Embed Size (px)
Citation preview

CUII I WIN
Highlightsfrom EH/
10 Anni di Highlights
Alessandro M. Vannucchi CRIMM- Center of Research and Innovation of MPN
Azienda Ospedaliera Universitaria Careggi University of Florence, Italy

CUII I WIN
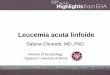
Highlightsfrom EH/ Figure 1: MPN timeline: critical research and clinical data
William Dameshek uses the term
"myeloproliferative''
Heuck describes PMF and Vaquei PV
Bergamo trial of hydroxycarbamlde
In ET H i Description of JAK2V617K
Approval of ruRolltlnlb for PV
PV5G studies vnth hydroxycarbamlde, busulfan,
pipobroman venesection, chlorambucil, 32P are reported
_I_
RIC-alloSCT for Myelofibrosis
reported
Description of CALR mutations
~r 1879
Hemorrhagic thrombo-cythemla or ET, Epstein & Goedel
T 2016
ECIAP study aspirin In PV PT-1 study
hydroxycarbamlde vs anagrellde In ET
PVSG studies Initiated and first diagnostic
criteria
First use of Interferon (Unkesch) and anagrellde
ISIIversteln)
Trials with JAK inhibitors begin
CYTOPV study confirms target PCV
Approva I of ruxolltlnlb for MF
AM Vannucchi, C Harrison, unpublished, 2

CUII I WIN
Highlightsfrom EH/ Figure 1: MPN timeline: critical research and clinical data
William Dameshek uses the term
"myeloproliferative''
Heuck describes PMF and Vaquei PV
Bergamo trial of hydroxycarbamlde
In ET til
PV5G studies vnth hydroxytarbamlde, busulfan,
pipobroman venesection, chlorambucil, 3ZP are reported
_I_
RIC-alloSCT for Myelofibrosis
reported
™r 1879
Hemorrhagic thrombo-cythemla or ET, Epstein & Goedel
ECIAP study asplr PT-1 study
hydroxycarbaml anagrellde In
Description of JAK2V617K
Approval of ruxolltlnlb for PV
o o
Description of CALR mutations
PVSG studies Initiated and first diagnostic
criteria
First use of Interferon (Llnkesch) and anagrellde
(Sllversteln)
AM Vannucchi, C Harrison, unpublished, 2

l U11 I WIN
Biologia molecolare delle MPN Highlightsfrom EH/
JAK2 Chr 9p24.1
FERM
MPL Chrl p34.2 ■ F b n
type II
CALR Chr 19 pl3.13
535 547 | V617F
SH2 JH2 exl2 JH1 (kinase)
li
in S505N S515N
I I
wsxw
TM JM ! 1
* 591 626 631
491 513 518
—I Q- CO N P
r m L Q mi
(typel mutation) 1 II Q- CO N p c 5-bp Insertion 1
1 (type2 mutation) 1 II ■ II mutant specific
Nonmutant CALR I II II
52-bp Deletion
sequence

l U11 I WIN
Biologia molecolare delle MPN Highlightsfrom EH/
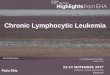
Pre- 5o, PMF 6%
10%
12% 67%
N= 286
Type 2-like 39% Type -| _|ike
57%
Essential thrombocythemia
Type 2-like 15%
Type 1-like 83%
Primary myelofibrosis
Overt- 14%
PMF 6% 4%
18%
►
N= 390
58%
JAK2V617F B
JAK2 Exl 2 CALR
Typel CALR Type2
MPZ.W515 Triple
Negativ
Pietra D et al, Leukemia 201 ( 30:431-8;
PV, ET: Database of CRIMM; Florence; PMF: Database AGIMM, Guglielmelli Petal, Blood 2017; 129:3227-36.

l U11 I WIN
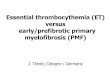
Biologia molecolare delle MPN Highlightsfrom EH/ Gene N= ASXL1 EZH2
SRSF2
IDH1/2
TET2
LNK/SH3B3
ZRSR2
SF3B1
SETBP1
DNMT3A
CSF3R
NRAS
CBL
U2AF1
RUNX1
TP53
133 12%
0 3%
2%
22%
2%
5%
3%
2%
2%
3%
0
1%
0 2% 1%
183 11%
3%
2%
1%
16%
0
3%
5%
2%
6% 3%
1%
1%
1% 2% 2%
Pre-PMF 27S 18%
4%
9%
3%
24%
5%
0
5%
0
4%
9% 4%
7%
3%
3% 4%
Overt MF
17%
3% 4%
8%
4%
4%
9%
4% 6%
1% 3%
Vannucchi AM etal, Leukemia 2013; 27:1861-9. TefferiAet al, BoodAdv 2016; 1:21-30; TefferiAetal, Blood Adv 2016; 1:105-111; Guglielmelli Pet al, Blood; 2017:129:3227-3

CUI1 IV-HN
Biologia molecolare delle MPN Highlightsfrom EH/
clinical practice guidelines
Philadelphia chromosome-negative chronic myeloproliferative neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
Vannucchi AM et al, Ann Oncol 2015; 26: v85-v9<

1 VS CUIIIVJIN
Biologia molecolare delle MPN Highlightsfrom EH/ High Molecular Risk Prognostic Category
harboring >1 mutation in any one of ASXL1, EZH2, SRSF2, IDH1/2
Overall Survival Blast Transformation
• A HMR status is associated with reduced OS and increased risk of blast transformation ir PMF patients independent of IPSS/DIPPS-plus
Vannucchi AM, et al. Leukemia. 2013;27:186

Influence of the Number of Mutations on OS and LFS in PMF
HMR mutations
Time (years)
Transformation to AML Number of mutations
100-
— 0 75- 1 — 2 50-
— 3-4 25-
0-
log rank p=0.0003
Years "io"
Number of mutations — 0 1
— 2 — 3-4
Guglielmelli P, et al. Leukemia. 2014; 28: 1804-1810. Lundberg P et al. Blood 2014;123:2220-2

l U11 I WIN
Biologia molecolare delle MPN Highlightsfrom EH/
Prognostically Relevant Non-Driver Gene Mutations in PV and ET
PV= 133 Mayo, 215 Florence 27-gene panel ET= 183 Mayo, 174 Florence PMF= 182 Mayo
Tefferi A. et al. Blood Adv 2016:1:21-30

1 VS CUIIIVJIN
Biologia molecolare delle MPN Highlightsfrom EH/ MYSEC (MYelofibrosis SECondarv to PV and ET)-PMF a Molecular-Enriched Prognostic Model • Includes 685 patients, 397 with PET-MF and 384 with PPV-M
Co variate HR (95% Cl) P value Points
Age at MF dx* 1.07 (1.05-1.09) <.0001 0.15
Hb <11 g/dL 2.3 (1.6-3.3 <.0001 2
Pit <150xl09/L 1.7 (1.2-2.5) .006 1
PB blasts >3% 2.9 (1.8-4.8 <.0001 2
CALR wt 2.6 (1.2-5.3) .001 2
Const, symptoms 1.5 (1.0-2.0) .03 1
* continuous, 0.15 point/year
• Of the HMR mutations, only SRSF2 mutations were significant for reduced OS in PET-MF.
Passamonti F et al. Leukemia 2017, in press; Rotunno G et al, AJH, 2016;91:6(

l U11 I WIN
Biologia molecolare delle MPN Highlightsfrom EH/ Clonal Hematopoiesis of Indetermined Potential
CL 3
o o cn JC u
■ <9
s ■ 3 < a o S 5= CO
o
6
5 - 4
-3-
Genes ■ ASXU U DNMT3A U GNAS U JAK2 U SF3B1 TET2 Total
2 ■
1 ■
T-r
<40 40-49 (o = 214) (n = 341)
.j 1 i i
50-59 60-69 (0 = 707) (0 = 767)
T
70-79 (0 = 475)
II 80-89
(o = 132) Age (years)
• Clonal hematopoiesis is increasingly common with aging (10% of persons older than 65 vs 1 % of <50y).
Thorsten Klampfl et al. Blood 2011;118:167-176; Xie M et al. Not Med. 2014 ;20(12):1472-8; Jaiswal S et al. N Engl JI 2014 Dec 25;371(26):2488-98; Genovese G et al. N Eng! J Med. 2014 25;371(26):2477-8; Jaiswal S et al, NEJM,:

l U11 I WIN
Biologia molecolare delle MPN Highlightsfrom EH/
Association with the risk of Hematologic Cancers and Coronary Heart Disease/Early Ml
A Hematologic Cancer Events/No. at Risk Hazard Ratio (95% Cl) P Value
No mutation (referent) 11/3208 JHS 10/2326 MEC 1/882
Mutation 5/134 <0.001 JHS 3/83 -■- 7.1 (2.0-25) 0.002 MEC 2/51 -*-I 36 (4.9-270) <0.001 Mutation, VAF ^0.10 5/57 M 49 (21-120) <0.001
JHS 3/34 -■- 21 (5.7-80) <0.001 MEC 2/23 -m 90 (29-280) <0.001
|-1-■ I ■ I » M|-1......... 1 10 100
B c P=0.002 by Wilcoxon test
o.o-i- No Hematologic Hematologic
Cancer Cancer
A CHIP and Coronary Heart Disease No. of Participants with
Subgroup Coronary Heart Disease/ No. at Risk
Biol mage No mutation (reference) 94/326 Mutation 19/44 MDC
No mutation (reference) 299/607 Mutation 21/33
Fixed-effects meta-analysis 0.7
Hazard Ratio (95% Cl) P Vali
1.8 (1.1-2.9) 0.03
2.o (1.2-3.i) o.oo:
1.9 (1.4-2.7) <0.00!
L0 5 4.0
B CHIP and Early-Onset Myocardial Infarction
No. of Participants with Myocardial Infarction/ Subgroup No. at Risk Odds Ratio (95% Cl)
ATVB No mutation (reference) Mutation PROMIS No mutation (reference) Mutation Fixed-effects meta-analysis
P Vali
<o.oo:
<o.oo: <o.oo:
Jaiswal S et al. N Engl J Med 2014;371:2488-2498 Jaiswal S et al. N Engl J Med 2017;377:111

Criteri Diagnostici CUII IV-HN
Highlightsfrom EH/ PV ET Pre-PMF Maior criteria Maior criteria Maior criteria
1. Hb >16.5g/dL in men, or 16.0 1. Platelet count >450xl09/L 1. BM biopsy with Mk g/dL in women, or Hct >49% 2. BM biopsy with proliferation proliferation and atypia, w/o and 48%, or increased RCM mainly of the Mk lineage with reticulin fibrosis >G1; with incr. 2. BM biopsy with hyper- mature enlarged Mk with cellularity, granulocytic prolifer. cellularity with panmyelosis and hyperlobulated nuclei and often decreased erythr'iesis Mk proliferation with 3. Not meeting WHO criteria for 2. Not meeting WHO criteria for
pleomorphic Mks other myeloid neoplasms other myeloid neoplasms 3. Presence of JAK2MS17? or 4. Presence of JAK2MS17?, 3. Presence of JAK2MSYJ?, JAK2 exl2 mutation CALR or MPL mutation
CALR or MPL mutation, or in the absence of these mutations, presence of another clonal marker, or absence of minor reactive BM reticulin Minor criteria l.Anemia
Minor criteria Minor criteria 2.Leucocytosis >llxl09/L 1. Subnormal sEPO levels 1. Presence of a clonal marker, or
absence of evidence of reactive thrombocytosis
3.Palpable splenomegaly 4.Increased LDH
3 major or first 2 major + minor 4 major or first 3+ minor 3 major + >1 minor
Overt PMF Major criteria
1. BM biopsy with Mk proliferation and atypia with either reticulin fibrosis G2-3 and/or collagen 2. Not meeting WHO criteria for other myeloid neoplasms 4. Presence of JAK2MS11?, CALR or MPL mutation, or in the absence of these mutations, presence of anothei clonal marker, or absence of reactive myelofibrosis Minor criteria 1. Anemia 2. Leucocytosis >llxl09/L 3. Palpable splenomegaly 4.Increased LDH 5. Leukoerythroblastosis
3 major + >1 minor
In the absence of any of the 3 major clonal mutations, the search for the most frequent accompanying mutations (eg, ASXL1, EZH2, TET2, IDH1/IDH2, SRSF2, SF3B1) are of help in determining the clonal nature of the disease.
Arber DAetal, Blood 2016; 127:2391-4

Studi Clinici CUIIHU IN
Highlightsfrom EH/ 1JAK inhibitor (Company) MF PV/ET Note
phase, status
CEP701 (Cephalon) STOP
AZD1480 (AstraZeneca) STOP
XL019 (Exelixis) STOP
NS-018 (NS Pharma) 1 ?
BMS-911543 (BMS) I/II ? LY2784544 (Lilly) II 1 STOP
Momelotinib (Gilead) III, lst/2nd line COMPLETE --->
Pacritinib (CTI) III, lst/2nd line COMPLETE, on Hold-->re-test
Fedratinib (Sanofi) III, lst/2nd line l/ll STOP
Ruxolitinib (Incyte/Novartis) 111(2) II (ET,PV) III (PV) MF & PV 2nd line APPROVED

Studi Clinici l U11 I WIN
Highlightsfrom EH/
COMFORT I
Patients with MF (N = 309)
Randomized 1:1 <
Ruxolitinib 15 mg BID or
20 mg BID
Placebo BID
_II COMFORT II
Patients with MF (N = 219)
Randomized / 2:1 \
Ruxolitinib 15 mg BID or
20 mg BID
Best available therapy (BAT)
Primary Endpoint • Number of subjects achieving >35% reduction in spleen volume* from baseline to week 24 Secondary Endpoint • Proportion of patients with >50% reduction in Total Symptom Score (mod. MFSAF v2.0 electronic diary)
Primary Endpoint • Number of subjects achieving > 355 reduction in spleen volume* from baseline to week 48 Secondar/Exploratorv endpoints • Changes in functioning and sympto
Ruxolitinib MTD: 25 mg twice daily or 100 mg once daily with thrombocytopenia as DLT
* As measured by MRI/CT scan Verstovsek S et al. NEJM 2012; 366:799-807; Harrison C et al. NEJM 2012; 366:787

Studi Clinici I VS CUII IvIN
Highlightsfrom EHP
Resistance to or intolerance of HU (modified ELN criteria) Phlebotomy requirement Nonpalpable spleen
Prerandomization (day -35)
Hct, 40%-45%
RESPONSE: Spleen >5 cm
ECOG PS < 2
Ruxolitinib 10 mg bid
n = 74
Extended treatment phase H > Week 26
Crossover to ruxolitinib
>|-^Week 26
n = 75 Week 28 (pr imary analysis)
Week 80 _
RESPONSE: Week 32
Final analysis
• Ruxolitinib-randomized patients had their doses individually titrated for efficacy and safety (to a maximum of 25 mg bid) • Investigator-selected BAT as monotherapy included HU (at a tolerated dose if the patient were likely to receive benefit), interferon (IFN)/peg-IFN, anagrelide, pipobroman, immunomodulatory drugs, or observation • All patients received low-dose aspirin unless medically contraindicated
bid, twice daily; VannucchiAM et al, NEJM2015; 372:426; Passamonti F et al, Lancet Oncol 2017; 18:88-'

Studi Clinici l U11 I WIN
Highlightsfrom EH/ Target Hematocrit for Optimal Management of PV: Results of the CYTO-PV Stud
n HCT HCT <45% 45-50% HR P
N = 182 N=183 (95%CI)
Primary Endpoint (CV death, MI, stroke, PAT, DVT, PE, TIA, abdominal thrombosis)
5 (2.8%)
18 (9.8%)
3.91 (1.45- 10.53)
0.005
IR % person/year 1.1 4.4
Total CV events (Primary plus superficial vein thrombosis)
8 (4.4%)
20 (10.9%)
2.69 (1.19- 6.12)
0.012
IR % person/year 1.9 5.0
Marchioli R, et al. NEJM. 2013; 368:22-

Studi Clinici l U11 I WIN
Highlightsfrom EH/ Symptoms burden in MPN
Significant symptom heterogeneity exists within each MPN subtype, sometimes independent c disease features or prognosis, i.e. symptoms are prominent even in low-risk MPN populations.
100%
■ ET(N=874)
■ PV(N=729)
MF (N=486)
■ MPN Total (N=2089)
10
> Q> LD
E o -t-> Q.
E IS)
c fD
ET(N=874)
PV(N=729)
MF (N=486)
MPN Total (N=2089)
(/I VI
o u =■ 3 £ 00 CO
2- Q; 15 Z c o
2 c o
w 0 H
CUD £
c '<5
k. 01 >
VI VI
£ > v IE Q. 01
*-» «c bp ai
% E Qi Ml i
8 E E o o ■O o -Q .52
U ■ C
TO L 0 c 01
? v> £
u OJ c o CO
u_ £ bp *5
5
5 o.
S Ui
< *D u c o u
CUO Z
5
Geyer et al, Blood, 2014

Studi Clinici
PHYSICIANS
ET - Prevent vascular events -Slowor
delay condition Healthy blood
counts ■ Better QoL ^Symptom
improvement Reduction in spleen
size Reduce frequency of
phlebotomy
PV - Prevent vascular events
-Slowor delay condition
Healthy blood counts ■
Better QoL ^Symptom
improvement Hematocrit
<45% Reduce
phlebotomies Reduce
spleen size
MF — Prevent vascular
events
— Slow or delay condition
Healthy blood counts
— Better QoL
^Symptom improvement
Anemia treatment Reduce
blood transfusion Reduce
spleen size
CUIIIVJIN
Highlightsfrom EH/
PATIENTS
ET - Prevent vascular events
- Slow or delay condition Healthy
blood counts
- Better QoL
^Symptom improvement Reduction
in spleen size Reduce frequency of
phlebotomy
PV
MF
- Prevent vascular
events
- Slow or delay condition
Healthy blood counts
■ Better QoL
- Symptom improvement
Hematocrit <45% Reduce
phlebotomies Reduce
spleen size
— Prevent vascular
events
— Slow or delay
condition Healthy blood
counts
■ Better QoL ^Symptom
improvement Anemia
treatment Reduce
phlebotomies Reduce
spleen size
Mesa R et al, 2i

Prossimi 10 anni: wish list CUIIIVJIN
Highlightsfrom EH/
• Definire le forme Triplo-Negative • Sviluppare score molecolari piu performanti • Diagnosi multiparametrica (senza BOM?) • Parametri predittivi di evoluzione in sMF e LA • Terapie “eradicanti” (?) • Rischio di trombosi ancora elevato • Immunoterapia (?) • Controllo duraturo della patologia

Prossimi 10 anni l U11 I WIN
Highlightsfrom EH/ II Futuro negli Studi clinici nelle MPN — c o m e la
vedo?

Prossimi 10 anni l U11 I WIN
Highlightsfrom EH/ II Futuro negli Studi clinici nelle MPN — c o m e la
vedo?
"Dov'e che sono? Mi sembra di non stare in nessun posto. Ma se la morte e cosi, non e un bel lavoro. Sparito tutto: la gente, gli alberi, gli
uccellini per aria, il vino...Te cul”
AMARCORD, Federico Fellini (1973)

Report del gruppo di lavoro • F Silvestri Udine • L Pedrazzi Modena • C Gasparrini Campobasso • S Santini Prato • E Ruggeri Milano • L Cimarosto Belluno • F Ballerini Genova • 0 Racchi Genova • G Lo Scocco Firenze • R La Tagliata Roma • AM Vannucchi Firenze • A. Tondo Firenze-Meyer • G Musardo Faenza • E Raviolo Cuneo • F Faccinelli Perugia • T Petrucci Roma

Report del gruppo di lavoro • F Silvestri Udine • L Pedrazzi Modena • C Gasparrini Campobasso • S Santini Prato
• E Ruggeri Milano G TOdt f U11!!!!! • L Cimarosto Belluno • F Ballerini Genova • 0 Racchi Genova • G Lo Scocco Firenze • R La Tagliata Roma • AM Vannucchi Firenze • A. Tondo Firenze-Meyer • G Musardo Faenza • E Raviolo Cuneo • F Faccinelli Perugia • T Petrucci Roma

Cugina 73 anni
1- BOM: si per conoscenza scientifica 2- BOM: potrebbe essere non tanto ET o prePMF ma una PMF iniziale
3- Regole WHO: difensiva nostra?
4- Cambia trattamento ? NO 4-
prospettiva ?

OS and LFS in relation to diagnosis and IPSS risk categories in study patients population.
A
C 1.0 ■ „L„, Pre-PMF
0.8 ■ Overall survival O O 05 _i_i_
\ \ 1-1 LOW t INT2
0.2 ■ HIGH |
0.0 ■ 1 P<.0001 -i-i-i-i-i-r 0 5 10 15 20 25 30
Years
B
D
0 5 10 15 20 25 30
Years
Paola Guglielmelli et al. Blood 2017;129:3227-3236
©2017 by American Society of Hematology * blood

Diagnosi di Policitemia Vera:
Qunti sani giovani hanno un valore a livello WHO?
Come rendere cost-effective il percorso dx Iter
mutazionale Apnee notturne

Triple-negativity • Istopatologia: non differenze evidenti • Fenotipo clinico
• Permane incertezza ???
• Forte implicazione diagnostica nella MF
• Implicazioni di gestione nella ET

Albumina
•And so what?
•Critica interpretazione
•Utilizzazione terapeutica ??
•Si va verso score “oggettivi”

Interferone:
• Dati???
• Progressione??? • Non pud cambiare OGGI il nostro approccio terapeutico

Ruxolitinib:
• PV: quanti e quali pazienti? • MF: basse dosi? • Precoce • Discussione sulle inicazini in base alia classe di rischio
Timing del trapianto (Carella)