Embed Size (px)
Citation preview

1
Basic laboratory tests in renal diseases
Jana Granátová
Dept. of clinical chemistry, Thomayer Hospital
and 3rd Medical Faculty of Charles University
ONLY FOR EDUCATIONAL PURPOSE FOR STUDENTS OF THE THIRD FACULTY OF MEDICINE !!!

2
Useful references:
• The presentation
• Important numerical values
• Basic laboratory tests – practical advices („a cookery – book“)
• https://sites.google.com/site/nphrologic/Home/course-8-edema-and-renal-disorders

3
When and whom to examine?
• asymptomatic population: 17% with GFR < 1,0 ml/s, renal disorder = preexisting risk
• pre-operative (peri-, postoperative complications)
• potentially nephrotoxic therapy (aminoglycosides, contrast media, nonsteroid antiinflammatory drugs)
+ age, diabetes, hyper/hypotension, combined therapy
• drug administration (doses cumulation)
• Diseases that can damage kidney - diabetes, hypertension, cardiovascular diseases
• long-term observation in renal diseases

4
Glomerular filtration rate
(GFR)

5
• a basic test of renal function• severity of damage: - chronic - K/DOQI classification (Kidney Disease Outcome Quality
Initiative)
appropriate therapy, drug administration, indication to renal
replacement therapy, predialysis care
(mild, moderate, severe renal insufficiency – descriptive - no
definition, no clinical classification)
- acute – RIFLE criteria (s-creat., GF, urine output)
CKD stage
GFR (ml/s/1,73m2)
1 normal GFR + kidney damage (PU, HU)
≥ 1,5
2 „mild renal insufficiency“ 1,0 – 1,49
3 „moderate renal insufficiency“ 0,50 – 0,99
4 „severe renal insufficiency“ 0,25 – 0,49
5 kidney failure, ESRD/RRT < 0,25

6
Glomerular filtration rate
ultrafiltrative pressure (blood flow in the kidney), filtrative area,
number of nephrons • approx. 2 ml/s/1,73m2 lower in female • physiological decrease with age 0,17 ml/s/1,73m2/10 years (80 – 90 y. = 50 % of function in 20 y.)• decreases in kidney disease – acute (AKI) and chronic chronic kidney disease (FSGS): decreased number of
nephrons, compensatory residual hyperfiltration … overload, nephron death, fibrosis….progressive worsening,
fall in GF
• indirect indicator = renal clearance (plasma volume cleaned off from substance XY in a time unit)

7
Renal clearance
GF = clearance + tubular secretion (or - tubular resorption)
• Clearance of inulin: a golden standard, GF = Cin, not for daily practice
• Radionuclid methods: 99mTc-DTPA, 51Cr-EDTA, 125I-thalamate - more accurate (drop in plasma after i.v.
administration) - both the kidneys separately (before kidney
transplant., stenosis of a. renalis)

8
Clearance of endogenous creatinine, Ccr
- daily 1-2 % creatine (muscles, brain) → creatinine (liver) - free filtred + secreted in tubuli (physiologically 10 % x in a chronic kidney failure >
100%, + excreted through a gut)
- as decreased GF, as overestimated Ccr
- calculation based on u-creat., urine volume, time period (24 h),
s-creat. - adjusted to body surface (weight, height) – ml/s/1,73m2
- reference values: 1,5 – 2,0 ml/s/1,73m2 (gender, age) females: 8 - 10% lower

9
- limitations: - to collect urine correctly better in a hospital stay (x confused collecting
vessels)
(outpatient dpt.: 40% pts. differ > 30% in collected
volume = more than 50% in calculated GFR value)
- low muscle mass (low s-creatinine)
- obese, fluid retention, swellings (creatinine distribution)
- short time of collection (circadial rythms)
- urine output < 500 ml / 24 h
- less realiable in late stages of CKD (overestimated GF)

10
S-creatinine
• elevated: - low excretion: altered structure of kidney
(glomerulonephritis, interstitial nephritis, obstruction,
malformation,…) - functional: altered renal perfusion (hypoxia, severe cardiac insuficiency,…) - high production (polytrauma, acromegalia,…) • muscle mass, physique, diet, physical excercise, hydratation
REMEMBER: TO SEE YOUR PATIENT !!!
• limitations: - muscle atrophy (age, immobilization, malnutrition) - swellings, hyperhydrated patient, (pregnancy) - rapid changes (biological half-time 24 h!) – critically ill
patients (s-cystatin C, u-NGAL are better ) Reference values: male: 62 – 115 µmol/l female: 53 – 97
µmol/l

11
• non-linear dependence s-creat. and GFR (hyperbolic)
• a late indicator of kidney damage (GFR ≤ 50% = CKD-3)
• not to use for early diagnostics of decreased function (nephrotoxic therapy, early therapy)
• only 6/10 with slightly decreased GFR has increase in s-creat.
CREATININE
CYSTATIN C
„creatinine-blind“

12
s-cystatin C• produced by all nuclear cells at a constant rate• serin proteases inhibitor• free filtered in glomeruli + completely resorbed + metabolized in proximal tubuli• its concentration in serum = glomerular filtration • estimated GFR (Grubb: eGFR = 1,412 x Scyst.
-1,68 x F)
• EARLIER INCREASE THAN S-CREATININE • an early indicator of decreased GF („creatinine-blind “, GF
50 – 99%)• independent on age, muscles, height and weight
indication: children, elderly, long-term immobilized, nephrotoxic therapy
muscle atrophy, cachexia, pregnancylimitations: - steroid therapy („worse“ GF) Δ 25 – 50 %, evaluate with s-creat., dependent on a
dose - decompensed thyroid function („better“ in hypofunction)

13
Estimated GFR (eGFR)
THE ONLY S-CREAT. IS INACCURATE AND LATE
S-creat., age, gender, (black/other), without an urine collection
recommended together with s-creatinine if it is standardized (enzymatic)
calculators (www.kidney.org/professionals/tools/index.cfm)
„value“ + clinical conditions, patient´s individuality ≥ 1,5 - „normal“, higher values not given (underestimate
-15-17%) 1,0 – 1,49 - to evaluate individually (age, clinical conditions) < 1,0 - pathological (LM: in screen - if 0,67
ml/s/1,73m2: CKD 3 – 5 in > 90% pts., AUC 0,97 for CKD
3- 5)
not to use: - rapid sudden changes - pregnancy - muscle atrophy (s-creat. < 40 µmol/l) - young, healthy

14
adults:
• MDRD formula:
eGFR = 515,3832 x (s-creat)-1,154 x age-0,203 x F1 (x F2)
• CKD-EPI formula:
female: eGFR = 144 x (S-creat. / 62-F) x 0,993age , F: S-creat < / > 62 μmol/l
male: eGFR = 141 x (S-creat. / 80-F) x 0,993age F: S-creat < /
> 80 μmol/l • Lund-Malmö formula:
eGFR = eX - 0,1124 x age + 0,339 x ln(age) – 0,226 (if female)
X= 4,62 – 0,0112 x (s-creat), if < 150 μmol/l X = 8,17 + 0,0005 x (s-creat) x ln(s-creat.), if >150 μmol/l, (correct. To LBM (lean body mass)
• (Cockroft – Gault: age, weight, s-creat., gender – not recommended)

15
Formulas are relatively comparatible:
MDRD: better: for GF 0,5 – 1,0 ml/s/1,73m2
worse: elderly > 80 let (+18%)
CKD-EPI: better: for GFR 1,0 – 1,5 ml/s/1,73m2 (differs at 10 - 12 x 17%)
for general screen, elderly the both are inaccurate: - in young, healthy individuals (CKD-EPI +22%, MDRD
+14%) - in males with low BMI < 20 (CKD-EPI +36%, MDRD
+46%) - if GF < 0,5 ml/s/1,73m2
- in children
LM: better: for GFR near to 1,5 ml/s/1,73m2
for GFR < 0,5 ml/s/1,73m2
can be used for children older 1 y.

16
children:
• Schwartz: s-creat., age, gender, height eGFR = (F. height) : s-creat.
• based on cystatin C (the same as in adults)
• Lund-Malmö (the same as in adults)
• maximal s-creatinine: height (cm) x 0,54 = the highest „normal“ s-creat . value fitted to „normal“ GF (1,5 ml/s/1,73m2) (3 years = approx. 100 cm: 54 μmol/l x 2 years = 86cm – 46,5 μmol/l f.e.)

Závěr do praxe 1:
Chci v praxi vědět, jakou funkci ledvin má můj pacient?
Dospělý „běžný“ pacient : S-kreatinin (+odhad GF) (eGF: MDRD, event. CKD-EPI, Lund-Malmö)
kreatinin ne → S-cystatin C (+ odhad GF z cystatinu): funkce štítné žlázy???, steroidy???• svalová atrofie (kachexie, po imobilizaci, dystrofie, senioři) / muskulatura• těhotná• extrémně obézní• pro dávkování léků
Dítě: S-cystatin C (fyziognomie, svalová atrofie /dystrofie, věk) s-kreatinin (+ eGF-Schwartz nebo Lund-Malmö, ne MDRD/CKD-EPI), orientačně maximální S-kreatinin

18
diagnosis and management of AKI
From: Vaidya, et al. Ann Rev Pharmacol Toxicol 2008
NGAL
Traditional diagnosis:
- rise in s-creatinine
(24 – 72h, fluctuating,
50% of function lost)
- fall in GF
- fall in urine output
(!! non-oliguric AKI)
- changes in a function
NGAL:
- real-time (30 – 120 min)
- changes in a structure

19
NGAL (neutrophil gelatinase-asscociated lipocalin)
• physiologically in neutrophile granules – binds iron – bacteriostatic effect• produced early after the renal insult by epithelial cells in distal tubuli• significan rise in 2 – 4 hours after nephrotoxic, ischemic insult• functions:
- protective: early, protects/reduces tubular epithelium damage
- proliferative: late, growth and differentiation of new tubular cells
• predicts the development of AKI on 2 days earlier than s-creat.
(sepsis, major operations, cardiogenic shock, nephrotoxins,…)
• proportional reponse to injury, no differentiation in causes• measured in urine, results early (till 1 hour)• indications: ICU patients, major operations, cardiac surgery, contrast
induced / cis-Pt nephropathy, graft recovery prediction

20
s-urea (blood nitrogen)• protein metabolism (NH2) end-catabolite, in liver• excreted 90 % in kidney: GF + tubular resorption (30 – 40%),
(+ gut, skin in chronic kidney failure)
• increase not only if damaged kidney
- high protein intake - catabolism (fever, sepsis, starvation, bleeding) - hydration (volume depletion) - congestive heart failure • increases later than s-creatinine (if GF < 30%) • faster and more in dehydrated and volume depleted
patients• diff. dg prerenal x renal causes of renal failure:
prerenal: ↑ s-urea > > ↑ S-creat., ↑ u-urea, ↑ u-osmol.
• reference values: 1,7 – 8,3 mmol/l

Závěr do praxe 2:
Podezření na postižení ledvin – běžný pacient, susp. chronické onemocnění:
S-kreatinin (+ eGF: MDRD, event. CKD-EPI, Lund-Malmö)
S-urea, albumin v moči - ACR (je-li diabetik, hypertonik)
Podezření na akutní poškození ledvin (AKI):
Ambulant: trend s-kreatininu 3- 4 dny (event. cystatin C, viz výše)
pokračující trend → hospitalizovat
cave:
biologická + analytická variabilita s-kreat. mezi dny cca 15%
změny s-kreatininu se zpožděním 24 – 48h po inzultu Hospitalizovaný: S-cystatin C, (event. NGAL)

22
Proteinuria(PU)

23
The kidney:→ very efficiently ultrafiltrates water, mineral and
small molecules → efficiently restricts protein loss from plasma to
ultrafiltrate (recirculation,
resynthesis)
blood flow rate at 1,2 l / min → daily 40 - 50 kg albumine → 2 - 3 g/d into the ultrafiltrate → only 30 mg/d into a
definitive urine
glomerular wall integrity, tubular resorption, physical-chemical characteristics of proteins, microcirculation in glomeruli

24
The glomerulus wall
Endothelium negatively charged
Base membrane – 3D sieve, loops – diameter, negatively charged
Podocytes – amount of water (and protein) passing through a glomerulus wall

25
Proteinuria:
• transient: functional – in healthy kidneys - excessive physical excercise, severe stress - orthostatic: in a standing, not in a lying
position, till adolescence, asthenic physique, other laboratory tests normal,
observe
• persistent: repeately, always observe - kidney disease, even if normal GFR
• a sign of kidney / urinary tract disease• an independent risk factor

26
Protein in urine – urinary strips
• different limit of detection: 0,15 - 0,30 g/l, low reliable
• concentration of proteins in urine, dehydration/polyuria
false negative: other proteins than albumine (tubular proteins
– interstitial nephritis, myeloma) false positive: dehydrated, hematuria, pH > 7-8, disinfectants, artificial (malingerers)
• A NEGATIVE RESULT DOESN´T EXCLUDE PATOLOGICAL PROTEINURIA
(normal total protein amount + patological composition,
other proteins than albumin,
proteinuria ≤ 15 g/mol creat. - in 1/3 pathological composition)

27
• NOT FOR EARLY DIAGNOSTICS (early stages not detected, no intervention, no prophylaxis)
• not recommended for screen or follow-up (low reliability of changes in a semiquantitative scale)
• if positive ≥ 1+ → a quantitative test
• plus a test with 20% sulfosalicylic acid (the same reaction with all proteins in urine, „confirmation“ of a negative result)
Proteinuria = risk factor – renal (ESRD) and cardiovascular (mort., morbid.)

28
Proteinuria - quantity:
• physiological: previously: ≤ 0,150 g/d (0,07 - 0,10 g/l) -
consensual now: adjusted to u-creat. - PCR (protein-to-
creatinine-ratio) ≤ 15 g/mol creat
• pathological: mild < 1 g / 24 h moderate 1 - 3 g /24 h high > 3 g /24 h, PCR > 100
g/mol nephrotic > 3,5 g/24 h nephrotic PU = a risk of nephrotic syndrome (NS)NS = nephrotic PU + clinical and laboratory signs (swellings, low s-albumin, low s-total protein,
dyslipidemia (↑cholesterol, later triglycerides), accelerated
atherosclerosis, thromboembolic complications (adults), infection
(children)

29
Microalbuminuria:
• mild elevated urinary albumin undetectable by ususal urinary strips (< < 150 mg/l)
microalbuminuria strips: limit of detection 30 - 40 mg/l - for GP (positive)
• measure quantitative - ACR (mg/mmol creat.) ACR: albumin-to-creatinine-
ratio (not recommended in ug/min,
mg/l, mg/d)
• a random urine sample, not collected urine
• physiological values: < 2,6 mg/mmol (male), < 3,6 mg/mmol (female)
– lower?
• microalbuminuria: ACR 2,6 (3,6) – 29,9 mg/mmol (30 mg/l)

30
MAU = elevated cardiovascular and renal risk
• elevated risk also in high normal albuminuria (higher than 2 mg/mmol in male / 3 mg/mmol
in female)!
cardiovascular morbidity
and mortality / 5 years, LIFE
Incidence of ESRD and albuminuria – 10,3 r. follow-up, HUNT-2 (Hallan et al, JASN 2009)

31
• not to test: - urinary tract infection, - after physical exercise - menses, - if positive protein in urinanalysis, - in acute diseases
• high variability in excretion (CVi 30%) - to test repeately
• criteria: positive in ≥ 2/3 tests in 3 - 6 months
• recommended to test regularly in: - hypertension, - diabetes - cardiac ischemia

32
Microalbuminuria in diabetes (DM):
DM+MAU = a sign of incipient nephropathy (stage 2-3 from 5)
10x higher risk of ESRD 4x cardiovascular complications 2x total mortality / 5 years
DM-1: 50% MAU → 80% dia nephropathy (DN) with PU
50% without MAU → vascular changes DM-2: 40 - 50% MAU, manifest DN in fewer
patients, more often nephrotic
syndrome
good metabolic control, corrected hypertension, ACEI = to reduce / stop the progression to renal
failure
screen: 1x in a year, - DM type 1: in 5 years after the
diagnosis is given, - DM type 2: immediately

33
PU composition – PU types:indication: - diff. dg. (f.e. PU 1 g/l – cause: GN / DM, HT / TIN?)
- new PU (esp. in young, with a nephrotic sy, typical diagnosis and atypical findings)
PU in DM: 30 – 50% = other than dia nephropathy
- indication to renal biopsy (profit x risks)
- „replacement“ of renal biopsy if RB is not possible / at risk
- how much altered – progression - appropriate therapy (conventional x immune-supressive)
- therapeutic response, compliance

34
Proteinuria types:
according to its composition: - glomerular - tubular - mixed (glomerulo-tubular) - prerenal - (postrenal)
• qualitative pattern (electrophoresis in urine)
• quantitative (some excreted proteins)
albumin, IgG, α1microglobulin
+ ratios, graphs, cut-off values

35
Physiological PU: • selective glomerular filter -
(charge, large, Mr, shape) Mr < 67 kD (albumin)• tubular resorption (99%)• secretion
• 50 - 80 mg / 24 h• consensually 150 mg / 24 h• PCR ≤ 15 g/mol creat.
uromodulin, THP 30 - 50 mg
albumin 10 - 30 mgsIgA 10 - 15 mgpolyclonal light chains 10 - 15 mg
Schneiderka P.: Vybrané kapitoly z klinické biochemie

36
Glomerular PU:altered glomerular filter
selective PU: • loss of a negative charge• albumin, (transferin)• minimal change
nephritis, early stages of glom.
diseases• better prognosis
nonselective PU:• more severe wall alteration – large molecules are
passed • albumin, IgG
index of selectivity : IgG / Alb
≤ 0,03 - selective PU (MCN,
response to steroids)
> 0,04 – nonselective

37
Tubular PU:altered tubular resorption• mild PU (less than 1 g/d)
• microproteins (Mr < albumin)
α1microglobulin, β2micro, RBP,
• strips often negative (sulfosalicylic acid
positive)
• toxins (cisPt, aminoglycosides, heavy metals, X-ray contrast, toxins), ischemia, hypoK, hyperCa, hyperuricemia, acute obstruction, inflammation
• also a late consequence of glomerular PU (tubular atrophy + fibrosis) - advanced changes

38
Mixed PU:
advanced disease (glomerular, systemic disease, severe chronic interstitial nephritis)
tubular cells and glomeruli are altered by PU - toxicity of PU (glomerular sclerosis, atrophy of tubuli, sterile inflammation, nephrons are replaced by interstitial fibrosis)
• moderate / heavy, nonselective• albumin, IgG + α1microglobulin, and other
proteins, …
• as higher PU, as faster progression• in DM, HT earlier than in GN

39
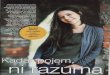
1 – normal tissue
2 – mild fibrosis and atrophy
3 – moderate fibrosis and atrophy
4 – severe fibrosis and atrophy

40
Prerenal PU:healthy kidney initially + ↑↑↑ microproteins from
blood (monoclonal light chains,
hemoglobin, myoglobin)
overestimated capacity of tubular resorption
• strips often negative (sulfosalicylic acid
positive)
• myeloma, intravascular hemolysis, muscle
contusion, catabolism, fever,
inflammation, tissue necrosis
• leads later to altered tubuli

41
Postrenal PU:
proteins secreted in a lower urinary tract
• mild (less than 0,5 g/d)• dominates leucocytes +
hematuria• typical: α2-
macroglobulin, IgG
• inflammation, trauma, tumors

42
Patient 1: 25 y., male:
1/2011: 2 weeks ago tonsillitis (antibiotics) + cold
clinical: fatigue, mild hypertension
lab.: S-creat. 140 … 168 µmol/l, border Ckr 1,82 ml/s/1,73m2, urinanalysis: active sediment (ery ++++, leucocytes ++,
casts) microHU, PU 2,8 g/l elevated C3+C4, ASLO normal, negative autoantibodies
(ENA, ANA,…)
suspected: acute GN (post-infectious)?
• children 3 – 10 y, young, 10% > 60 years• infection in a history (bacterial, viral, toxopl., parazit.), may be asymptomatic - only with HU,
• ↑ ASLO (anti-DNase, anti-hyaluronidase), • PU 0,5 – 2 g/d, mixed nonselective ↑ S-creat, active sediment (erythrocytes + casts,
leucocytes), ↓C3+C4, ↑ CIK, cryoglobulin

43
PU typing: PU 2,8 g/l, ↑↑↑ albumin, ↑ IgG + ↑ transferin, normal a1micro,
IgG/Alb. 0,07
Concl.: glomerulonephritis with glomerular nonselective PU, without tubulo-interstitial damage, glomerular HU
renal biopsy: IgA nephropathy with crescents 30%, active form
IgA nephropathy: always hematuria - repeately macroHU (respiratory, intestinal infecton) + mild
PU, with/without renal insuficiency, - proportional PU a HU, as higher PU, as worse prognosis - asymptomatic microHU (without PU / mild PU), - in all age, children and young, more often males (6x) - PU < 1 g/l, if PU > 1,5 g/l (10 - 15%) – steroid therapy
- correct diagnosis → renal biopsy - appropriate therapy: acute GN – non specific, if steroids – worse
reparation x IgAN mild form – regime, active form / heavy PU –
imune-supressive

44
Patient 2: 26 y., male:
2004 minimal change nephritis, MCN (RB), nephrotic sy, imune-therapy,
repeated relapses (the last one month ago)
MCN: fusion of podocate pedicels + regressive changes, normal glomeruli; normal GFR develops fast nephrotic PU without microHU, children 2 – 7 y., in adults rare, worse prognosis
(relapses) typical: glomerular selective PU: selectivity – effective
steroid therapy
1/2011 admission to hospital – worsening conditions – relapse?
other? swellings of both lower extremities, rise in PU
s-creat. 86 µmol/l, urea 10,6 mmol/l, low total protein (38 g/l), very low
albumin (16 g/l), high cholesterol (9,4 mmol/l), high triglycerides (4,5 g/l),
very low IgG (< 1,4 g/l), IgA + IgM norm., PU 3,6 g/l (10,1 g/d)
PU typing :↑↑↑↑ albumin, ↑ IgG, norm. a1micro, IgG/Alb. 0,008 Concl.: GN with glomerular high selective PU, without
altered interstitium, without microHU another relaps – effective
steroids: in 5 days: total protein to 53 g/l, albumin to 35 g/l, PU drop to
0,13 g/l

45
Patient 3: 52 y., female
2 weeks ago abdominal pains, fatigue, anorexia, diarrhea, dyspnea, S-krea 253 ... 410 µmol/l (in 4 days !), elevated CRP (144…129
g/l), inflammation and acute obstruction excluded
suspected rapid progressive GN (RPGN) → renal biopsy
rapid progressive GN (RPGN): HU + PU + rapid fall in glomerul. function (> 50% / 3 mths,
crescents > 50% - vasculitis (c-ANCA+) – Wegener granulomatosis - immune-complexes (post-infectious, collagenosis, other GN) - anti-GBM-nephritis (without/with pulmonal damage – Good-
Pasture sy) - can complicate any GN
weakness, fatigue, fever, anorexia, abdominal pain, swelling of joints,
(viral infection in the history) if not treated, in 3 months progression to ESRD

46
S-krea 871 … 532 … 242 µmol/l (10 days), normal value in 4 months
urea 24,9…28,9…17,3 mmol/l, elevated s-K+ (6,1 mmol/l), elevated s-P+
elevated s-CK, very high myoglobin (non-cardial), urinanalysis: protein +, blood ++, erythrocytes 5/ul, leucocytes
44/ul CRP 84…120,8…9,3 mg/l, elevated s-LD, high s-IgE (486…227) metabolic acidosis (pH 7,276, BE -11mmol/l) blood count: low Hb 86…120…83 g/l, eosinophiles PU typing: mild PU 0,16 g/l: ↑↑↑ α1-microglobulin, ↑
albumin Concl.: interstitial nephritis, interstitial mHU renal biopsy: acute interstitial nephritis Concl.: acute kidney failure - aTIN hypersensitive + rhabdomyolysis, hemolytic anemia, iridocyclitis, good response to steroids rhabdomyolysis: ↑s-CK + myoglobin, urinanalysis: blood ++, low ery hemolysis: ↓ Hb, ↑ s-LD, hypersensitivity: eosinofiles, high IgE AKF (s-creat. + urea)+ altered tubular functions: ↑ P; ↑ K, metabolic
acidosis diff. dg AKF (GN x TIN), therapy, early diagnosis → repaired
functions

47
Urinanalysis (chemical and morphological)

48
• results dependent on the quality of samples (middle stream of morning urine, hygiene, not
if menses)
• analyze to 1hour (changes in pH, destroyed elements)
• diagnostic strips • semiquantitative scale
• pH, specific gravity, protein, leucocytes, glucose, nitrites, blood/erythrocytes, ketones, bilirubin, urobilinogen

49
pH in urine:
usually: 5 – 6,5 • possible 4,5 – 8,0 (strips, pH-meter)• changes in pH - acidobase regulation
• alkalic pH (> 7): - vegetarians, - alkalizing therapy (diuretics, secondary prophylaxis of urolithiasis, hyperuricemia),
- vomiting - prolonged storage x - bacterial infection - compensatory in metabolic alkalosis - renal tubular acidosis (altered HCO3- resorption and acid urine production)

50
Blood in urine - strips:
• positive: erythrocytes / free hemoglobin / myoglobin (hem)
erythrocytes - urinary tracts, kidney disease, bleeding
hemoglobin - destroyed erythrocytes, intravascular
hemolysis (↑LD, total bilirubin, Coombs +)
myoglobin – muscle contusion (↑ s-Mgb)
• false positive: - menses, gynecologic (uterine cervix, vaginitis) - artificial (malingerers), - porphyria, dietary (red beet), drugs (rifampicine)

51
Why hematuria?
Renal: • glomerular: glomerulonephritis, systemic diseases,
hereditary (sy of thin membranes, Alport. sy)• tubulointerstitial: acute nephritis, toxicity, acute
obstruction• vascular: malignant hypertension, thrombosis / embolism • other: tumors (Grawitz / Wilms), cysts, necrosis of papila,
trauma, nefrolithiasis
Postrenal:• lithiasis, prostate, permanent urinary catheter, urothelial
carcinoma, urinary tract infection (cystitis), trauma, tuberculosis, malformation,
post-radiative, fistuli
persistent macroHU in elderly = in 20 % suspected urothelial ca
Extrarenal:• anticoagulants, polycytemia, hematological malignancies,
bleeding diathesis

52
Hematuria / ErythrocyturiaHematuria (HU) = blood in urine visible - macroHU – brown color („Coca-cola“)
(in)visible microHU - strips / urinary sediment („microscopy“)
Erythrocyturia = erythrocytes
> 30/µl
non-glomerular - interstitial (nephritis, Grawitz tu,
cysts), - lower urinary tracts (urolithiasis, infection, trauma, urothelial/renal carcinoma, prostate) usually only a mild PU
glomerular - glomerulonephritis, - other glomerular diseases, usually with PU if HU + PU = usually GN

53
Erythrocyturia typing:
1. Erythrocytes in phase contrast: glomerular: ≥ 80 % dysmorphic or ≥ 5 %
acanthocytes, „doughnuts-cells“, erythrocyte
casts non-glomerular: ≥ 80% eumorphic limitation: only in fresh urine, amount of cells in sediment, subjective evaluation, experience, grey zone

54
2. protein indexes (if proteinuria is present): u-albumin/u-total protein proteinurie:
glomerular ≥ 0,59 non-
glomerular < 0,40
protein indexes (α2macroglobulin, IgG, α1microglobulin und their ratios) – only in some laboratories
- more specific differentiation, objective

55
Patient 4: microHU renal glomerular
male, 61 y.:his history: 12/06 microHU, examined by an urologist (excluded urolithiasis, lower urinary tract infection and
prostate disease) first examined by a nephrologist (1/07): exanthema, PU
2,6 g/l, microHU, elevated IgA, urinanalysis: protein +++,
blood ++++
phase contrast: 90 % dysmorphic ery, 10 % acanthocytes
PU typing: PU 2,8 g/l ↑↑↑ albumin, IgG ↑, mildly α1micro, u-Alb/total
protein = 0,80 Concl.: glomerular nonselective PU, with mildly altered
interstitium) - glomerulonephritis, glomerular HU ↓ renal biopsy: focal segmental mesangioproliferative IgAN
with crescents (RPGN), Henoch-Schönlein purpur
→ early biopsy = early therapy, recovered renal function

56
Urinary sedimentBasic: morning urine, not older than 2h (destroyed elements), carefully centrifuge, differentiate elements - flow cytometry /
camera imaging + SW analysis (+ microscopy 400x) erythrocytes: 0 - 12 /µl leucocytes: 0 - 20 /µl sporadic hyaline casts (more frequent: diuretics,
excercise, fever, low water intake)
Collected urine 3 h – „Hamburger sediment“ - quantified elements
- disease „activity! erythrocytes: ≤ 2000/min leukocytes: ≤ 4000/min casts: ≤ 60 - 70/min

57
Leucocytes:
leucocyturia > 15 / µl• interstitial nephritis, cystitis, urethritis, prostatitis,
carcinoma,• surrounding organ diseases (gut, gynecological)
leucocyturia without bacteriuria:• glomerulonephritis, systemic lupus, papila necrosis, cysts,
nefrolithiasis,• possible contaminated by vaginal fluid

58
Casts:physiological: hyaline - Tamm-Horsfall. protein (THP), sporadic
pathological: precipitates of THP + content of distal tubuli and collecting ducts:
• leukocytar: interstitial nephritis, urinary tract infection, glomerulonephritis
• erytrocytar: glomerular diseases (GN)• granular: glomerulonephritis, interstitial nephritis, acute tubular
necrosis• wax: typical in diuresis-recovery stage just after oligo/anuria
(obstruction),
chronic renal failure • fatty – nephrotic sy• Bacterial• Epithelial – tubular
damaged tubuli

59
Urinary syndromes
nephritic: dysmorphic erythrocytes, leucocytes, casts
GN, systemic lupus, Henoch-Schönlein purpur, systemic vasculitis
(Wegener granulomatosis, Goodpasture sy,…), hemolytic-uremic sy
nephrotic: if nephrotic proteinuria (> 3,5 g / 24 h)
hyaline and fatty casts, possible cholesterol crystals,
dysmorphic erythrocytes less frequently
glomerular diseases (MCN, FSGS, MGN, diabetic nephropathy)
minimal abnormalities: isolated microHU
IgA nephropathy, residual after acute GN, systemic lupus,
Alport sy, hypertension,…

60
Concentration of urine

61
urine is hypertonic (if compared to ultrafiltrate): - regulation: antidiuretic hormone (ADH ) stimulus: s-osmolality changes ↑ S-osmol.: (pure water loss – unconsciousness,
polyuria, ↓ intake) → ↑ ADH → ↑ water resorption…. ↓ urine output, concentrated urine (↑u-osmol) ….. drop in s-
osmol., hypertonic urine osmolality in urine >> in serum (≥ 600
mmol/kg) If not: u-osmol. < 600: diabetes insipidus - central (tumors, trauma
hypophysis/hypothalamus) - peripheral (interstitial nephritis, toxins, hypoK) - mixed

62
↓S-osmol.: (polydipsia) → very low ADH …0 → impermeabile for water, only
NaCl resorbed → hypotonic urine, low u-osmol. osmolality in urine < in serum
If not: u-osmol. > s-osmol: SIADH (sy of inadequate ADH secretion)
(ADH secretion stimuled if not ↑ S-osmol, ↑U-osmol, ↓ S-Na)
– „water overdilution“ (pneumonia, tuberculosis, brain trauma or operation,
tumors – lung, pancreas, large operation)

63
• How to test?
- (fluid restriction 24 – 36 h → u-osmol.)
- in a daily practice: u-osmol. in morning urine = 2x s-osmol.
(approx. 600 mmol/kg), in young 900 mmol/kg (3x)
if not: isostenuria: u-osmol. = s-osmol. (advanced chronic renal insuficiency)
- adiuretin test: (DDVAP = ADH analogue): (DDVAP i.nas. administration in the morning, measured u-
osmol. in 4 h)
u-osmol. 1100 – 800 mmol/kg H2O - age)

64
osmolality:
Refer. values : serum: 275 – 295 mmol/kg H2O urine: 400 – 900 (50 – 1200)
mmol/kg H2O (u-osmol. lower in breast-feeding
and elderly)
in a daily practice – calculated osmolality: serum = 2 x s-Na + glucose + urea
osmolal gap: big difference measured vers. calculated value
normal = 5 - 10 mmol/kg H2O elevated: toxins (1‰ alcohol = + 23
mmol/kg H2O), catabolism, hyperglycemia
urine = 2 x (u-Na) +(u-K) + (u-urea) + NH4+
(NH4
+ – approx. 30 – 50 mmol/d)

65
Minerals

66
Sodium (Na)
• main extracellular cation – osmotic pressure to evaluate together with water: Na+ retention = water
retention, Na+ overload = water
overload• regulation: A) depleted EC fluids:
- loss of isotonic fluids (vomiting, bleeding, ascites, ileus) = risk of collapsed circulation - blood pressure
(BP) falls…
→ renin (juxtaglomerular): angiotensinogen (liver) … angiotensin-II
→ vasoconstriction … rise in blood pressure → aldosterone (adrenal cortex) Na+ and water reabsorbed in distal tubulus …
rise in BP u-Na+ < u-K+, u-Na + < 20 mmol/l (< 10 mmol/l)
- loss of pure water - low ADH, ↑ S-osmol. … changes between EC
and IC space, collapsed circulation observed until severe
dehydratation

67
B) excess Na + and water, expanded EC fluids – natriuretic peptides
regulates extracelular volume and blood pressure
ANP, BNP, CNP: left ventriculus and atrium, endotelium, brain, lung,
kidney, aorta, suprarenal glands stimulus: ↑ volume / filling pressure atrial / ventricular to protect pressure and volume overload -
endogenous diuretics: - ↑ urine output, u-Na excretion, - against renin-angiotensin-aldosterone - vasodilatation (sympathetic antagonists)
overloaded circulation (heart failure, left ventricular hypertrophy, renal
failure with oliguria, hyperaldosteronismus)
Reference values: serum: 135 – 146 mmol/l urine: 50 – 220 mmol/l FENa: 0,010 – 0,012

68
Potassium (K):• main intracellular cation (EC: IC = 4,5 : 140), irritability• to evaluate together with acidobase - H+ (acidosis - ↑K+,
alcalosis - ↓K+) pH Δ 0,1 = 0,3 - 0,4 mmol/l K+ • regulation: - resorbed in proximal tubulus, - secreted in distal tubulus (K+, H+/Na+) – aldosteron (stimulates K+ excretion) • elevated in urine: renal failure, loop diuretics, catabolism, hyperaldosteronism !! hyperaldosteronism: unclear hypoK, ↑ u- K+,
u- K+ > u-Na+
• decreased in urine: extrarenal loss - gastrointestinal (K+ 3x more vers
plasma), low intake, anabolism Reference values: serum: 3,8 – 5,4 mmol/l urine: 45 – 100 mmol/d FEK: 0,04 – 0,19

69
Excrete fractions:
• ratio of compound XY filtred by glomeruli and excreted in definite urine
• show tubular functions: FEx = Ux x Pkr / Px x Ukr
• FE H2O: 0,01 – 0,02 (max. 0,035)• FENa: 0,004 – 0,012 (max. 0,30 – 0,40)• FEK: 0,04 – 0,19 (max. 1,5 – 2,0)• FEosmol.: < 0,035 (max. 0,035)
• without long urine collection
• diff. dg.: prerenal x renal failure prerenal: low FENa < 0,01, (+ low u-Na + < 20
mmol/l) (intra)renal: high FENa > 0,03, (+ u-Na + > 30 mmol/l)