Embed Size (px)
Citation preview

Universidad Autónoma de Guadalajara1
The gastrointestinal tractThe gastrointestinal tract
Regulation and motility Regulation and motility part 1part 1
Dra. Ma. Elena Torres ZazuetaDra. Ma. Elena Torres Zazueta

Universidad Autónoma de Guadalajara2
Objectives
• Describe the overall role of the gastrointestinal system with respect to the whole body balance of water, electrolytes, carbohydrates, fats, and proteins. Include the processes of digestion, absorption, metabolic production, metabolic consumption, secretion, and excretion.

Universidad Autónoma de Guadalajara3

Universidad Autónoma de Guadalajara4
INTEGRATED RESPONSE TO A MEAL
From: Silverthorn. Human Physiology. 2nd Edition
Prentice Hall

Universidad Autónoma de Guadalajara5
Objectives• Describe the histoanatomical characteristics of the
enteric nervous system. Given either a cross section or a longitudinal section of the intestine, name and locate the myenteric and submucosal plexus.
• Contrast the sympathetic and parasympathetic modulation of the enteric nervous system and the effector organs of the GI tract.
• Classify the following enteric nervous system neurotransmitters as excitatory or inhibitory: norepinephrine, acetylcholine, CCK, VIP, histamine, and somatostatin.
• Describe the similarities and differences in regulating gastrointestinal function by nerves, hormones, and paracrine regulators. Include receptors, proximity, and local vs. global specificity.

Universidad Autónoma de Guadalajara6

Universidad Autónoma de Guadalajara7

Universidad Autónoma de Guadalajara8
NEURONS OF THE ENTERIC NEURONS OF THE ENTERIC NERVOUS SYSTEMNERVOUS SYSTEM

Universidad Autónoma de Guadalajara9
NEURONS OF THE ENTERIC NEURONS OF THE ENTERIC NERVOUS SYSTEMNERVOUS SYSTEM

Universidad Autónoma de Guadalajara10

Universidad Autónoma de Guadalajara11

Universidad Autónoma de Guadalajara12
The Enteric The Enteric Nervous Nervous
System and it System and it relationship relationship
with the ANS with the ANS

Universidad Autónoma de Guadalajara13

Universidad Autónoma de Guadalajara14
•Form hollow structures, do not contract against skeleton•Electrically coupled, gap junctions, contracts as syncitium•Actin:myosin ratio 15:1 (skeletal muscle 2:1)•Not striated, neurotransmitter released from varicosities•Have slow wave activity
From: Silverthorn. Human Physiology
Prentice Hall
Intestinal smooth muscleIntestinal smooth muscle

Universidad Autónoma de Guadalajara16
From: Silverthorn. Human Physiology Prentice Hall

Universidad Autónoma de Guadalajara17
Ca++Ca++
Ca++Ca++CalmodulinCalmodulin
Ca++ -Ca++ - CalmodulinCalmodulin
Inactive myosin Inactive myosin light chain kinaselight chain kinase
Active myosin Active myosin light chain kinaselight chain kinase
Muscle Muscle contractioncontraction
Phosphorilated myosin light chain

Universidad Autónoma de Guadalajara18

Universidad Autónoma de Guadalajara19
FUNCTIONS OF MOTILITY
• PROPULSION -propagated contractions-
• MIXING
- Mechanical dispersion
- Contact with digestive secretions
- Increasing contact with absorbing cells
• RESERVOIR FUNCTION
- Stomach
- Gallbladder
- Colon

Universidad Autónoma de Guadalajara20

Universidad Autónoma de Guadalajara21
Objectives
• State the stimulus that initiates the swallowing sequence. Identify the point at which the swallowing sequence becomes automatic (independent of voluntary control).
• Identify the normal resting esophageal pressure and explain why this pressure varies with the respiratory cycle.
• Contrast primary and secondary peristalsis based on initiating event, voluntary control, reflex propagation, and regions of the pharynx and esophagus involved.
• Describe the origin and consequence of the high basal tone found in the upper esophageal sphincter (UES) and lower esophageal sphincter (LES).

Universidad Autónoma de Guadalajara22
Objectives• Contrast the patterns of external and internal
innervations of the upper, middle, and lower esophagus. • Describe the pressure changes that occur in the
esophagus as a bolus of food moves from the pharynx to the stomach, including the pressures immediately oral and aboral to the bolus, and the pressures in the upper and lower esophageal sphincters.
• Contrast the lower espohageal tone, innervation, and motility defects that lead to heartburn with those leading to achalasia.

Universidad Autónoma de Guadalajara23
Swallowing sequence
1. Oral phase: [voluntary]
2. Pharyngeal phase: less than one second
3. Esophageal phase:
Primary peristalsis
Secondary peristalsis

Universidad Autónoma de Guadalajara24
1. Oral phase
Oral phase: [voluntary]. Bolus of food moved up and back, forced into pharynx, initiates reflex.
From: Silverthorn. Human Physiology Prentice Hall

Universidad Autónoma de Guadalajara25
2. Pharingeal phase.2. Pharingeal phase.Pharyngeal phase: less than one second:
1. Palatopharyngeal folds move in to close off nasopharynx.
2. Vocal cords come together and larynx is raised up and forward against epiglottis.
3. UES relaxes and superior constrinctor muscles of pharynx contract.
4. Peristaltic wave begins with superior constrictor muscles and moves toward the esophagus, forcing food through UES. From: Silverthorn. Human
Physiology Prentice Hall

Universidad Autónoma de Guadalajara26
• UES reflexly constricts after bolus passes.
• Primary peristalsis: Peristaltic wave travels length of esophagus in 5 to 10 sec.
•Secondary peristalsis:If food remains, it elicits secondary peristalsis, which is more locally controlled.
• Reflex relaxation of LES and stomach to receive food, followed by constriction of LES are part of normal swallowing reflex.
3. Esophageal phase:
From: Silverthorn. Human Physiology Prentice Hall

Universidad Autónoma de Guadalajara27
Swallowing initiates pharyngeal and esophageal peristalsis and sphincter relaxation
Manometry

Universidad Autónoma de Guadalajara28

Universidad Autónoma de Guadalajara29
NOVIP
ACh
VEF = vagal excitatory fiber
VIF = vagal inhibitory fiber
NEUROTRANSMITTERS MEDIATE LES RELAXATION
Action potentialsAction potentials

Universidad Autónoma de Guadalajara30

Universidad Autónoma de Guadalajara31

Universidad Autónoma de Guadalajara32

Universidad Autónoma de Guadalajara33
COMMON FACTORS CHANGING LES PRESSURE
INCREASE
• PROTEIN
• INTRA-ABDOMINAL
PRESSURE
• GASTRIC pH
DECREASE
• FAT
• CHOCOLATE
• PEPPERMINT
• ALCOHOL
• SMOKING
• GASTRIC DISTENSION (aerophagia)

Universidad Autónoma de Guadalajara34
EFFECT OF PEPTIDES AND HORMONES ON LES PRESSURE
INCREASE
• GASTRIN
• MOTILIN
• SUBSTANCE P
• PANCREATIC POLYPEPTIDE (PP)
• VASOPRESSIN
• ANGIOTENSIN II
DECREASE
• SECRETIN
• CHOLECYSTOKININ (CCK)
• GASTRIC INHIBITORY PEPTIDE (GIP)
• VASOACTIVE INTESTINAL PEPTIDE (VIP)
• PROGESTERONE

Universidad Autónoma de Guadalajara35
ACHALASIAACHALASIA

Universidad Autónoma de Guadalajara36
ACHALASIAACHALASIA

Universidad Autónoma de Guadalajara37

Universidad Autónoma de Guadalajara38

Universidad Autónoma de Guadalajara39
Copyright © 2004 by Karl Loren

Universidad Autónoma de Guadalajara40
ACHALASIAACHALASIA

Universidad Autónoma de Guadalajara42
Case-Based Learning in Gastroenterology and Hepatology: Esophageal DisordersA Classic Achalasia in a Young Woman
Klaus Bielefeldt, M.D., Ph.D. http://www.vh.org/adult/provider/internalmedicine/GICases/Esophageal/Achalasia/Achalasia.htmlhttp://www.vh.org/adult/provider/internalmedicine/GICases/Esophageal/Achalasia/Achalasia.html
A 19-year-old Caucasian woman presented with "problems swallowing." Ten months ago, she noted pressure and fullness in the retrosternal area immediately after swallowing. This initially subsided within a few minutes but progressively worsened.For several months, she had been unable to complete a meal, as she became very uncomfortable with significant pain triggered by food intake. The consistency of food did not significantly affect her symptoms. She frequently regurgitated undigested food, which alleviated the pressure and chest discomfort. She had lost about 25 kg during this time period.

Universidad Autónoma de Guadalajara43
She frequently awoke at night due to coughing spells. She did not have prior medical problems. On physical examination she was thin, but not anorectic. No other significant physical findings were noted.
Her symptoms are typical for esophageal dysphagia. The combination of dysphagia for liquids and solids suggests a motility disorder.
A barium swallow was performed as the initial evaluation.

Universidad Autónoma de Guadalajara44
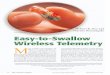
It demonstrated a distended esophagus with pooling of contrast and a "bird beak" appearance of the lower esophageal sphincter Over time, some barium passed into the stomach. However, the lower esophageal sphincter never fully opened
Copyright © 2004 by Karl Loren

Universidad Autónoma de Guadalajara45
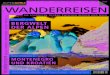
Retention of saliva in the distal esophagus was noted. The distal esophagus was macroscopically normal.
The lower esophageal sphincter area had a "pin hole" appearance . However, the endoscope could easily be passed into the stomach, which was unremarkable.
Endoscopy examinationEndoscopy examination
Copyright © 2004 by Karl Loren

Universidad Autónoma de Guadalajara46
A manometric study demonstrated no appreciable motility in the tubular esophagus.
The lower esophageal sphincter had a normal resting pressure but did not relax upon swallowing

Universidad Autónoma de Guadalajara47
Discussion to the clinical case Achalasia:
The diagnostic studies confirmed the initial impression that the patient has an esophageal motility disorder, demonstrating classical findings of achalasia. Achalasia is an idiopathic disorder of the esophagus.
Anatomically, the NO-containing neurons are absent from the myenteric plexus of the distal esophagus. The loss of these neurons results in an inability of the lower esophageal sphincter to relax. Concomitantly, the tubular esophagus typically demonstrates simultaneous, non-propagating contractions.

Universidad Autónoma de Guadalajara48
The diagnostic method of choice is the barium swallow, which shows a smooth narrowing of the distal esophagus ("bird beak"), often associated with distension of the tubular esophagus and food retention.
Mucosal irregularities or a long narrowing of the GE junction should raise the suspicion of "pseudo-achalasia" due to an infiltrating lesion. Not present in this patient.

Universidad Autónoma de Guadalajara49
Manometrically, the lower esophageal sphincter has a normal or high resting pressure that does not appropriately relax upon swallowing.
In the early stages, simultaneous contractions with normal or even high amplitudes can be recorded in the tubular esophagus ("vigorous achalasia").
With progression of the disease, the esophagus becomes distended and swallows trigger weak contractions that are similarly registered at several points due to a common cavity phenomenon
The main role of endoscopy is to rule out infiltrative processes in the GE junction.

Universidad Autónoma de Guadalajara50
The treatment: The goal is a reduction in the resting pressure to allow passage of the food bolus into the stomach.
Medical therapy with smooth muscle relaxants, primarily organic nitrates and calcium channel blockers, has only limited effectiveness.
More definitive treatment options include pneumatic dilation, injection of botulinum toxin and surgical myotomy.
Balloon dilation leads to improvement in about 60 to 80 % of the patients (risk of perforation between 2 - 6 %), more than half of the individuals will require a repeat dilation within less than 5 years.

Universidad Autónoma de Guadalajara51
• Continue with motility part 2: Continue with motility part 2: gastric and duodenal motilitygastric and duodenal motility