Embed Size (px)
Citation preview

1
The Role of Comprehensive Mental Health Law Reform in
System Transformation Richard J. Bonnie

2
Part I

3
Background
• Commission on Mental Health Law Reform conceived in late 2005 by Chief Justice Hassell in response to widespread and growing dissatisfaction with the operation of the civil commitment process and with increasing involvement of persons with mental illness in the justice system
• Complaints about the commitment process from all stakeholders. No one satisfied…with practices or results

4
Sample Complaints about Commitment Process
• ECO process: too short, beds not available, inefficient for L/E officers
• Transportation burden on LE and stigmatizing for patients
• Pressures on EDs• Unfair procedures (complaints from both families
and patients)• Inadequate fees and reimbursements• Inconsistent interpretations of law• Unduly restrictive interpretations of criteria,
especially “imminence” requirement

5
Other Concerns
• Widespread despair about avoidable criminalization of people mental illness: about 15% of the jail population has serious mental illness, as do about 45% of children in delinquency detention facilities.
• Frustration that families too often need to seek judicial assistance to get access to mental health services for children and adolescents (e.g., relinquishing custody)

6
The Underlying Problem
• Chief Justice convened planning group in spring, 2006 to develop charge for Commission.
• It soon became apparent that all these problems are to some extent spillover consequences of gaps in community mental health services
• Too many people with MH problems are not getting the help they need when they need it to prevent crises or ameliorate them before they spiral out of control
• Problems will not be solved solely by tinkering with the law. Solution requires closing gaps in the mental health services system.

7
Goals of Comprehensive Reform
• Reduce need for commitment and other types of judicial involvement and prevent criminalization of mental illness by enhancing access to services to prevent crises or ameliorate them… and by drawing people into services by their own choice – system transformation is also “law reform”
• Facilitate diversion from criminal justice system in appropriate cases and provide needed services while in CJS
• Redesign commitment process so that is more fair and effective…. Coercion should be used as last resort, and only when necessary….– but when it is needed, it should be used and… – when it is used, it should be used effectively…AND
fairly

8
Commission Research
• Survey experiences and attitudes of stakeholders in late 2006-early 2007.
• Study of hearings in May 2007
• Study of face-to-face crisis contact evaluations by CSBs in June 2007

9
Key Findings: Big Picture
• Around 50,000 crisis contact evaluations are conducted by CSB staff each year, and this does not include an undetermined number of such evaluations in EDs and elsewhere that do not involve CSBs. (About 5,000 of these evaluations involve children.)
• Almost 50% of these evaluations involve people who are not currently in treatment (ranges from 1/3 to 2/3 in different CSBs).
• More than 40% of persons in crisis have no insurance

10
Key Findings: Big Picture
• About 10,000 people are in police custody when these evaluations are conducted. (Does not include MI people who have been arrested.)
• About 2,000 of patients are in jail when CSB evaluation (manly for transfer to hospital) is sought -- a small fraction of the severely MI people in jail (and doesn’t count forensic IST evaluations)

11
Key Findings: Big Picture
• Although most people accept treatment voluntarily while in crisis, commitment proceedings are initiated in about 20,000 cases per year (40%). (About 600 involve children.)
• About 80% of these proceedings result in hospitalization (50% involuntary, 30% voluntary)
• Mandatory Outpatient Treatment (MOT) is rare (about 5%)
• About 15% of cases are dismissed

12
Key Findings: Big Picture
• Documented wide variations in practice, not only on procedures but also in outcomes, based on different interpretations of the criteria.
• Indicators of service gaps:– Access to immediate medication evaluation– Intensive crisis response alternatives to
hospitalization– Outpatient services

13
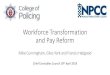
Illustrative Findings Regarding Outcome Variations
• The findings from CSB crisis contact study are preliminary
• Slides should not be reproduced or cited without permission from Professor Bonnie

14
55.346.9
32.6
58.7
29.5
77.1
41.329.2
40.937.8
69.7
49.542.9
29.3
46.847.5
53.8
22.6
38.9
20
22.2
16.7
39.1
47.452.6
5048.7
40.5
56.6
46.3
34.1
43.340.4
30.8
44.7
44.6
19.727.2
0
13.8
43.1
0
15
30
45
60
75
90
Community Service Boards in Virginia
STATE, n=2869 1, n=48 2, n=22 3, n=45 4, n=1755, n=103 6, n=56 7, n=37 8, n=47 9, n=6110, n=39 11, n=115 12, n=72 13, n=85 14, n=2015, n=216 16, n=6* 17, n=87 18, n=19 19, n=1920, n=62 21, n=76 22, n=42 23, n=53 24, n=10825, n=138 26, n=60 27, n=99 28, n=104 29, n=6430, n=46 31, n=103 32, n=65 33, n=66 34, n=10335, n=138 36, n=11 37, n=44 38, n=58 39, n=10940, n=48
*CSB has less than 10 cases
Percent of Crisis Contacts in which Involuntary Action was Taken by CSB
CSB Study 2007

15
17.48.7
013.6
10.312
30.818.2
36.618.2
13.510
18.20
2.61.9
19.226.1
2.639.2
9.125
6.80
13.335.7
33.327.1
020
21.715.3
0 10 20 30 40 50
VIRGINIA
1, n=23
2, n=10
3, n=17
4, n=48
5, n=30
6, n=14
7, n=15
8, n=27
9, n=59
10, n=24
11, n=11
12, n=79
13, n=38
14, n=46
15, n=52
16, n=104
17, n=39
18, n=15
19, n=11
20, n=20
21, n=37
22, n=11
23, n=41
24, n=22
25, n=13
26, n=92
27, n=29
28, n=22
29, n=61
30, n=23
31, n=138
Per
cen
t N
egat
ive
to C
om
mit
Negative Independent Examiner Certifications by District Court
District Court Hearing Study 2007

16
47.960.9
32.851.9
74.33838.5
5045.5
58.347.6
7063.6
68.464.4
87.750
2010.5
52.9100
29.630.2
25.966.7
57.130
62.941.2
72.717.4
49.2
0 25 50 75 100
VIRGINIA
1, n=23
2, n=11
3, n=17
4, n=62
5, n=30
6, n=14
7, n=15
8, n=27
9, n=63
10, n=27
11, n=10
12, n=87
13, n=38
14, n=45
15, n=52
16, n=106
17, n=45
18, n=19
19, n=11
20, n=20
21, n=42
22, n=12
23, n=44
24, n=34
25, n=13
26, n=100
27, n=35
28, n=27
29, n=64
30, n=23
31, n=140
Per
cen
t o
f C
ases
Res
ult
ing
in
Invo
lun
tary
Co
mm
itm
ent
for
In-P
atie
nt
Tre
atm
ent
Hearing Disposition by District Court, Involuntarily Committed to Inpatient Treatment
District Court Hearing Study 2007

17
7.10
10.90
2.94
00
6.80
11.95
27.30
8.96.6
7.717.8
09.2
00
1.611.1
6.700
4.811.8
00
5.7
0 10 20 30
VIRGINIA
1, n=23
2, n=11
3, n=17
4, n=62
5, n=30
6, n=14
7, n=15
8, n=27
9, n=63
10, n=27
11, n=10
12, n=87
13, n=38
14, n=45
15, n=52
16, n=106
17, n=45
18, n=19
19, n=11
20, n=20
21, n=42
22, n=12
23, n=44
24, n=34
25, n=13
26, n=100
27, n=35
28, n=27
29, n=64
30, n=23
31, n=140
Per
cen
t o
f C
ases
Res
ult
ing
in
Ord
er o
f In
volu
nta
ry O
ut-
Pat
ien
t T
reat
men
t
Hearing Disposition by District Court, Ordered to Obtain Outpatient Treatment
District Court Hearing Study 2007

18
43.639.1
48.440.7
14.331
15.432.4
2516.7
38.15
031.6
26.75.7
19.246.7
89.52.3
037
50.844.4
6.77.16.7
3.247.1
18.260.9
29
0 25 50 75 100
VIRGINIA
1, n=23
2, n=11
3, n=17
4, n=62
5, n=30
6, n=14
7, n=15
8, n=27
9, n=63
10, n=27
11, n=10
12, n=87
13, n=38
14, n=45
15, n=52
16, n=106
17, n=45
18, n=19
19, n=11
20, n=20
21, n=42
22, n=12
23, n=44
24, n=34
25, n=13
26, n=100
27, n=35
28, n=27
29, n=64
30, n=23
31, n=140
Per
cen
t o
f C
ases
in w
hic
h R
esp
on
den
t V
olu
nta
rily
Ad
mit
ted
fo
r In
-Pat
ien
t T
reat
men
t
Hearing Disposition by District Court, Voluntarily Admitted for Inpatient Treatment
District Court Hearing Study 2007

19
1.40
6.33.7
8.627
38.517.6
22.725
2.420
9.1000.9
17.32.2
035.6
033.3
17.514.8
2035.7
63.322.6
09.1
21.714.6
0 20 40 60 80
VIRGINIA
1, n=23
2, n=11
3, n=17
4, n=62
5, n=30
6, n=14
7, n=15
8, n=27
9, n=63
10, n=27
11, n=10
12, n=87
13, n=38
14, n=45
15, n=52
16, n=106
17, n=45
18, n=19
19, n=11
20, n=20
21, n=42
22, n=12
23, n=44
24, n=34
25, n=13
26, n=100
27, n=35
28, n=27
29, n=64
30, n=23
31, n=140
Per
cen
t o
f C
ases
Dis
mis
sed
Hearing Disposition by District Court,
Case Dismissed and Respondent Released
District Court Hearing Study 2007

20
Frequency of Dismissal by Judge
# of Judges # of Cases Heard # Dismissed/Rate
All (66) 1284 187 (14.6%)
8 326 99 (30.4%)
7 390 5 (1.3%)

21
Original Commission Game Plan
• Began 10/06 with 2-year work plan for comprehensive reform
• 5 task forces to report in fall, 2007: commitment, access to services, criminal justice, children and adolescents, empowerment and self-determination
• Final report in fall, 2008

22
Aims of Task Forces
• Facilitate access to mental health services for persons in need
• Remove unwarranted impediments to needed treatment for people in crisis who fail to seek treatment on their own while assuring adequate screening and respecting individual rights
• Improve the quality and effectiveness of the involuntary commitment process to assure due process and promote consumer well-being

23
Aims of Task Forces
• Facilitate engagement and empowerment of persons with severe mental illness based upon the fundamental and essential principle of human dignity
• Assure access to services for all children and adolescents with mental health and/or substance abuse service needs so that these juveniles and their families are not forced to seek judicial assistance to obtain needed services

24
Aims of Task Forces
Divert individuals with mental illness from the criminal justice system to the maximum extent consistent with the goals of criminal justice and increase access to appropriate mental health services for individuals with mental illness while detained, incarcerated or under community supervision

25
Then Tragedy on April 16, 2007
• Tech shootings called public attention to some of problems we were addressing
• E.g., inadequacy of evaluation process and weaknesses of law relating to mandatory outpatient treatment (MOT) resulted in missed opportunities to “connect the dots” about Cho’s problems in 12/05
• Created momentum for law reform and increased funding for community services, reinforced by Tech Panel report in late August

26
Tech shootings accelerated the timetable of reform …
• Commission accelerated its deliberations
• Challenge: Take advantage of opportunity to contribute to commitment law reforms while preserving goal of comprehensive reform
• In 12/07, Commission released blueprint for comprehensive reform with specific priorities for 2008

27
… and added new items to the list
• Relation between health information privacy and commitment process (Commission appointed new TF)
• Federal and state firearm reporting
• College mental health and FERPA

28
Remarkable Political Consensus
• Companion bi-partisan bills embraced by Governor Kaine and leadership of both Houses
• $42 million for community mental health services was untouchable
• Approx 150 bills introduced
• General Assembly did an excellent job of crafting a reform bill

29
Main Changes
• Modify commitment criteria to promote consistency and avoid unduly restrictive interpretations
• Improve quality of decision-making process from ECO/TDO through hearing (tied to $$ for CSBs)
• Specify procedures for MOT Orders, and clarify responsibilities (tied to $$ for CSBs)
• Clarify authority to disclose health information during commitment process but protect it from further disclosure
• Facilitate “drop-off” by person under ECO or in lieu of arrest by law enforcement to suitably licensed mental health facility

30
Part II

31
Taking Stock
• Events of past year heightened public awareness of gaps in services and weaknesses in the law that compromise the effectiveness of involuntary treatment
• If properly implemented, legal reforms should promote greater accuracy, effectiveness, and fairness in commitment process
• Increased resources ($42 million) for emergency services, case management and outpatient services can begin to close gaps in access

32
BUT…there are risks
• Loss of opportunity for comprehensive and sustained reform due to loss of public and legislative attention.
• Limited commitment reforms in response to the Tech shootings might increase stigmatization by reinforcing the erroneous perceptions that mental illness is strongly associated with violence, and that more coercion and less privacy provide the solution.
• These are real risks.

33
The message as we move forward
• Budget increase in 2009-10 biennium is only a down payment on a long-term investment in community mental health services
• Changes in commitment law are only first step in comprehensive reform.
• A key aim of mental health law reform is to lay legal foundation for a mental health system that mainstreams recovery-oriented services, reduces stigmatization, empowers consumers and gives them a meaningful measure of control over the services they receive.
• Another critical aim is to realign the mental health and criminal justice systems

34
How will we measure success?
• Public discourse about mental health law reform often makes it seem that we have to make trade-offs between public safety and individual liberty and privacy (the 9/11 paradigm)
• This implies that more commitments will be a measure of success.

35
How will we measure success?
• The surest path to pubic safety is not more coercion and less privacy for people with mental health problems, but rather establishing conditions that will lead to deeper and more enduring engagement of people with mental health needs in the services system.
• Over time, the best indicator of success of mental health system reforms is fewer TDOs and commitments, not more TDOs and commitments.

36
Commission Activities in 2008
• Develop the vision for establishing community service capacity, and a specific 6-year plan for implementation; study innovations in other states
• Monitor, evaluate and consolidate 2008 reforms
• Unfinished business in comprehensive mental health law reform

37
Unfinished Business on Comprehensive Law Reform
• Commission asked to study a number of bills introduced in 2008 and carried over
• Many components of Commission’s blueprint were not put forward in 2008 because they needed further study.

38
Unfinished Business on Commitment law Reform
• Transportation – three-tiered model based on risk• Extension of TDO period?• Compensation for SJs, counsel, IEs?• Counsel for petitioner?• Bifurcated commitment orders?• Access to Hearings?• Admission of assenting patients by guardians and health
care surrogates?• Lower threshold for MOT?• Many other proposed changes in TF reports

39
Other Important Unfinished Business on Mental Health Law Reform
• Implement recommendations of Task Force on Empowerment and Self-Determination, especially development of legislative proposal on advance directives for health care decisions in contexts other than end-of-life care, including mental health care: A major priority in 2009
• Implement recommendations of Task Force on Children and Adolescents
• Issues related to crisis intervention, commitment, information sharing, and continuity of care for college and university students with mental health problems

40
Need for Caution
• 2008 reforms should be adequately evaluated before major additional changes are made.
• For MOT in particular, attention needs to be paid to the risk that MOT orders will swallow up resources for voluntary OP services. Any new steps in 2009 should be limited to opportunity for local innovation.

41
Schedule
• Report in November to Joint Commission on Health Care
• Report in December to legislative committees on bills referred to Commission for study
• It all begins again in January, 2009

42
Stay Tuned