Embed Size (px)
Citation preview

THE FEMUR
15The Femur: Perspective
51
Fractures of the shaft of the adult femur aretransfixed with the curved pin one fourth inch indiameter. We have two basic options. The pincan be introduced via the greater trochanter anddriven downward or through the external condyleand driven upward.
The greater trochanter is general preferablebecause it avoids the possibility of infection of
the knee joint. Introduction of the pin throughthe supero-lateral cortex of the great trochanteris not difficult when semi-open reduction is electedbecause one can become oriented by palpatingthe distal end of the proximal fragment. However,in closed reduction and closed pinning of thefemur shaft, we have found it much easier to pinthe fracture via the external condyle.
Pin options for shaft fractures.
The medullary cavity of the lower femoral shaftis trumpet shaped in contract to the tubularshaped medullary canal of the upper shaft.Double pins three sixteenths inch in diameterare utilized in this area via the condyles. In the
intermediate region, the junction of the middleand lower thirds of the shaft, a combination ofthe two technics is used combining the curvedone fourth inch as above with the small pin viathe medial condyle.
Double pins for the supracondylar area.
LOWER EXTREMITY TECHNICS
52
This bone is amenable to pinning from thesubtrochanteric area (except in old people) toand including the condyles. There must be somevariance of operative technic at different levelsbecause of the bone structure and the differingmuscle pulls at these levels.
Fracture of the mid-shaft is easiest to deal withand will be discussed first. The operation willthen be modified for adaptation to other regionsof the femur in a natural progression of technic.
To follow the orthodox textbook approach wouldbut cause confusion. Fracture levels will bediscussed in this order:
1. Mid-shaft.
2. Junction upper and middle thirds.
3. Subtrochanteric region.
4. Supra-condylar region.
5. Junction middle and lower thirds.
6. The condyles.
MID SHAFTThe deformity here results from the force ofviolence rather than muscle pull. Bones overlapmarkedly and may be displaced in any direction,but distal fragment is usually posterior.
Any fracture table is satisfactory. There is nonecessity for the lateral position or for specialattachments for the table.
The lateral incision can be used. The antero-lateral approach is almost bloodless and givesmechanical advantages for semi-open operation.
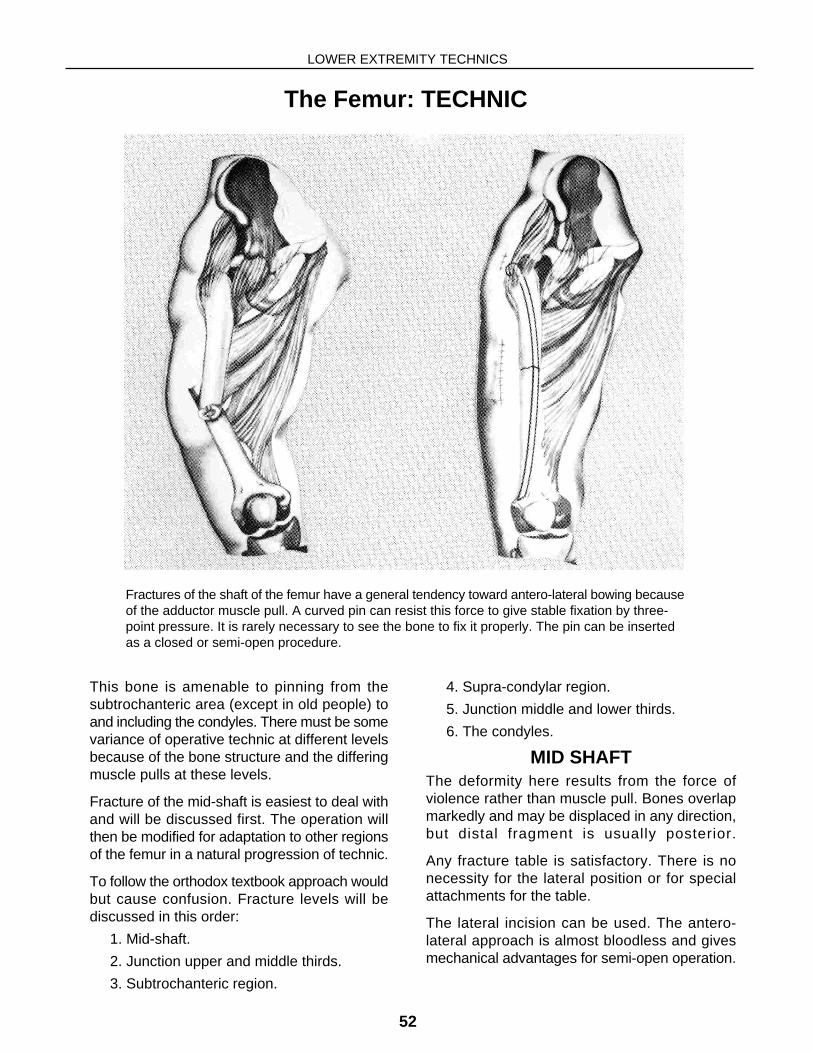
Fractures of the shaft of the femur have a general tendency toward antero-lateral bowing becauseof the adductor muscle pull. A curved pin can resist this force to give stable fixation by three-point pressure. It is rarely necessary to see the bone to fix it properly. The pin can be insertedas a closed or semi-open procedure.
The Femur: TECHNIC

Technic: Mid Shaft
THE FEMUR
53
The pin should be inserted and the point bepalpable at the fracture line before bonemanipulation begins. There is no point inmanipulating the bone until the pin is ready toenter the distal fragment. By following thisprocedure it becomes necessary to hold thebone in the reconstructed position but a fewseconds as the pin crosses the fracture line.
The muscles of the thigh are strong andmanipulation time should be minimal because itis exhausting to the surgeon. For this reason theprimary incision should be made first to identifythe position of the proximal fragment by palpation.This orientation makes a simple procedure ofinserting the pin in the proximal fragment.
(A) POSITION OF PATIENT on fracture table. Simple recumbency, hip adducted and neutralas to rotation. Moderate, not strong, traction to overcome shortening. Incisions indicated.
(B-D) THE ANTERO-LATERAL INCISION for semi-open reduction
(B) SIX-INCH INCISION through skin, fat and fascia lata exposes cleavage line between rectusfemoris and vastus lateralis muscles.
(C) RECTUS FEMORIS reflected medially exposing aponeurosis covering vastus intermedius.Small incision is made through aponeurosis only, not cutting muscle.
(D) ARTERY FORCEPS pushed through vastus intermedius into hematoma. Blades spreaduntil opening admits two examining fingers.
A
B
C
D

LOWER EXTREMITY TECHNICS
54
(A) The proximal fragment does not rotate andthe great trochanter is directly lateral. It isidentified by palpation and exposed by a two-inch incision which extends through the fascialata.
With fingers in each wound, line of proximalfragment is easily visualized mentally withoutactual exposure of the bone.
Identify point of insertion which is the supero-lateral surface of the great trochanter. Startopening in bone at this point with awl-reamer.Drill not deeper than one-half inch. During thisprocedure keep palpating fingers on end ofproximal fragment for orientation. Direct the awl-reamer at a point just medial to finger tips and
ream hole to depth of one and one-half inches.Leave reamer in place.
(B) Select pin from rack No. 1 (one fourth inchdiameter) of proper length to reach into condyle.Allow one extra length for curve. Shape pin intoslight curve (B) using bending iron.
(C) Remove reamer and insert pin into trochanter.As it is tapped with mallet, the sled runner willengage far cortex and ride it down to the fractureline. Continue driving until point can be palpatedat fracture line. Allow pin to rotate. It guides itselfin this manner.
In closed pinning of the femur shaft, we now findthe pin can be introduced more easily throughthe lateral wall of the external condyle, driving itproximally into the region of the great trochanter.
The Proximal Fragment
A B C
Transfixion
THE FEMUR
55
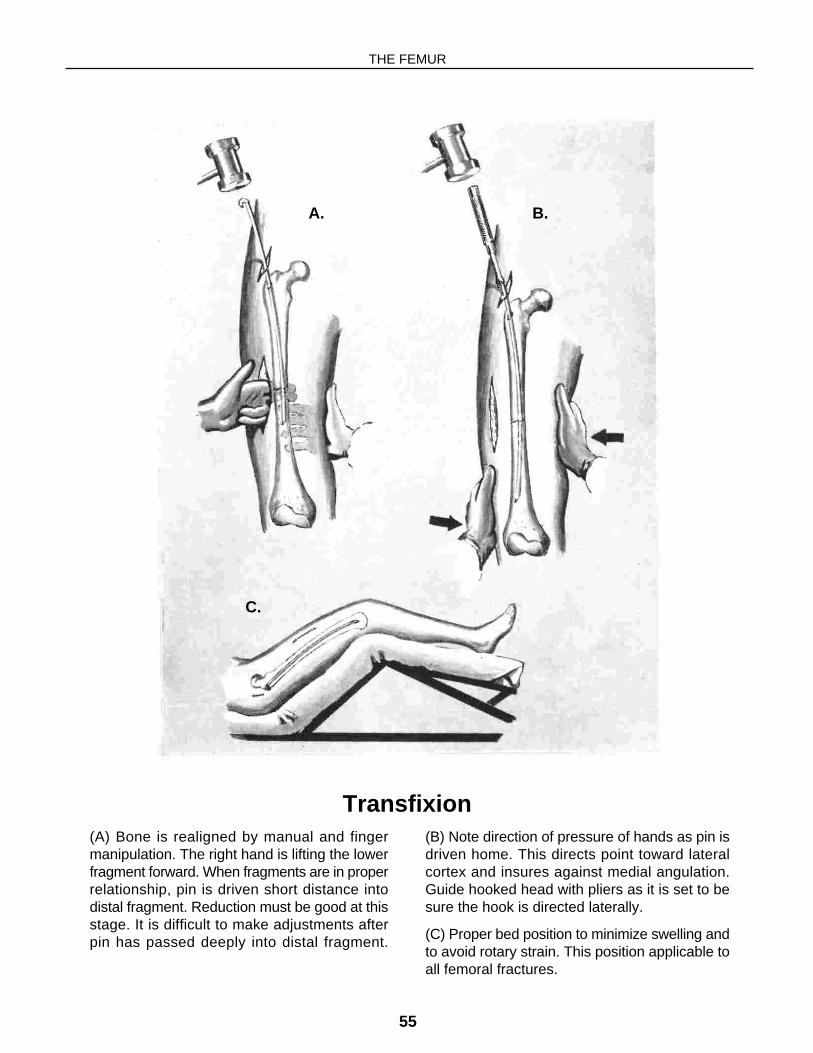
(A) Bone is realigned by manual and fingermanipulation. The right hand is lifting the lowerfragment forward. When fragments are in properrelationship, pin is driven short distance intodistal fragment. Reduction must be good at thisstage. It is difficult to make adjustments afterpin has passed deeply into distal fragment.
(B) Note direction of pressure of hands as pin isdriven home. This directs point toward lateralcortex and insures against medial angulation.Guide hooked head with pliers as it is set to besure the hook is directed laterally.
(C) Proper bed position to minimize swelling andto avoid rotary strain. This position applicable toall femoral fractures.
A. B.
C.
LOWER EXTREMITY TECHNICS
56
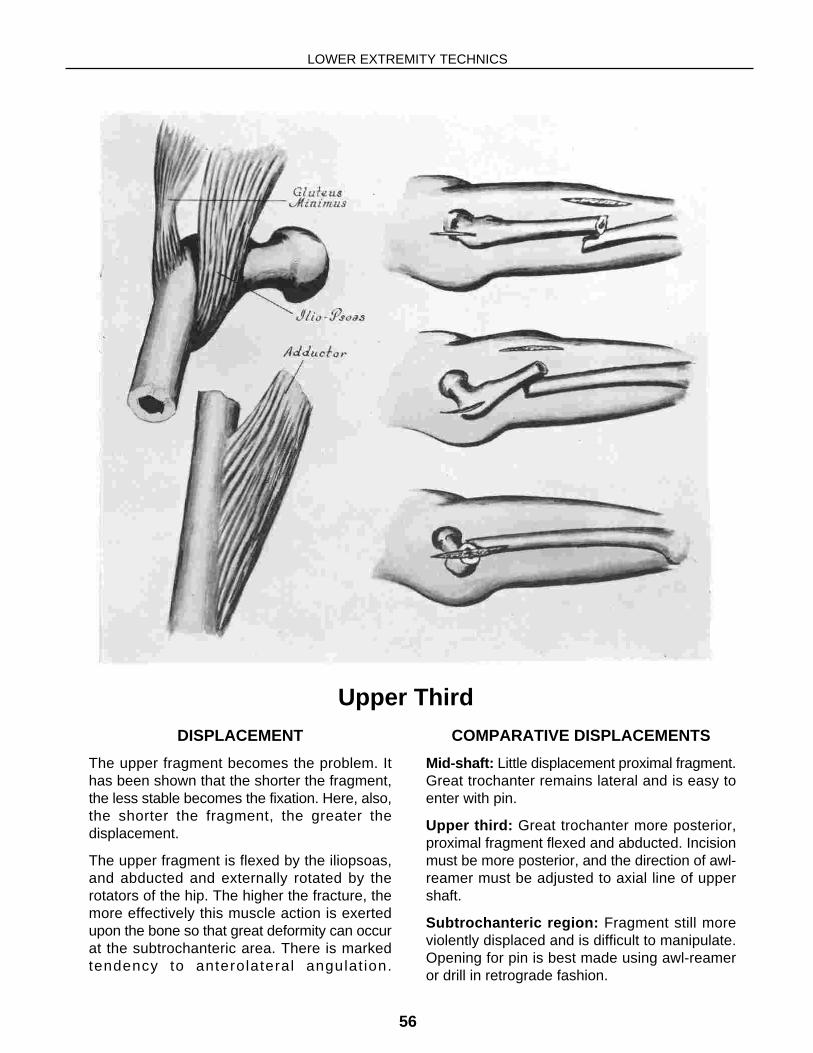
DISPLACEMENT
The upper fragment becomes the problem. Ithas been shown that the shorter the fragment,the less stable becomes the fixation. Here, also,the shorter the fragment, the greater thedisplacement.
The upper fragment is flexed by the iliopsoas,and abducted and externally rotated by therotators of the hip. The higher the fracture, themore effectively this muscle action is exertedupon the bone so that great deformity can occurat the subtrochanteric area. There is markedtendency to anterolateral angulat ion.
COMPARATIVE DISPLACEMENTS
Mid-shaft: Little displacement proximal fragment.Great trochanter remains lateral and is easy toenter with pin.
Upper third: Great trochanter more posterior,proximal fragment flexed and abducted. Incisionmust be more posterior, and the direction of awl-reamer must be adjusted to axial line of uppershaft.
Subtrochanteric region: Fragment still moreviolently displaced and is difficult to manipulate.Opening for pin is best made using awl-reameror drill in retrograde fashion.
Upper Third
Technic: Junction Upper and Middle Thirds
THE FEMUR
57
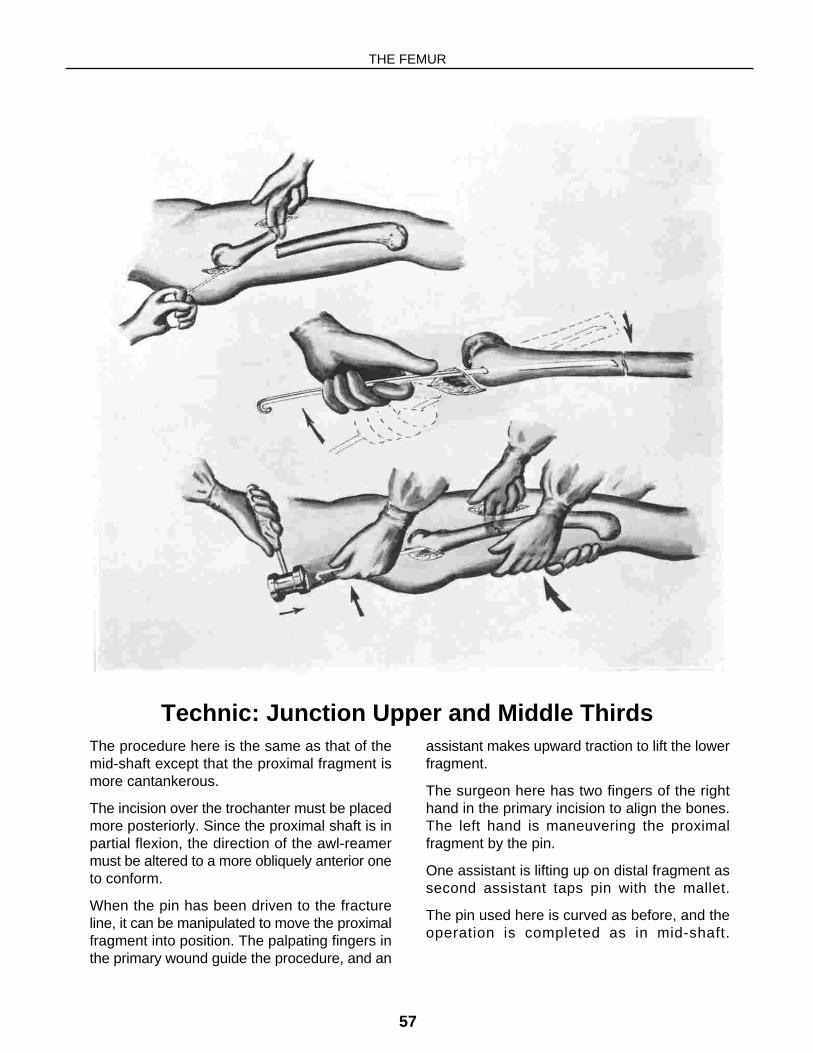
The procedure here is the same as that of themid-shaft except that the proximal fragment ismore cantankerous.
The incision over the trochanter must be placedmore posteriorly. Since the proximal shaft is inpartial flexion, the direction of the awl-reamermust be altered to a more obliquely anterior oneto conform.
When the pin has been driven to the fractureline, it can be manipulated to move the proximalfragment into position. The palpating fingers inthe primary wound guide the procedure, and an
assistant makes upward traction to lift the lowerfragment.
The surgeon here has two fingers of the righthand in the primary incision to align the bones.The left hand is maneuvering the proximalfragment by the pin.
One assistant is lifting up on distal fragment assecond assistant taps pin with the mallet.
The pin used here is curved as before, and theoperation is completed as in mid-shaft.
LOWER EXTREMITY TECHNICS
58
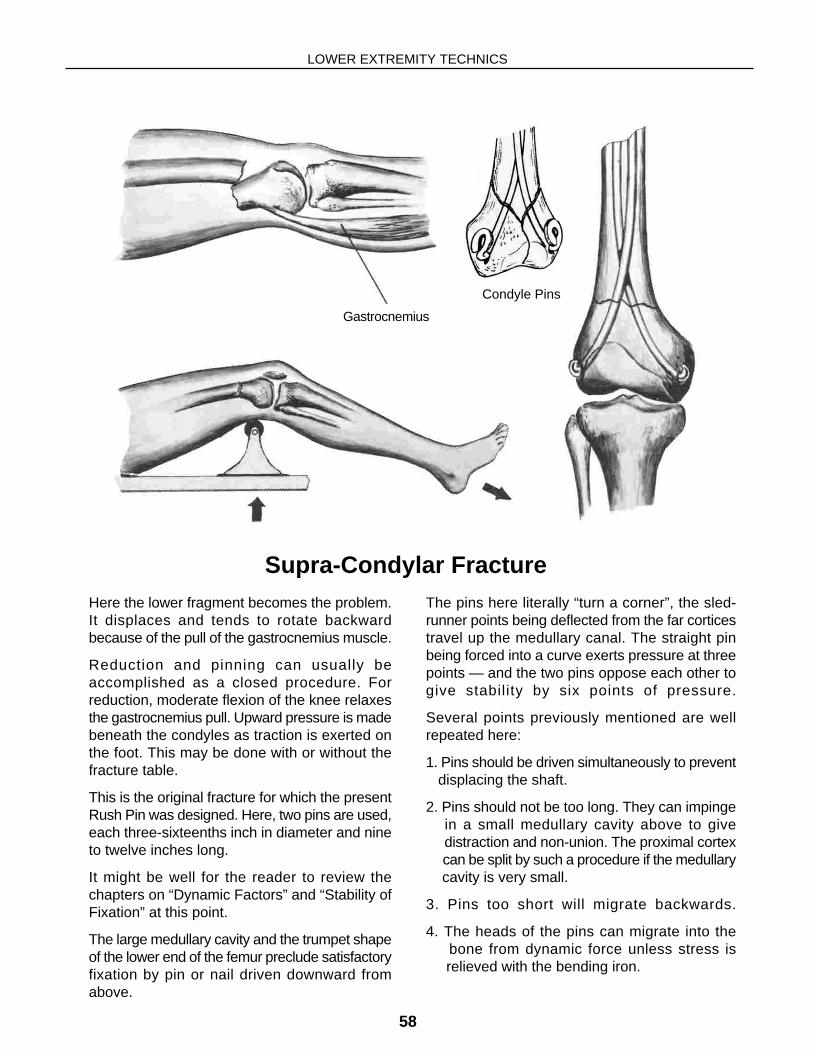
Here the lower fragment becomes the problem.It displaces and tends to rotate backwardbecause of the pull of the gastrocnemius muscle.
Reduction and pinning can usually beaccomplished as a closed procedure. Forreduction, moderate flexion of the knee relaxesthe gastrocnemius pull. Upward pressure is madebeneath the condyles as traction is exerted onthe foot. This may be done with or without thefracture table.
This is the original fracture for which the presentRush Pin was designed. Here, two pins are used,each three-sixteenths inch in diameter and nineto twelve inches long.
It might be well for the reader to review thechapters on “Dynamic Factors” and “Stability ofFixation” at this point.
The large medullary cavity and the trumpet shapeof the lower end of the femur preclude satisfactoryfixation by pin or nail driven downward fromabove.
The pins here literally “turn a corner”, the sled-runner points being deflected from the far corticestravel up the medullary canal. The straight pinbeing forced into a curve exerts pressure at threepoints — and the two pins oppose each other togive stability by six points of pressure.
Several points previously mentioned are wellrepeated here:
1. Pins should be driven simultaneously to prevent displacing the shaft.
2. Pins should not be too long. They can impinge in a small medullary cavity above to give distraction and non-union. The proximal cortex can be split by such a procedure if the medullary cavity is very small.
3. Pins too short will migrate backwards.
4. The heads of the pins can migrate into the bone from dynamic force unless stress is relieved with the bending iron.
Supra-Condylar Fracture
Gastrocnemius
Condyle Pins

Anatomy
THE FEMUR
59
The condyles of the femur are enveloped in anaponeurotic capsule. On flexion and extensionof the knee this capsule glides obliquely overthe condyles. If this capsule is compromised bythe pin, it will adhere to the bone to give limitationof motion at the knee.
The collateral ligaments must not be injured bythe surgical procedure. Partially flexing the kneecarries them backward out of harm’s way.
These ligaments are not infrequently torn ininjuries of this and are best repaired immediately.After the bone has been transfixed, it is possible
to test the ligaments for laxity (lateral mobility ofthe knee).
The point of entrance for the pin is about oneinch central to the periphery or articular marginof the condyle. This can be determined bypalpation when the knee is flexed. The reamermust be inserted, in the lateral plane, so that itwill approximate the long axis of the shaft. If thepoint of insertion is too far posteriorly or at thewrong angle, the condyle will angulate as thepin enters the medullary canal.
A one-inch incision is sufficient for inserting thepin and must extend through the capsule.

LOWER EXTREMITY TECHNICS
60
For this procedure the pins should not be pre-curved but should be driven straight. The pindevelops the curve from pressure within thebone.
In the front view the two pins enter the condyleat such an angle that they cross at a point aboutfour inches above the insertion points. Theopenings for the pins must be accurate and canbe directed much more simply with the awl-reamer than with the drill.
Each sled-runner point glides up the oppositecortex directing the pin into the medullary canal.
Before the pins are driven completely home, theheads should be stress relieved (bent) with thebending iron to prevent their cutting into the bone.
The capsule of the joint must be sutured over theheads of the pins, and the knee should be testedto be sure there is full range of motion at completionof the operation. This can save laterembarrassment.
Splinting is usually unnecessary but might beneeded in comminuted fractures or in elderlypatients where fixation is not stable. Double pinsof three-sixteenths diameter do not nearly possessthe strength of a single one-fourth inch pin. If thereis doubt as to stability, splint!
Double Pinning

Junction Mid and Lower Thirds
THE FEMUR
61
The displacement is similar to but less markedthan in the supracondylar region. Here semi-open reduction is usually indicated, but closedpinning can sometimes be done.
The reduction is accomplished either as in themid-shaft or as for the supracondylar fracture.
Here it is difficult to get complete fixation becauseof the size and shape of the bone. Rocking atthe fracture site delays healing. And this is theslowest healing area of the femoral shaft. It mayrequire four to eight months to secure goodhealing in this area.
The best fixation (lower left) combines the curvedl/4 inch pin as used for the shaft with a curved3/16 inch pin driven upward from the medial
condyle. The larger (l/4 inch) pin can enter thebone via the external condyle and be drivenupwards. If this is elected, the head of the pinshould be carefully stress relieved to preventlateral angulation of the fracture. The pin fromthe medial condyle should not be too longbecause in the average young adult the isthmusof the bone will not accept both pins.
The three alternatives shown give less stablefixation, but are at times adequate. Of thesethree, the curved quarter-inch pin is best. Thestraight pin might permit rotation or soon workloose in the cancellous bone to permit rocking.The double pins, as used for the supracondylarfracture, permit more rocking at this level thanone would expect.
External fixation is rarely necessary.

LOWER EXTREMITY TECHNICS
62
This type fracture results in widening. Thefragment moves up, out and is rotated backwardby the pull of the gastrocnemius muscle.
The medullary pin (3/16 inch) when properlyplaced will compress the fracture to give stablefixation and rapid healing.
This fracture must be accurately reduced evenif it requires an incision. Closed reduction mightbe accomplished by the same procedure usedin the supracondylar region — traction on footwith the knee moderately flexed and with counter
traction upward beneath condyles.
The awl-reamer might be used to lever the fragmentinto better position. The small transverse pinsafeguards the integrity of the articular surfacebut is not always essential.
The single larger intramedullary pin is introducedjust as for the supracondylar fracture. Individualjudgment will have to be used as to how much tostress-relieve the head of the pin with the bendingiron. Here a limited amount of pin pressure isnecessary.
Femur: Condyle

Femur Condyles: ‘T’ or ‘Y’ Fracture
THE FEMUR
63
The problem now becomes more complex butis dealt with by using the same principles asbefore.
The procedure is modified first to bring the twocondylar fragments into proper relationship witheach other. The articular surface must be restored
to the proper contour, and this is safeguardedby passage of the small transverse pin.
The relationship of the Condyles to the shaft isreestablished, and the two pins (3/16 inch) drivenupward to transfix the supracondylar fracture asbefore.
LOWER EXTREMITY TECHNICS
64
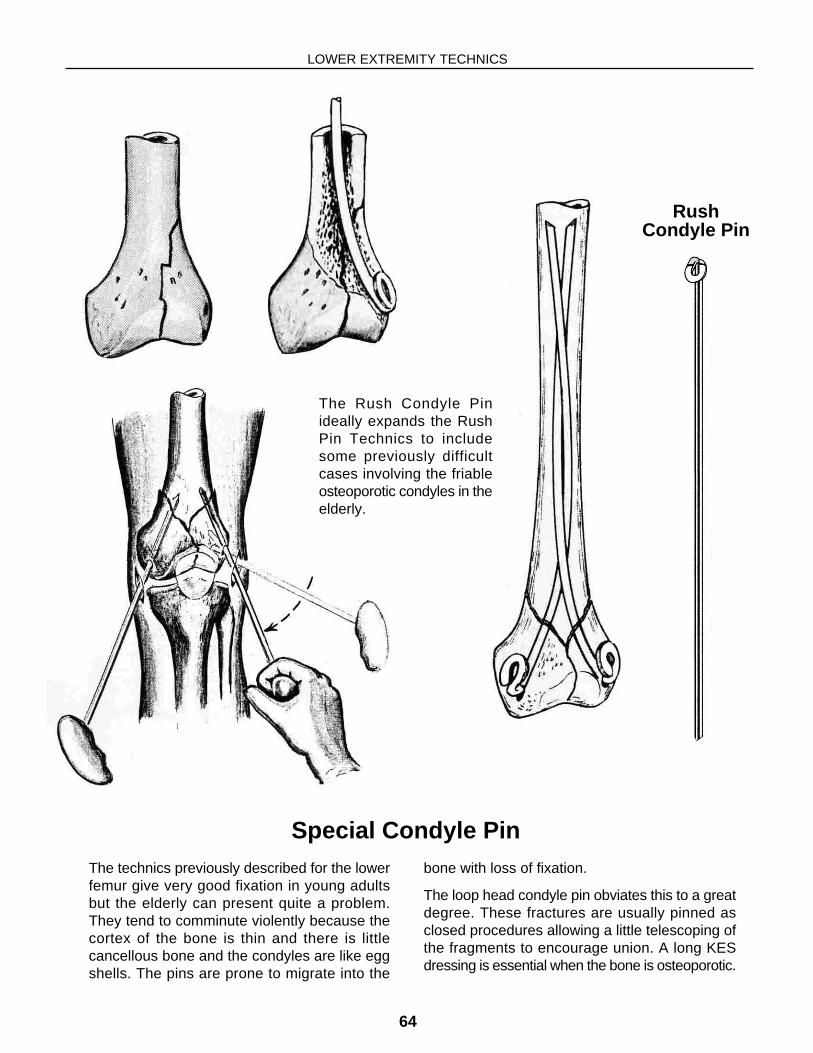
The technics previously described for the lowerfemur give very good fixation in young adultsbut the elderly can present quite a problem.They tend to comminute violently because thecortex of the bone is thin and there is littlecancellous bone and the condyles are like eggshells. The pins are prone to migrate into the
bone with loss of fixation.
The loop head condyle pin obviates this to a greatdegree. These fractures are usually pinned asclosed procedures allowing a little telescoping ofthe fragments to encourage union. A long KESdressing is essential when the bone is osteoporotic.
Special Condyle Pin
The Rush Condyle Pinideally expands the RushPin Technics to includesome previously difficultcases involving the friableosteoporotic condyles in theelderly.
RushCondyle Pin