Embed Size (px)
Citation preview

10/5/2014
1
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP
Education Specialist
LRM Consulting
Nashville, TN
Learning Outcomes
Differentiate between diabetes insipidus and
syndrome of inappropriate ADH.
Analyze management strategies for
hyperglycemic emergencies (DKA & HHNK).
Evaluate the common causes and
management strategies for patients with
adrenal insufficiency.
Defining Characteristics
•uncontrolled hyperglycemia
•profound dehydration
•electrolyte disturbances
•acid - base abnormalities

10/5/2014
2
Signs & Symptoms
•coma
•abdominal pain
•polydipsia, polyuria
•Kussmaul respirations
•fruity breath
Signs & Symptoms
•N/V, weakness
•weight loss
•hypotension
•ketonuria
•tachycardia
Treatment
•ABCs
•restore fluid balance
–NS
–D5½NS????

10/5/2014
3
Treatment
•restore metabolism
–regular insulin
•correct acidosis
–? NaHCO3?
•restore electrolyte
balance
Treatment
•Electrolyte Management
–potassium
–phosphate
–sodium
Case Study
• 37 – year – old male
– found stuporous but responsive
to vigorous shaking
– transported to the ED

10/5/2014
4
• Initial Assessment:
– warm, dry, flushed skin
– poor skin turgor
– rapid, deep respirations
– fruity odor to breath
– finger stick reveals level that exceeds
upper limits of dextrometer
• Management
– physician notified
– IV started – NS wide open
Case Study
• Vital signs:
HR 118/minute
BP 80/40
RR 24/minute
T 37 °C (98.6 °F)

10/5/2014
5
• Laboratory Data
Sodium 124
Potassium 6.2
Chloride 92
Carbon dioxide 6
Creatinine 1.9
Glucose 704
Case Study
• Laboratory Data:
Hemoglobin 12
Hematocrit 36
WBC 24, 000
Platelets 358,000
Case Study
• ABGs
pH 7.0
paCO2 17
paO2 90
HCO3 4
SaO2 94%

10/5/2014
6
Case Study
• Laboratory Data - Other
Serum Ketones 45
Urine Ketones +
Anion Gap 26
Carbon dioxide 6
Lungs Clear to
auscultation
Interventions:
–cultures: 2 sets of blood,
urine & sputum
– IV NS
– regular insulin
–electrolyte replacement
Case Study
• Laboratory Data 1515 1615 1715 1815
Creatinine 1.9 2.0 2.0 1.9
Sodium 124 127 129 131
Potassium 6.2 4.5 3.7 3.2
Carbon dioxide 6 8 7 9
Chloride 92 87 92 93
Glucose 704 625 538 387
Urine Output 500 500 250 205

10/5/2014
7
Case Study
• Laboratory Data 1915 2015 2115
Creatinine 1.8 1.8 1.6
Sodium 131 135 131
Potassium 2.9 2.8 3.1
Carbon dioxide 9 17 19
Chloride 95 100 97
Glucose 300 284 235
Urine Output 205 190 110
Defining Characteristics
•Type II diabetes
•mortality 40 - 60%
•severe dehydration
•profound hyperglycemia
•sodium abnormality
Signs & Symptoms
•N/V, weight loss
•hypotension, tachycardia
•coma
•poor skin turgor
•seizures, hyperreflexia,
disorientation

10/5/2014
8
Treatment
•ABCs
•restore fluid balance –NS
•restore metabolism –insulin
–treat cause
Treatment
•restore electrolytes
–potassium
–phosphate
•monitor for cerebral
edema
Case Study
•72 – year old female
•admitted to ICU – became
progressively unresponsive at
nursing home
•developed a mild pneumococcal
pneumonia

10/5/2014
9
Case Study
•PMH
–CAD & chronic CHF for 6 years
–Non – insulin – dependent diabetes
mellitus for 12 years
–Medications: digoxin,
hydrochlorothiazide, potassium,
micronase
Case Study
•Assessment
–LOC: unresponsive; no
verbalization
–GCS: 7
–Pupils: Equal (3 mm), round,
reacts slowly to light
–Seizures – no seizure activity
Case Study
•Assessment
–Pulmonary: diminished
in right lower lobe
–RR: 22/minute
–O2 therapy: intubated;
TV 700 mL, FiO2 0.40

10/5/2014
10
Case Study
• ABGs Admission 8 hours
pH 7.23 7.38
paCO2 32 39
paO2 77 88
HCO3 17 21
SaO2 92% 94%
Case Study
• CV Status Admission 8 hours
HR 124 88
Rhythm ST, PAC, PVC SR
BP 78/52 108/72 (RA)
102/70 (LA)
CVP 1 5
Capillary refill > 3 sec 3 sec
Case Study
• Renal Status Admission 8 hours
Urine Output < 20 40
Urine Color dark amber clear yellow
Urine Glucose 4+ 4+
Urine Ketones trace negative
Infection: urine culture pending

10/5/2014
11
Case Study
•Assessment
–GI
–Abdomen: moderately distended,
soft & tympanic
–Bowel sounds: hypoactive
–NG: moderate amount of bilious
drainage, guaiac negative
Case Study
• Lab Values Admission 8 hours
Glucose 1260 620
Sodium 146 140
Potassium 3.5 3.7
Chloride 103 100
Carbon Dioxide 19 23
Magnesium 1.0 1.0
Case Study
• Lab Values Admission 8 hours
BUN 72 52
Creatinine 2.3 1.7
WBC 22,000 17,000
Hematocrit 49% 42%
Digoxin Pending 2.0

10/5/2014
12
Diabetes Insipidus
Defining Characteristics
•defect in release or synthesis
of ADH (neurogenic)
•defect in response to ADH at
the distal tubule (nephrogenic)
Diabetes Insipidus
Etiology
•Traumatic
•Inflammatory
•Pharmacologic agents
–alcohol
–dilantin
–lithium carbonate
Signs & Symptoms
•polyuria
•polydipsia
•dehydration
–dry skin
–confusion
–poor skin turgor

10/5/2014
13
Lab Tests
•Serum osmolality
–Normal: 285 – 295 mOsm/kg
–Critical values
• <265 mOsm/kg
• >320 mOsm/kg
–(increased in DI)
– > 295 mOsm/kg
Lab Tests
•Urine osmolality
–12 – 14 hour fluid restriction
(> 850 mOsm/kg)
–random sample 50 – 1200 mOsm/kg
–(decreased in DI)
– < 500 mOsm/kg
Diabetes Insipidus
Complications
•dehydration
•bladder hypertrophy
•resistance to vasopressin therapy

10/5/2014
14
Diabetes Insipidus
Treatment
•correct water & electrolyte
imbalance
•administer vasopressin
•watch for water intoxication
Case Study
•20 – year college student
•waking up 1 – 2 times each
night (started 1 month ago)
•Increased output during day
– attributed to coffee intake
•urine pale and colorless
Case Study
•ED visit
–No abnormalities on PE
–Labs
•Sodium 149 mEq/L
•Serum Osm. 308 mOsm/L
•Urine Osm. 200 mOsm/L
•Glucose 85 mg/dL

10/5/2014
15
Case Study
•Water deprivation test
–Serum Osm. 315 mOsm/L
–Urine Osm. Unchanged
•DDAVP
–Serum Osm. 290 mOsm/L
–Urine Osm. 425 mOsm/L
Case Study
•MRI
–Idiopathic pituitary
diabetes insipidus
SIADH
Defining Characteristics
•increased secretion of ADH
•results in water intoxication

10/5/2014
16
SIADH
Etiology
•tumors (extracranial & cranial)
•traumatic
•infections
•pharmacologic agents
–chlorpropamide
–thiazides
–acetaminophen
SIADH
Signs & Symptoms
•water intoxication
–altered LOC
–diminished DTR
–Seizures
SIADH
Signs & Symptoms
•Lab Values –Normal: 285 – 295 mOsm/kg
–Serum osmolality: low
–Urine osmolality: high

10/5/2014
17
SIADH
Complications
•coma
•seizures
•death
SIADH
Treatment
•fluid restriction
•hypertonic saline
•diuretics
•democlocycline
Case Study
•37 – year admitted to Neuro
ICU with SAH
•Dilantin, nimodipine &
amicar started
•GI ulcer & DVT prophylaxis
•Day 2 surgical clipping

10/5/2014
18
Case Study
•Postoperatively
–Fluids
•Maintain blood pressure
•Minimize/prevent vasospasm
Case Study
•7th postoperative day VS
T 37.2C
HR 112
RR 24
BP 115/56
CVP 3
Case Study
•Laboratory Data
Glucose 113 mg/dL
Sodium 128 mEq/L
Potassium 4.8 mEq/L
Chloride 100 mEq/L

10/5/2014
19
Case Study
•Laboratory Data
BUN 21 mg/dL
Creatinine 1.0 mg/dL
Uric Acid 3.0 mg/dL
WBC 7,300
Hct 48%
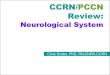
• Reported in critically ill patients
• Subnormal adrenal corticosteroid production
• Hypoadrenal state without clearly defined defects in HPA axis
• Difficult to define based on serum cortisol concentrations:
– Although cortisol level may be normal, it may remain inadequate for the patient’s metabolic demands
• Rapid improvement on Hydrocortisone therapy
Relative Adrenal Insufficiency
0%
10%
20%
30%
40%
50%
60%
70%
Septic Shock Other ICU Patients
CABG
Dissecting AAA
JCEM (2006) 91: 105–114
Incidence of Relative Adrenal Insufficiency

10/5/2014
20
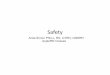
CORTISOL
ACTH
CRH
STRESS:
Physical stress
Emotional stress
Hypoglycemia
Cold exposure
Pain
Adrenal Cortex
Anterior Lobe of
Pituitary Gland
Hypothalamus
• Increased sensitivity to pressors
• Anti-inflammatory effect on immune
system
• Maintenance of vascular tone &
endothelial integrity
• Modulation of angiotensinogen synthesis
• Reduction of NO-mediated vasodilation
Cortisol Action
Classical regulators of the axis continue to
be operable in critically ill patients but with significant alterations:
– Hypothalamic hormones
– CRH
– Vasopressin
– Inflammatory cytokines: IL-1, IL-6,TNF-α
– ANS
modulators of HPA function
Anesthesiology (1993) 77: 426–431
HPA Alteration During Critical Illness

10/5/2014
21
• Impaired hepatocellular
function
• Impaired hepatic blood
flow
• Impaired renal/thyroid
function
J Clin Invest (1958) 37: 1791–1798
• Increased steroid production
•Decreased steroid clearance
Increased Serum Cortisol
(free cortisol level)
Stress
• ACTH and cortisol responsiveness to exogenous CRH is enhanced during critical illnesses
• ACTH = dominant factor stimulating cortisol secretion throughout the critical illness → other factors play a significant modulating influence on the axis
J Inflamm (1996) 47: 39–51
Arginine Vasopressin
Endothelin
Atrial Natriuretic Factor
(ANF)
Variety of Cytokines
(IL-6)
Type & Severity of Illness • Acute phase of illnesscortisol levels proportionate to
degree of stress
• Cortisol levels: major surgery vs sepsis SIMILAR ELEVATION
• Cortisol elevations in sepsis: -wide range
-? don’t correlate with APACHE
-highest levels highest mortality
• Sepsis vs Trauma patients: -similar cortisol elevation
-levels markedly higher in:
– Sepsis,
– Progression to ARDS
– Patients who didn’t survive
• Glucocorticoid resistant patients have higher levels
JCEM (2001) 86: 2811–2816 Intensive Care Med (2001)27: 1584-1591 Clin Endocrinol (2004) 60:29-35.

10/5/2014
22
Short-Term Stressors vs. Protracted Critical Illness
• Initial phase is characterized by:
» ↑ACTH
» ↑Cortisol
• Protracted critical illness:
» ↓ACTH
» ↑Cortisol
cortisol secretion is being regulated and stimulated by
alternative pathways other than the classical hypothalamic CRH
JCEM (1998)83: 1827-34
J Trauma (1987)27: 384-392
Persistent Hypercortisolism Observed in Protracted Critical Illness
J Trauma (1987) 27: 384–392
Benefits Related To Long Term Complications
Providing energy Hyperglycemia
Maintaining volume Myopathy
Minimizing inflammation Psychiatric alterations
Poor wound healing
Diagnostic Clues in Critically Ill Patients
• persistent hypotension despite
adequate volume resuscitation
• hyperdynamic circulation and low SVR
• ongoing inflammation w/o obvious
source that does not respond to empiric
treatment

10/5/2014
23
High-Dose ACTH Stimulation Test:
• Can be done at any time of day
• Baseline cortisol 250g ACTH measure cortisol at 30 and 60 minutes
• Non-stressed pt: increase to 18 g /dL R/O AI
• High sensitivity & specificity for primary AI using
threshold value of 15 g /dL
• Less sensitive for secondary AI
Critical Care Clinics (2006) 22 (2): 245-53
Random Cortisol Level
Poor prognosis in septic shock patients:
– extremely HIGH (>34g/dL) total cortisol
– extremely LOW (<25g/dL) total cortisol
N Engl J Med (2003) 348 (8): 727-734 Chest (2002) 122 (5): 1784-1796 Critical care medicine (2003) 31 (1): 141-145
• Unstressed subjects, AI:
– ACTH stimulated cortisol 18-20 ug/dl
• Critically illness, AI:
– random cortisol <15 or 25 ug/dl (if on pressors)
– cortisol increment after ACTH stimulation < 9ug/dl
• Severe hypoproteinemia, AI:
– serum free cortisol < 2 ug/dl or
– ACTH stimulated value < 3.1 ug/dl
N Engl J Med (1996) 335: 1206-1212 N Engl J Med (2003) 348: 727–734
Diagnostic Criteria

10/5/2014
24
Case Study
• 24-year-old white female
• presented with a 5-day history of
periumbilical abdominal pain,
non-bilious emesis, fatigue, and
intermittent low-grade
temperature
• no significant medical history
Case Study
•VS
T 37.1C
HR 113
RR 14
BP 60/32
capillary refill 5-6 sec
Case Study
•Laboratory Data
Glucose 112 mg/dL
Sodium 126 mEq/L
Potassium 4.3 mEq/L

10/5/2014
25
Case Study
•Laboratory Data
BUN 33 mg/dL
Creatinine 1.6 mg/dL
WBC 17,000
Hct 16.7
Case Study
• CVP 8 to 11
NS (20 mL/kg) + 5%
albumin (30 mL/kg) over 3
hours
• UO 1.6 mL/kg/hr
Case Study
• Dopamine (10 mcg/kg/min)
• Epinephrine (0.12 mcg/kg/min)
• Norepinephrine (0.18
mcg/kg/min)
No Change in Blood Pressure

10/5/2014
26
Case Study
•Laboratory Data
Random cortisol (< 1.0 mcg/dL)
normal 5 – 25 mcg/dL
Cosyntropin stimulation test (<
1.0 ug/dL) after 30 & 60 minutes
Case Study • Hydrocortisone 100 mg/m2 IV
• Hydrocortisone 100 mg/m2/day
• BP improved, vasoactive agents
discontinued within 36 hours
• Cultures negative – antibiotics
stopped

10/5/2014
27