-
e186 | www.pidj.com The Pediatric Infectious Disease Journal
Volume32,Number5,May2013
Original StudieS
Background: Children with petechial rash are more likely to
undergo inva-sive diagnostics, to be treated with antibiotics for
potential bacterial infec-tion and to be hospitalized. However,
viruses have also been associated with petechial rash. nonetheless,
a systematic analysis of viral infections with modern available
techniques as quantitative real-time polymerase chain reaction in
the context of petechial rash is lacking. the purpose of this
pedi-atric study was to prospectively uncover viral pathogens that
may promote the emergence of petechiae and to analyze the
correlation with the clinical characteristics and course.Methods:
We conducted a prospective study in children (0 to 18 years)
pre-senting with petechiae and signs or symptoms of infection at
the emergency department between november 2009 and March 2012. in
nasopharyngeal aspirates the following viruses were analyzed by
quantitative real-time poly-merase chain reaction: cytomegalovirus,
epsteinBarr virus, parvovirus B19, influenza a and B, parainfluenza
viruses, human respiratory syncytial virus a and B, human
metapneumovirus, rhinovirus, enterovirus, adenovi-rus, human
coronavirus OC43, 229e, nl63 and human bocavirus.Results: a viral
pathogen was identified in 67% of the analyzed 58 cases with
petechial rash. Virus positive patients showed a significantly
higher incidence of lower respiratory tract infections. Forty-one
percent were viral coinfections, which were significantly younger
than virus negative patients, had a higher leukocyte count and were
hospitalized for a longer time.Conclusions: a petechial rash is
frequently associated viral single- and coinfections and can
rapidly be identified via quantitative real-time poly-merase chain
reaction.
Key Words: petechiae, fever, viral infections, management,
polymerase chain reaction
(Pediatr Infect Dis J 2013;32: e186e191)
Petechiae in children often pose a diagnostic dilemma lead-ing
to an enhanced rate of hospitalizations, invasive proce-dures such
as blood sampling for blood cultures, assessment of the
inflammation parameters and lumbar punctures, as well as antibiotic
treatment for possible sepsis or meningitis with bac-teria such as
Neisseria meningitidis.16 in the past, the probabil-
ity of a severe bacteremia in children with petechiae and fever
was estimated at 10% to 20% with the presence of skin hemor-rhages
(diameter >2 mm) as a risk factor.2,3,5,6 in up to 72% of the
patients with fever and a petechial rash, no causing pathogen was
identified, whereas viruses were only identified in 11% to 15% of
the cases.2
Human respiratory syncytial virus (rSV), epsteinBarr virus
(eBV), cytomegalovirus (CMV), adenovirus, enterovirus (eV) and
parvovirus B19 are reported to be associated with a pete-chial
rash. the proportion of viral infections in children with
pete-chiae and fever is understated.2,711 additionally, currently
avail-able studies on children with a petechial rash (with the most
recent being performed in 2001) noted an association between
evolve-ment of petechiae in children and upper respiratory tract
infec-tions (urtis) commonly caused by so called respiratory
viruses as influenza types (inf) a, B and H1n1, parainfluenza type
1, 2 and 3, rSV, rhinovirus (rV), eV and adenovirus.3,1214
Moreover, previously unknown viruses as human metapneumovirus,
human coronavirus and human bocavirus (HBoV) associated with urti
and specific viral diagnostics have been discovered recently.1420
it is now possible to specifically detect viruses within hours with
nucleic acid amplification tests as quantitative real-time
polymer-ase chain reaction (q-PCr).3,15 Modern viral diagnostics
might help further itemize the 45% of urti in children with a
petechial rash as systematic analysis of the presence of viral
pathogens in children with petechiae is lacking.2 the main aim of
the study was to analyze prospectively the rate of viral (single
and co-) infec-tions in children with a petechial rash applying
q-PCr techniques of nasopharyngeal aspirates (nPas), to identify
viruses associated with the emergence of petechiae and to correlate
them with disease severity.
MATERIALS AND METHODS
Study Populationthe prospective clinical study was performed
from novem-
ber 2009 to March 2012 at the university Childrens Hospital
Mannheim, Heidelberg university and the Childrens Hospital St.
annastiftkrankenhaus in ludwigshafen. identification and
recruit-ment of patients was made by the responsible physician in
the emergency department or the unit within the hospital after
admis-sion. We included children between 0 and 18 years presented
with a nonblanching rash not greater than 2 mm in diameter of
unknown origin with signs and symptoms of an ongoing infection.
Patients with thrombocytopenia, preexisting coagulation disorder,
clinical vasculitis (purpuric lesion with a diameter of >2 mm),
meningo-coccal disease or with primary or secondary immune
dysfunction were excluded. Clinical data were prospectively
collected using a standard data collection form. additional
diagnostics apart from nasopharyngeal aspirates (nPa) as chest
radiogram, blood sam-pling for laboratory parameters or blood
cultures, analysis of the urine or lumbar puncture were not a study
requirement. results of additional diagnostics were documented and
analyzed within the study when available.
Copyright 2013 by lippincott Williams & WilkinsiSSn:
0891-3668/13/3205-0e186dOi: 10.1097/inF.0b013e318280618d
ClinicalCharacteristicsofChildrenWithViralSingle-and
Co-infectionsandaPetechialRash
Henriette Schneider, MD,* Ortwin Adams, MD, Christel Weiss, ScD,
Ulrich Merz, MD, Horst Schroten, MD,* and Tobias Tenenbaum, MD*
accepted for publication november 28, 2012.From the *Paediatric
infectious diseases, university Childrens Hospital
Mannheim, Heidelberg university, Mannheim, germany; institute of
Virol-ogy, university Childrens Hospital,
Heinrich-Heine-university, dsseldorf, germany; department of
Statistics, Medical Faculty Mannheim, Heidel-berg university,
Mannheim, germany; and Childrens Hospital St.
annas-tiftkrankenhaus, ludwigshafen, germany.
H.S. and O.a. contributed equally to this article and share
first authorship.the concept of the study was honored in 2011 by
the german Society of Paediat-
ric infectious diseases (dgPi) with an investigator award (5000
euro). the authors have no other funding or conflicts of interest
to disclose.
address for correspondence: Henriette Schneider, Md, Paediatric
infectious diseases, university Childrens Hospital Mannheim,
Heidelberg university, theodor-Kutzer-ufer 13, 68167 Mannheim,
germany. e-mail: [email protected].
the Pediatric infectious disease Journal
32
5
Copyright 2013 by lippincott Williams & Wilkins
0891-3668
inF
203077
Viral infections and Petechial rash
Schneider et al
2013
May
00
00
10.1097/inF.0b013e318280618d
2013
Pediatr infect dis J
lippincott Williams & Wilkins
Hagerstown, Md
divya J
XXX
-
The Pediatric Infectious Disease Journal
Volume32,Number5,May2013 Viral Infections and Petechial Rash
2013 Lippincott Williams & Wilkins www.pidj.com | e187
Ethical Statementapproval was provided by the local ethics
committees (Med-
ical Faculty of Mannheim, Heidelberg university [2009-323n-Ma]
and Mainz [837.021.10 (7030)]). Written informed consent was
obtained from parents and children (when possible according to
their age) before any study procedures being performed.
Analysis of Nasopharyngeal AspiratesOn the day of admission or
detection of petechial rash, nPas
were collected and evaluated in the institute of Virology in
dssel-dorf with q-PCr for CMV, eBV, parvovirus B19, inf a and B,
inf a H1n1 (H1n1), parainfluenza 1, 2 and 3, rSV a and B, human
metapneumovirus, rV, eV (coxsackie a and B viruses and echo-viruses
except for polioviruses 13), adenovirus, human corona-virus and
HBoV. the quantification of the viruses was performed by a
previously described 1-step real-time PCr method of which
sensitivity and specificity have been demonstrated
elsewhere.14,2123 in brief, the Quantitect Multiplex q-PCr kit (no.
204643, Qiagen, Hilden, germany) containing HotStartaq dna
Polymerase was used for the assay. amplification was performed in
an aBi7500 thermocycler using conditions as recommended by the
manufac-turer of the multiplex rt-PCr kit. as standards, dna
plasmids that encompass the amplified region were created and
serially diluted after purification. Standard graphs of the CT
values obtained from serial dilutions of the standards were
constructed and the numbers of specific genomes were calculated by
the software. nPa as a method for the detection of a viral
infection was chosen as non-invasive procedure, of which reference
values for the viral load in copies per milliliter (ml) of
respiratory viruses exist.21 in cases in which lumbar puncture was
performed, the cerebrospinal fluid was send for bacterial culture
and analyzed with a standard commer-cial multiplex PCr (reverse
Hybridization assay kit CnS, labo Bio-Medical Products B.V., the
netherlands) for herpes simplex virus type 1, herpes simplex virus
type 2, eV, CMV, varicella zoster virus, eBV, human John Cunningham
virus, human herpes virus type 6 and Toxoplasma gondii.
StatisticsQualitative variables are presented as absolute and
rela-
tive frequencies; quantitative parameters are given as mean and
standard deviation or median and range. Clinical characteristics
and laboratory variables have been compared using t tests of the
pooled method (identical variances) and Satterthwaite method
(dif-fering variances). For skewed distributed quantitative data,
MannWhitney U test has been performed. to compare frequencies of 2
samples, test or Fishers exact test has been used, for ordinal
scaled data Cochranarmitage trend test was preferred. a 2-sided P
value 100 petechiae (P = 0.0247) between virus positive and virus
negative patients (table 1). the distribution of petechiae did not
differ sig-nificantly in virus positive and negative patients.
Blood samples were taken in the majority of the analyzed
children (45/58; 78%) to examine full blood cell count and the C
reactive protein value (14 virus negative and 31 virus positive
patients) and revealed no significant difference between virus
posi-tive and virus negative patients (table 2). Blood cultures
were only analyzed in hospitalized children without any antibiotic
treatment before admission. in 3 of 38 blood culture samples (8%),
bacteria were detected (Flavimonas oryihabitans, Streptococcus
agalac-tiae and coagulase negative staphylococci each in 1
patient). Only the patient with proven S. agalactiae infection
received antibiotic treatment.
Identification of Viral Causes in Children With a Petechial
Rash
in 39 of the 58 patients analyzed during the study period, at
least 1 virus was detected within the nPa. the majority were single
viral infections (23/39; 59%) whereas coinfections with 2 pathogens
were as frequent as coinfections with >2 pathogens (each 8/39;
20.5%). Children with viral coinfections were signifi-cantly
younger (2.3 2.16 years) than the children with a single viral
infection (4.18 3.26 years) (P = 0.0440) (data not shown).
Coinfections led to a significant higher hospitalization rate
(15/16; 93.75%) compared with virus negative patients (12/19; 63%;
P = 0.0472) (data not shown). interestingly, children with viral
coinfections presented with a significant higher leukocyte count
(12641 3274/l) compared with virus negative (8455 3155/l; P =
0.0063) and single viral infections (9393 4780/l; P = 0.0642) (data
not shown).
the most frequent pathogens in association with a petechial rash
were CMV and eBV (each 11/58; 18% of all patients) fol-lowed by eV
and rV (each 8/58; 14% of all patients) and H1n1 and HBoV (each
5/58; 9% of all patients). eBV and CMV were frequently found as
coinfections (only 1 single infection with eBV and CMV within the
study collective). ten of 11 CMV positive patients (91%) and 9 of
11 eBV positive patients (82%) were hospitalized. CMV positive
patients were with 2.07 2.53 years younger than virus negative
(4.19 3.84 years; P = 0.01108) and
-
Schneider et al The Pediatric Infectious Disease Journal
Volume32,Number5,May2013
e188 | www.pidj.com 2013 Lippincott Williams & Wilkins
CMV negative (4.57 4.88 years; P = 0.0208) patients. as to the
laboratory findings, the CMV positive patients showed elevated
platelet counts (297970 99617/l) compared with the CMV neg-ative
patients (251142 70249/l; P = 0.0818) and a significant
leukocytosis (13630 3337/l) compared with the CMV nega-tive (8455
3155/l; P = 0.0109) and all virus negative patients (9251 3979/l; P
= 0.0043). Moreover, the eBV positive patients showed a
significantly higher rate of lymphadenitis (3/11; 27%) compared
with eBV negative patients (1/47; 2%; P = 0.0191) and virus
negative patients (0/19; 0%; P = 0.0406). eV was detected in 5
cases as single and in 3 cases as coinfection. the eV positive
patients were likely to present in summer (5/8; 63%) compared with
eV negative patients (6/50; 12%; P = 0.0164) and 3 of 5
patients
(60%) received a lumbar puncture for neurological symptoms as
febrile seizures, meningism or even meningitis. the majority of rV
positive patients (7/8; 87.5%) was hospitalized. nine (23%) of the
39 virus positive patients were well appearing, treated as
outpa-tients without antibiotics and scheduled for a clinical
control on the consecutive days despite a high number of petechiae
(6/67% had around 100 petechiae).
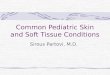
PCr-positive samples could qualitatively clearly be
distin-guished from negative samples with mean viral loads ranging
from 438 103 for coronavirus to 805 109 for adenovirus (Fig. 1),
but it should be emphasized that there exist no clear cutoffs for
clinical significant values for respiratory virus infections.
especially adeno-virus, rSV and HBoV were found with a high viral
load.
TABLE 2. Laboratory Findings in Children With or Without a Viral
Infection and Petechial Rash
All Patients Positive Patients Negative Patients P
Total number 58 39 19Hemoglobin (g/dL) 12 1 12 1 12 2
0.7886Thrombocytes (/L) 257,556 82,567 260,197 87,981 25,1143
70,250 0.9614Leukocytes (/L) 10,080 4200 10,767 4446 8455 3155
0.5775Segmented neutrophils* 38 24 39 24 36 29 0.4302Banded
neutrophils* 10 19 9 20 14 16 0.7628Lymphocytes* 35 23 36 21 33 30
0.7720Monocytes* 8 6 9 7 6 3 0.2971C reactive protein (mg/L) 23 34
20 25 31 49 0.9393INR 1.07 0.11 1.07 0.12 1.06 0.08 0.5735Ptt (s)
29 8 30 9 25 7 0.0638
*% of total leukocytes.
TABLE 1. Clinical Characteristics of All Patients, Virus
Positive and Negative Patients With Petechiae
All Patients Positive Patients Negative Patients P
Total number 58 39 19Age (yr) 3.8 3.7 3.4 3.0 4.6 4.9
0.7972Gender Male 41 (71%) 26 (67%) 15 (79%) 0.3349 Female 17 (29%)
13 (33%) 4 (21%)Number of petechiae 100 14 (24.6%) 6 (15%) 8 (45%)
0.0247Symptoms Coughing 28 (48%) 21 (54%) 7 (37%) 0.2239 Vomiting
16 (28%) 11 (28%) 5 (26%) 0.8799 Diarrhea 14 (24%) 11 (28%) 3 (16%)
0.3495 Meningism 7 (12%) 4 (10%) 3 (16%) 0.6726 Swelling of joints
2 (3%) 1 (3%) 1 (5%) 1 Maximal temperature (C) at admission 38.3 1
38.8 1 38.5 1.3 0.8737Diagnosis URTI 20 (34%) 13 (33%) 7 (37%)
0.7919 Bronchitis 8 (14%) 8 (21%) 0 (0%) 0.0437 Pneumonia 2 (3%) 0
(0%) 2 (11%) 0.1034 Gastroenteritis 11 (19%) 8 (21%)* 3 (16%) 1
Lymphadenitis 4 (7%) 4 (10%) 0 (0%) 0.2921 Febrile seizure 3 (5%) 3
(8%) 0 (0%) 1 Meningitis 2 (3%) 1 (3%) 1 (5%) 1 Presumed sepsis 5
(9%) 2 (5%) 3 (17%) 0.3125 Others 14 (24%) 8 (21%) 6 (32%)
0.5141Invasive diagnostics Lumbar puncture 10 (17%) 5 (13%) 5 (26%)
0.2704Therapeutic strategies Antibiotics 17 (29%) 11 (28%) 6 (32%)
0.7911 Hospitalization rate 42 (72%) 30 (77%) 12 (63%) 0.271
*Of the patients with diarrhea, 4 were positive for an enteric
virus (2 norovirus and 2 rotavirus).In 1 of the patients with
presumed sepsis, blood cultures were positive for S. agalactiae.Of
the patients who underwent a lumbar puncture, 1 of the virus
positive and 2 of the virus negative patients underwent lumbar
puncture for their young age
-
The Pediatric Infectious Disease Journal
Volume32,Number5,May2013 Viral Infections and Petechial Rash
2013 Lippincott Williams & Wilkins www.pidj.com | e189
Central Nervous System Symptoms in Children With Petechial
Rash
as to central nervous system symptoms, 7 of the 58 (12%)
presented with nuchal rigidity and 3 of the 58 (5%) with a febrile
seizure. ten children (17%) received a lumbar puncture at
admission. in 5 out of these, a virus was detected in the nPa (1
coinfection of H1n1, CMV, eBV and eV, 1 coronavirus, 2 single
infections with eV and 1 coinfection of parainfluenza and CMV). all
7 children with meningism were hospitalized. Four of them (2 virus
positive and 2 virus negative within the nPa) were treated with
antibiotics. additionally, 4 children underwent lumbar puncture due
to the presence of a petechial rash in combination either with
their young age 2 mm were excluded from the study as they seem more
likely to suffer from meningococcal disease.6 Main aim was to
estimate the amount of viral pathogens within the nasopharynx
measured with q-PCr analysis in the context of a petechial rash
with a noninvasive procedure for which information about the viral
load in disease exit. in 67% of the included patients, 1 or several
viral pathogens have been detected. the viral loads in the nPa for
the different viruses in this study (Fig. 1) were comparable to
described viral loads for infections with respiratory viruses
either in single or in coinfections and in a higher range than
viral loads in healthy children.21,26 Still, there is no consensus
in the literature on clinical significant values for respiratory
infections. as a result of low case numbers for each pathogen viral
load results have to be interpreted with caution. For rV, a
previous prospective study with healthy children has shown that
shedding of picornavirus rna was episodic with positive q-PCrs for
1 to 3 weeks followed by weeks of negative tests; chronic carriage
did not occur.27 the mean viral load of the rV samples in our study
was with 136 105 copies/ml equal or higher than viral loads found
with other viruses (ie, influenza or parainfluenza) indicating that
the detection of rV may be associated with an acute infection.
Otherwise it cannot com-pletely be excluded that in some cases we
detected rV rna from a previous episode of infection. Concerning
herpesviruses (CMV and eBV), a critical point with the detection is
the long lasting oral shedding after primary infection. in adults,
CMV and eBV can be detected in 10%20% of asymptomatic individuals
and is assumed to be more frequent during childhood.28
Consequently, a combi-nation of q-PCr of nPa with a serological
analysis may help to differentiate between acute viral infection
and reactivation. as our study was meant to apply as few additional
invasive diagnostics in the children as possible, serological
correlation with the findings, which was part of the study design,
was not always possible. this might limit the interpretation of the
study. Blood culture sampling
FIGURE 1. Meanviral loaddetectedinchildrenwithviral
infectionsandpetechialrash.Thehighestviral
loadvaluesweredetectedinchildrenwithadenovirus(AV),RSVandHBoVinfections.PVB19indicatesparvovirusB19;hMPV,humanmetap-neumovirus;HCoV,humancoronavirus;Para,parainfluenza.
-
Schneider et al The Pediatric Infectious Disease Journal
Volume32,Number5,May2013
e190 | www.pidj.com 2013 Lippincott Williams & Wilkins
was performed in the hospitalized patients without prior
antibiotic treatment (38/58; 66%) and revealed only 1 clinically
relevant case of bacterial blood stream infection (S. agalactiae)
in the study pop-ulation.
Between virus negative and virus positive patients with a
petechial rash, there were no significant differences in clinical
appearance, cardinal symptoms, diagnostic parameters, treat-ment
and hospitalization rate despite the higher rate of
bronchitis/bronchiolitis in virus positive patients and the number
of pete-chiae (table 1). Patients with viral coinfections were
significantly younger than virus negative patients, had a higher
leukocyte count and were longer hospitalized.
interestingly, within the small subgroup of patients with
central nervous system symptoms (10 patients), virus positive
patients displayed the petechial rash in a more generalized fashion
(head: 3/5; 60%; upper extremities: 2/5; 40%; trunk: 4/5; 80% and
the lower extremities: 3/5; 60%), whereas in virus negative
patients the rash was centered on the trunk (2/5; 40%) and lower
extremities (3/5; 60%).
in previous studies, authors suggested to combine the clini-cal
criteria general appearance and skin lesion (either petechiae or
purpuric lesions) with the WBC to detect children with bacterial
sepsis whereas viral pathogens were not investigated due to
compli-cated virus diagnostics.4,15 applying these criteria (either
general appearance, WBC and skin lesions or irritability, lethargy
and low capillary refill) to our study population, all children
with viral coinfections fulfill the criteria for bacterial
septicemia/bacteremia and would receive an antibiotic treatment at
least until bacterial cultures were proven negative.4,12 thus, our
study provides evidence that also viral infections can lead to a
reduced clinical appearance and an elevated WBC. due to efficient
vaccination programs within europe and the united States, herd
immunity and herd protection against Streptococcus pneumoniae, N.
meningitidis and Haemophi-lus influenzae improved.2932
Consequently, the use of the clinical and diagnostic criteria (see
above) set the era before the availabil-ity of elaborate viral
diagnostics as q-PCr and before the imple-mentation of directed
vaccination programs might lead nowadays in europe and the united
States to an overestimation of bacterial infections in such
children with a petechial rash.3,4,12 additional studies have to
further clarify whether rather the infection with a specific
pathogen or coinfections with different viruses determine the
appearance of a petechial rash in children.
in our study, 17 (11 virus positive and 6 virus negative)
children in total were treated with antibiotics due to suspicion of
potential bacterial infection and/or young age. in the 11 virus
posi-tive patients (8 viral single and 3 coinfections), viral
infection fully accounted for the symptoms they presented and
antibiotic treatment might have been dispensable. there is strong
discordance about the suitable treatment for children with a
petechial rash that are in a good general state of health and young
aged children are more likely to be treated with antibiotics or to
be admitted to hospital for a petechial rash even when their
clinical condition is not reduced1,13
Petechial rash in children needs thorough examination to
distinguish between life threatening diagnosis as fulminant sepsis
and self-limiting viral infection. novel viral diagnostics as
multi-plex q-PCr enables the rapid detection of viral causes and
might avoid unnecessary antibiotic treatment, invasive diagnostics
and hospitalizations.
ACKNOWLEDGMENTSWe are grateful for the support offered by the
staff of the
2 childrens hospitals, the University Childrens Hospital
Man-nheim, Germany Heidelberg University and the Childrens
Hospi-tal St. Annastiftkrankenhaus in Ludwigshafen, Germany, and
the
members of the working group of Prof. O. Adams in the Institute
of Virology, University Childrens hospital,
Heinrich-Heine-Univer-sity, Dsseldorf, Germany.
REFERENCES 1. nelson dg, leake J, Bradley J, et al. evaluation
of febrile children with
petechial rashes: is there consensus among pediatricians?
Pediatr Infect Dis J. 1998;17:11351140.
2. Baker rC, Seguin JH, leslie n, et al. Fever and petechiae in
children. Pedi-atrics. 1989;84:10511055.
3. nielsen He, andersen ea, andersen J, et al. diagnostic
assessment of haemorrhagic rash and fever. Arch Dis Child.
2001;85:160165.
4. Mandl Kd, Stack aM, Fleisher gr. incidence of bacteremia in
infants and children with fever and petechiae. J Pediatr.
1997;131:398404.
5. Van nguyen Q, nguyen ea, Weiner lB. incidence of invasive
bacterial dis-ease in children with fever and petechiae.
Pediatrics. 1984;74:7780.
6. Wells lC, Smith JC, Weston VC, et al. the child with a
non-blanching rash: how likely is meningococcal disease? Arch Dis
Child. 2001;85: 218222.
7. Coffin Se, gest Kl, Shimamura a. respiratory syncytial virus
as a cause of fever and petechiae in infants. Clin Pediatr (Phila).
1993;32: 355356.
8. Sahler OJ, Wilfert CM. Fever and petechiae with adenovirus
type 7 infec-tion. Pediatrics. 1974;53:233235.
9. deVries J. the aBCs of CMV. Adv Neonatal Care. 2007;7:248255;
quiz 256.
10. elling r, Hufnagel M, Henneke P. infektionsassoziierte
Hauteinblutungen. Monatsschr Kinderheilkd. 2012;160:111.
11. Mcneely M, Friedman J, Pope e. generalized petechial
eruption induced by parvovirus B19 infection. J Am Acad Dermatol.
2005;52(5 suppl 1): S109S113.
12. Brogan Pa, raffles a. the management of fever and petechiae:
making sense of rash decisions. Arch Dis Child. 2000;83:506507.
13. legg JP, Warner Ja, Johnston Sl, et al. Frequency of
detection of picornavi-ruses and seven other respiratory pathogens
in infants. Pediatr Infect Dis J. 2005;24:611616.
14. Bonzel l, tenenbaum t, Schroten H, et al. Frequent detection
of viral coin-fection in children hospitalized with acute
respiratory tract infection using a real-time polymerase chain
reaction. Pediatr Infect Dis J. 2008;27:589594.
15. Mahony JB. detection of respiratory viruses by molecular
methods. Clin Microbiol Rev. 2008;21:716747.
16. van den Hoogen Bg, de Jong JC, groen J, et al. a newly
discovered human pneumovirus isolated from young children with
respiratory tract disease. Nat Med. 2001;7:719724.
17. Peiris JS, lai St, Poon ll, et al.; SarS study group.
Coronavirus as a possible cause of severe acute respiratory
syndrome. Lancet. 2003;361: 13191325.
18. Viazov S, ratjen F, Scheidhauer r, et al. High prevalence of
human metap-neumovirus infection in young children and genetic
heterogeneity of the viral isolates. J Clin Microbiol.
2003;41:30433045.
19. allander t, Jartti t, gupta S, et al. Human bocavirus and
acute wheezing in children. Clin Infect Dis. 2007;44:904910.
20. allander t, tammi Mt, eriksson M, et al. Cloning of a human
parvovirus by molecular screening of respiratory tract samples.
Proc Natl Acad Sci USA. 2005;102:1289112896.
21. Franz a, adams O, Willems r, et al. Correlation of viral
load of respiratory pathogens and co-infections with disease
severity in children hospitalized for lower respiratory tract
infection. J Clin Virol. 2010;48:239245.
22. Klein rM, Jiang H, niederacher d, et al. Frequency and
quantity of the parvovirus B19 genome in endomyocardial biopsies
from patients with suspected myocarditis or idiopathic left
ventricular dysfunction. Z Kardiol. 2004;93:300309.
23. Schnberger S, Meisel r, adams O, et al. Prospective,
comprehensive, and effective viral monitoring in children
undergoing allogeneic hematopoi-etic stem cell transplantation.
Biol Blood Marrow Transplant. 2010;16: 14281435.
24. Soheilifar J, ahmadi M, ahmadi M, et al. Prevalence and
location of pete-chial spots in well infants. Arch Dis Child.
2010;95:518520.
25. downes aJ, Crossland dS, Mellon aF. Prevalence and
distribution of pete-chiae in well babies. Arch Dis Child.
2002;86:291292.
-
The Pediatric Infectious Disease Journal
Volume32,Number5,May2013 Viral Infections and Petechial Rash
2013 Lippincott Williams & Wilkins www.pidj.com | e191
26. Jansen rr, Wieringa J, Koekkoek SM, et al. Frequent
detection of respiratory viruses without symptoms: toward defining
clinically relevant cutoff values. J Clin Microbiol.
2011;49:26312636.
27. Winther B, Hayden Fg, Hendley JO. Picornavirus infections in
children diagnosed by rt-PCr during longitudinal surveillance with
weekly sam-pling: association with symptomatic illness and effect
of season. J Med Virol. 2006;78:644650.
28. Frana trt, albuquerque tavares Carvalho a, gomes VB, et al.
Salivary shedding of epsteinBarr virus and cytomegalovirus in
people infected or not by human immunodeficiency virus 1. Clin Oral
Invest. 2011;16:659664.
29. ardanuy C, tubau F, Pallares r, et al. epidemiology of
invasive pneumo-coccal disease among adult patients in barcelona
before and after pediatric
7-valent pneumococcal conjugate vaccine introduction, 1997-2007.
Clin Infect Dis. 2009;48:5764.
30. Pollard aJ, Perrett KP, Beverley PC. Maintaining protection
against invasive bacteria with protein-polysaccharide conjugate
vaccines. Nat Rev Immunol. 2009;9:213220.
31. ladhani Sn, ramsay M, Slack MP. the impact of Haemophilus
influen-zae serotype B resurgence on the epidemiology of childhood
invasive Hae-mophilus influenzae disease in england and Wales.
Pediatr Infect Dis J. 2011;30:893895.
32. trotter Cl, gay nJ, edmunds WJ. dynamic models of
meningococcal car-riage, disease, and the impact of serogroup C
conjugate vaccination. Am J Epidemiol. 2005;162:89100.