-
Leucemia acuta linfoblastica
F. Ferrara
-
Boiers C, EHA,2015
EDUCATIONAL PROGRAM
-
Boiers C, EHA,2015
-
Boiers C, EHA,2015
-
Boiers C, EHA,2015
Quiescent leukaemic cells account for minimal
residual disease in childhood lymphoblastic leukaemia.
-
Boiers C, EHA,2015
-
The need to eliminate highly quiescent cALL cells
providesaplausible explanation for the requirement for prolonged
(23 years) maintenance therapy to achieve durable
clinicalremissions in cALL.
It also provides a plausible explanation for cALL cases, in
whichthe relapse clone resembles the presentation leukaemic clone
up to 8 years between diagnosis and relapse.
-
Boiers C, EHA,2015
-
Moorman A, EHA, 2015
EDUCATIONAL PROGRAM
-
Moorman A, EHA, 2015
-
Moorman A, EHA, 2015CNA: copy number alterations
(microdeletions, point mutations)
-
Moorman A, EHA, 2015
-
Moorman A, EHA, 2015
Children/adolescents Adults
-
Most relevant abstracts
One session: Immunotherapy of ALL
-
EFFICACY AND SAFETY OF INOTUZUMAB OZOGAMICIN (INO) VS STANDARD
OF CARE (SOC) IN SALVAGE 1 OR 2 PATIENTS WITH ACUTE LYMPHOBLASTIC
LEUKEMIA (ALL): AN ONGOING GLOBAL PHASE 3 STUDY
De Angelo et al, Late Breaking Abstract 2, EHA 2015
In this phase 3 trial (NCT01564784), patients were randomized
to
InO (starting dose 1.8 mg/m2/cycle [0.8 mg/m2 on d1; 0.5 mg/m2
on d8 and 15 of a 2128 d cycle [6 cycles])
or
SOC (either FLAG, or HAM, or HD-ARA-C).
A split- design was used for 2 primary endpoints: 1) CR or Cri
2) OS
Secondary endpoints: duration of remission (DOR), MRD-neg;
-
De Angelo et al, Late Breaking Abstracts 2, EHA 2015
Survival data blinded and expected in 2016
-
For InO vs SOC, Gr3 hepatobiliary AEs occurred in 9% vs 3%
pts;
Any grade veno-occlusive liver disease (VOD) occurredin 15 vs 1
pts (Gr3, 13 vs 1 pts).
More patients proceeded to allogeneic SCT with InO(n=48) vs SOC
(n=20)
In the InO arm, 5 VOD cases (2 in pts with prior SCT) occurred
during treatment and 10 after subsequentSCT (2 fatal).
TOXICITY
De Angelo et al, Late Breaking Abstracts 2, EHA 2015
-
INOTUZUMAB OZOGAMICIN IN COMBINATION WITH LOW-INTENSITY
CHEMOTHERAPY (MINI-HYPER-CVD) FOR THE FRONTLINE THERAPY IN
ELDERLY
PATIENTS (>60 YEARS) WITH ACUTE LYMPHOBLASTIC LEUKEMIA
(ALL)
Pts 60 years (yrs) with newly-diagnosed B-cell ALL were
eligible.
Mini-hyper-CVD (cyclophosphamide and dexamethasone at 50% dose
reduction, no anthracycline, methotrexate at 75% dose reduction,
cytarabine at 0.5 g/m2 x 4 doses). Rituximab and intrathecal
chemotherapy were given for first 4 courses.
INO was given on Day 3 of each of the first 4 courses. The first
6 pts received 1.3 mg/m2 for cycle 1 followed by 0.8 mg/m2 for
subsequent cycles;
Pts 7 onwards received 1.8 mg/m2 for Cycle 1 followed by 1.3
mg/m2 for subsequentcycles.
Jabbour et al, Abs S114, EHA 2015
-
Jabbour et al, Abs S114, EHA 2015
-
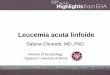
MiniHCVD-INO in ALL. Outcome
N=28 pts
N=1
Resistant
N=27
responders
22 CR; 5 CRp
N=2
Relapse
N=0
Early death
N=1
Died of PD
N=1
Allo-SCT
N=4
Died in CR/CRp
2 Sepsis
1 Gunshot wound
1 Unknown
N=17
POMP maintenanceN=3
Consolidation
Median follow up of 15 months (4-31)
N=2
Died of PD
Jabbour et al, Abs S114, EHA 2015
-
CAR-T
-
T Cells Engineered with a Chimeric Antigen Receptor (CAR)
Targeting CD19 Have Long Term Persistence and Induce Durable
Remissions in Relapsed,
Refractory ALL.
-
PENNCHOPMSKCC
-
EFFICACY AND SAFETY OF CD19-TARGETED 19-28Z CAR MODIFIED T CELLS
IN ADULT PATIENTS WITH RELAPSED OR REFRACTORY B-ALL
Park J, Abs S112, EHA 2015
Adult patients with R/R B-ALL underwent leukapheresis, and T
cells were transduced with a gammaretroviralvector encoding a CAR
construct composed of anti-CD19 scFv linked to CD28 and CD3
signaling domains (19-28z).
All patients received conditioning chemotherapy followedby
13x106 19-28z CAR T cells/kg.
-
33 patients have been treated, and 32 patients are evaluable for
response.
The median age was 54 years (range, 22-74).
12 patients (36%) had Ph+ ALL
11 patients (33%) had prior allo-SCT
14 patients (42%) had 3 prior lines of therapy.
Park J, Abs S112, EHA 2015
-
19-28z CAR T cells can induce a high CR rate of 91% in
adultpatients with R/R ALL.
The risk of sCRS correlates with disease burden and can be
effectively managed.
These findings strongly support the use of 19-28z CAR T cellsin
adults with R/R ALL and warrants investigation in a phase2
trial.
Park J, Abs S112, EHA 2015
-
CHIMERIC ANTIGEN RECEPTOR (CAR)-MODIFIED T CELLS TARGETING CD19
INDUCE SUSTAINED REMISSIONS IN CHILDREN
AND YOUNG ADULTS WITH RELAPSED/REFRACTORY ALL
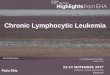
Maude S, Abs S111, EHA 2015
Aims
Establish the safety and efficacy of CTL019 for patients with
relapsed/refractoryCD19+ ALL.
Methods
After informed consent, T cells collected from the patient were
transduced with a lentiviral vector encoding a CAR composed of
anti-CD19 scFv, CD3z, and 4-1BB domains, activated/expanded ex vivo
with anti-CD3/anti-CD28 beads, cryopreserved, and then infused.
35/40 patients received lymphodepleting chemotherapy the week prior
to cell infusion
-
93 92
25
93
0
10
20
30
40
50
60
70
80
90
100
CR CR MRD- RELAPSE CRS
Maude S, Abs S111, EHA 2015
RESULTS
-
Most responding pts developed grade 1-4 CRS at peak T
cellexpansion (increases of IL6 and IFN, both up to 1000x, and
IL2R).
Treatment for CRS was required for hemodynamic or
respiratoryinstability in 37% of patients and was rapidly reversed
in all caseswith the IL6-receptor antagonist tocilizumab, together
with corticosteroids in 5 pts.
Grade 4 CRS was strongly associated with high disease
burdenprior to infusion and with elevations in IL-6, ferritin
(suggestingmacrophage activation syndrome) and CRP.
Although T cells collected from pts who had relapsed after allo
SCT were median 100% donor origin, no GVHD has been seen.
CRS
Maude S, Abs S111, EHA 2015
-
Maude S, Abs S111, EHA 2015
-
PENN University
Maude S, Abs S111, EHA 2015
-
Single-agent CTL019 immunotherapy can induce potent and durable
responses in patients with R/RALL.
CRS was effectively controlled with IL6 blockade.
Long-term disease control is possible withoutsubsequent stem
cell transplantation
Conclusions
Maude S, Abs S111, EHA 2015
-
Such TRUCK T cells are moreover envisioned to be
applied in fields beyond cancer therapy including the
therapy of virus infections, auto-immune diseases
or metabolic disorders.
TRUCK T cells
-
CAR-T or TRUCK T CELLS : FURTHCOMING ISSUES
For all relapsing patients ?
For first, second or subsequent relapse ?
For patients who are candidate to SCT ?
For the treatment of MRD+ patients ?
Costs and feasibility
-
QUESTIONS
Is it time for a new integrated diagnostic/prognostic
classification(MOL/GEN BASED) in ALL (either for children or
adults) ?
Which is the role of new monoclonal antibodies (Blinatumomab,
Inotuzumab-GO) in the treatment of ALL ?
Which patiens should receive CART therapy ?