Embed Size (px)
Citation preview

Leanna R. Miller, RN, MN, CCRN,-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP
Education SpecialistLRM Consulting
Nashville, TN

DefinitionDefinition tissue perfusion that is tissue perfusion that is
inadequate to maintain inadequate to maintain normal metabolic and normal metabolic and nutritional functionsnutritional functions
potentially fatal if not potentially fatal if not identified & treatedidentified & treated

Introduction 12% to 18% of patients 12% to 18% of patients
presenting initially in severe presenting initially in severe shock have increased shock have increased mortality or morbidity related mortality or morbidity related to secondary organ failureto secondary organ failure


Clinical Signs of ShockClinical Signs of Shock
Preterminal StagesPreterminal Stages severe hypotensionsevere hypotension agonal respirationsagonal respirations thready pulsethready pulse tachy or bradydysrhythmiastachy or bradydysrhythmias

Shock IndexShock Index HR / systolic blood pressureHR / systolic blood pressure inversely related to LVSWinversely related to LVSW abnormal > 0.9abnormal > 0.9 application:application: persistently abnormal persistently abnormal
shock index in patient with normal shock index in patient with normal VS suggests need for more VS suggests need for more invasive monitoringinvasive monitoring
Rady (1992) Resuscitation 23:227 - 234

most important most important feature to the care of feature to the care of a critically ill patient a critically ill patient is delivery of oxygen is delivery of oxygen to the cellsto the cells

CO X CaOCO X CaO2 2 X 10X 10 CaOCaO22 = Hgb x SaO = Hgb x SaO22 x 1.38 x 1.38
Normal 900 - 1100 mL/minNormal 900 - 1100 mL/min DODO22I = 360 - 550 mL/min/mI = 360 - 550 mL/min/m22

oxygen consumptionoxygen consumption CO x (SaOCO x (SaO22 - SvO - SvO22) Hgb x 1.38 x 10) Hgb x 1.38 x 10
VOVO22 = 220 - 290 mL/min = 220 - 290 mL/min
VOVO22I = 108 - 165 mL/min/mI = 108 - 165 mL/min/m22

normally VOnormally VO2 2 is is 25% of DO25% of DO22

SvOSvO22
• SaOSaO22
• HgbHgb• COCO• VOVO22

amount of oxygen extracted amount of oxygen extracted from blood as it passes from blood as it passes through the tissuesthrough the tissues
(CaO(CaO22 - CvO - CvO2 2 )/ CaO)/ CaO22
values > 0.30 abnormalvalues > 0.30 abnormal > 0.35 serious> 0.35 serious normal 22% to 27%normal 22% to 27%

> 0.35> 0.35• increased VOincreased VO22
• decreased DOdecreased DO22
• bothboth

CI 4.5 L/min/mCI 4.5 L/min/m22
DODO22I 600 L/min/mI 600 L/min/m22
VOVO22I 170 mL/min/mI 170 mL/min/m22

inadequate pulmonary inadequate pulmonary gas exchangegas exchange
inadequate oxygen inadequate oxygen carrying capacitycarrying capacity
inadequate COinadequate CO


conditions and conditions and activities that alter activities that alter demand and demand and consumptionconsumption

critically low DOcritically low DO22
vasodilated statevasodilated state vaso-obstructed statevaso-obstructed state diffusion distancesdiffusion distances
affinity of Hgb for Oaffinity of Hgb for O22

increased extractionincreased extraction once extraction maximized – once extraction maximized –
consumption is dependent consumption is dependent on deliveryon delivery
demand > consumption = demand > consumption = OO22 debt debt

may be may be or normal in or normal in presence of hypoxiapresence of hypoxia
not reliable reflection not reliable reflection of tissue hypoxia of tissue hypoxia
reliable indicator of reliable indicator of tissue perfusiontissue perfusion

arterial more precisearterial more precise normal < 1 mEq/Lnormal < 1 mEq/L > 3 - 4 mEq/L significant > 3 - 4 mEq/L significant
hypoperfusionhypoperfusion will decrease 5 - 10% / hr will decrease 5 - 10% / hr
when appropriate when appropriate therapy usedtherapy used

pHipHi early warning of early warning of
inadequate splanchnic inadequate splanchnic tissue oxygenationtissue oxygenation
low pH = poor prognosis low pH = poor prognosis (consistently < 7.3) (consistently < 7.3)

Lab StudiesLab Studies Normal value: - 2 to + 2Normal value: - 2 to + 2 reflects the extent to which reflects the extent to which
the body buffers have been the body buffers have been exhaustedexhausted
rapidity of normalizing base rapidity of normalizing base deficit decreases morbidity deficit decreases morbidity & mortality& mortality

Most Reliable Perfusion Most Reliable Perfusion MarkersMarkers
Serum lactateSerum lactate Base deficitBase deficit

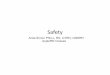
StO2
near infrared light illuminates tissue
light scatters and is absorbed differently by oxygenated and deoxygenated hemoglobin in the microcirculation
light returns to sensor and is analyzed and displayed as % StO2

StO2

StO2
.75 - .90

volumevolume inotropesinotropes vasodilatorsvasodilators assess peripheral assess peripheral
circulation circulation

Identify potentially Identify potentially inadequate DOinadequate DO2 2 statesstates
• clinical evidence clinical evidence of shockof shock
• SvOSvO2 2 < 50% < 50%• OO22ER > 30%ER > 30%

Identify pathological Identify pathological flow dependency stateflow dependency state
DODO22 with fluids or with fluids or inotropeinotrope
–recalculate VOrecalculate VO22
–VOVO2 2 > 10-20 L/m> 10-20 L/m22

ensure accurate parameters
index to body size eliminate sources of
error use parameters with
< 5-10% variance

calculate actual VO2
estimate potential VO2 (look at factors that demand)

delivery needs to delivery needs to
by at least sameby at least same
percentage as demandpercentage as demand

OO2 2 demands are demands are 30-50%30-50%
triggers systemic triggers systemic inflammatory inflammatory responseresponse

Hgb/Hct < 11/33 is Hgb/Hct < 11/33 is associated with delivery-associated with delivery-dependencedependence
mortality if therapeutic mortality if therapeutic targets reached < 12 - 24 targets reached < 12 - 24 hourshours

CI > 4.5 DOI2 700
VOI2 170

46 - year old male• motor vehicle crash• injuries: aortic disruption,
severe bilateral pulmonary contusions, bilateral rib fractures, splenic fracture
• traumatic shock due to injuries

Which hemodynamic Which hemodynamic findings are abnormal?findings are abnormal?

HR 67 BP 122/64/82 RAP / PAOP 10/11 CI 4.6 PVRI / SVRI 143/317RVSWI / LVSWI 17/61 PAP 46/22/32

EDV / EDVI 237/107
EF 60%
O2ER 26.8
SvO2 .74
DO2 / DO2I 1603/722
VO2 / VO2I 430/194

ABGs (.40 FiO2)pH 7.31
pCO2 42
pO2 157
SaO2 .99
HCO3 20.8
SvO2 74% P/F ratio 314.0

Lab Values Hgb 12.1 Hct 31.0 Sodium 139 Chloride 112 Magnesium 1.7 Lactate 5.1 Base Deficit -5.1

What is the underlying What is the underlying pathophysiology?pathophysiology?

What is are the priority What is are the priority interventions?interventions?

33 yr with GSW to chest 4 units of PRBC due to Hct of 27 SVO2 – 70 after blood administration
StO2 – 80% Lactate 1.2 Does he need further treatment?
StO2 and Hemodynamic Monitoring