common conversions done is
a conversion from a prior hemiarthroplasty orendoprosthesis to a total hip replacement. The
most common reason for conversion from afailed hemiarthroplasty to total hip replace-
ment is groin pain; however, thigh pain, stiff-ness in approximately 10% of patients, and ac-etabular bone loss are other important reasons
for conversion.3
The fate of conversion total hip replacement
has been reported previously. In 1972, Dupontand Charnley7 reported on 41 failed femoral
Conversion of Failed HipHemiarthroplasties After Femoral
Neck Fractures
Rafael J. Sierra, MD; and Miguel E. Cabanela, MD
From the Department of Orthopedic Surgery, MayoClinic, Rochester, MN.
Reprint requests to Miguel E. Cabanela, MD, MayoClinic, Rochester, 200 First Street, Rochester, MN 55905.
List of Abbreviations Used
IL-1 interleukin-1 beta
PGE2 prostaglandin E2

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 2/11
prostheses revised to total hip arthroplasties in49 patients. At 1 year, 70% of these patients
were pain-free. Later studies with longer fol-
lowup have shown an increased rate of radio-graphic loosening of the femoral compo-nent.12,13 There also have been reports of highintraoperative and postoperative complications
associated with conversion procedures.13,16,17
Several previous studies however, report
on conversion of hemiarthroplasties as aggre-gates, without specifically addressing differ-
ent prior diagnoses.12,13 The mode of failure of hemiarthroplasties done for patients with fem-oral neck fractures has been reported to differ
from hemiarthroplasties done for other rea-sons. Llinas et al12 reported that after femoral
neck fractures, there is a tendency of the fem-oral neck to resorb allowing the hemiarthro-
plasty to sink into the medullary canal to thelevel of the lesser trochanter. Conversion totalhip arthroplasty in this subgroup therefore
may be more challenging and should be donewith a great deal of caution to prevent intraop-
erative complications.The objective of the current study was to re-
port on the long-term followup of patients withconversion of hemiarthroplasties to total hip re-placements done for femoral neck fractures.
MATERIALS AND METHODS
All conversions from hemiarthroplasty to total hip
arthroplasty done at the authors’ institution from
1985 to 1995 were identified from the total joint
registry. Patients with hemiarthroplasties done for
diagnoses other than femoral neck fractures were
excluded from the study. Patients with acute femo-
ral neck fractures treated primarily with hemi-
arthroplasty and patients who had hemiarthroplasty
for failed hip fracture fixation were included in the
study. One hundred thirty-two conversion total hip
arthroplasties were identified during the study pe-
riod, and these represent a consecutive series.Demographic information was obtained from
the joint registry and from the patients’ charts. In-
formation dating to the patients index procedure
(femoral neck fracture reduction) or acute femoral
neck fracture was collected if available. This infor-
mation included date of fracture, date of hemi-
arthroplasty, time of onset of symptoms before
conversion total hip arthroplasty, date of conver-
sion total hip arthroplasty and intraoperative and
postoperative complications for each of the surgi-cal procedures.
Preoperatively all patients were evaluated for
severity of pain, range of motion (ROM), walking
distance, stair climbing ability, need for ambulatory
support, ability to get into a car, and ability to stoop.
All patients routinely were asked to attend followup
at 3 months, 1 , 2, 5, and 10 years postoperatively.
When this was not possible, clinical followup was
obtained by letter or telephone questionnaire.
Radiographs taken at the last followup were re-
viewed for evidence of acetabular and femoral
loosening, wear, or failure. All radiographs taken
preoperatively were reviewed by the authors. Forty
percent of radiographs taken at the last followupwere available for review. Kaplan-Meier survivor-
ship analysis10 was done to assess the probability of
clinical or radiographic failure. Survival free of re-
vision surgery or recommended revision surgery
and survival free of aseptic loosening (defined as
radiographic evidence of acetabular or femoral
loosening) were used as end points. In addition,
survival free of any reoperation was calculated.
Of the 132 conversions, 108 patients were fe-
male and 24 were male. Sixty surgeries were done
on the left hip and 72 were done on the right hip. At
the time of final followup, 49 patients had died and
83 were alive. All patients were followed up until
death or for a minimum of 5 years. Patients inwhom the conversion total hip replacement was re-
vised also were followed up after their revision to-
tal hip replacement. The last followup was recorded
at the clinic visit in 25 patients, by telephone inter-
view in 43 patients, and by written questionnaire in
62 patients. Two patients were lost to followup.
Two additional patients died before completing 2
years of followup. The mean clinical followup was
7.1 years 3.5 standard deviation for the entire
group, 7.0 years 3.0 standard deviation for the
patients who died, and 5.3 years 3.0 standard de-
viation for patients who were alive. Radiographic
followup greater than 2 years was available on 118
hips (89%).
Original Endoprosthetic Replacement
The underlying diagnosis for all patients was a
femoral neck fracture. One hundred seventeen en-
doprosthetic replacements were done acutely and
15 were done for a prior failed surgical intervention
Clinical Orthopaedics130 Sierra and Cabanela and Related Research

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 3/11
such as a failed open reduction and internal fixation,
a failed hip pinning, or a failed Girdlestone proce-
dure. The average age of the patients at surgery was
68.4 years 11 (standard deviation). The prosthe-ses implanted included 77 uncemented and three ce-
mented Austin-Moore prostheses (Howmedica Inc,
Rutherford, NJ), three uncemented and seven ce-
mented Thompson prostheses (Howmedica Inc),
five uncemented and seven cemented bipolar pros-
theses (Osteonics UHR, Osteonics Corporation, Al-
lendale, NJ), one cemented and 10 uncemented
Cathcart prostheses (Depuy Inc, Warsaw, IN), nine
uncemented Matchett-Brown prostheses (Howmed-
ica Inc), one uncemented head and neck prosthesis
(Howmedica Inc), six unspecified cemented unipo-
lar prostheses, and two unspecified uncemented
unipolar prostheses. No prosthetic information was
available in one patient. The majority of these surg-eries were done at an outside institution.
Conversion Surgery
The mean age of the patients at the time of the con-
version total hip arthroplasty was 73.1 years 10
(standard deviation) The average time from endo-
prosthetic replacement to conversion total hip
arthroplasty was 4.9 years 6.1 (standard devia-
tion). The reasons leading to the conversion in-
cluded groin pain with acetabular wear in 38 pa-
tients, thigh pain with loosening of the femoral
component in 22 patients, acetabular bone loss with
protrusio in eight patients, the combination of fem-
oral loosening and acetabular wear with or withoutacetabular protrusio in 54 patients, infection in
three patients, and a periprosthetic fracture in two
patients. The reason for conversion was unavail-
able in five patients. The average time from onset
of symptoms to conversion was 21 months 20
(standard deviation) The average anesthesia time
was 265 minutes 66 (standard deviation) and the
average operative time was 199 minutes 66
(standard deviation). The surgical interventions
that were done are shown in Table 1. Bone graft
was used in 13 patients during femoral reconstruc-
tion (eight had allografts and five had autologous
bone grafts) and also was used in 17 patients dur-ing acetabular reconstruction (11 had allografts and
six had autologous bone grafts). All patients re-
ceived perioperative antibiotics and some form of
postoperative deep venous thrombosis prophy-
laxis, most commonly warfarin.
RESULTS
Clinical Results
All patients were evaluated preoperatively be-fore conversion total hip arthroplasty; how-
ever, some data were not recorded for all pa-
tients. Fifty-one patients had severe pain, 52had moderate pain, 12 had slight pain, and twopatients had no pain preoperatively (n 117).Two patients did not limp, 36 had a slight
limp, 58 had a severe limp, and 14 patientswere unable to walk without support to evaluate
their limp preoperatively (n 110). Twenty-three patients used no support, 15 patients oc-
casionally used a cane, 51 patients used a canefull-time, two patients used one crutch, onepatient used two canes, seven patients used
two crutches, 10 patients used a walker, andtwo patients were unable to walk (n 111).
Five patients were able to walk unlimited dis-tances or for longer than 1 hour, 19 patients
walked a distance of 4 to 6 blocks, 51 pa-tients walked a distance of 1 to 3 blocks, 24patients walked indoors only, three patients
walked from their bed to a chair, and two pa-tients were unable to walk (n 104). Four pa-
tients could ascend stairs in a normal manner,60 patients used the railing, 24 patients as-
Number 399June, 2002 Conversion of Failed Hip Hemiarthroplasties 131
TABLE 1. Type of Components Implanted at the Time of Conversion Total HipReplacement
Type of Surgery Number Percentage
Both components cemented 88 66%
Both components uncemented 17 12.8%
Cemented femur, uncemented acetabulum (hybrid) 25 18.8%
Cemented acetabulum, uncemented femur 2 1.5%

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 4/11
cended one step at a time, and five patientswere unable to use stairs (n 93). Twenty-
three patients were able to get in a car without
difficulty, 64 patients were able to get in a carbut with difficulty, and one patient was unableto get in a car (n 88). No patient was activein heavy labor preoperatively or participated
in high demand sports such as jogging or ten-nis, four patients walked greater than a mile or
participated in sports such as golfing that putlow stress on the hip, 25 patients were com-
munity ambulators, 21 walked in their houseonly, and one only was able to move from thebed to a chair (n 81).
Physical examination showed that 100 pa-tients had no flexion contracture before the-
surgical procedure. Seven patients had a 5,two had a 10, one had a 20, and one a 25
flexion contracture preoperatively. Flexionranged from 30 to 125with an average of 90preoperatively (n 111). Abduction ranged
from 10 to 50 with an average of 28 preop-eratively (n 108). Adduction ranged from 0to 50 with an average of 22 preoperatively(n 105). External rotation ranged from 5 to
85with an average of 30 preoperatively (n109). Internal rotation ranged from 0 to 45
with an average of 11 preoperatively (n 109). A positive Trendelenburg sign was seenin 56 of 89 patients in whom it was recorded.
A leg length discrepancy was recorded in 68of 99 patients in whom it was recorded.
The average age of the patients at last fol-lowup was 80.7 years 9.6 (standard devia-
tion). Fourteen patients were older than 90years. These patients had multiple comorbidi-ties at the time of their last followup, which
should be taken into consideration when ana-lyzing these data. At last followup, six patients
had Parkinson’s disease, four had Alzheimer’sdisease, nine patients had been diagnosed with
some form of malignant disease, three patientshad strokes with resultant hemiparesis, 13 pa-tients had some other musculoskeletal prob-
lem that limited their activity such as distal fe-mur fractures, total knee arthroplasty, or severe
back pain, and another subgroup of patientshad end stage renal, cardiac, pulmonary, or
vascular disease. Despite these comorbidities,the overall satisfaction rate was high, with
70% of patients considering themselves to be
much better after the conversion.At last followup, 69 patients had no pain in
their hip, 32 patients had slight pain, 12 patients
had moderate pain, and five patients had severepain (n 118). Fifty-three patients did notlimp, 35 patients had a slight limp, 17 patients
had a severe limp, and 12 patients were unableto walk without support to evaluate their limp
postoperatively (n 117). Forty-six patientsused no support, 20 patients used a cane occa-
sionally, 18 patients used a cane full-time, onepatient used one crutch, two patients used twocanes, two patients used two crutches, 21 pa-
tients used a walker, and nine patients were un-able to walk (n 119). Twenty-six patients
were able to walk unlimited distances or longerthan 1 hour, 19 patients walked a distance of 4
to 6 blocks, 37 patients walked a distance of 1to 3 blocks, 20 patients walked indoors only,five patients walked from their bed to a chair,
and 10 patients were unable to walk (n 116).Twenty-three patients could ascend stairs in a
normal manner, 46 patients used the railing, 24patients ascended stairs one step at a time, and
22 patients were unable to use stairs (n 115).Seventy-one patients were able to get in a car
without difficulty, 28 patients were able to getin but with difficulty, and 10 patients were un-able to get in a car (n 109). One patient was
active in heavy labor or participated in high de-mand sports such as jogging or tennis at last fol-
lowup, 11 patients walked greater than a mile orparticipated in sports such as golfing that put
low stress on the hip, 47 patients were commu-nity ambulators, 15 patients walked in theirhouse only, and one patient was able to move
from the bed to a chair (n 102).Range of motion at last followup was 0 to
120 for flexion with an average of 92 (n 77). Abduction ranged from 0 to 50 with an
average of 33.9 (n 77). The average ad-duction was 27 (range, 10-35), the averageexternal rotation was 31 (range, 10-40), and
the average internal rotation was 23 (range,0-45) at last followup (n 36).
Clinical Orthopaedics132 Sierra and Cabanela and Related Research

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 5/11
Complications
The overall complication rate was 60%. Fifty-
eight (44%) major complications were recorded
in this group of patients after conversion totalhip replacement. These complications are shownin Table 2. In addition to these complications,
there were 21(16%) minor inhospital complica-tions that merited consultation by other services.These complications included cardiac compli-
cations with intensive care monitoring or cardi-ology evaluation in eight patients, postoperative
confusion in six patients, postoperative urinaryretention in five patients, postoperative ileus in
one patient, and a postoperative gouty attack inone patient.
ReoperationsFifteen patients had reoperation (17 surgeries).The overall reoperation rate was 12.8% that in-
cluded a 6.75% reoperation rate for asepticloosening, 1.5% for dislocation, 0.7% for in-fection, and 1.5% for fracture. Eight femoral
components (6%) and one acetabular compo-nent (0.7%) were revised for aseptic loosening.
The specific type of reoperation that was done
is shown in Table 3. When stratified by type of endoprostheses converted, eight of nine revi-
sions for loosening (89%) were in patients in
whom an uncemented Austin-Moore type pros-thesis had been replaced (Figs 1, 2). Ten of 77(13%) uncemented Austin-Moore prosthesesthat were converted to total hip arthroplasty
were documented as being loose at last fol-lowup (eight were revised and two were not re-
vised). The other three events of documentedloosening were in patients with conversions
from a cemented bipolar prosthesis, a cementedThompson prosthesis, and an unspecified ce-mented unipolar prosthesis. In addition, when
stratified by femoral fixation, eight of 113 ce-mented (7%) and five of 19 noncemented (29%)
conversion total hip arthroplasties were loose atlast followup.
Survivorship Analyses
Survivorship free of reoperation for all causeswas 92.5% at 5 years (95% confidence interval,
88%–98%), 88.4% at 10 years (95% confi-dence interval, 82%–95%) and 81% at 15years (95% confidence interval, 60%–93%)
Number 399June, 2002 Conversion of Failed Hip Hemiarthroplasties 133
TABLE 2. Major Postoperative Complications After Conversion Total Hip
Replacement
Percent With Percent InComplication Number Complications All Patients Comment
1 or more dislocations 13 22% 9.8% 2 led to revision of components
Intraoperative femoral 12 21% 9.0% 3 of these have been revised
fractures for femoral component loosening
Postoperative femoral 4 7.0% 3.0% Distal fractures
fractures
Loosening 13 22% 9.0% One led to refracture of the femur
and 9 have undergone revision of
components
Wear 4 7.0% 3.0% One patient also had a dislocation
Hematomas 4 7.0% 3.0% One after a femoral fracture
Superficial infection 1 1.7% 0.7% Later had multiple dislocations
Deep infections 1 1.7% 0.7% 1 debridementSoft tissue avulsion 1 1.7% 0.7% Led to abductor muscle repair
Vascular complication 1 1.7% 0.7% Led to a contained hematoma and
later to a dislocation
Deep venous thrombosis 1 1.7% 0.7%
Delayed wound healing 1 1.7% 0.7%
Heterotopic ossification 1 1.7% 0.7%

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 6/11
(Fig 3). Survivorship free of revision surgeryfor any cause was 96.5% at 5 years (95% con-
fidence interval, 93%–100%), 92% at 10 years(95% confidence interval, 86%–98%) and 86%
at 15 years (95% confidence interval, 64%–97%) (Fig 4). Survivorship free of femoral
component loosening was 97% at 5 years (95%confidence interval, 94.5%–100%), 92% at 10years (95% confidence interval, 86%–98%)
and 80% at 15 years (95% confidence interval,53%–96%) (Fig 5). Survivorship free of ac-
etabular component loosening was 99% at 5years (95% confidence interval, 97%–100%),
96% at 10 years (95% confidence interval,91%–100%), and 86% at 15 years (95% confi-dence interval, 62%–100%) (Fig 6).
DISCUSSION
Elderly patients with femoral neck fractures
commonly have been treated with hemiarthro-plasty or total hip arthroplasty. Hemiarthro-plasty has been shown to restore a functional
level of activity.2,4,9,15,17 Compared with a pri-
mary total hip replacement, it has been foundto have a higher revision rate especially in pa-tients with high physical demands in whom
wear of the acetabular side of the hip is an is-sue. The rate of degeneration of cartilage fromhumans has been studied in patients with a
hemiarthroplasty and it was shown that after 5
years, there is nearly complete loss of acetab-ular cartilage as seen on histologic examina-
tion.5 Groin pain and protrusio acetabuli arecommon causes of conversion of hemiarthro-
plasties to total hip replacements.2,4,6,9
Preoperative planning is essential in conver-
sion total hip replacements. Assessment of ac-etabular and femoral bone quality and stock,presence of endosteal cortical shell, and status of
the greater trochanter are all important. Knowl-edge of the prior approach, ROM, and power of
the abductors are essential in planning the pro-cedure. It may be necessary to plan ahead for a
trochanteric osteotomy or trochanteric slide asproposed by Glassman et al.8
Revision of an endoprosthesis to total hip
arthroplasty can be separated into five distinctgroups depending on the type of prosthesis, pa-
tient’s symptoms, and the quality of the fixationof the femoral component. These categories
are: (1) patients with an uncemented well-fixedprosthesis with symptomatic acetabular ero-sion; (2) patients with a loose uncemented pros-
thesis with either groin or thigh pain, or both;
(3) patients with a loose cemented unipolarprosthesis with either groin or thigh pain, orboth; (4) patients with a well-fixed cemented
unipolar prosthesis with symptomatic acetabu-lar erosion; and (5) patients with a well-fixedmodular stem (unipolar or bipolar) and symp-
tomatic acetabular erosion.
Clinical Orthopaedics134 Sierra and Cabanela and Related Research
TABLE 3. Number and Percentage of Reoperations Done After Conversion TotalHip Replacement
Percentage Percentage Reason ForType of Surgery Number (Reoperations) (All Patients) Surgery
Replacement of multiple components 5 29.4% 3.7% Loosening
Replacement of femoral component only 3 17.6% 2.2% Loosening
Replacement of acetabular component 2 11.7% 1.5% 1 for loosening,
1 for dislocation
Same acetabular component reinserted 1 5.8% 0.7% Dislocation
Open reduction and internal fixation 2 11.7% 1.5% Fractures (same
patient)
Debridement 1 5.8% 0.7% Infection
Removal of wires, foreign body 1 5.8% 0.7% Foreign body
Abductor muscle repair 2 11.7% 1.5% 1 for dislocation,
1 for soft tissue
avulsion

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 7/11
Number 399June, 2002 Conversion of Failed Hip Hemiarthroplasties 135
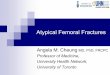
Fig 1 A–C. (A) A preoperative radiograph of a 62-year-old woman shows a loose uncemented Austin
Moore endoprosthesis and acetabular wear. (B) Aradiograph taken immediately after conversion toan uncemented total hip arthroplasty is shown. (C)A radiograph obtained 7 years postoperative showsclear evidence of femoral component looseningand subsidence.
A B
C

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 8/11
Clinical Orthopaedics136 Sierra and Cabanela and Related Research
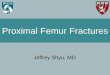
Fig 2A–B. (A) A preoperative radiograph of a 65-year-old woman shows a loose uncemented AustinMoore endoprosthesis. (B) A radiograph obtained 4 years after conversion total hip arthroplasty isshown. This patient had revision surgery to a cemented femoral component. There was no evidenceof loosening at the time of death, 5 years after conversion.
A B
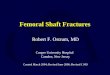
Fig 3. A Kaplan–Meier curve shows survivorshipfree from any reoperation.
Fig 4. A Kaplan-Meier curve shows survivorshipfree of revision surgery for any cause.

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 9/11
Intraoperatively, the treatment of each of
these patients differs. Previous authors havestated that potential difficulties included thedifficulty of detaching a fragment of the
greater trochanter of proper size and shape, thedifficulty in extracting the prosthesis evenwhen it was loose in the medullary canal, and
the fact that the track left by the prosthesis inthe canal often was lined with either endosteal
sclerotic bone or fibrous tissue, which madeanchoring a new prosthesis with cement more
difficult.13 Curettage of the canal has been ad-vocated to remove all fibrous tissue and reac-tive bone around the stem.13
The most common scenarios are the firsttwo of which conversion of an Austin-Moore
prosthesis or one of its variants is the most fre-quent. Either with a well-fixed or loose pros-
thesis, the danger of this procedure is fractur-ing the greater trochanter when extracting the
stem. As mentioned previously, the lateral as-pect of the metaphysis of the prosthesis often isembedded in the substance of the greater
trochanter and forceful blows on the extractorcan jam the lateral aspect of the prosthesis
against the trochanter and fracture it. The lateral-
most aspect of the prosthesis must be seen andno bone should be in the extraction path. If thisis encountered, a decision should be made to ei-ther burr the medial aspect of the trochanter or
alternatively to do a trochanteric osteotomy.The surgeon, however, must be aware that this
might leave a very poor trochanteric bed for
subsequent reattachment. A trochanteric slide
is worth considering in this situation. Whenthe prosthesis is well-fixed by bone that hasgrown through the fenestrations, freeing its
anterior and posterior surface with flexibleosteotomes between the prosthesis and the en-
dosteal surface of the femur may be necessary.Once the prosthesis is out, preparation of themedullary canal of the femur demands re-
moval of the neocortex that often surroundsthe stem of the extracted prosthesis. Revision
of an uncemented prosthesis is most com-monly done with cement, and the use of a small
burr to make irregularities in the medullarycanal might facilitate and enhance cement fix-ation. In the current study, there were 23 (32%)
uncemented Austin-Moore prostheses convertedfor acetabular erosion and five of these had ev-
idence of protrusio acetabuli. Four of these 23patients (17%) had evidence of loosening at
last followup. Thirty-nine additional Austin-Moore prostheses (54.5%) were converted for
a loose femoral stem. Six of these 39 patients(15.3%) had evidence of loosening at last fol-lowup. This underscores the difficulty in ob-
taining durable cement fixation in these situa-
tions. Despite these technical difficulties, thecurrent study showed that the conversion of the femoral component should be done with
cement (8% versus 29% incidence of loosen-ing at last followup).
The conversion of a loose cemented mono-
block femoral prosthesis is similar to the fem-
Number 399June, 2002 Conversion of Failed Hip Hemiarthroplasties 137
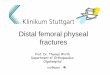
Fig 5. A Kaplan–Meier curve shows survivorshipfree of femoral component loosening (includesrevised and nonrevised femoral components.)
Fig 6. A Kaplan–Meier curve shows survivorshipfree of acetabular component loosening (includesrevised and nonrevised femoral components.)

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 10/11
oral side of a revision total hip replacement. If the prosthesis is fixed firmly with cement and
revision becomes necessary because of acetab-
ular symptoms (groin pain) and radiographicsigns in the acetabulum, the risks are perfora-tion or fracture of the femur. Cement occa-sionally can be removed with an extended
femoral osteotomy, although this seldom isadvisable unless bone quality is good, which is
rare. If the cement mantle is good, cementa-tion of a new stem into the cement is reason-
able. Revision of the acetabulum in these situ-ations may not present a problem unless therehas been considerable migration of the pros-
thesis inside the pelvis. In this situation, care-ful reaming technique, packing of cancellous
bone into the cavitary defects of the back andmedial aspects of the acetabulum, and the
placement of an uncemented acetabular com-ponent is the preferred technique. Occasion-ally, when prosthetic protrusio is extreme, ex-
posure may be difficult, a trochanteric osteotomyand removal of a thin rim of peripheral ac-
etabular bone to facilitate dislocation may beneeded. In the current study 18 cemented
monoblock prostheses were converted to totalhip arthroplasties. Two of these (11%) had ev-
idence of loosening at last followup. Both of these patients had conversion total hip arthro-plasty primarily for groin pain.
Conversion of a modular prosthesis is sim-ple, particularly in the case of a well-fixed mod-
ular, bipolar component. In the case of a bipo-lar prosthesis, the femoral component may be
left in its place if the head size can be accom-modated by a standard acetabular component.Hip instability attributable to poor soft tissue
tension may be a problem because neck lengthcannot be adjusted. A greater trochanteric os-
teotomy and advancement may solve this fairlyfrequent problem. In the current study, 13 bipo-
lar endoprostheses were converted to total hiparthroplasties. All were converted for a loosefemoral stem with or without acetabular symp-
toms. One of these (7.6%) had loosening at fi-nal followup.
The results of conversions from hemiarthro-plasty to total hip arthroplasty have been re-
ported at diverse followup periods. Sarmientoand Gerard13 reported their results in 95 pa-
tients at an average of 3 years. At this short fol-
lowup, they reported one acetabular compo-nent loosening and six femoral componentswith evidence of radiographic loosening. Am-stutz and Smith1 reported a 14.6% rate of fem-
oral component loosening and a 26.8% rate of nonprogressive loosening of the femoral com-
ponent at an average followup of 5.5 years. Twothirds of their patients had an index diagnosis of
a femoral neck fracture. Llinas et al12 also re-ported their experience with 99 conversionsfrom hemiarthroplasties and compared them
with cemented primary total hip arthroplasties.At an average of 7.6 years, they had a 6% re-
vision rate (two acetabula, one femur, andthree both) and the incidence of cement fracture,
cement-bone radiolucency, and progressiveloosening of the femoral component was higherfor patients with prior hemiarthroplasty. Stam-
bough et al16 reported the results of the conver-sion of 32 endoprostheses to cemented total hip
replacements. At an average of 6.4 years, therewas a 94% survival rate when compared with
a 96% survival rate in the control group. Inaddition, there were 10 times greater rates of nonunion and separation of the greater tro-
chanter, increased bone-cement demarcationlines (22% versus 4.6%), and subsidence (9.3%
versus 6.4%) when compared with total hiparthroplasty. The current study showed that at
an average of 7 years, the overall revision ratewas approximately 7%, the incidence of femo-ral loosening was 8.3%, and the incidence of ac-
etabular component loosening was 5.3%.The overall high rate of revisions in the
current series is comparable with other ratesreported in the literature.1,12,13,16 The high in-
cidence of revisions may be attributable toextensive resorption of the endosteal bone,
incomplete removal of the surrounding mem-brane, and the resulting poor quality of ce-ment mantle. In addition, the residual mem-
brane, besides its mechanical effect on thecement fixation, has been suggested to be
very active metabolically producing PGE2,collagenase, and IL-1; all these factors con-
Clinical Orthopaedics138 Sierra and Cabanela and Related Research

8/6/2019 2002 - Conversion of Failed Hip Hemiarthroplasties After Femoral neck fractures
http://slidepdf.com/reader/full/2002-conversion-of-failed-hip-hemiarthroplasties-after-femoral-neck-fractures 11/11
tributing to resorption of adjacent bone andultimately loosening.13
The incidence of complications after con-
version total hip replacement ranges from 7%to 64% in several series.4,10,14,15 The overallmajor complication rate in the current studywas approximately 45%. This reflects the
risk attendant to surgery in the elderly pa-tient. Additionally, there is an inherent risk to
the surgical procedure, with a high incidenceof intraoperative femoral fractures or pene-
trations, early postoperative trochanteric de-tachments, dislocations, deep venous throm-bosis, and major wound infections. The current
study showed that these patients are at an in-creased risk of intraoperative femoral frac-
tures (9.%) and recurrent dislocations (9.8%).Three of 12 intraoperative femoral fractures
later resulted in femoral component loosen-ing. Nine of the 12 (75%) intraoperative fem-oral fractures occurred while removing eight
noncemented and one cemented Austin-Mooreprostheses.
Lee et a111 reported their experience withprimary total hip replacement in patients with
femoral neck fractures. Their survivorshipanalysis showed a probability of survival of the prosthesis without revision of 95% at 5
years, 94% at 10 years, and 89% at 15 years.Compared with the study of Lee et al,11 the
survivorship results of the-current study areworse at 10 and 15 years. However, patients in
both studies had a high incidence of perioper-ative complications.
Conversion of endoprostheses to total hip
replacements is challenging. Special atten-tion should be given to the greater trochanter
and to the femoral shaft to prevent intraoper-ative fractures. The incidence of periopera-
tive complications in this subgroup of elderlyindividuals is high. When compared with pri-
mary total hip replacement after femoralneck fractures, patients having conversionfrom endoprostheses to total hip replacement
fare worse at long-term followup. Careful pa-tient selection for each type of arthroplasty
after femoral neck fractures may decrease theincidence of complications and ameliorate
the outcomes in the treatment of femoral neckfractures.
References
1. Amstutz HC, Smith RK: Total hip replacement fol-lowing failed femoral hemiarthroplasty. J Bone JointSurg 61A:1161–1166, 1979.
2. Bray TJ, Smith-Hoefer E, Hooper A, Timmerman L:The displaced femoral neck fracture: Internal fixa-tion versus bipolar endoprosthesis: Results of aprospective, randomized comparison. Clin Orthop230:127–140, 1988.
3. Cabanela ME: Conversion of Cup Arthroplasty andFemoral Endoprostheses to Total Hip Arthroplasty. InSteinberg ME, Garino JP (eds). Revision Total HipArthroplasty. Philadelphia, Lippincott Williams &Wilkins 537–544, 1999.
4. Clayer M, Bruckner J: The outcome of Austin-Moore hemiarthroplasty for fracture of the femoralneck. Am J Orthop 26:681–684, 1997.
5. Dalldorf PG, Banas MP, Hicks DG: Rate of degen-eration of human acetabular cartilage after hemi-arthroplasty. J Bone Joint Surg 77A:877–882,1995.
6. D’Arcy J, Devas M: Treatment of fractures of thefemoral neck by replacement with the Thompsonprosthesis. J Bone Joint Surg 58B:2779–2786,1976.
7. Dupont JA, Charnley J: Low-friction arthroplasty of the hip for the failures of previous operations. J BoneJoint Surg 54B:77–87, 1972.
8. Glassman AH, Engh CA, Bobyn JD: A technique of extensile exposure for total hip arthroplasty. JArthroplasty 2:11–21,1987.
9. Johnston CE, Ripley LP, Bray CB, et al: Primary endo-prosthetic replacement of acute femoral neck fractures:A review of 150 cases. Clin Orthop 167:123–130,1982.
10. Kaplan E, Meier P: Nonparametric estimation from in-
complete observations. J Am Stat Assoc 53:457–481,1958.11. Lee PB, Berry Di, Harmsen WS, Sim FH: Total hip
arthroplasty for the treatment of an acute fracture of the femoral neck: Long term results. J Bone JointSurg 80A:70–75, 1998.
12. Llinas A, Sarmiento A, Ebramzadeh E, Gogan WJ,McKellop HA: Total hip replacement after failedhemiarthroplasty or mould arthroplasty. J Bone JointSurg 73B:902–907, 1991.
13. Sarmiento A, Gerard FM: Total hip arthroplasty forfailed endoprostheses. Clin Orthop 137:112–117,1978.
14. Souminen S: Total hip replacement after failed hemi-arthroplasty. Ann Chir Gynaecol 78:309–315, 1989.
15. Squires B, Bannister G: Displaced intracapsularneck of femur fracture in mobile independent pa-
tients: Total hip replacement or hemiarthroplasty?Injury 30:345–348, 1999.16. Stambough JL, Balderston RA, Booth RE, Rothman
RH, Cohn JC: Conversion total hip replacement: Re-view of 140 hips with greater than 6-year followupstudy. J Arthroplasty 1:261–269, 1986.
17. Warwick D, Hubble M, Sarris I, Strange J: Revisionof failed hemiarthroplasty for fractures at the hip. IntOrthop 22:165–168, 1998.
Number 399June, 2002 Conversion of Failed Hip Hemiarthroplasties 139