Embed Size (px)
Citation preview
Are vaccinations really different to pharmaceuticals with respect to market access in Germany? – A systematic analysis of the German vaccine market access route Droeschel D1,2, Vollmer L 1,3, Krone FA2, Walzer S1,4
1 MArS Market Access & Pricing Strategy GmbH, Weil am Rhein, Germany
2 SRH Mobile University, Riedlingen, Germany
3 Christian-Albrechts-University, Kiel, Germany
4 State University Baden-Wuerttemberg, Loerrach, Germany
Corresponding author:Daniel Dröschel
MArS Market Access & Pricing Strategy GmbH
Geffelbachstr. 6
79576 Weil am Rhein
Germany
Contact: [email protected]
ISPOR 18th EuropeanCongress 2015
INTRODUCTION: l Since 2007 vaccinations have been a mandatory service of statutory health insurances (GKV) in Germany which was previously only been
a voluntary service according to the optional benefit package of the particular health insurance funds.[1, 2] l Although AMNOG was introduced to reorganize the medicine products market, it is not applicable for vaccines. l Immunization in Germany is organized de-centrally under the responsibility of the individual social health insurances and the state
ministries of health and municipality health authorities.l The inclusion of a vaccination in the GKV service catalogue requires a recommendation by the Robert Koch Institute (RKI) in Berlin as basis
for the Federal Joint Committee (G-BA) that further specifies details of the GKV‘s obligation to render services.[3]l The aim of this study was to analyze the market access route and compare that to the AMNOG process.
METHODS: l We reviewed systematically the regulatory and general information of relevant German authorities – of G-BA, STIKO (Staendige Impf-
kommission), Robert-Koch-Institute, SHI (Gesetzliche Krankenversicherungen), Head Association of Statutory Health Insurance Funds (GKV-Spitzenverband), different Associations of the Statutory Health Insurance Physicians (Kassenaerztliche Vereinigungen), IQWiG (Insti-tute for Quality and Efficiency in Health Care), Ministry of Health (Bundesministerium für Gesundheit), The Information System of the Fe-deral Health Monitoring (Gesundheitsberichterstattung Deutschland), Advisory Council on the Assessment of Developments in the Health Care System (Sachverständigenrat-Gesundheit), and did as well a grey literature research on publications of particular interest.
l Based on the information provided the market access routes have been analyzed and a pathway mapped.
RESULTS: l Based on the results of the systematic analysis we could ascertain specifics for the vaccination market. For an overview see Figure 1.
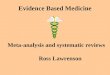
Figure 1: Stakeholders, processes and responsibilities for vaccination services in Germany (Source: Own representation following IGES Institute et al.[4])
Social Health Insurance (GKV Regional Level)
General directories and Surveillance
Appointing the commitee
The Standing Committee on Immunisation
State Ministries of Health
State Public Health Authorities
Municipality Public health authorities
Gives general directories and delegates the implementation and Surveillance to the states
Wholesaler/Pharmacies
Manufacturer
Framework agreement according to §20 Abs. 3 SGB V
Direct billing
evtl . Negotiations / Tendering
evtl. Negotiations / tendering
Evtl. Procurement of vaccines
Receiving Data on vaccinations administered
O er conditions negotiated
Assigns to negotiate and tendering
evtl . Negotiations / tendering
Assign to provide vaccination services to population
Federal Ministry of Health (Bundesministerium für Gesundheit)l The MoH gives general directories and delegates the implementation and Surveillance to the states.l Generally the MoH decides which vaccinations have to be covered by the SHIs, other can be provided by the public health offices.[5]
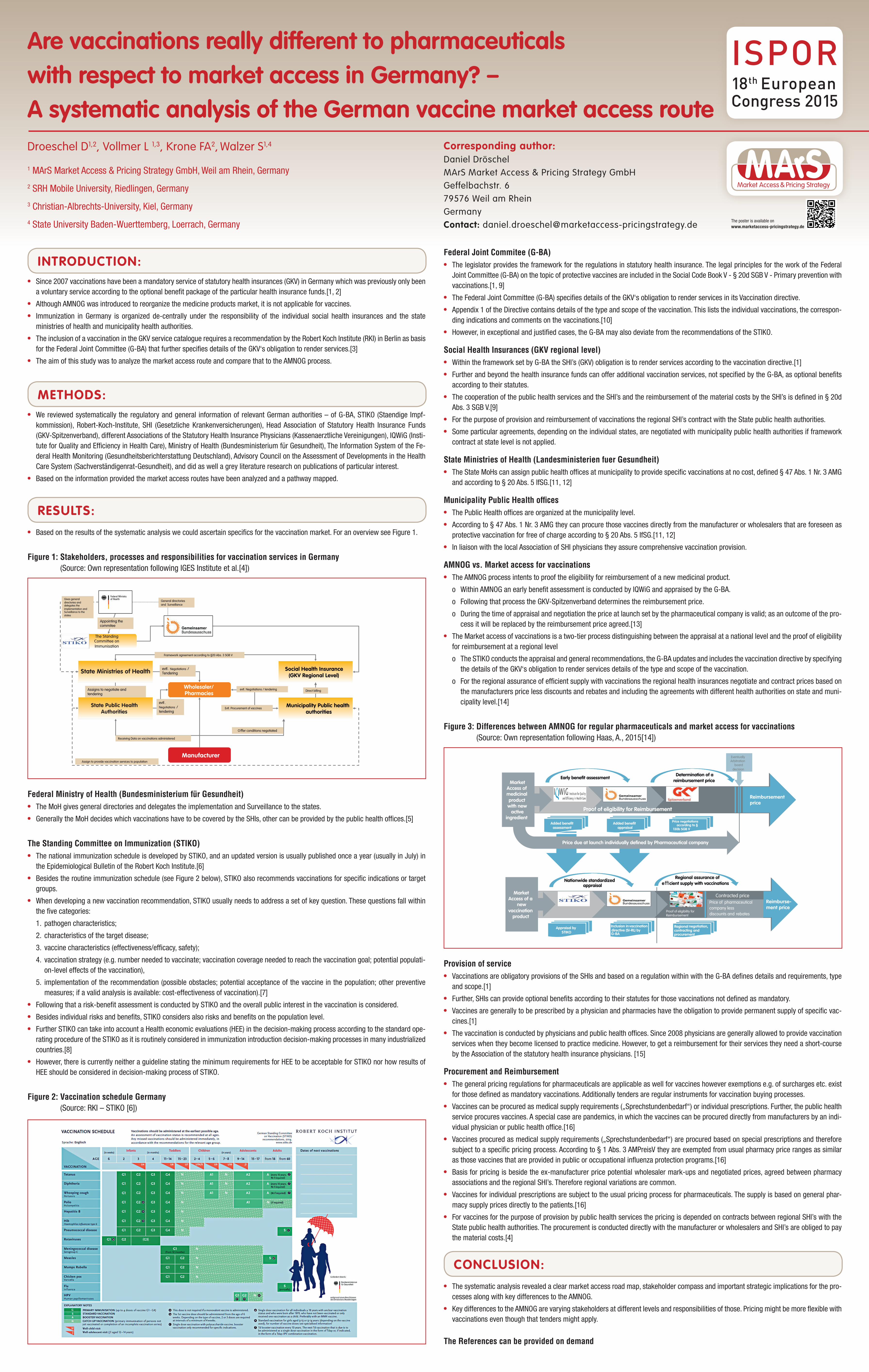
The Standing Committee on Immunization (STIKO) l The national immunization schedule is developed by STIKO, and an updated version is usually published once a year (usually in July) in
the Epidemiological Bulletin of the Robert Koch Institute.[6]l Besides the routine immunization schedule (see Figure 2 below), STIKO also recommends vaccinations for specific indications or target
groups.l When developing a new vaccination recommendation, STIKO usually needs to address a set of key question. These questions fall within
the five categories:
1. pathogen characteristics;
2. characteristics of the target disease;
3. vaccine characteristics (effectiveness/efficacy, safety);
4. vaccination strategy (e.g. number needed to vaccinate; vaccination coverage needed to reach the vaccination goal; potential populati-on-level effects of the vaccination),
5. implementation of the recommendation (possible obstacles; potential acceptance of the vaccine in the population; other preventive measures; if a valid analysis is available: cost-effectiveness of vaccination).[7]
l Following that a risk-benefit assessment is conducted by STIKO and the overall public interest in the vaccination is considered. l Besides individual risks and benefits, STIKO considers also risks and benefits on the population level.l Further STIKO can take into account a Health economic evaluations (HEE) in the decision-making process according to the standard ope-
rating procedure of the STIKO as it is routinely considered in immunization introduction decision-making processes in many industrialized countries.[8]
l However, there is currently neither a guideline stating the minimum requirements for HEE to be acceptable for STIKO nor how results of HEE should be considered in decision-making process of STIKO.
Figure 2: Vaccination schedule Germany (Source: RKI – STIKO [6])
Federal Joint Commitee (G-BA)l The legislator provides the framework for the regulations in statutory health insurance. The legal principles for the work of the Federal
Joint Committee (G-BA) on the topic of protective vaccines are included in the Social Code Book V - § 20d SGB V - Primary prevention with vaccinations.[1, 9]
l The Federal Joint Committee (G-BA) specifies details of the GKV‘s obligation to render services in its Vaccination directive.l Appendix 1 of the Directive contains details of the type and scope of the vaccination. This lists the individual vaccinations, the correspon-
ding indications and comments on the vaccinations.[10]l However, in exceptional and justified cases, the G-BA may also deviate from the recommendations of the STIKO.
Social Health Insurances (GKV regional level)l Within the framework set by G-BA the SHI’s (GKV) obligation is to render services according to the vaccination directive.[1]l Further and beyond the health insurance funds can offer additional vaccination services, not specified by the G-BA, as optional benefits
according to their statutes.l The cooperation of the public health services and the SHI’s and the reimbursement of the material costs by the SHI’s is defined in § 20d
Abs. 3 SGB V.[9]l For the purpose of provision and reimbursement of vaccinations the regional SHI’s contract with the State public health authorities.l Some particular agreements, depending on the individual states, are negotiated with municipality public health authorities if framework
contract at state level is not applied.
State Ministries of Health (Landesministerien fuer Gesundheit)l The State MoHs can assign public health offices at municipality to provide specific vaccinations at no cost, defined § 47 Abs. 1 Nr. 3 AMG
and according to § 20 Abs. 5 IfSG.[11, 12]
Municipality Public Health officesl The Public Health offices are organized at the municipality level. l According to § 47 Abs. 1 Nr. 3 AMG they can procure those vaccines directly from the manufacturer or wholesalers that are foreseen as
protective vaccination for free of charge according to § 20 Abs. 5 IfSG.[11, 12]l In liaison with the local Association of SHI physicians they assure comprehensive vaccination provision.
AMNOG vs. Market access for vaccinationsl The AMNOG process intents to proof the eligibility for reimbursement of a new medicinal product.
o Within AMNOG an early benefit assessment is conducted by IQWiG and appraised by the G-BA.
o Following that process the GKV-Spitzenverband determines the reimbursement price.
o During the time of appraisal and negotiation the price at launch set by the pharmaceutical company is valid; as an outcome of the pro-cess it will be replaced by the reimbursement price agreed.[13]
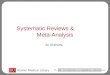
l The Market access of vaccinations is a two-tier process distinguishing between the appraisal at a national level and the proof of eligibility for reimbursement at a regional level
o The STIKO conducts the appraisal and general recommendations, the G-BA updates and includes the vaccination directive by specifying the details of the GKV‘s obligation to render services details of the type and scope of the vaccination.
o For the regional assurance of efficient supply with vaccinations the regional health insurances negotiate and contract prices based on the manufacturers price less discounts and rebates and including the agreements with different health authorities on state and muni-cipality level.[14]
Figure 3: Differences between AMNOG for regular pharmaceuticals and market access for vaccinations (Source: Own representation following Haas, A., 2015[14])
Determination of a reimbursement priceMarket
Access of medicinal product with new
active ingredient
Added benefit assessment
Early benefit assessment
Added benefit appraisal
Price negotiations according to §
130b SGB V
Eventually Arbitration
board decision
Price due at launch individually defined by Pharmaceutical company
Proof of eligibility for Reimbursement
Regional assurance of e cient supply with vaccinations
Market Access of a
new vaccination
product
Appraisal by STIKO
Nationwide standardized appraisal
Inclusion in vaccination directive (SI-RL) by G-BA
Regional negotiation, contracting and procurement
Price of pharmaceutical company less discounts and rebates
Proof of eligibility for Reimbursement
Contracted price
Reimbursementprice
Reimburse-ment price
Provision of servicel Vaccinations are obligatory provisions of the SHIs and based on a regulation within with the G-BA defines details and requirements, type
and scope.[1]l Further, SHIs can provide optional benefits according to their statutes for those vaccinations not defined as mandatory. l Vaccines are generally to be prescribed by a physician and pharmacies have the obligation to provide permanent supply of specific vac-
cines.[1]l The vaccination is conducted by physicians and public health offices. Since 2008 physicians are generally allowed to provide vaccination
services when they become licensed to practice medicine. However, to get a reimbursement for their services they need a short-course by the Association of the statutory health insurance physicians. [15]
Procurement and Reimbursementl The general pricing regulations for pharmaceuticals are applicable as well for vaccines however exemptions e.g. of surcharges etc. exist
for those defined as mandatory vaccinations. Additionally tenders are regular instruments for vaccination buying processes. l Vaccines can be procured as medical supply requirements („Sprechstundenbedarf“) or individual prescriptions. Further, the public health
service procures vaccines. A special case are pandemics, in which the vaccines can be procured directly from manufacturers by an indi-vidual physician or public health office.[16]
l Vaccines procured as medical supply requirements („Sprechstundenbedarf“) are procured based on special prescriptions and therefore subject to a specific pricing process. According to § 1 Abs. 3 AMPreisV they are exempted from usual pharmacy price ranges as similar as those vaccines that are provided in public or occupational influenza protection programs.[16]
l Basis for pricing is beside the ex-manufacturer price potential wholesaler mark-ups and negotiated prices, agreed between pharmacy associations and the regional SHI’s. Therefore regional variations are common.
l Vaccines for individual prescriptions are subject to the usual pricing process for pharmaceuticals. The supply is based on general phar-macy supply prices directly to the patients.[16]
l For vaccines for the purpose of provision by public health services the pricing is depended on contracts between regional SHI’s with the State public health authorities. The procurement is conducted directly with the manufacturer or wholesalers and SHI’s are obliged to pay the material costs.[4]
CONCLUSION:l The systematic analysis revealed a clear market access road map, stakeholder compass and important strategic implications for the pro-
cesses along with key differences to the AMNOG. l Key differences to the AMNOG are varying stakeholders at different levels and responsibilities of those. Pricing might be more flexible with
vaccinations even though that tenders might apply.
The References can be provided on demand
The poster is available on www.marketaccess-pricingstrategy.de