Embed Size (px)
Citation preview
19/04/23
The First Congress of Traumatologists and Orthopaedists “TRAUMATOLOGY AND ORTHOPAEDICS OF THE CAPITAL.
PRESENT AND FUTURE”February 16-17, 2012
The Moscow city Govermnent building
Zimmer® Knee - Continuum of Care
NEW TRENDS IN KNEE ARTHROPLASTY:NEW TRENDS IN KNEE ARTHROPLASTY: EARLIER INTERVENTION EARLIER INTERVENTION
AND NEXGENAND NEXGEN®® FLEX GENDER SOLUTIONS FLEX GENDER SOLUTIONS™™
Prof. S. Zanasi (Bologna, Italy)

2
KNEE IS CONSTITUTED BY THREE COMPARTMENT: KNEE IS CONSTITUTED BY THREE COMPARTMENT: IN ELDERLY AS WELL AS IN YOUNGER PATIENT IN ELDERLY AS WELL AS IN YOUNGER PATIENT
OUR CHOICE IS OUR CHOICE IS TO RECONSTRUCT ONLY THE DISEASEDTO RECONSTRUCT ONLY THE DISEASED
COMPARTMENTCOMPARTMENTnot substituting the whole knee not substituting the whole knee
IN ORDER TO MAINTAIN IN ORDER TO MAINTAIN BEST PROPRIOCEPTIVITY, COMFORT, PERFORMANCEBEST PROPRIOCEPTIVITY, COMFORT, PERFORMANCE
TAYLORED RESURFACING IMPLANT TAYLORED RESURFACING IMPLANT ARTHROPLASTYARTHROPLASTY

19/04/233
3
InUNI/BI/ THREE
COMPARTMENTALOA INVOLVEMENT
A new approach is
RESURFACINGCOMBINATION
arthroplasty
i.e.Gender
IMPLANTARTHROPLASTY +

4
to achieve SIGNIFICATIVE INCREASING OF IMPLANT PERFORMANCE AND SURVIVORSHIP
MIS TECHNIQUEMIS TECHNIQUE
HIGH FLEX BEARING UNI/TKAHIGH FLEX BEARING UNI/TKA
EARLIEST STANDING-UP EARLIEST STANDING-UP
AND MOBILIZATIONAND MOBILIZATION
GENDER SOLUTIONGENDER SOLUTION

9
1. UNICOMPARTMENTAL MEDIAL OR LATERAL OSTEOARTHRITIS

Unicompartmental knee arthroplasty has had varying degrees of acceptance since its introduction
approximately 30 years ago.
Frequent and early failures were cited in initial studies.
By the late 1990s, however, unicompartmental knee arthroplasty for the treatment of localized knee arthritis was becoming more common, and early
outcome reports were favorable.
UNI

THEORETICAL ADVANTAGES OF THE PROCEDUREINCLUDE
preservation of uninvolved tissue and bone,reduced operative time, better range of motion,
improved gait, increased patient satisfaction.
With appropriate patient selection, careful surgical technique,
proper implant design,
unicompartmental knee arthroplasty can now be viewed as a procedure with reliable medium to long-term success

1. LATERAL UNI INVOLVMENT


40 days f.up

35
.
2. PATELLO-FEMORAL JOINT ISOLATED 2. PATELLO-FEMORAL JOINT ISOLATED OSTEOARTHRITISOSTEOARTHRITIS

37
Frequency
Approximately 5/10% of patients with osteoarthritis of the knee have symptomatic patellofemoral arthritis in the absence of tibiofemoral arthritis.
Etiology Patellofemoral arthritis can be a result of inflammatory conditions or mechanical abnormalities.
Inflammatory conditions include rheumatoid arthritis; often, the entire knee joint is involved.
Mechanical abnormalities can be a result of prior fractures,
inherent malalignment, muscle imbalances, or chronic instability.
Association with anterior cruciate ligament reconstruction Some orthopedists believe that reconstruction of the anterior cruciate ligament (ACL) with a patella tendon graft
may lead to later problems of patellofemoral pain, loss of motion, and arthritis. However, whether these late complications are a result of the injury itself, the anatomic alignment that
contributed to the injury, or a result of the surgical reconstruction is not clear

39
SGB m 58yrsBilateral patello-femoral OA
left

40
41

42
SGB m 58yrs3ms f.up

45
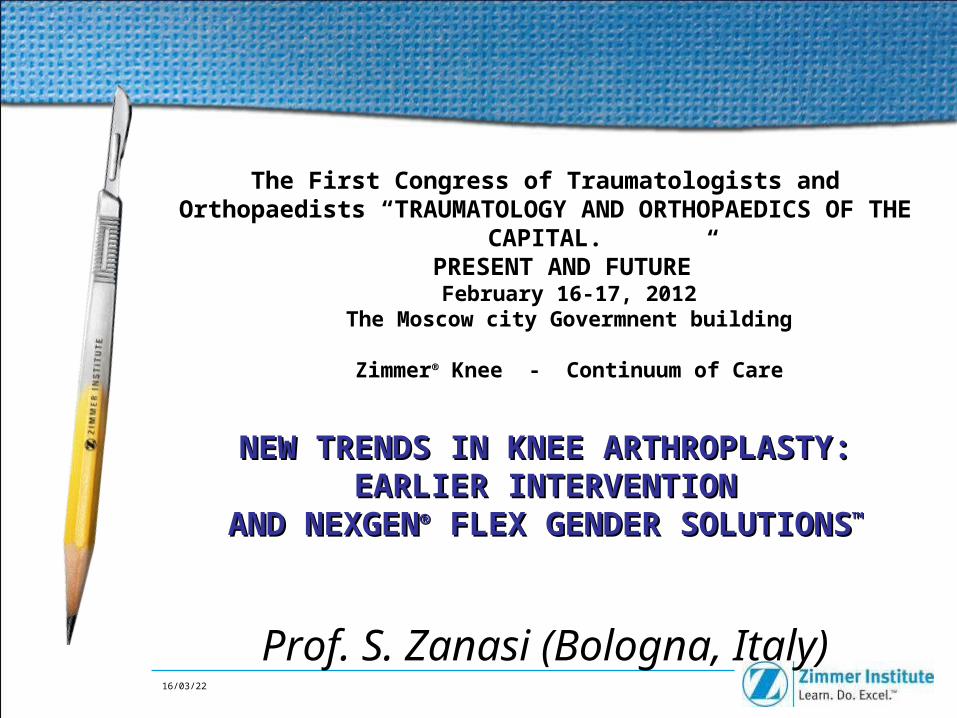
3. BI-UNICOMPARTMENTAL ARTHRITIS

46
BIUNICOMPARTMENTAL ARTHROPLASTYWITH FEMORO-PATELLAR CONSERVATION
B.E. 52ys
474747
THE PRINCIPAL FEATURE OF THE BI-UNIIS THE USE OF 2 FEMORAL AND 2 TIBIAL INDIPENDENT COMPONENTS
In our experience the advantages of this procedure are the same as those regarding UKR:
PRESERVATION THE INTERCONDYLAR EMINENCE WITH THE
CRUCIATEs, rotational axis respect,
bone stock respect, normal patellar level and tracking
normal joint kinematic and gait reproduction leg’s morphology respect
proprioception maintanance
Obviously a surgical mistake due to the difficulty of the technique or due to the loosening of a component is calculated.

484848
To follow /reproduce the own anatomy
Coronal Plane

49

50
3rd day postop3rd day postop
9th day postop9th day postop
postop. X-Raypostop. X-Ray
140°
19/04/2361
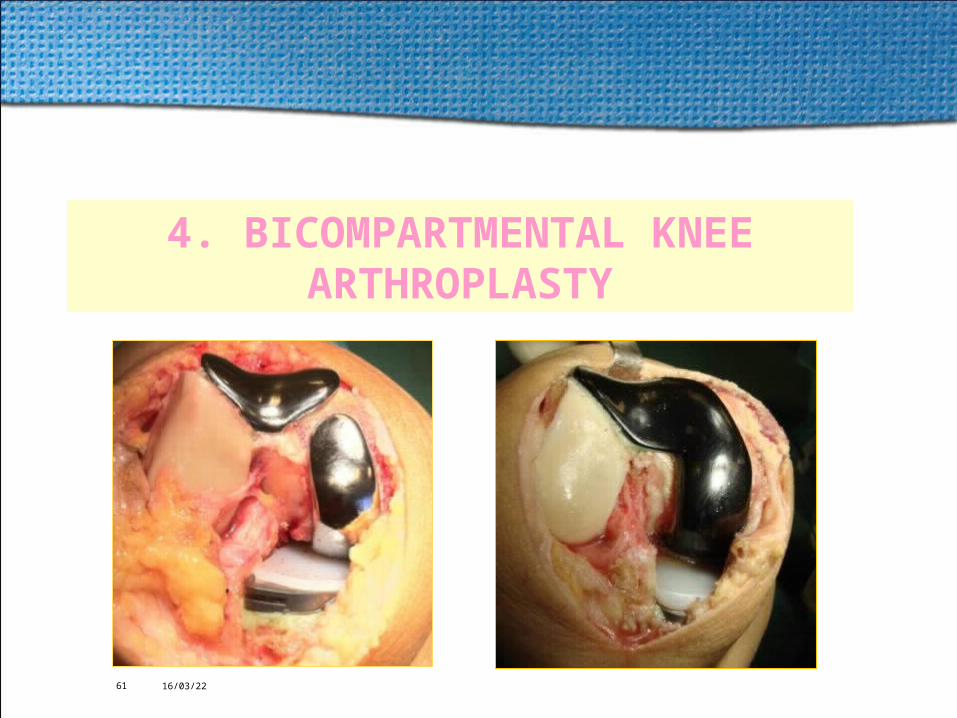
4. BICOMPARTMENTAL KNEE ARTHROPLASTY

64
1,5.X 1.5
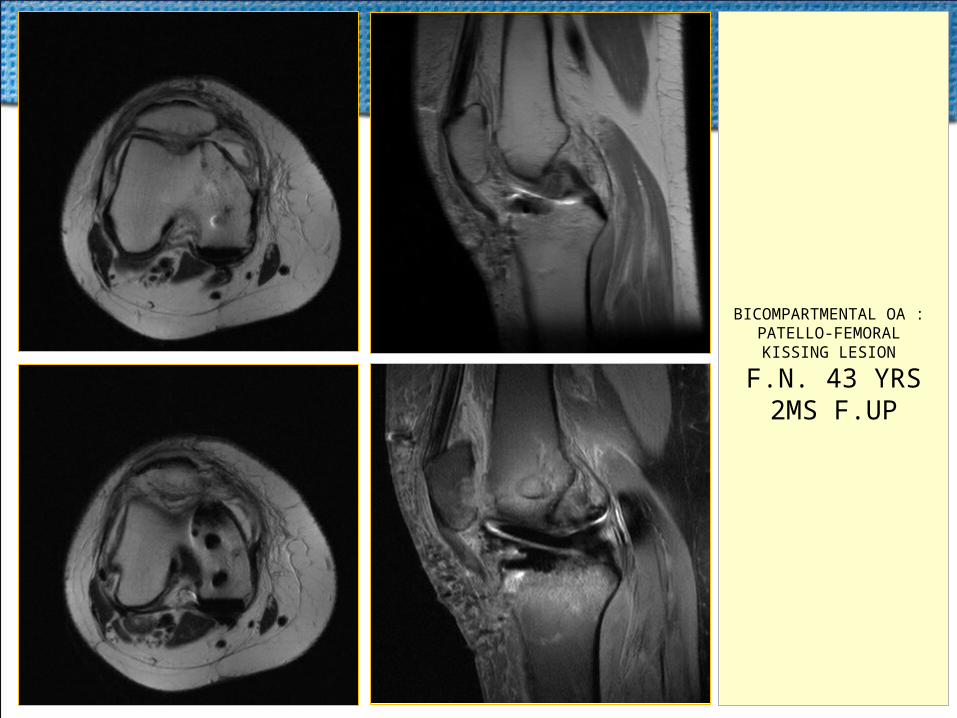
F.N. 43 YRS BICOMPARTMENTAL OA : PATELLO-FEMORAL KISSING LESION
3,5.X 1.5

F.N., female, 43 years old - grafted on 11/04/2010

F.N., female, 43 years old - grafted on 11/04/2010
67
BICOMPARTMENTAL OA : PATELLO-FEMORAL
KISSING LESION
F.N. 43 YRS2MS F.UP

BI-COMPARTMENTAL SOLUTION
2-Piece bi-compartmental solution
Zimmer Uni and Gender Solutions™ PFJ can be used as a bi-compartmental solution

1: INDEPENDENT APPROACH
Components positioned independently
Result: Proper balancing achieved
PFJ positioned in trochlear groove
Uni femoral component balanced parallel to the Uni tibial component

2: PROPER ALIGNMENT
PFJ implant alignment and external rotation achieved• Result: Assists in proper patella tracking
• PFJ to UKA Kinematics:• Extension: Patella tracks on the trochlear groove• Higher Flexion: Patella transitions to the condyles

3: TRUE PATIENT MATCHING
Not all femurs are alike – clearance depends on the anatomy Independently size the Zimmer Unicondylar implant
Independently size the Gender Solutions PFJ
Result: Bi-compartmental approach
Larger Gap
Smaller Gap
Femur #1900f (size E)
PF Size 2, ZUK Size 3
Femur #2890f (size D)
PF Size 2, ZUK Size 3
Factors affecting clearance:
PFJ size, UKA size, femur size, implant placement

93
5. TRICOMPARTMENTAL ARTHRITIS:RESURFACING
TOTAL KNEE ARTHROPLASTY
19/04/2394
With current designs of prosthesis and surgical techniques, it is reasonable to expect gaining a range of motion of the knee from 0° to 110°
after total knee arthroplasty (TKA)
In some countries, squatting and sitting on the floor are essential
in their activities of daily lives:
deep flexion of the knee after TKA may be required.
Achieving a deep flexion angle andmaintaining the stability of the knee
are competing goals and require refinements in design and
careful surgical technique.

19/04/2395 19/04/2395
WHAT ABOUT NORMAL KNEE FLEXION ROM ?
Dati: Dr NiwaAigh UniversityNagoya, Giappone
FlessioneRotazione
InternaRotazione
EsternaAdduzione Abduzione
Camminare in piano 55-75° 4-7° 3-7° 8-10° 1-3°
Salire/scendere scale 75-140° 4-19° 2-5° 9-19° 0-5°
Alzarsi/sedersi da sedia 90-130° 3-25° 0-7° 10-20° 0°
Sedersi "boh" (Giappone) 130-150° 22-29° 0° 10-34° 0°
Sedersi accosciati 147° 23° 0° 8° 0°
Alzarsi da terra 136° 39° 0° 30° 0°
Walk
Up / Down Stairs
Up / Down Chairs
Kneeling / Squatting
Japanese Stay
Standing up
Flexion Internal rotation
Extern rotation
19/04/2397
WHAT ABOUT FLEXION AFTER TKA?
“...The study does confirm that, for most patients, knee replacement
restores significant degree of function […] However, these patients report
significant limitations in doing some activities that are more physically demanding
but nonetheless important”
J.M. Weiss et al.:
“What Functional Activities Are Important to Patients With Knee Replacements?”
CORR, n. 404, pagg. 172-188, 2002

19/04/2398
CALLAGHAN, J.A.M.A., 1994CALLAGHAN, J.A.M.A., 1994
Meta - Analisys (57 jobs)
Average highest flexion in traditional 110°
NexGen Clinical Feedback Study (Rest of the World)
0
500
1000
1500
2000
2500
<60 65 75 85 95 105 115 125 135 145 155 +
Post-op flexion
Nu
mb
er o
f p
atie
nts
Li et al, JBJS 2004Li et al, JBJS 2004
WHAT ABOUT FLEXION AFTER TKA?

19/04/2399
Patients needs are constantlly increasing:
our average profile patients are
always younger
always more active
always more informed
always more demanding,
…
but some very common physical activities but some very common physical activities need higher knee flexion (> 120°)...need higher knee flexion (> 120°)...

19/04/23100
100100
Elements to flexion optimize in TKAElements to flexion optimize in TKA
1. Patient choice and former flexion degree
2. Surgical technique
3. Prosthesis Design
4. Post-op. rehab.

104104104
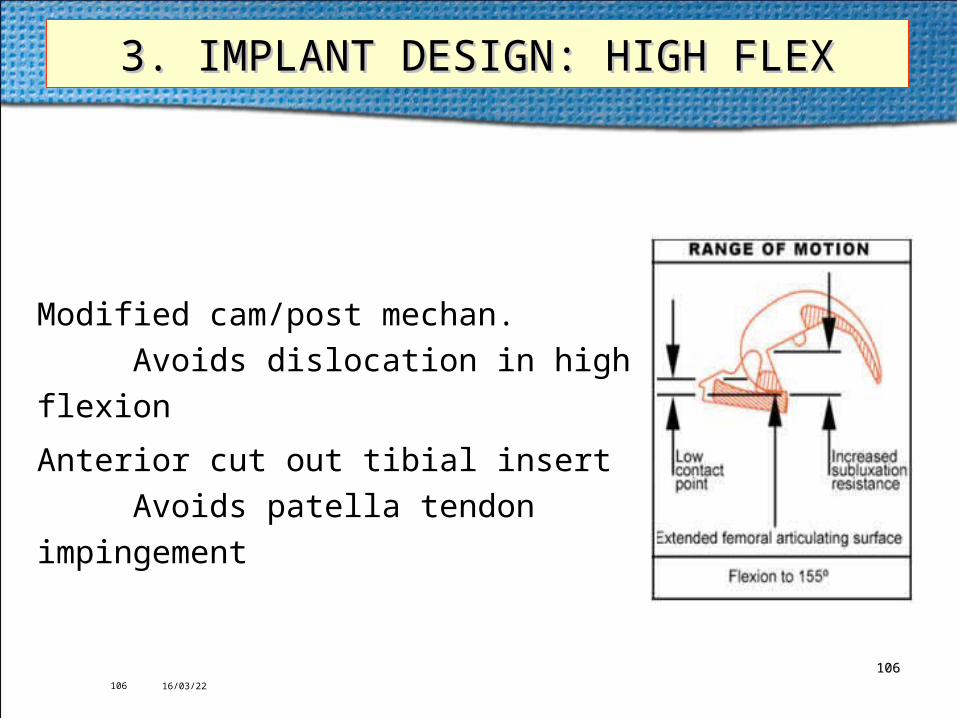
- 2 mm more in Flexion . The radius of the posterior femoral condyles has been
extended to provide larger tibio-femoral contact area
in high flexion
- Increased contact area
- Increased posterior femoral translation
- Modified cam/post mechanism to avoid
dislocation in high flexion
-Anterior cut out tibial insert to avoid patella
tendon impingement
Theoretical flexion > 130° to 155° 104104
3. IMPLANT DESIGN3. IMPLANT DESIGN

19/04/23105
105105
3. IMPLANT DESIGN: HIGH FLEX3. IMPLANT DESIGN: HIGH FLEX
• a PCL-substituting design can provide more predictable postoperative a PCL-substituting design can provide more predictable postoperative flexion because of the absence of the PCL, which is tight in deepknee flexion because of the absence of the PCL, which is tight in deepknee flexionflexion
• a smaller posterior femoral condyle componenta smaller posterior femoral condyle component provides a larger flexion provides a larger flexion gap, and passive flexion can be increased with this type of prosthesis. A gap, and passive flexion can be increased with this type of prosthesis. A smaller flexion gap can be obtained by a larger posterior femoral smaller flexion gap can be obtained by a larger posterior femoral component, and less passive flexion is obtained with this type of prosthesis.component, and less passive flexion is obtained with this type of prosthesis.
19/04/23106
106106
3. IMPLANT DESIGN: HIGH FLEX3. IMPLANT DESIGN: HIGH FLEX
Modified cam/post mechan.
Avoids dislocation in high flexion
Anterior cut out tibial insert
Avoids patella tendon impingement

19/04/23107
3. IMPLANT DESIGN: HIGH FLEX3. IMPLANT DESIGN: HIGH FLEX
The NexGen Flex Knees have addressed this issue with extended posterior femoral condyles. The radius of the posterior femoral condyles has been extended to
provide larger tibio-femoral contact area in high flexion (Fig.)In effect, the conformity between the femoral component and the tibial articular surface is enhanced. Increased contact area during flexion of up to 155° helps
reduce the possibility of point loading in high flexion.
In addition, an anterior cut out oftibial insert is made to avoid patellar tendonimpingement during deep flexion.

19/04/23108
108108
3. IMPLANT DESIGN : HIGH FLEX3. IMPLANT DESIGN : HIGH FLEX
In a posterior stabilized design, the cam/spine mechanism provides mechanical rollback while reducing the potential of anterior subluxation of the femur.
In some posterior stabilized knees, as the knee goes into deeper flexion, the cam on the femoral component begins to move superiorly on the spine of the tibial articular surface. This may increase the
possibility of anterior femoral subluxation.
To address this subluxation issue, the shape of the cam on the LPS-Flex Femoral Component has been modified to contact the spine more
inferiorly and thereby provide a greater jump height at flexion angles greater than 130°
19/04/23109
109109
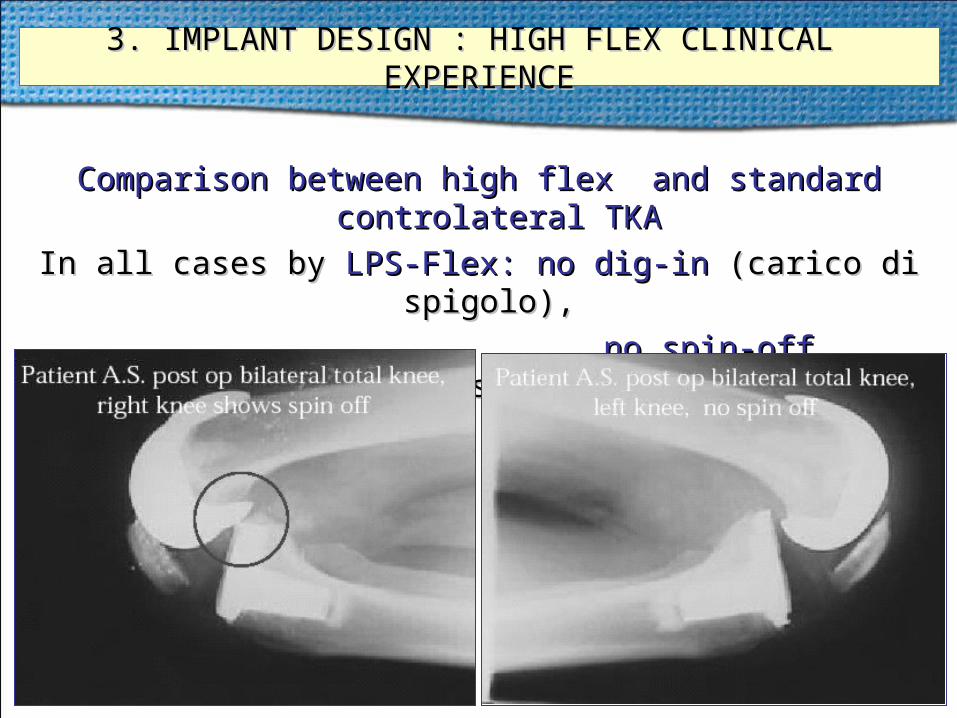
3. IMPLANT DESIGN : HIGH FLEX CLINICAL EXPERIENCE3. IMPLANT DESIGN : HIGH FLEX CLINICAL EXPERIENCE
Comparison between high flex and standard controlateral TKAComparison between high flex and standard controlateral TKA
In all cases byIn all cases by LPS-Flex: no dig-inLPS-Flex: no dig-in (carico di spigolo),(carico di spigolo),
no spin-offno spin-off (sublussazione)(sublussazione)

19/04/23110
3. IMPLANT DESIGN : HIGH FLEX - I ESPERIENZA CLINICA
Il 71% delle articolazioni protesizzate ha riacquisito una flessione 140°
Nessuna complicanza a carico della femoro-rotulea e dell’apparato estensore
Dr. Sam Tarabichi, American Hospital, Dubai, E.A.U.
174 TKA in 100 pazienti (74% bilaterali) dal 01/1999 al 02/2002 Protesi impiantata: NexGen® LPS-Flex Mobile
19/04/23114
114114
RESULTS IN LITERATURERESULTS IN LITERATURE
• Better Contact in High Flexion
reduced stress & wear of the poly and No difference after 2 years in flexion
• Better flexion of 12° after 2 years
Kim et al, 2005, JBJS
Huang et al, 2005, J Arthroplasty

115115115
10 to 12 mm TOTAL RESECTIONNEXGEN FLEX LPS
TANTALUM –UHMWPERESURFACING TKA

116116116

119
Bi-Lateral Implant
119119

120120120

121
M.R. m 70 yrs old : concurrent bilateral bicompartmental arthroplasty DEUCE on 07/02/2010
10 ms f.up

19/04/23122
KNEE DEEP FLEXION AVERAGE 141.9° (PREOP. 112.8°)BMI < 29 normal/overweight PREOP 138° POSTOP 151°
BMI> 30 (obese class I) PREOP 115° POSTOP 123°
• CROSS-LEG SITTING possible in 90.6%
• SQUATTING 39.5%• KNEELING 38.9%
• STANDING-UP FROM THE FLOOR 87%• STANDING-UP FROM A CHAIR 99.9
• ASCENDING STAIRS 98%• DESCENDING STAIRS 92%

19/04/23127
Why Gender?
• NexGen Clinical Feedback Program.
The European subset includes:13,970 ♀, 6,102 ♂
70% ♀, 30% ♂
• Register of the Primary TKA's performed in
Germany in 2004:77,848 ♀, 32,501 ♂
71% ♀, 29% ♂
Epidemiology – TKA in Europe
More than two-thirds of the patients who undergo TKA in Europe are women

19/04/23128
Why Gender?
Women have more knee pain(Source: Arthritis Foundation)
" […] women post–total knee arthroplasty (TKA) were more likely to have complications and longer average hospital lengths of stay“Weaver et al. J. Arthroplasty 2003; 18:693
Women have more post-TKA complications
"Gender was a predictor in thephysical performance measure models"Kennedy et al. J. Arthroplasty 2006
Women have slower and worse post-TKA functional recovery
"Revision rates seem to be affected by both age and gender“Kurtz et al. "The future burden of hip and knee revision" 2006
Women have a higher revision rate

19/04/23129 19/04/23129
Why Gender?
Women have higher rate of serious post-TKA PF complications that now have been solved
2001 - 2005 Istituto Ortopedico Galeazzi, Milano - Prof. S. Romagnoli
- 3112 Primary TKA's: 2,128 ♀, 984 ♂ (68.4% ♀, 31.6% ♂)
- 361 Revision TKA's : 302 ♀, 59 ♂ (83.7% ♀, 16.3% ♂)
- 45 Revision TKA’s for PF complications (1.46%): 41 ♀, 4 ♂ (91.2% ♀, 8.8%♂)
2006 - 08/2010 Villa Erbosa Hospital, Bologna - Prof. S. Zanasi - 998 Primary TKA's: 635 ♀, 363 ♂ (63.6% ♀, 36.4% ♂)- 176 Revision of other surgeon TKA's : 103 ♀, 73 ♂ (58.5% ♀, 41.5% ♂)- 6 Revision of our TKA’ s for PF complications from 2006 to 2007 ( no gender ) : : 6/185 (3.2%) 6/185 (3.2%) - 5 Revision of our navigated TKA’ s for PF complications from 2006 to 2010 ( no gender ) : 5/167 (3%)5/167 (3%)- 0 Revision TKA’s for PF complications from 2008 to 2010 ( gender ) :

19/04/23130
IntraOp Tricks
Lateral Release of the patella:
From literature 65% of the cases
Almost women
Undersize of the femoral component:
If the M/L dimension is too wide -> overhang,
The surgeon can decide to undersize the component but has to accept one of these 3 compromises:
1. Anterior Notching
2. overcut of the posterior condyles
3. Flexion position of the femoral component

19/04/23131
131131
Gender SolutionsGender Solutions
Females have a more trapezoidal distal femur as compared to males who have a rather rectangular oneFemales have a more trapezoidal distal femur as compared to males who have a rather rectangular one
• Females have a smaller M/L femoral width than males for the same A/P femoral heightFemales have a smaller M/L femoral width than males for the same A/P femoral height• Females have less prominent anterior condyleFemales have less prominent anterior condyle• Females have a relatively more internally rotated distal femur than malesFemales have a relatively more internally rotated distal femur than males
ThereforeTherefore::
The female knee is not simply a smaller version of a male kneeThe female knee is not simply a smaller version of a male knee The anatomic The anatomic shapeshape of a female bone is distinctive from that of a male bone of a female bone is distinctive from that of a male bone

19/04/23132
1. Thinner Profile
The bone in the front of a woman's knee is typically less prominent than in a man's.
TRADITIONAL IMPLANTS HAVE A THICKNESS IN FRONT THAT MAY END UP MAKING THEM FEEL "BULKY,“
WHICH MAY RESULT IN PAIN AND A DECREASE IN RANGE OF MOTION.The Zimmer Gender Knee has a thinner profile to
accommodate this anatomical difference between men and women.
Gender SolutionsGender Solutions

19/04/23133
2. More Natural Movement
The angle between the hip and the knee affects how the kneecap moves over the
thighbone when the knee is in motion.
WOMEN HAVE A DISTINCT SHAPE THAT FREQUENTLY RESULTS
IN A DIFFERENT ANGLE BETWEEN THE HIP AND THE KNEE WHEN COMPARED TO MEN. THE ZIMMER GENDER KNEE ACCOUNTS FOR THIS DIFFERENCE,
ALLOWING FOR MORE NATURAL MOVEMENT.
Gender SolutionsGender Solutions

19/04/23134
3. Contoured Shape The Zimmer GENDER KNEE HAS A CONTOURED SHAPE to
more closely match the narrower anatomy of a woman's knee.
This contouring PROVIDES FOR A MORE PRECISE FIT AND
MAY PREVENT THE IMPLANT FROM OVERHANGING THE BONE AND POTENTIALLY PRESSING ON OR DAMAGING SURROUNDING LIGAMENTS OR TENDONS.
Gender SolutionsGender Solutions

19/04/23137
R.S. 59yrs old F12nd day postop.
at discharge

19/04/23138
45th days postop
150°
R.S. 59yrs old F35th day postop.
at 1st f.up
139139139

19/04/23143
998 PRIMARY TKA FROM 1/2006 8/2010 635 TKA IN FEMALE SEX ( 63.6%) 468 NEXGEN FLEX LPS TKA - 185 STD FROM 1/2006 TO 11/2008 6 REVISION FOR PF COMPLICATION (3.2%) - 283 GSF FROM 1/2009 TO 08/2010 0 REVISION FOR PF COMPLICATION 167 NAVIGATED NO FLEX/NO GENDER TKA 5 REVISION FOR PF COMPLICATION (3%)

19/04/23144
283 NEXGEN FLEX GSF FROM 1/2009 TO 08/2010
• KNEE DEEP FLEXION AVERAGE 142° (PREOP. 121.6°)
• CROSS-LEG SITTING possible in 90.6%• SQUATTING 35.5%• KNEELING 29.9%
• STANDING-UP FROM THE FLOOR 87%• STANDING-UP FROM A CHAIR 99.9
• ASCENDING STAIRS 98%• DESCENDING STAIRS 94%
NO CASES TO REVIEW FOR PATELLO-FEMORAL COMPLICATIONS BUT• LIGHT ANTERIOR PAIN 5/283
• LIGHT PATELLAR PAIN 2/283 • NOT SEVERE BULKY KNEE SENSATION 3/283

19/04/23
The First Congress of Traumatologists and Orthopaedists “TRAUMATOLOGY AND ORTHOPAEDICS OF THE CAPITAL.
PRESENT AND FUTURE”February 16-17, 2012
The Moscow city Govermnent building
THANK YOU
Prof. S. Zanasi (Bologna, Italy)