Embed Size (px)
Citation preview

18 The Somatosensory System II: Touch, Thermal Sense, and
Pain
Suhail Abdulla AlRukn
18-3-2008

Out-line
• ObjectiveObjective• TestTest• Main Sensory PathwayMain Sensory Pathway• Sensory dysfunctionSensory dysfunction• Anterolateral SystemAnterolateral System• Peripheral Sensitization and Central Peripheral Sensitization and Central
SensitizationSensitization• Spinal Trigeminal PathwaySpinal Trigeminal Pathway

Objectives
• Define the main pathway for the Define the main pathway for the – Anterolateral pathwayAnterolateral pathway
– Spinal Trigeminal PathwaySpinal Trigeminal Pathway
• The mechanism of peripheral Vs The mechanism of peripheral Vs centrat sensitisationcentrat sensitisation

Test
• What are the main sensory pathways (body and face), what function, and where it cross?

Main Sensory Pathway
Posterior Column-madial lemniscal pathway
Vib, joint position, fine touch
Internal arcuate fibers (lower medulla)
Anterolateral pathway
Pain, Temp, crude touch
Anterior commissure (spinal cord)

• Anterolateral system (ALS):– Crude touch– Thermal sanitation– Pain
• Anterior Trigeminothalamic pathway (Spinal (Spinal
Trigeminal Pathway): Trigeminal Pathway):
– Crude touch– Thermal sanitation– Pain
Trunk, limbs, back of the
head
Face and from of the head

Anterolateral Anterolateral system and system and
anterior anterior trigeminothalamic trigeminothalamic
PathwayPathway

ALS Vs post. Colum pathways:ALS Vs post. Colum pathways:
(1) Generalized feeling of being touched (1) Generalized feeling of being touched but do not give precise localization, but do not give precise localization,
(2) Receptive fields are larger, (2) Receptive fields are larger,
(3) Fibres are smaller in diameter and (3) Fibres are smaller in diameter and more slowly conducting. more slowly conducting.

Peripheral Sensory and Motor Fibers: Groups, Diameters, and Conduction Velocities
ElectrophysiolElectrophysiologic ogic Classification Classification of Peripheral of Peripheral NervesNerves
Classification of Classification of Afferent Fibers ONLY Afferent Fibers ONLY
(Class/Group)(Class/Group)
Fiber Fiber Diameter Diameter
(μm)(μm)
Conduction Conduction Velocity Velocity
(m/s)(m/s)Receptor Receptor SuppliedSupplied
Sensory Fiber TypeSensory Fiber Type
AαAα Ia and IbIa and Ib 13-2013-20 80-12080-120 Primary muscle Primary muscle spindles, Golgi tendon spindles, Golgi tendon organorgan
AβAβ IIII 6-126-12 35-7535-75 Secondary muscle Secondary muscle spindles, skin spindles, skin mechanoreceptorsmechanoreceptors
AδAδ IIIIII 1-51-5 5-305-30 Skin Skin mechanoreceptors, mechanoreceptors, thermal receptors, and thermal receptors, and nociceptorsnociceptors
CC IVIV 0.2-1.50.2-1.5 0.5-20.5-2 Skin Skin mechanoreceptors, mechanoreceptors, thermal receptors, and thermal receptors, and nociceptorsnociceptors


Sensory dysfunction• Hypesthesia: reduced sensibility, • Paresthesia: numbness, tingling, and prickling,
• Anesthesia loss of sensibility. • Allodynia: an innocuous stimulus will result in a
perception of pain in the absence of a proper pain stimulus.
• Hyperalgesia: is a heightened sensitivity to painful stimuli

Anterolateral System
• spinothalamic fibers
• spinomesencephalic fibers
• spinoreticular fibers
• spinobulbar fibers
• spinohypothalamic fibers

• Spinothalamic fibers project directly from the spinal cord to the ventral posterolateral (VPL) nucleus
• Spinomesencephalic axons project to the periaqueductal area and to the tectum; the latter are spinotectal fibers. Play role in central modulaton of pain.
• Spinoreticular tract: carried the emotional and arousal aspect of pain.
Anterolateral System

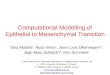
Figure 18-1 Summary Figure 18-1 Summary of anterolateral of anterolateral system and anterior system and anterior trigeminothalamic trigeminothalamic tract fibers conveying tract fibers conveying nondiscriminative nondiscriminative tactile, thermal, and tactile, thermal, and nociceptive inputs to nociceptive inputs to the contralateral the contralateral somatosensory somatosensory cortex. cortex.

Figure 18-1 Summary Figure 18-1 Summary of anterolateral of anterolateral system and anterior system and anterior trigeminothalamic trigeminothalamic tract fibers conveying tract fibers conveying nondiscriminative nondiscriminative tactile, thermal, and tactile, thermal, and nociceptive inputs to nociceptive inputs to the contralateral the contralateral somatosensory somatosensory cortex. cortex.

To summarize
• If you step on a sharp object with your left foot, your spinothalamic tract enables you to realize “something sharp is puncturing the sole of my left foot”.
• Your spinothalamic intralaminar projections and spinoreticular tract cause you to feel “ouch, that hurts!”;
• And your spinomesencephalic tract leads to pain modulation, allowing you eventually to think “aah, that feels better”.

Peripheral Sensitization and Primary Hyperalgesia
• Following an insult, Following an insult, – pain receptors become more sensitive pain receptors become more sensitive – lower pain thresholdlower pain threshold– increases in firing rate to noxious stimulation. increases in firing rate to noxious stimulation.
• So there will be So there will be increase in spontaneous activity in increase in spontaneous activity in the Aδ and C fibersthe Aδ and C fibers..
• Although the mechanisms responsible for receptor Although the mechanisms responsible for receptor sensitization are not completely known, chemicals sensitization are not completely known, chemicals released by the damaged skin or by products from released by the damaged skin or by products from plasma, or both, are thought to contribute to this plasma, or both, are thought to contribute to this phenomenon. phenomenon.

• As a result of this heightened sensitivity, the As a result of this heightened sensitivity, the affected area is super-sensitive to painful stimuli affected area is super-sensitive to painful stimuli and patients experience and patients experience hyperalgesiahyperalgesia..
• Primary hyperalgesiaPrimary hyperalgesia: : occurs in the region of occurs in the region of damaged skin and is probably the result of damaged skin and is probably the result of receptor sensitization. receptor sensitization.
• An example of primary hyperalgesia is the extreme An example of primary hyperalgesia is the extreme sensitivity of sunburned skin, which results from sensitivity of sunburned skin, which results from sensitization of the skin pain endings by local tissue sensitization of the skin pain endings by local tissue products from the burn-perhaps histamine, products from the burn-perhaps histamine, prostaglandins, and othersprostaglandins, and others
Peripheral Sensitization and Primary Hyperalgesia

Central Sensitization and Central Sensitization and Secondary Hyperalgesia Secondary Hyperalgesia
• Secondary hyperalgesia occurs in the skin Secondary hyperalgesia occurs in the skin bordering the damaged tissue. Although bordering the damaged tissue. Although receptor sensitization may contribute to receptor sensitization may contribute to secondary hyperalgesia, there is likely to be secondary hyperalgesia, there is likely to be a central (e.g., spinal) component as well. a central (e.g., spinal) component as well.
• There is hyper-activation of the cell in the There is hyper-activation of the cell in the posterior horn. posterior horn.

• This could be explain by:This could be explain by:– increase in the receptive field size of the posterior increase in the receptive field size of the posterior
horn neuron horn neuron – an increased response of the cells to the an increased response of the cells to the
application of suprathreshold stimuli, application of suprathreshold stimuli,
• This phenomenon is known as central This phenomenon is known as central sensitization, and it represents a potentiated sensitization, and it represents a potentiated state in which the system has been shifted state in which the system has been shifted from one functional level (normal) to another from one functional level (normal) to another (sensitized) by a change in transcription. (sensitized) by a change in transcription.
Central Sensitization and Central Sensitization and Secondary Hyperalgesia Secondary Hyperalgesia

Pain Receptors in Muscles, Joints, and Viscera
• In addition to the cutaneous pain receptors, pain receptors in muscles, joints, and viscera have also been identified, which are also carried by III and IV afferent fibers type.
• A pinprick exam usually activates Aδ fibers.
• Dull, persistent ache that follows a muscle pull results from activation of C fibers.

Dermatom of Dermatom of the body the body and faceand face

Central Pathways
• Aδ and C fibers enter the spinal cord via the lateral division of the posterior root entry zone. The fibers enter the posterolateral fasciculus (Lissauer tract) and bifurcate into ascending and descending branches


Summary of posterior horn laminae and their major sensory inputs (A) and major outputs (B).

• When Aδ fibers enter the posterolateral fasciculus and bifurcate, their branches travel rostrocaudally for three to five spinal levels.
• The descending branches terminate on interneurons within the spinal gray that participate in segmental spinal reflexes.
Central Pathways


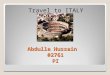
The general somatotopic arrangement of the anterolateral system

ARM
Trunk
LEG
Somatotopically Arrange Somatotopically Arrange
ALS
CST
DCT

• The ascending branches terminate on second-order neurons (tract cells) in lamina I of the posterior horn (Fig. 18-7A). These tract cells, in turn, project to the thalamus.
• The great majority of their axons cross the midline of the spinal cord obliquely via the anterior (ventral) white commissure and ascend in the contralateral ALS.
• A few ascend in the ipsilateral ALS. • The thalamic (third-order) neurons of these
pathways are located mainly in the VPL, the posterior nucleus, and the intralaminar nuclei.

The anterolateral
system

Blood supply to the anterolateral
system in the spinal cord and
medulla

Brown-Séquard syndrome
• (1) contralateral loss of pain and thermal sensations over the body below the level of the lesion
• (2) ipsilateral loss of discriminative tactile, vibratory, and position sense over the body below the level of the lesion
• (3) ipsilateral paralysis of the leg or leg and arm, depending on the level of the hemisection.

Brown-Séquard syndrome

Cervical syringomyelia

Summary of the spinocervicothala
mic tract that carries innocuous
discriminative tactile, thermal, and nociceptive
sensations.

Spinal Trigeminal Pathway: Anterior Trigeminothalamic Tract

Spinal Trigeminal Pathway: Anterior Trigeminothalamic Tract
• Cranial nerves V, VII, IX, and X serve the cutaneous receptors of the face, the oral cavity.
• The primary sensory fibers of these nerves have their cell bodies in the:– Trigeminal ganglion, – Geniculate ganglion of cranial nerve VII, – Superior ganglia of cranial nerves IX and X.

Anterior Trigeminothalamic Tract
• Aδ and C fiber are found throughout the face and oral cavity.
• The meninges are also supplied by fibers of the trigeminal ganglion cells that terminate in the spinal trigeminal nucleus.

Trigeminal sensory nucleus
• Mesencephalic trigeminal nucleus• Propriception
• Chief trigeminal nucleus• Fine touch
• Spinal trigeminal nucleus• Pain, temp, crude touch

Trigeminal lemniscus Tract

Anterior Trigeminothalamic
Tract

The spinal trigeminal nucleus
• Divided into:–pars caudalis,
• nondiscriminative touch, pain, and thermal sensations.
–pars interpolaris,
–pars oralis.

Trigeminal nerve distribution
Pars caudalis cross section

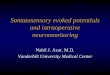
Lateral medullary (Wallenberg) syndrome.
Dysfunction Effects
Lateral soinothalamic TractContralateral deficits in pain and temperature sensation from body
Spinal Thalamic NucleusIpsilateral loss of touch pain and temperature sensation from face
Nucleus Ambiguus (which affects X and nerves IX)
Dysphagia, horseness, diminished gag reflex
Vestibular system Vertigo, nystagmus, vomiting
descending sympathetic fibers ipsilateral Horner’s syndrome
Centarl Tegmental Tract Palatal myoclonus
Inferior Cerebellar PeduncleIpsilateral cerebellar signs including ataxia

Chronic painThalamic lesioning
• Lateral thalamic lesions involve: VPL/VPM.– pain relief – S/E: loss of cutaneous and position sense in the affected limb,
impaired motor function.
• Medial thalamus lesion involve: the centromedian-parafascicular complex CM-PF, the central lateral nucleus, the medial dorsal nucleus. – Pain relief. – Less S/E

• Deep brain stimulation.– Stimulating electrodes centered in the
somatosensory thalamus, the CM-PF complex, or the periventricular gray (PVG)-PAG activate neurons.
Chronic pain

QuestionsQuestions

Test
• What are the nucleus:– Mesencephalic trigeminal nucleus
• Propriception
– Chief trigeminal nucleus• Fine touch
– Spinal trigeminal nucleus• Pain, temp, crude touch

Test
• Draw a medulla cross section, and label the Lateral medullary (Wallenberg) syndrome.

Lateral medullary (Wallenberg) syndrome.

• Which arteries can result in a Wallenberg syndrome? Name 4
– Vertebral artery (most common)– PICA– Superior medullary artery– Lateral medullary artery– Middle medullary artery