Embed Size (px)
DESCRIPTION
Fracture
Citation preview

CASE REpORT
Coronal Fractures of the Femoral CondyleA Brief Report of Five Cases
Stephanie M. Holmes, MD, David Bomback, MD, and Michael R. Baumgaertner, MD
Summary: Coronal fractures of the femoral condyle (Hoffa fractures) are uncommon injuries that have a better outcome when treatedsurgically. We report a series affive Hoffa fractures (including onenonunion) treated at a Levell trauma center by one surgeon employing a protocol ofopen reduction and internal fIxation with lag screwsthrough a formal parapatellar approach. Postoperatively, all patientsbegan immediate unrestricted range ofmation. Initial weight bearingwas limited, but all patients were permitted full weight bearing by 10weeks. All fractures healed within 12 weeks without complications.The fInal range of mation for the patients with acute fractures was atleast0° to 115°. The patientwith a nonunionhad a preoperative flexion contracture of 20° and a final range of motion of 20° to 125°.Long-termfollow-up (average37 months,range 18-57 months)wasavailable for 3 of the 5 patients, and Knee Societyscores' were calculatedfor these patients (average 173of200 points, range 160-180points). The literature regardingthemanagementof Hoffafractures isreviewed.
Key Words: Hoffa,femoralcondyle, articular fracture
(JOrthop Trauma 2004;18:316-319)
UnicondYlar fractures of the femur in the coronal plane,first described by Hoffa in 1904,2 are rare injuries. Non
operative treatment of unicondylar femur fractures, includingHoffa fractures, yields poor rcsults.t? By definition, Hoffafractures are intraarticular, and the principles oftheirtreatmentparallel those ofother intraarticular fractures: atraumatic, anatomic reduction, with fracture fixation secure enough to allowfimctional aftertreatment. We report our results oftreatment infive consecutive patients with a straightforward surgical pro-
Accepted for publication May 20, 2003.From the Department of Orthopaedics and Rehabilitation, Yale University
School ofMedicine, New Haven, cr.No financial support of this project occurred. No party has received any com
pensation due to their work on this project.The device described in this article is FDA approved. No aclmowledgments
are requested.Reprints: Michael R. Baumgaertner, MD, Department of Orthopaedics and
Rehabilitation, Yale University School ofMedicine, PO Box20807l, NewHaven, cr 06520 (e-mail: [email protected]).
Copyright CJ 2004 by Lippincott Williams & Wilkins
316
tocol designed to achieve those goals and review the literatureconcerning the treatment of Hoffa fractures.
MATERIALS AND METHODSFive patients with isolated Hoffa fractures (AOIOTA
33.b3.2) presented to the senior author (M.R.B.) and weretreated using a standardized protocol. The average age of thepatients was 51 years (range 37-70 years). Three fractureswere medial, and two were lateral. The mechanism of injurywas a motor vehicle accident in four patients and a fall in onepatient. Four patients were treated acutely; one was treated following a referral for a symptomatic nonunion after nonoperative treatment. Three of the four acutely treated patients hadconcomitant skeletal injuries requiring concurrent intervention, but none of these compromised immediate functionaltreatment of the knee joint. The preoperative radiographs,computed tomography (CT) scan, intraoperative images, andpostoperative radiographs from one of the patients with anacute fracture are shown in Figures 1 to 4.
Surgical TechniqueA midline incision is made, and a medial or lateral para
patellar arthrotomy is performed over the involved condyle,preserving the fat pad. After routine joint inspection, the fracture is displaced with a bone spreader and debrided. The fracture is anatomically reduced and held compressed with pointedWeber bone clamps. Drilling for screw placement is initiatedjust proximal to the patellafemoral joint, is directed perpendicular to the fracture line, and continues deliberately throughthe articular surface of the posterior condyle. This allows forexact length measurement and assists in maintaining thespread and parallelism of the remaining screws (Fig. 3). Following overdrilling, multiple parallel 3.5-rnrn screws areplaced across the fracture site from anterior to posterior. Depending on the quality of the anterior cortex, screws can becountersunk, or a small plate functioning as a washer can beused (Fig. 4).
The tourniquet times ranged from 45 to 74 minutes.Blood loss was less than 150 rnL in all patients except the patient with the nonunion, who required iliac crest bone grafting.Postoperatively, all patients began unrestricted immediate
J Orthop Trauma» Volume 18, Number 5, May/June 2004

JOrthop Trauma • Volume 18, Number 5, May/June 2004
FIGURE 1. Anteroposterior and lateral radiographs of coronalplane fracture of the distal femur. The step-off on the lateralcondyle is clearly visible on both views.
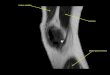
FIGURE 2. Sagittal plane computed tomographic reconstruction of distal femoral Hoffa fracture. Note the separation of thetibiofemoral joint from the patellofemoral joint and shaft bythe fracture. Shearing forces along the fracture plane increasewith knee extension.
c 2004 Lippincott Williams & Wilkins
Case Report
range ofmotion. Initial weight-bearing status was limited, butall patients were allowed full weight bearing within 10 weeks.
RESULTSAt 12 weeks, all fractures were healed clinically and ra
diographically. There were no superficial or deep infections orhardware removals. All patients had a documented range ofmotion of 0° to at least 115° except the patient with the nonunion, who had a severe preoperative flexion contracture of20° and whose range of motion when lost to follow-up after5 months was 20° to 125°. Long-term follow-up (average37 months, range 18-57 months) was available for 3 of the5 patients. Their average Knee Society score was 173 (average160-180).
FIGURE 3. Temporary coronal and epicondylar fracture stability is achieved with Weber pointed forceps and pelvic reduction clamps to allow for lag screw fixation . The posterior condylar articular surface is breached to facilitate exact measurement for implant length and to maximize lag screw purchase.
317

Case Report
FIGURE 4. Seven-month follow-up radiographs of fractureshown in Figures 1 and 2. A plate was used to function like awasher, counteracting a thin anterior cortex.
DISCUSSIONHoffa fractures are rare injuries, and lateral fractures are
more common than medial fractures. They usually occur as anisolated injury to the involved femur, but bilateral Hoffa fractures 7 and unilateral bicondylar Hoffa fractures" have been reported. In addition, Hoffa fractures associated with supracondylar intercondylar (AO/OTA 33C) femur fractures have beenobserved," and the reporting authors highlight the need for preoperative detection ofthe Hoffa fracture to select the appropriate fixation method for the supracondylar fracture.
The specific mechanism of injury that produces theHoffa fracture is unknown, but a shearing force on the posterior femoral condyle is postulated."? Lewis et al4 argued thataxial load to the lateral femoral condyle with the knee in 90° ormore of flexion produces posterior tangential fracture patterns.Four ofseven patients in their series were riding motorcycles atthe time of injury, placing the knee in 90° of flexion and positioning the lateral femoral condyle to receive an impact. TheHoffa fracture effectively separates the patellofemoral jointfrom the tibiofemoral joint; knee movement and particularlyweight bearing cause high shear forces along the fracture line,making non operative management unpredictable and adequatestabilization challenging.
Examination invariably identifies effusion, but varusand valgus instability may be subtle. The neurovascular statusshould be assessed as in all high-energy knee injuries. Initialanteroposterior and lateral radiographs may be unimpressivebecause Hoffa fractures, especially when nondisplaced, aresometimes difficult to detect. 11 On the anteroposterior view,the foreshortened fractured condyle may lead to the appearance of varus or valgus malalignment. On a true lateral view,the femoral condyles are not superimposed, and this may bemisinterpreted as a poor radiographic view of a normal knee(Fig. 1). Oblique radiographs may be helpful, but if the stan-
318
JOrthop Trauma • Volume 18, Number 5, May/June 2004
dard radiographic views do not confirm and define the fracture, a CT scan is necessary (Fig. 2).
In an attempt to predict which coronal plane fractures ofthe femoral condyle would progress to avascular necrosis,Letenneur et ae proposed dividing Hoffa fractures into threetypes, based on the distance of the fracture line from the posterior cortex of the femoral shaft. A subsequent report fromLewis et al" failed to validate this classification. The AO Comprehensive Classification oflong bone fractures and the OTAFracture Compendium identify the unicondylar coronal fracture as 33.b3.2 but provide little information about prognosisor treatment. 12, 13
Although it is generally accepted that surgical stabilization is necessary to achieve satisfactory function following aHoffa fracture.i"? the few reports in the literature that describeoperative treatment do not outline clearly a straightforward,dependable treatment approach with its underlying rationale,and they vary considerably with respect to the surgical approach, postoperative protocol, and outcome measures. Thereis a dearth of specific information on the preferred management of this fracture in several popular orthopaedic fracturemanagement texts. 14
-16 We found 18 articles concerning the
management of Hoffa fractures; 5 of these reports simply includedHoffa fractures as a part ofa series ofunicondylar distalfemur fractures. The report of Lewis et al" on seven coronalfractures of the lateral femoral condyle represents the largestsingle group of patients studied, but only five fractures weretreated operatively. They used either a medial parapatellar arthrotomy or a direct lateral approach between the iliotibialband and the biceps tendon to expose the fracture and two nonparallel screws to fix it. Postoperatively, patients were placedin cylinder casts for 2 to 6 weeks depending on the stabilityachieved intraoperatively. All five fractures treated surgicallyhealed, and at final follow-up (average 13 months), knee rangeof motion averaged 110° (range 95° to 130°).
Two reports of arthroscopically assisted reduction andinternal fixation of femoral condyle fractures have appeared.!" 17 Wallenbock and Ledinski 10 reported a series of24intraarticular knee fractures that they treated with arthroscopically assisted reduction and internal fixation, which includedtwo Hoffa fractures. Although noting that the technique of arthroscopically assisted reduction is demanding, they reportedgood early results. They did not describe specifically the technique or outcome of the patients with coronal fractures. MeCarthy and Parker!" described a patient with a sagittal planelateral femoral condyle fracture. Although their fixation didnot appear to achieve rigid compression, 18 they cited reducedsoft tissue dissection, blood loss, and operative time and afaster recovery time after arthroscopic management as advantages over formal open reduction. It is difficult to concludefrom these two reports that arthroscopically assisted reductionand internal fixation has any clear advantage over the opentechnique.
© 2004 Lippincott Williams & Wilkins

J Orthop Trauma» Volume 18, Number 5, May/june 2004
Ostermann et al'? emphasized fracture compression andrigid internal fixation to allow immediate postoperative kneemotion in their report on the long-term (average 68 months)results of29 unicondylar femur fractures, ofwhich there weresix Hoffa fractures. They did not describe their surgical approach or the outcomes ofthe patients with Hoffa fractures, butthey noted that 23 of27 patients available for follow-up had anexcellent result.
Manfredini et al ' surgically treated 19 patients withunicondylar femur fractures, six of which were Hoffa fractures, using a variety of open reduction and internal fixationtechniques. Four patients with unicondylar femur fractureswere treated nonoperatively in casts. Of the patients treatedsurgically, 16 were available for follow-up at a mean of 60months; 11 had good or excellent results, and 5 had fair or poorresults. The four patients treated nonoperatively had an unfavorable outcome, with three fair and one poor result.
Liebergall et afo described a lateral approach to theknee, using an osteotomy ofGerdy's tubercle, in the treatmentof a lateral coronal condylar fracture, but did not offer anyoutcome data on this single case. The authors argued that theosteotomy permits improved visualization for open reductionand internal fixation.
A cadaveric study compared the stiffuess and load tofailure of 3.5-mm cortical lag screws, 4.5-mm cortical lagscrews, and 6.5-mm cancellous screws used to fix experimentally created Hoffa fractures.:" There was no difference instiffness between any ofthe groups, but the load to failure wassignificantly higher for 6.5-mm screws compared with 3.5-mmscrews. The investigators questioned whether that result wasclinically significant and noted that smaller screws, such as3.5-mm cortical screws, may be much easier to fit around arigid implant if such fixation is necessary, as in the case of asupracondylar femur fracture with an associated Hoffa fracture.
Commonly referenced orthopaedic fracture management textbooks offer a paucity of information regarding thepreferred surgical management of Hoffa fractures. One majortexr'" does not even mention this fracture pattern. Muller andAllgower's Manual ofInternal Fixation 15 includes a diagramof a Hoffa fracture fixed with two anteroposterior screws butdoes not offer a text description. Schatzker and Tile 16 described the Hoffa fracture pattern and noted that nonoperativetreatment of Hoffa fractures leads to poor function but otherwise did not offer a management approach.
Our series of five operatively treated isolated Hoffa fractures is unique in that, in contrast to the reports ofLewis et al"and Manfredini et al," we employed a standardized surgicalapproach to the fracture and achieved rigid fixation with optimally positioned lag screws placed perpendicularly to the fracture plane. We believe that an ipsilateral parapatellar approach
© 2004 Lippincott Williams & Wilkins
Case Report
provides the visualization of the fracture and articular surfacenecessary for achieving a perfect anatomic reduction and theexposure to compress and rigidly fix the fracture with multiplelag screws. The excellent fracture stability that is achieved allows for unrestricted immediate range of motion of the joint,minimizing the risk of postoperative joint ankylosis. As morefractures are managed with limited open and percutaneoustechniques, the Hoffa fracture pattern stands out as one thatstill is managed best by a "low-tech" formal open reductionand classic lag screw fixation. In our hands, this method has ledto uniformly good results without complications.
REFERENCES
1. Insall IN, Dorr LD, Scott RD, et al. Rationale of the Knee Society clinicalrating system. Clin Orthop. 1989;248:13-14.
2. Hoffa A. Lehrbuch der Frakturen und Luxationen. Stuttgart: Verlag vonFerdinand Enke, 1904:451.
3. Letenneur J, Labour PE, Rogez lM, et al. Fractures de Hoffa: a propos de20 observations. Ann Our. 1978;32:213-219.
4. Lewis SL, Pozo JL, Muirhead-Allwood WFG. Coronal fractures of thelateral femoral condyle. J Bone Joint Surg Br. 1989;71: 118-120.
5. Manfredini M, Gi1done A, Ferrante R, et al. Unicondy1ar femoral fractures: therapeutic strategy and long-term results. Acta Orthop Belg. 2001;6n32-138.
6. McDonough PW, Bernstein RM. Nonunion ofa Hoffa fracture in a child.J Orthop Trauma. 2000;14:519-521.
7. Heuschen UA, Gohring U, Meeder PJ. Die beidseitige Hoffa-Fraktureine Raritat. Aktuelle Traumato!' 1994;24:83-86.
8. Zeebregts CJ, Zimmerman KW, ten Duis HJ. Operative treatment of aunilateral bicondy1ar fracture of the femur. Acta Chir Belg. 2000;100:1104-1106.
9. Baker BJ, Escobedo EM, Nork SE, etal. Hoffa fracture: a common association with high-energy supracondylar fractures of the distal femur. AJRAm J Roentgeno!. 2002;178:994.
10. Wallenbock E, Ledinski C. [Indications and limits of arthroscopic management ofintraarticular fractures of the lmee joint] [German]. AktuelleTraumato!' 1993;23:97-101.
11. Allmann KH, A1tehoefer C, Wi1danger G, et al. Hoffa fracture-a radiologic diagnostic approach. J Belg Radio!' 1996;79:201-202.
12. Muller ME, Nazarian S, Koch P, Schatzker J. The Comprehensive Classification of Fractures of Long Bones. Berlin: Springer-Verlag,1990,144-145.
13. Orthopaedic Trauma Association Committee for Coding and Classiflcation. Fracture and Dislocation Compendium: distal femur fractures. J Orthop Trauma. 1996;1O(Suppl. 1):45.
14. Browner BD, Jupiter JB, Levine AM, et al. Skeletal Trauma. 2nd ed.Philadelphia, PA: WB Saunders, 1998.
15. Muller ME, Allgower M, Schneider R, eta1. Manual ofInternal Fixation.3rded. New York, NY: Springer-Verlag, 1995:549.
16. Schatzker J, Tile M. The Rationale ofOperative Fracture Care. 2nd ed.Berlin: Springer-Verlag, 1996:390-391.
17. McCarthy JJ, Parker RD. Arthroscopic reduction and internal fixation ofa displaced intraarticular lateral femoral condyle fracture of the lmee. Arthroscopy. 1996;12:224-227.
18. Stern RE. Comment. Arthroscopy. 1996;12:760-761.19. Ostermann PA, Hahn MP, Ekkernkamp A, et al. Monocondy1are Frak
turen des Femur. Oururg. 1997;68:72-76.20. Liebergall M, Wilber JH, MosheiffR, et al. Gerdy's tubercule osteotomy
for the treatment of coronal fractures of the lateral femoral condyle. JOrthop Trauma. 2000;14:214-215.
21. Becker PL, Staford PR, Goulet R, et al. Comparative analysis for the fixation of coronal distal intraarticu1ar femur fractures. Presented at the 67thannual meeting of the American Academy of Orthopaedic Surgeons,March 15-19,2000.
319