Embed Size (px)
Citation preview

Proximal Femur Fractures
Jeffrey Shyu, MD

Learning Objectives
Provide an intuitive understanding of the
morphologic types, injury mechanisms, and
classification systems of adult proximal femur
fractures, using multimodality imaging
examples, 3-D models, and animations.
Review the potential complications and
management.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Proximal Femur Fractures:
Organization Tree
* Basicervical fractures, although intracapsular, are managed like intertrochanteric fractures.
Proximal Femur Fractures
Femoral Head
Osteochondral
Subchondral
Extracapsular
Intertrochanteric
Greater Trochanter
Lesser Trochanter
Subtrochanteric
Intracapsular
Basicervical*
Transcervical
Subcapital
Proximal femur fractures may be divided into femoral head, intracapsular femoral neck, and
extracapsular fractures. Accurately categorizing the anatomic location and subtype of the
fracture has significant implications for surgical management.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

osteochondral fracture subchondral fracture subcapital fracture transcervical fracture basicervical fracture intertrochanteric fracture greater trochanter fracture lesser trochanter fracture subtrochanteric fracture
Proximal Femur Fractures
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Anatomy
MOVIE: Computer generated tour of the relevant muscular, ligamentous, labral, and bony
anatomy of the hip.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Anatomy
The hip is a synovial joint with wide range of rotational motion and stability
Stability is conferred by its ball and deep socket configuration, acetabular labrum, a strong joint capsule,
articular cartilage, and surrounding muscle
One of the few inherently stable joints because of its bony anatomy
Iliofemoral and pubofemoral ligaments cover hip joint anteriorly. Ischiofemoral ligament covers hip joint
posteriorly
Byrne DP et al. The Open Sports Medicine Journal 2010
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Anatomy: Arterial Supply
Medial femoral circumflex artery• Largest, most important contributor
• Posterior portion of vascular ring
• Supplies superolateral femoral head
Lateral femoral circumflex artery• Anterior portion of vascular ring
• Supplies inferoanterior femoral head
Obdurator artery• Via ligamentum teres
• Little supply to femoral head, inadequate in
setting of displaced head/heck fractures
Ascending cervical arteries • Feeder vessels arising from extracapsular ring
• Penetrate capsule
• Run parallel to femoral neck towards the head
• Lateral vessels provide greatest supply
A major concern of femoral head and
neck fractures is disruption of the
arterial supply, which results in
avascular necrosis. In fractures, the
intraosseous cervical vessels are
disrupted.
Trueta J et al. J Bone Joint Surg BR 1953; Ly TV et al. J Boint Joint Surg Am 2008.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
Lat. fem
circumflex
Med. fem
circumflex
Deep femoral
art.
Obdurator art.

Hip experiences combined
mechanical loads• Axial load along shaft, compressive stress
• Bending load along neck, tensile stress applied
at upper neck and compressive stress at lower
neck
Cancellous bone arranged along
principal lines of stress• Primary medial trabeculae resist compression
• Primary lateral trabeculae resist tension
Stress lines explain patterns of injury
Ward’s Triangle: Weakest point of
femoral neck
Tensile groupCompressive group
Ward’s Triangle
Anatomy: Stress Lines
Byrne DP et al. The Open Sports Medicine Journal 2010; Bowman KF Arthroscopy 2010.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Imaging Modalities
Dominguez S et al. Acad Emerg Med 2005; Frihagen F et al. Acta Orthop 2005; Kirby MW et al. AJR Am J Roentgenol 2010; Khurana B et al. AJR 2012
Plain Film Radiography• First line study
• 90% sensitive, however 2-11% of ED patients
have radiologically occult fractures
• AP and lateral radiographs of the hip
• AP radiograph of the pelvis, to assess for
pelvic injury and compare with contralateral
hip
CT• More readily accessible than MRI in acute ED
settings
• Useful in trauma for detecting intra-articular
extension, acetabular fracture, pelvic ring, and
sacral fractures
• However, second-line compared to MRI
because of concerns for missing fracture lines
• May be useful for preoperative evaluation
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
Coronal CT demonstrates a valgus impacted
femoral neck fracture

Imaging Modalities
Dominguez S et al. Acad Emerg Med 2005; Frihagen F et al. Acta Orthop 2005; Kirby MW et al. AJR Am J Roentgenol 2010 Khurana B et al. AJR 2012
MRI• Obtain if radiographs are negative/equivocal and clinical suspicion is high
• More sensitive than CT for evaluating occult fractures
• Best for evaluating bone marrow, joint space, osteochondral injuries, early diagnosis
and staging of AVN
• May be limited in access in an acute ED setting
• Technique: Useful MR sequences include the following: coronal STIR, coronal T1, axial
dual-echo, axial T2 fat-saturated FSE, axial fat-saturated FSE proton density, sagittal
T1, axial T1.
• Most useful sequences are coronal STIR (for edema) and coronal T1 (for fracture line)
Bone Scan• Indicated for suspected fracture or AVN not demonstrated on plain film, and where MRI
unavailable
• High sensitivity, but poor specificity
• Minimum of 4 hours to perform, and may take up to 24-48 hours
• Relatively less useful in osteoporotic patients
• Poor spatial localization of fracture lines
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Occult Femoral Neck Fracture
Seen Only on MRI
Dominguez S et al. Acad Emerg Med 2005
AP radiograph of the hip demonstrates no
evidence of fracture.On coronal T1 MRI, a hypointense fracture
line is present.
Up to 11% of ED patients have radiologically occult hip fractures
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Traumatic Femoral Head
(Osteochondral) Fractures
Traumatic femoral head fractures typically result from high energy impact, and are often
associated with hip dislocations
Posterior dislocations 9x more common than anterior
Partial flexion, internal rotation typically leads to a posterior fracture-dislocation pattern
Ross JR et al. Curr Rev Musculosk Med. 2012
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Femoral Head Fractures:
Pipkin Classification
Posterior dislocation
Fracture below fovea, non-weight-bearing
Posterior dislocation
Fracture above fovea, weight-bearing
Associated femoral neck fracture Type I, II, or III, associated acetabular fracture
Rockwood and Green’s Fractures in Adults 2010; Ross JR et al. Curr Rev Musculosk Med 2012
Most commonly used classification for femoral head fractures, and used to guide
operative versus nonoperative managementDisclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Traumatic Femoral
Head Fractures
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
Femoral head fracture with posterior dislocationFemoral head fracture with subfoveal
involvement (Pipkin I)

Traumatic Femoral Head Fractures:
Surgical Considerations
Intra-capsular fracture, concern for avascular necrosis
• Emergent closed reduction as soon as feasible, preferably within 6 hours
• If irreducible, or with femoral neck fracture, then ORIF
Above or below fovea?
• Above fovea, weight bearing
• Below fovea, non-weight bearing, could potentially be treated conservatively
Is traction indicated?
• If fracture flipped, then traction indicated
Congruent?
• If incongruent, then operative management
Management Strategies
• Conservative management: Pipkin I
• ORIF: Pipkin II, Pipkin III, IV, irreducible fracture-dislocation
• Core decompression for osteonecrosis is controversial
Rockwood and Green’s Fractures in Adults 2010; Ross JR et al. Curr Rev Musculosk Med. 2012
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Subchondral Insufficiency
Versus Osteonecrosis
Osteonecrosis• Typically 30s-40s in age
• Associated with steroid/alcohol use
• 50-70 percent bilateral
MRI
• T1: Smooth band that is concave to the articular surface,
and circumscribes necrotic segments
Treatment• No femoral head collapse: conservative treatment
• Femoral head collapse: THA or hemiarthroplasty
Yamamoto T Clin Orthop Surg 2012; Ikemura S et al. AJR 2010
Subchondral insufficiency fractures are a recently recognized entity that may mimic osteonecrosis of the
femoral head. However, certain clinical and imaging features will favor one diagnosis over the other.
Osteonecrosis: coronal T1: bilateral decreased T1 signal in the femoral
heads, and serpiginous bands concave to articular surface
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
A B
Subchondral Insufficiency• Biphasic pattern: elderly females and young active individuals
• Typically unilateral
MRI
• Irregular, hypointense disconnected band that runs almost
parallel to femoral head
• High signal proximal segment on C+ images
Treatment• No femoral head collapse
• Young: Trochanteric rotational osteotomy
• Elderly: THA or hemiarthroplasty
Subchondral Insufficiency: coronal STIR (A) demonstrates
irregular band parallel to the femoral head. Post-contrast T1
image (B) in a different patient demonstrates femoral head
enhancement

Femoral Neck Fracture:
Mechanism
Caused by fall with applied force to the greater trochanter
High energy impact in younger patients, and low energy impact in elderly patients
Weakest site just below articular surface
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Subcapital, Transcervical,
Basicervical Fractures
TranscervicalTreated as intracapsular fx
BasicervicalTreated as extracapsular fx
e.g. like intertrochanteric fx
SubcapitalTreated as intracapsular fx
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Incomplete
Valgus impaction + retroversionComplete, non-displaced
Marked angulation
Minimal/no proximal translationComplete displacement
Proximal translation
Commonly used classification for
surgical management of femoral
neck fractures
Valgus impacted fractures are
often missed
Good interobserver agreement
between I-II and III-IV, but poor
between all groups
Better to distinguish I-II and III-IV,
as types III and IV typically treated
with arthroplasty
IVIII
I II
Garden Classification
Frandsen PA et al. Acta Orthop Scand 1984; Kreder HJ J Bone Joint Surg AM 2002
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

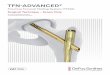
Pauwel Classification
Type IMore stable
Type IIIMore unstable, higher energy injury
Determined by angle of fracture from horizontal plane
Increased shear forces with increased angles worsens prognosis
Better categorizes stability than the Garden Classification
Better predicts difficulty of obtaining stable fixation
More vertically oriented fractures may also require plate fixation
Type III fractures complicated by nonunion may require intertrochanteric osteotomy to reorient the fracture
line to a more Type 1 (stable) angle
Ly TV et al. J Bone Joint Surg Am 2008
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
ReferencesType II
Most common

Types of Stress Fractures
TensileUnstable, fracture can
propagate
CompressiveMore stable
DisplacedUnstable
Worse prognosis and risk for
avascular necrosis
Emergent operation and reduction
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
Femoral neck stress fractures are often related to increased activity. The
pattern of the stress fracture relates to the lines of stress within the
proximal femur and has significant management implications

Tensile Stress FractureSuperior, lateral aspect of the femoral neck
Bimodal distribution: Elderly individuals and young runners
Potentially unstable, obtain MRI to assess fracture extent
Warrants internal fixation (nail fixation in young athletes)
Femoral Neck:
Tensile Stress Fracture
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Femoral Neck:
Tensile Stress Fracture
Tensile stress fracture in the superolateral
femoral neck in an elderly patient. Note
osteoarthritis of the hip.
Tensile stress fracture (Garden III) in the
superolateral femoral neck in a young, active,
patient. Note the normal bone mineral density.
Bimodal distribution: elderly individuals and young runners
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Femoral Neck:
Fatigue Compression Fracture
Fatigue Compression FractureInferior aspect of femoral neck
Active individuals
May potentially be treated non-operatively
Coronal STIR image demonstrates edema at the
inferomedial femoral neck.Coronal T1 image demonstrates a hypointense
region and a subtle fracture line.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Femoral Neck Fractures: Surgical
Considerations
AVN, nonunion may result from delayed diagnosis• Risk for AVN is greater for femoral neck fractures than for pertrochanteric fractures
Young ( < 65) and/or active• Goal: preserve femoral head, avoid osteonecrosis, achieve union
Old ( > 75) and/or immobile• Goal: restore mobility and minimize complications
Fracture pattern determines treatment• Basicervical fracture treated like intertrochanteric fracture
• Nonoperative management associated with higher complication and increased risk of
displacement
• If nondisplaced, internal fixation preferred
• If displaced fracture, elderly, arthroplasty preferred
• Most studies find improved function with THA compared to hemiarthroplasty
Miler BJ et al. J Bone Joint Surg Am 2013; Goh SK et al. J Arthroplasty 2009; Cserhati P et al. Injury 1996
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Femoral Neck Fracture:
Treatment Algorithm
Nondisplaced
Displaced
Total Hip Arthroplasty
Hemiarthroplasty
OldYoung
PC Screw or ArthroplastyPercutaneous Cancellous (PC) Screw
Miler BJ et al. J Bone Joint Surg Am 2013
Open Reduction Internal Fixation
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Intertrochanteric Fracture
Koval KJ et al. J Am Acad Orthop Surg 1994
Nondisplaced Intertrochanteric fracture (Evans I)
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
Anatomy• Intertrochanteric line: anterior ridge between greater and lesser trochanters
• Extracapsular, transition between femoral neck and shaft
• Iliofemoral ligament attaches above, vastus medialis attaches below
Mechanism• Resulting from fall
Unstable features• Loss of medial buttress
• 4-part fractures, and 3-part fractures with
lesser trochanter involvement
• Reverse obliquity
• Comminution
Stable features• Near anatomic reduction achievable
• Lesser trochanter nondisplaced
• Medial cortices in alignment
• No comminution

Evans Classification
Trafton PG. Orthop Clin North Am 1987; Koval KJ et al. J Am Acad Orthop Surg 1994
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References
I II III
Two part, undisplaced
Stable
Two part, displaced
Stable
Three part, posterolateral comminution
Unstable
Three part, posteromedial comminution
Unstable
Four Part
Unstable
Useful for deciding stability and treatment of intertrochanteric fractures. Also, reverse obliquity
fractures are unstable and treated like subtrochanteric fractures
IV V

Intertrochanteric Fracture:
Management
Incomplete• Obtain MRI to ensure fracture not complete
• If incomplete and <50% fracture width,
potentially can treat conservatively
• Risk of fracture completion
Complete• Stable: Dynamic plate and screw
• Unstable or reverse obliquity:
Intramedullary device
Management depends on completeness and stability
Risk of AVN and nonunion less than in femoral neck fractures
Again, basicervical fractures treated like intertrochanteric fractures
Su BW, Orthopedics 2006; Forte ML et al. J Bone Jint Surg Am 2008
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Greater Trochanter Fracture
Anatomy• Greater trochanter is the insertion site for hip
abductors (gluteus medius and minimus) and
external rotators (piriformis, gemelli, obdurators)
Mechanism• Isolated greater trochanter fracture may be related
to impaction from fall, versus avulsion
Imaging• If incomplete, obtain MRI to assess extent of
fracture
Management• Most heal well with nonoperative management
• If significant displacement, then ORIF
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Lesser Trochanter Fracture
Anatomy• Lesser trochanter is attachment site for iliopsoas
Mechanism• Fracture may be due to avulsion
• In the absence of injury, isolated lesser
trochanter fracture is highly suspicious for an
underlying malignancy
Imaging• Obtain MRI to assess extent of fracture
• Evaluate for underlying malignancy
Management• Nondisplaced fractures heal well with
nonoperative management
• If significantly displaced, then ORIF
James SL et al. Eur Radiol 2006
Mildly displaced lateral trochanter fracture
in a patient with prostate cancer and
diffuse blastic metastases. Also note the
extensive periosteal reaction.
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

Subtrochanteric and Proximal Femoral Shaft:
Traumatic Versus Atypical Fractures
Shane E et al. J Bone Miner Res 2010. Park-Wyllie LY et al. JAMA 2011
Atypical FracturesLong-term bisphosphonate usage, o/minimal trauma
ImagingTypically subtrochanteric or femoral shaft
Transverse or short oblique orientation
Lateral beaking (arrow)
Normal bone mineral density
ManagementEvaluate contralateral femur
Treat with ORIF, intramedullary nail and screw0
It is important for the radiologist to recognize the different patterns of traumatic and
atypical subtrochanteric and proximal shaft fracturesDisclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References Typical FracturesOften traumatic, high impact
ImagingRadiographs generally diagnostic
Oblique or spiral in orientation
Proximal piece is flexed, abducted, and externally rotated
MR/CT if concern for pathologic fracture
ManagementORIF
Higher rates of failure due to high stress anatomy

Conclusion
• Proximal femoral fractures can be classified as
femoral head, intracapsular, and extracapsular
• Increased concern for AVN and nonunion for
intracapsular fractures due to vascular compromise
• Important to understand how imaging features reflect
underlying mechanical forces and mechanisms of
injury, and how these in turn guide management
• If a patient has hip pain and negative x-rays, strongly
consider further imaging with MRI
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References

References
• Trueta J, Harrison MH. The normal vascular anatomy of the femoral head in adult man. J Bone Joint Surg Br. 1953;35:442-61
• Ly TV, Swiontkowski MF. Treatment of femoral neck fractures in young adults. J Bone Joint Surg Am. 2008;90:2. 254-66
• Byrne DP et al. The Open Sports Medicine Journal 2010;4;51-7.
• Bowman KF Jr, Fox J, Sekiya JK. A clinically relevant review of hip biomechanics. Arthroscopy 2010;26(8):1118-29.
• Dominguez S, Liu P, Roberts C et al. Prevalence of traumatic hip and pelvic fractures in patients with suspected hip fracture and negative initial
standard radiographs—a study of emergency department patients. Acad Emerg Med 2005;12(4):366-9.
• Frihagen F, Nordsletten L, Tariq R, et al. MRI diagnosis of occult hip fractures. Acta Orthop 2005;76(4):524-30.
• Kirby MW, Spritzer C. Radiographic detection of hip and pelvic fractures in the emergency department. AJR Am J Roentgenol 2010;194(4):1054-60.
• Khurana B, Okanobo H, Ossiani M, et al. Abbreviated MRI for patients presenting to the emergency department with hip pain. AJR Am J Roentgenol
2012;198(6):581-8.
• Ross JR, Gardner MJ. Femoral head fractures. Curr Rev Musculoskelet Med 2012;5(3):199-205.
• Rockwood and Green’s Fractures in Adults, 7th Edition. Wolters Kluwer/Lippincott Williams & Wiilkins, New York, 2010.
• Yamamoto T. Subchondral insufficiency fractures of the femoral head. Clin Orthop Surg. 2012:4(3):173-80.
• Ikemura S, Yamamoto T, Motomura G, et al. MRI evaluation of collapsed femoral heads in patients 60 years old or older: differentiation of subchondral
insufficiency fracture from osteonecrosis of the femoral head. AJR Am J Roentgenol 2010;195:W63-W68.
• Frandsen PA, Andersen PE Jr, Christoffersen H et al. Osteosynthesis of femoral neck fracture. The sliding-screw-plate with or without compression.
Acta Orthop Scand 1984;55(6):620-3.
• Kreder HJ. Arthroscopy led to fewer failures and more complications than did internal fixation for displaced fractures of the femoral neck. J Bone Joint
Surg Am 2002;84:2108.
• Miller BJ, Lu X, Cram P. The Trends in Treatment of Femoral Neck Fractures in the Medicare Population from 1991 to 2008. J Bone Joint Surg Am
2013:95(18):1-8.
• Goh SK, Samuel M, Su DHC et al. Meta-analysis comparing total hip arthroplasty with hemiarthroplasty in the treatment of displaced neck of femur
fracture. J Arthroplasty. 2009:24(13):400-6.
• Koval KJ, Zuckerman JD. Hip fractures, II: evaluation and treatment of intertrochanteric fractures. J Am Acad Orthop Surg 1994;2(3):150-6.
• Trafton PG. Subtrochanteric-intertrochanteric femoral fractures. Orthop Clin North Am 1987;18(1):59-71.
• Su BW, Heyworth BE, Protopsaltis TS et al. Basicervical versus intertrochanteric fractures: an analysis of radiographic and functional outcomes.
Orthopedics 2006;29(10):919-25.
• Forte ML, Vimig BA, Kane RL. Geographic variation in device use for intertrochanteriic hif fractures. J Bone Joint Surg Am 2008;90(4):691-9.
• James Sl, Davies Am. Atraumatic avulsion of the lesser trochanter as an indicator of tumour infiltration. Eur Radiol. 2006;16(2):512-4
• Shane E, Burr D, Ebeling PR et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society of Bone
and Mineral Research 2010; 25(11):2267-94
• Park-Wyllie LY, Mamdani MM, Juurlink DN. Bisphosphonate use and the risk of subtrochanteric or femoral shaft fractures in older women. JAMA
2011;305(8):783-9.
• Tornetta P III. Subtrochanteric femur fracture. J Orthop Trauma 2002;16(4);280-3
Thank You For Viewing Our Exhibit – Jeffrey Shyu ([email protected])
Disclosures
Learning
Objectives
Organization
Anatomy
Imaging
Osteochondral
Subchondral
Femoral Neck
Intertrochanteric
Greater Troch.
Lesser Troch.
Subtrochanteric
Conclusion
References