Embed Size (px)
Citation preview
睡眠Sleep
Professor Tung-Ping SuDepartment of Psychiatry
National Yang-Ming University
Taipei Veterans General Hospital
Dec. 24, 2007
Lecture for the 4th class of Dept of Medicine Lecture for the 4th class of Dept of Medicine
National Yang-Ming UniversityNational Yang-Ming University
Sleep Sleep
disturbancesdisturbances
正視失眠問題• 從流行病學角度來看,保守估計全台灣大約有 150~200 萬的人飽受失眠之苦
• 由於慢性失眠可能導致的社會問題 意外或交通事故 ( 高四倍 ) 個人健康、家庭生活與人際關係的干擾 因為注意力及記憶力障礙造成的損失
( 慢性失眠者比睡眠良好的人認知功能 表現降低大約 20%)
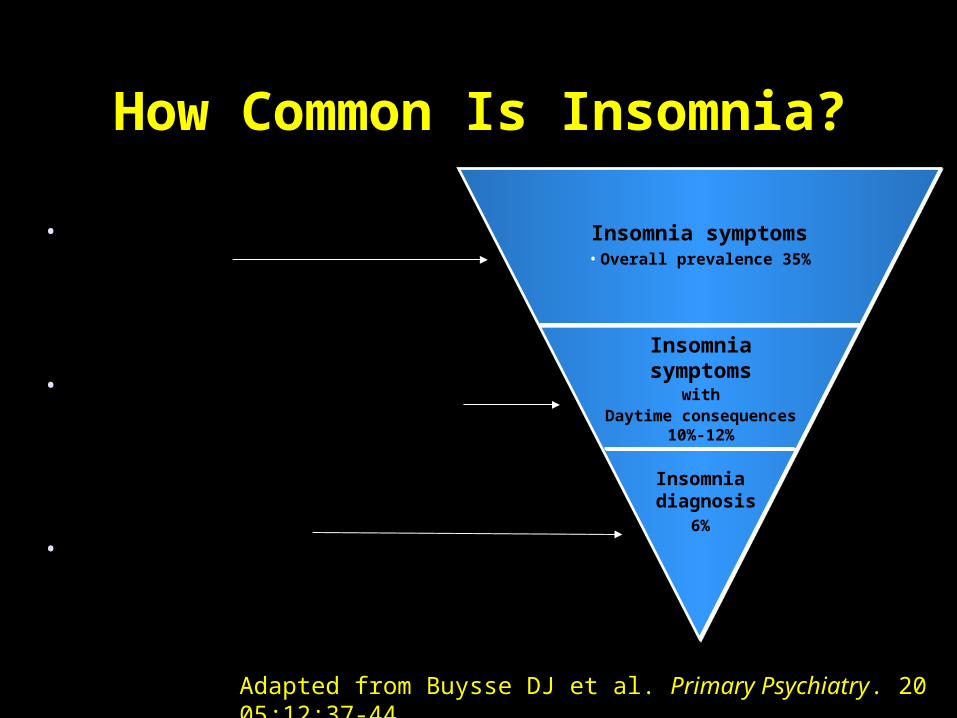
Insomnia diagnosis
6%
Insomnia symptoms
withDaytime consequences
10%-12%
Insomnia symptoms• Overall prevalence 35%
Adapted from Buysse DJ et al. Primary Psychiatry. 2005;12:37-44.
• Overall prevalence
• Symptomatic with consequences
• Actually diagnosed
How Common Is Insomnia?How Common Is Insomnia?
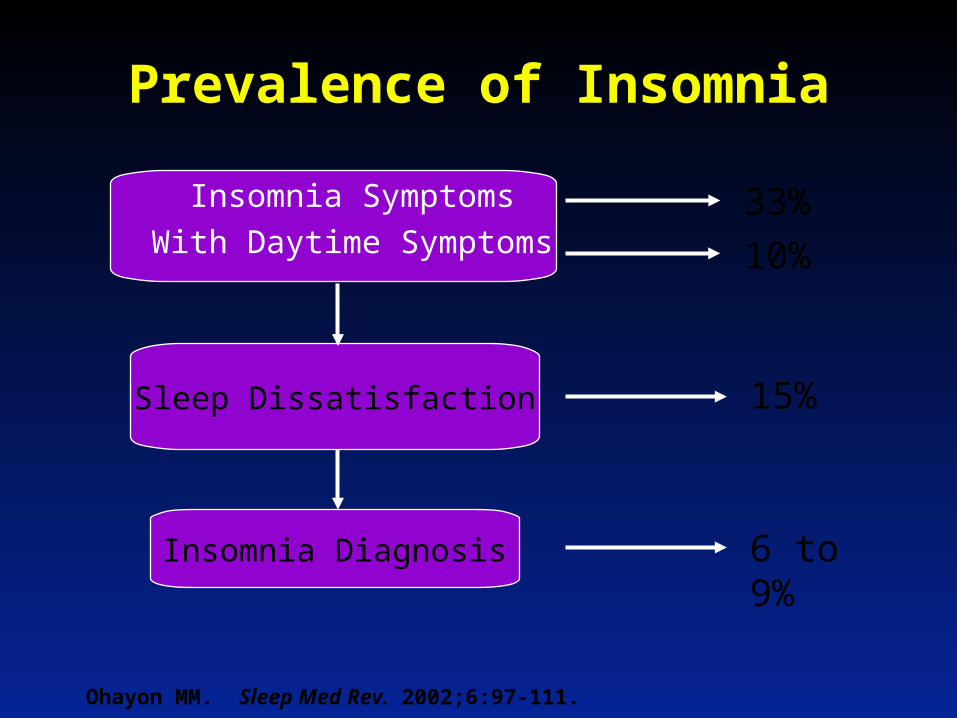
Sleep Dissatisfaction
Prevalence of Insomnia
Insomnia Symptoms
With Daytime Symptoms33%
10%
Ohayon MM. Sleep Med Rev. 2002;6:97-111.
Insomnia Diagnosis 6 to 9%
15%
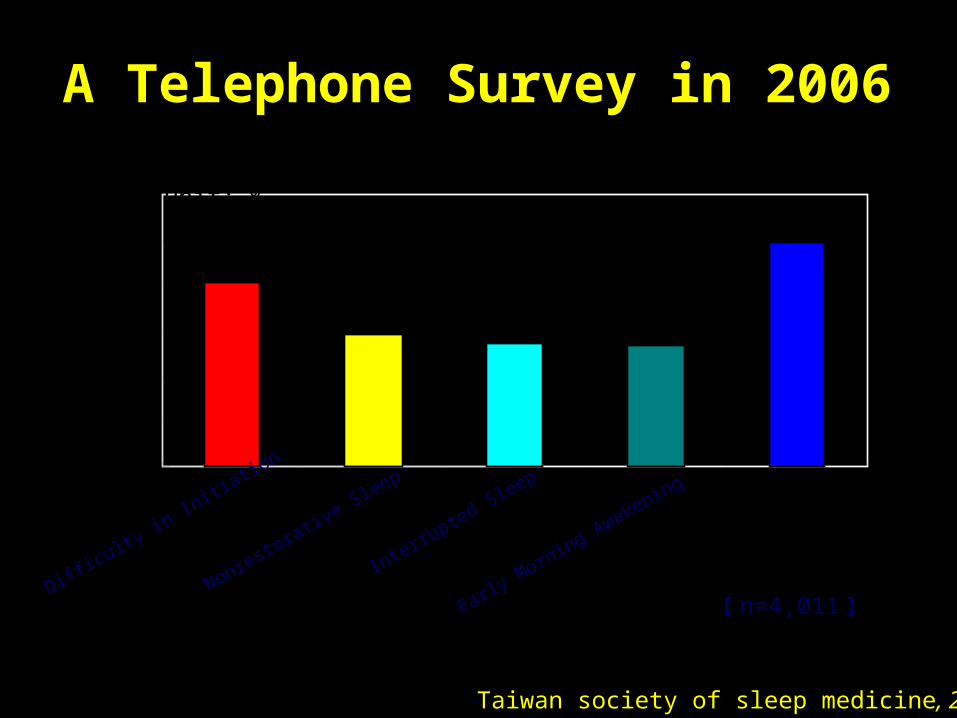
Taiwan society of sleep medicine, 2006
A Telephone Survey in 2006A Telephone Survey in 2006
20.2%
14.6% 13.5% 13.3%
24.8%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Difficulty in In
itiation
Nonrestorative Sleep
Interrupted Sleep
Early Morning AwakeningTOTAL
Unit: %
【 n=4,011】
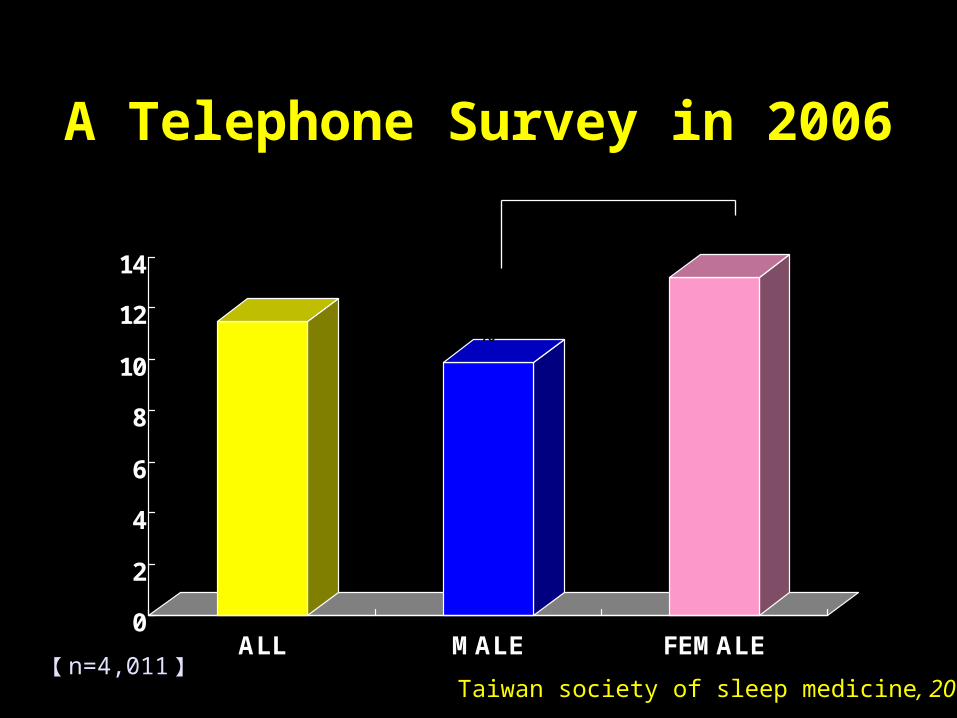
A Telephone Survey in 2006A Telephone Survey in 2006
0
2
4
6
8
10
12
14
ALL MALE FEMALE
11.5%
9.9%
13.2%
【 n=4,011】
P < 0.01
Taiwan society of sleep medicine, 2006
40-44 45-54 55-64 65-74 >=75
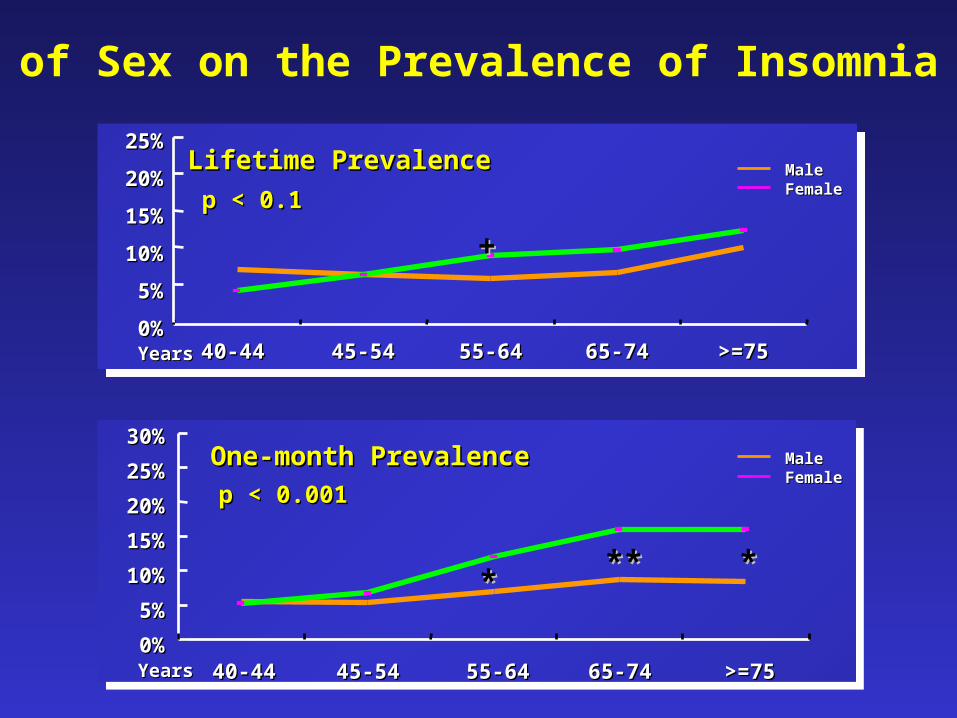
6.60% 6.20% 6.90% 10.30%6.60% 9.20% 9.90% 12.60%
40-44 45-54 55-64 65-74 >=75
5.50% 5.30% 7% 8.65% 8.40%5.20% 6.70% 12% 16% 16%
40-4440-44 45-5445-54 55-6455-64 65-7465-74 >=75>=75
40-4440-44 45-5445-54 55-6455-64 65-7465-74 >=75>=75
MaleMaleFemaleFemale
Lifetime PrevalenceLifetime Prevalence
p < 0.1p < 0.1
25%25%
20%20%
15%15%
10%10%
5%5%
0%0%
One-month PrevalenceOne-month Prevalence
p < 0.001p < 0.001
30%30%
25%25%
20%20%
15%15%
10%10%
5%5%
0%0%
MaleMaleFemaleFemale
Effect of Sex on the Prevalence of Insomnia by Age
YearsYears
YearsYears
++
****** **
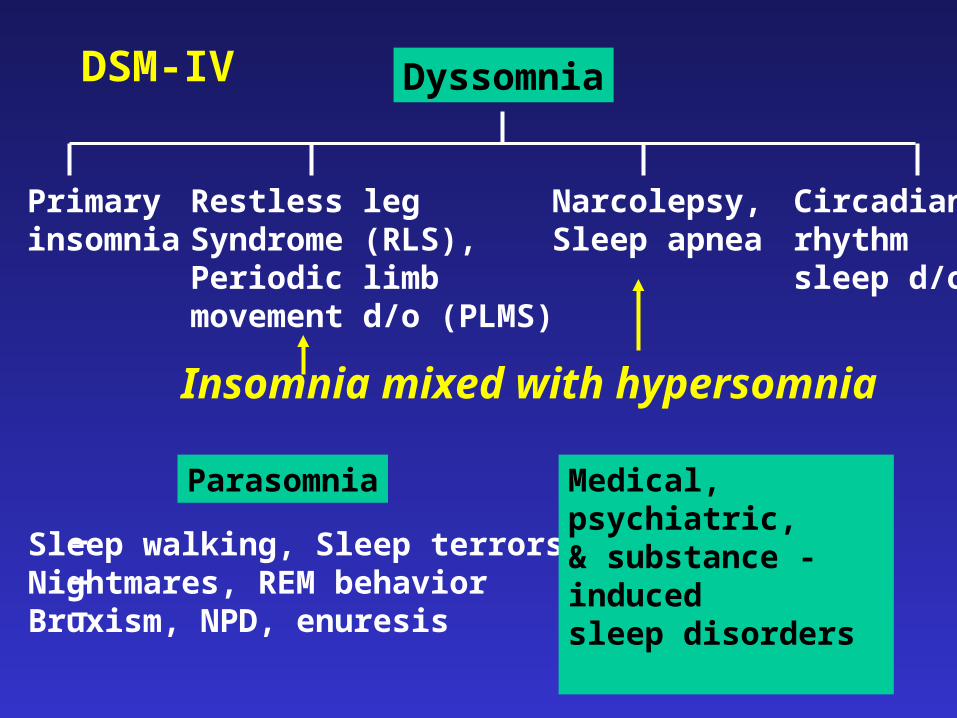
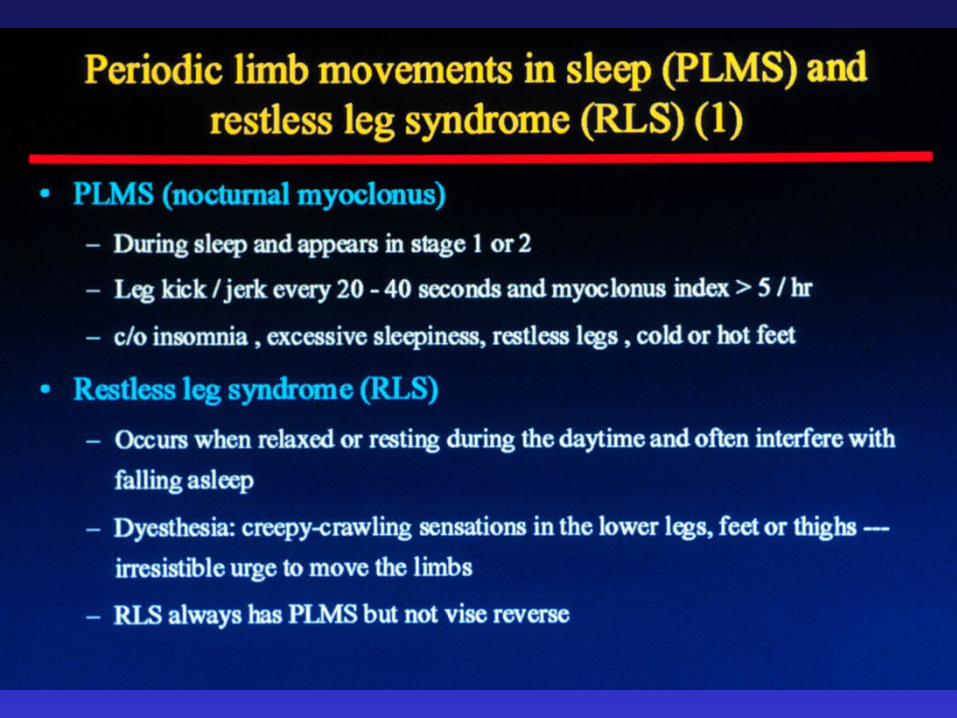
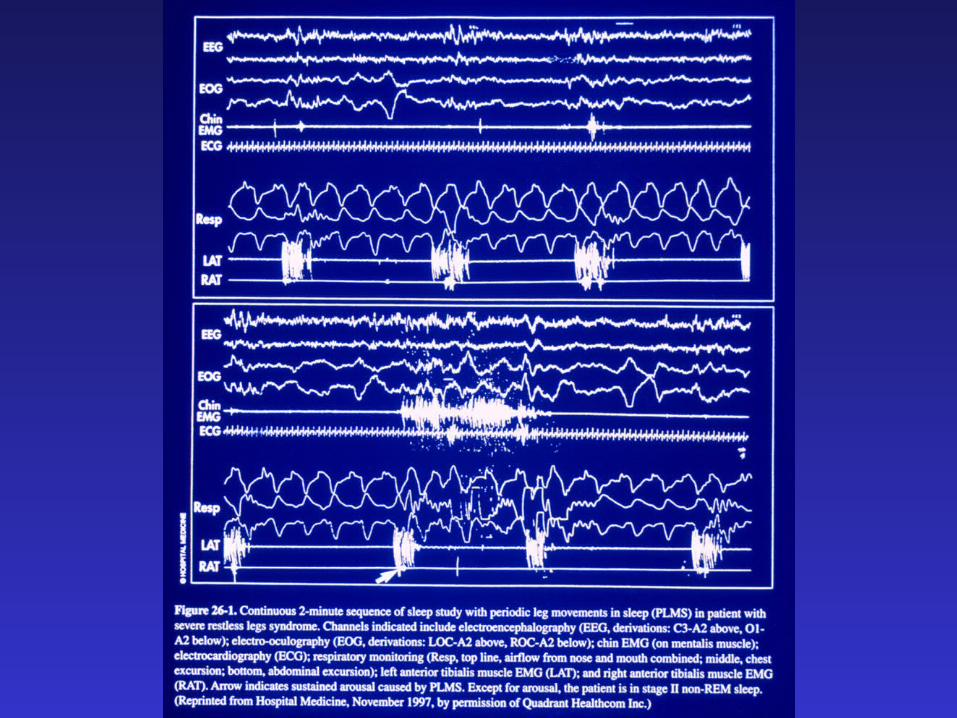
Dyssomnia
Primaryinsomnia
Restless legSyndrome (RLS),Periodic limbmovement d/o (PLMS)
Narcolepsy,Sleep apnea
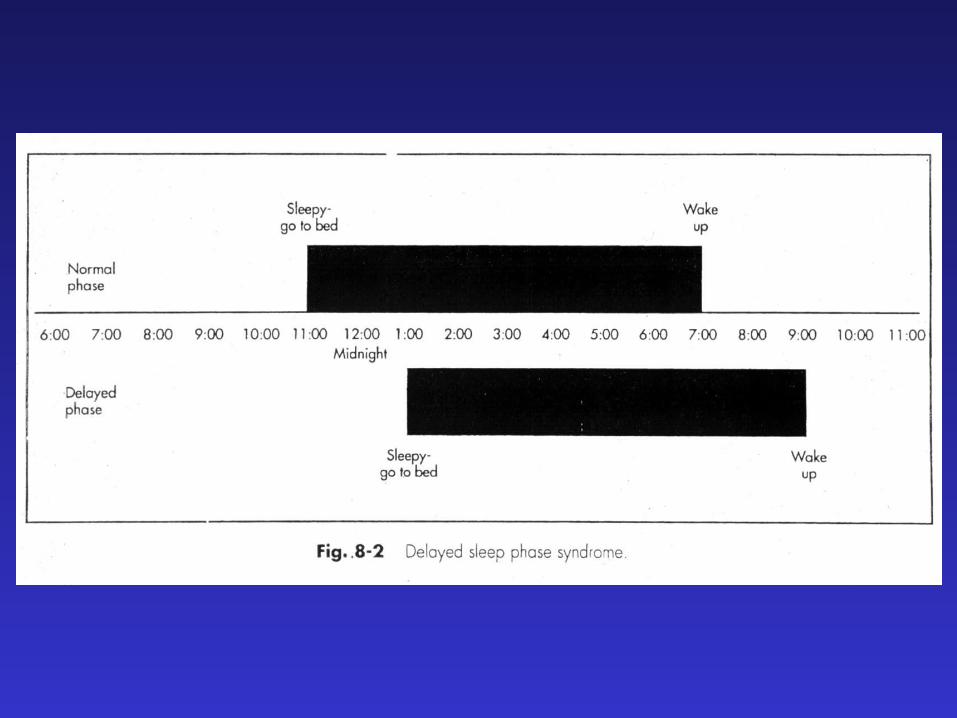
Circadianrhythmsleep d/o
Parasomnia
Insomnia mixed with hypersomnia
Sleep walking, Sleep terrorsNightmares, REM behaviorBruxism, NPD, enuresis
Medical, psychiatric,& substance - induced sleep disorders
DSM-IV
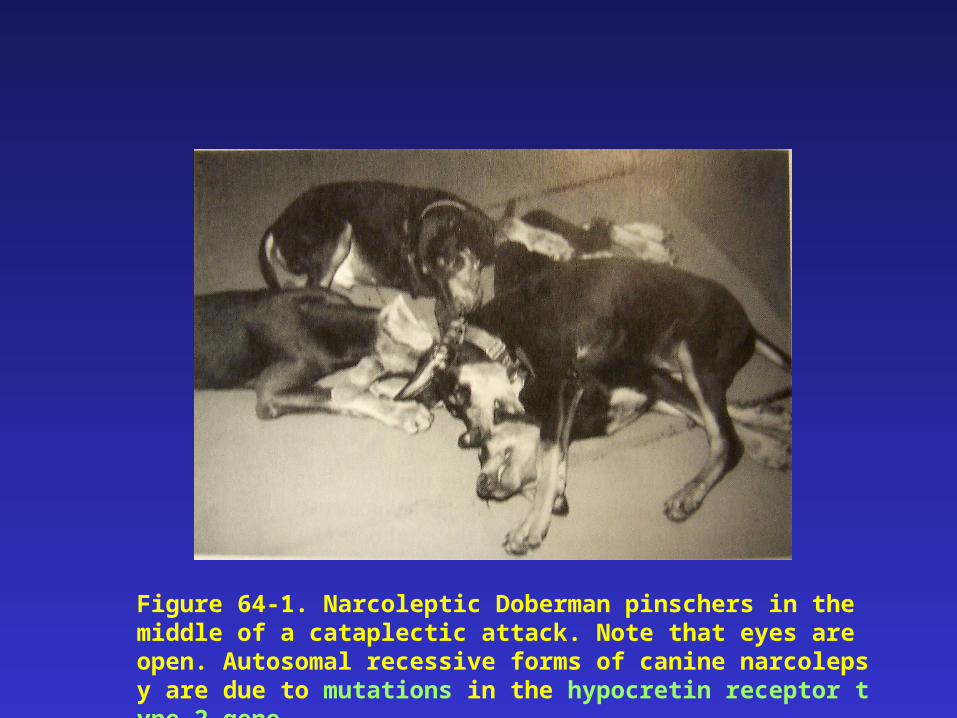
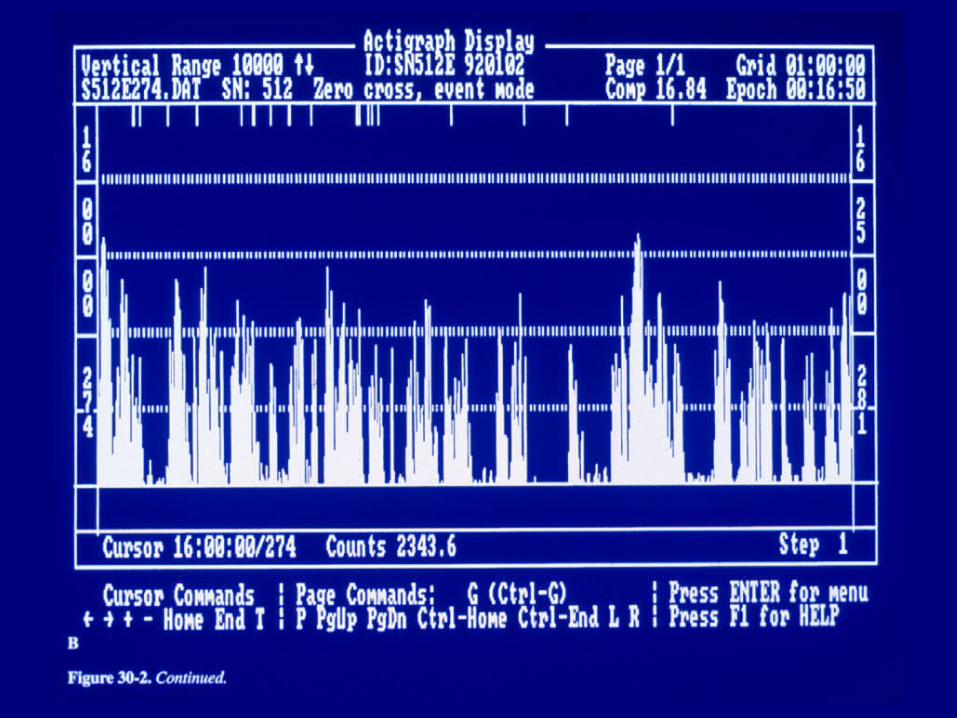
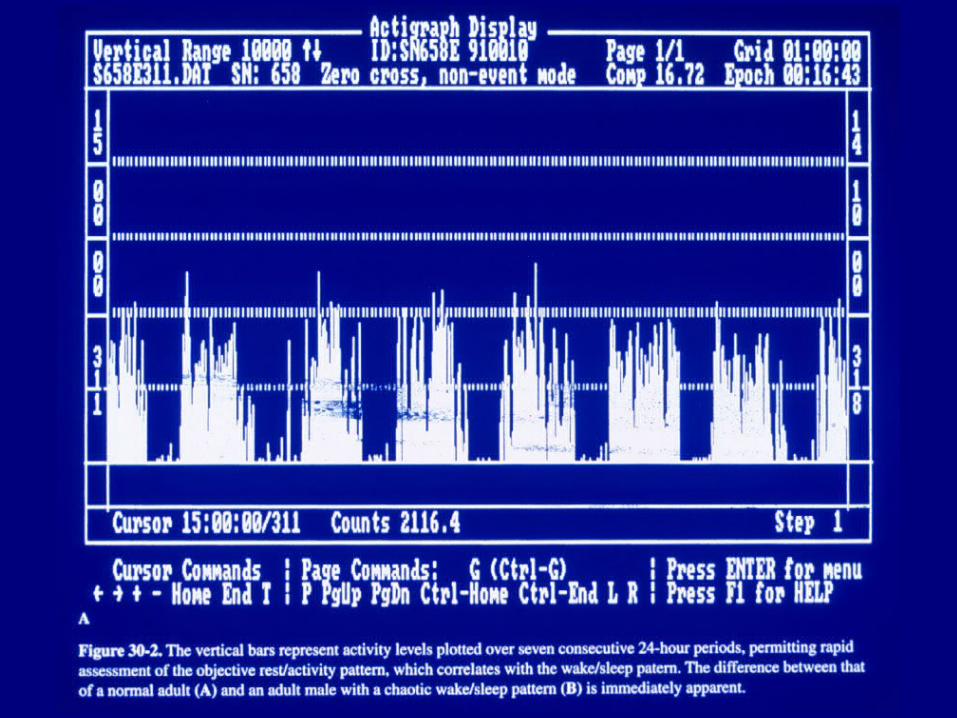
Figure 64-1. Narcoleptic Doberman pinschers in the middle of a cataplectic attack. Note that eyes are open. Autosomal recessive forms of canine narcolepsy are due to mutations in the hypocretin receptor type 2 gene.
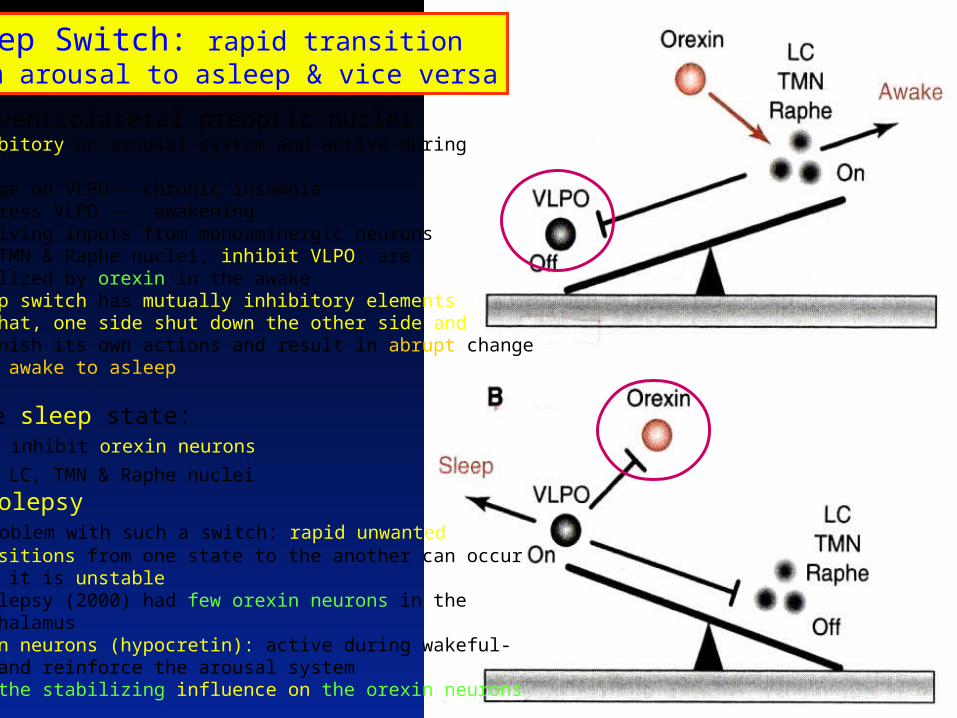
Sleep Switch: rapid transitionFrom arousal to asleep & vice versa
•VLPO: ventrolateral preoptic nuclei - Inhibitory on arousal system and active during sleep - Damage on VLPO---chronic insomnia - Suppress VLPO --- awakening - receiving inputs from monoaminergic neurons - LC, TMN & Raphe nuclei, inhibit VLPO, are stabilized by orexin in the awake - Sleep switch has mutually inhibitory elements - In that, one side shut down the other side and diminish its own actions and result in abrupt change from awake to asleep • In the sleep state: - VLPO inhibit orexin neurons
and LC, TMN & Raphe nuclei • Narcoolepsy - a problem with such a switch: rapid unwanted transitions from one state to the another can occur when it is unstable - Narcolepsy (2000) had few orexin neurons in the hypothalamus - Orexin neurons (hypocretin): active during wakeful- ness and reinforce the arousal system - Lost the stabilizing influence on the orexin neurons
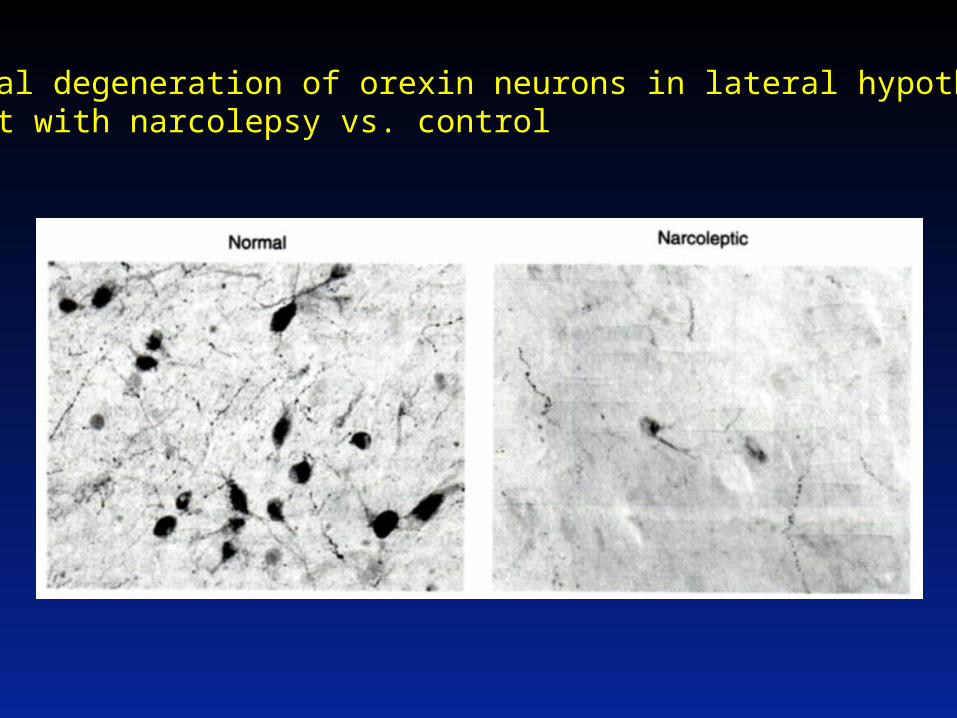
Neuronal degeneration of orexin neurons in lateral hypothalamusOf a pt with narcolepsy vs. control
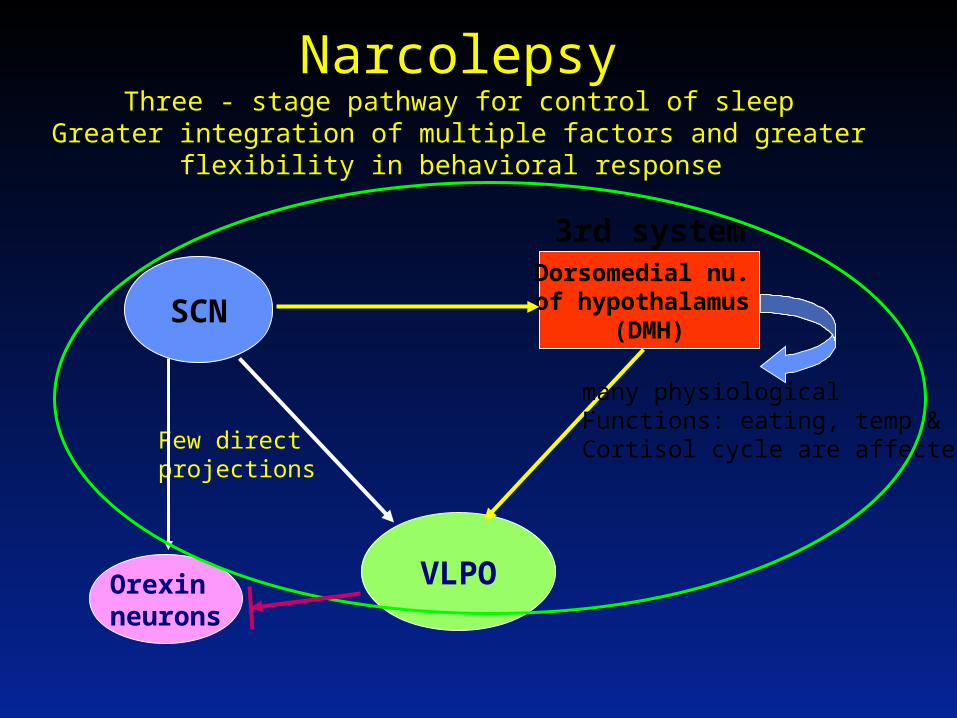
NarcolepsyThree - stage pathway for control of sleep
Greater integration of multiple factors and greater flexibility in behavioral response
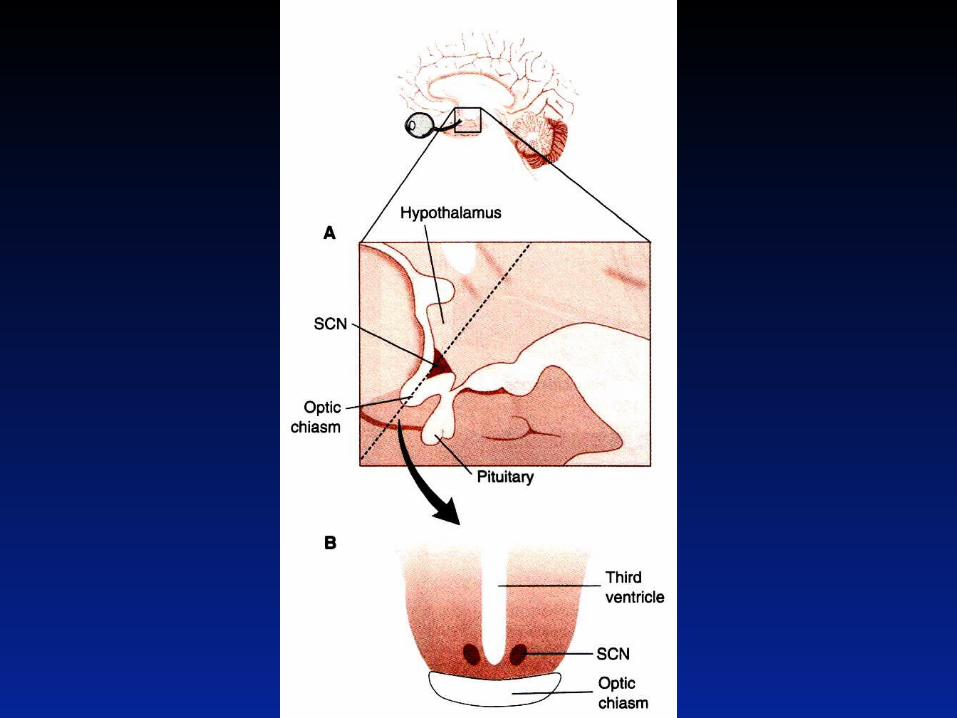
SCN
VLPO
Few directprojections
Orexin neurons
Dorsomedial nu. of hypothalamus
(DMH)
3rd system
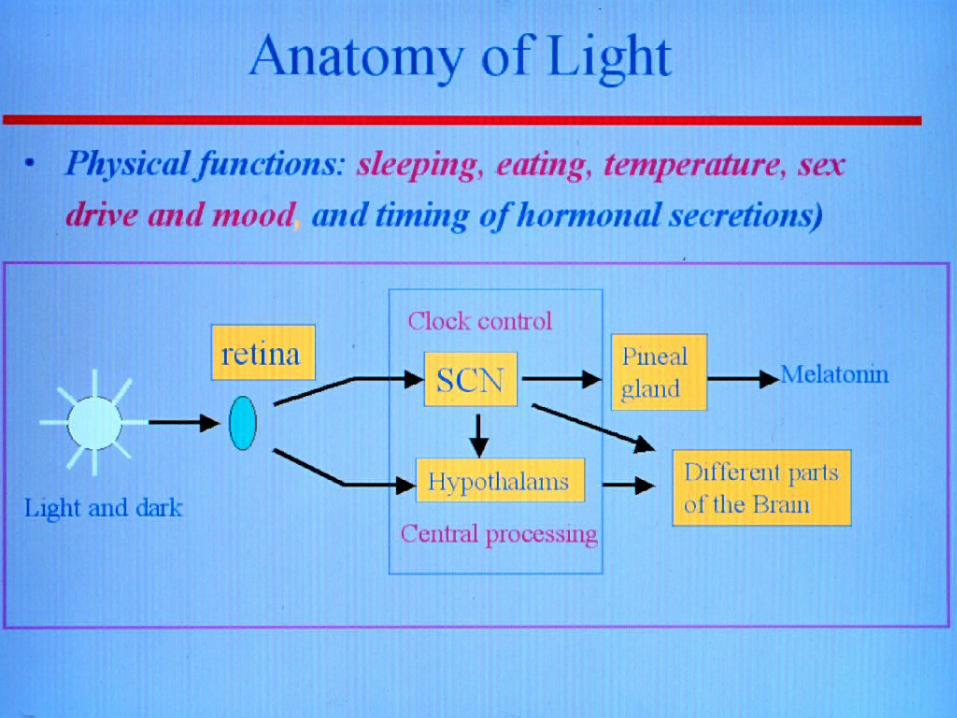
many physiologicalFunctions: eating, temp &Cortisol cycle are affected.
Obstructive Sleep Apnea
in Psychiatry
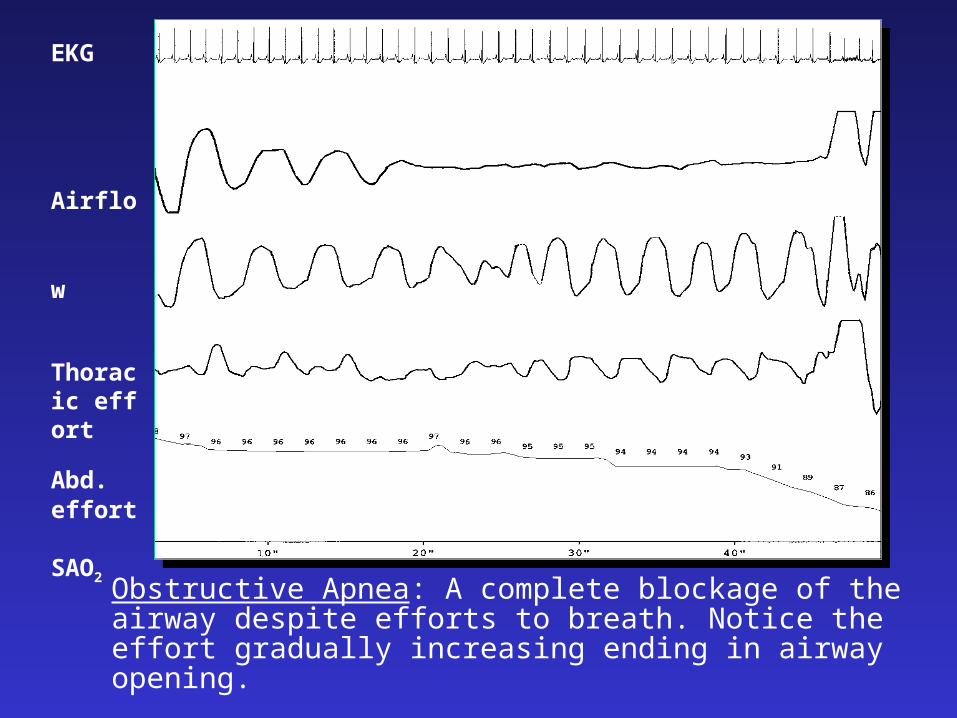
Obstructive Apnea: A complete blockage of the airway despite efforts to breath. Notice the effort gradually increasing ending in airway opening.
EKG
Airflow
Thoracic effort
Abd. effort
SAO2
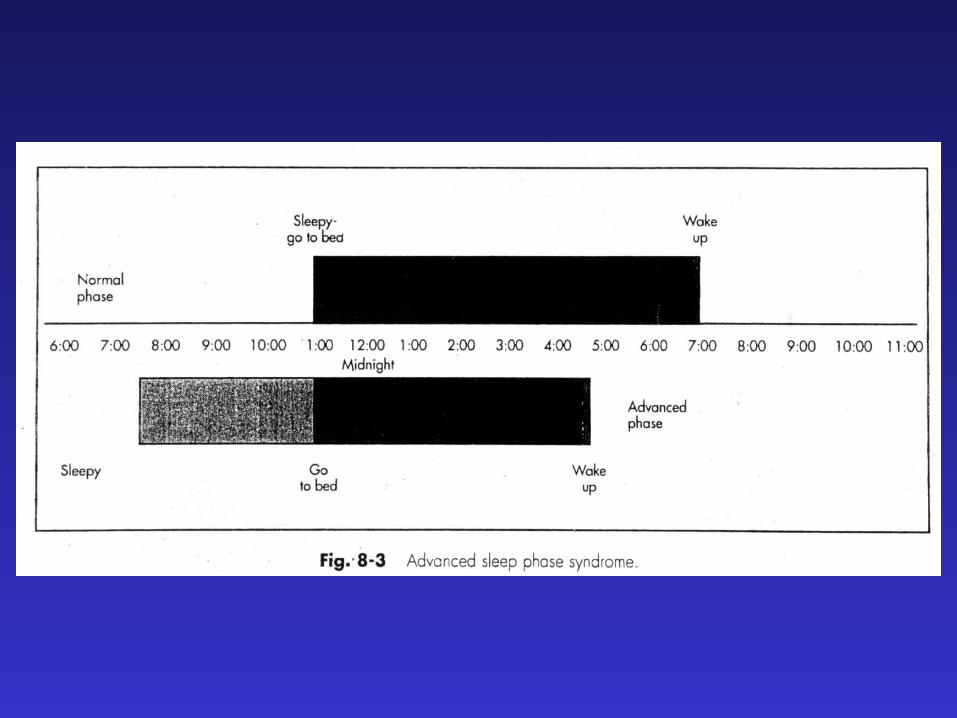
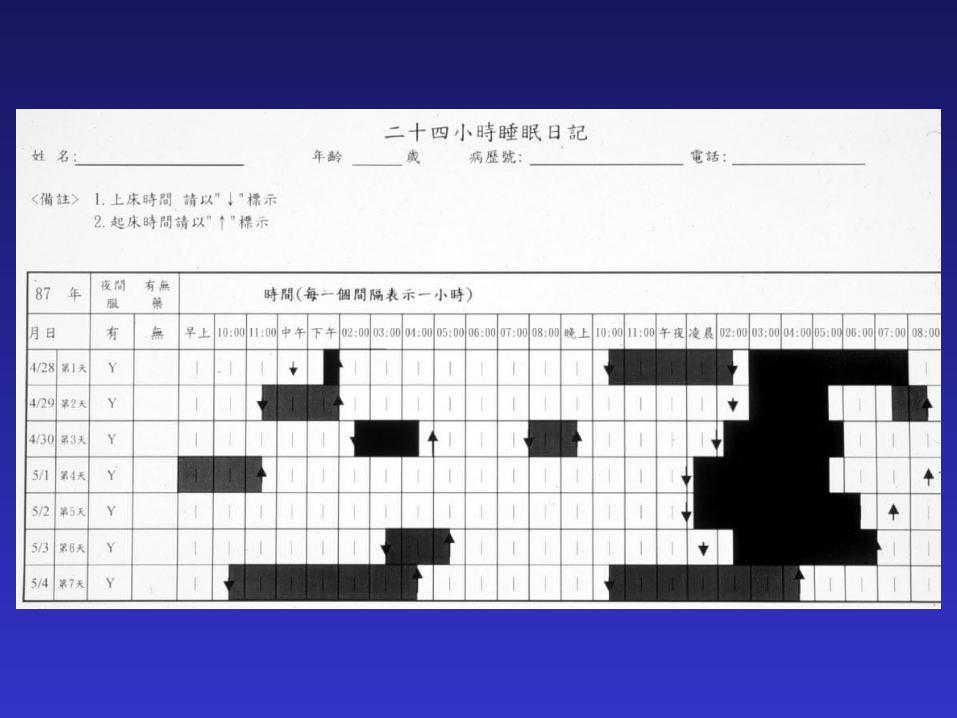
Circadian rhythm sleep disorder
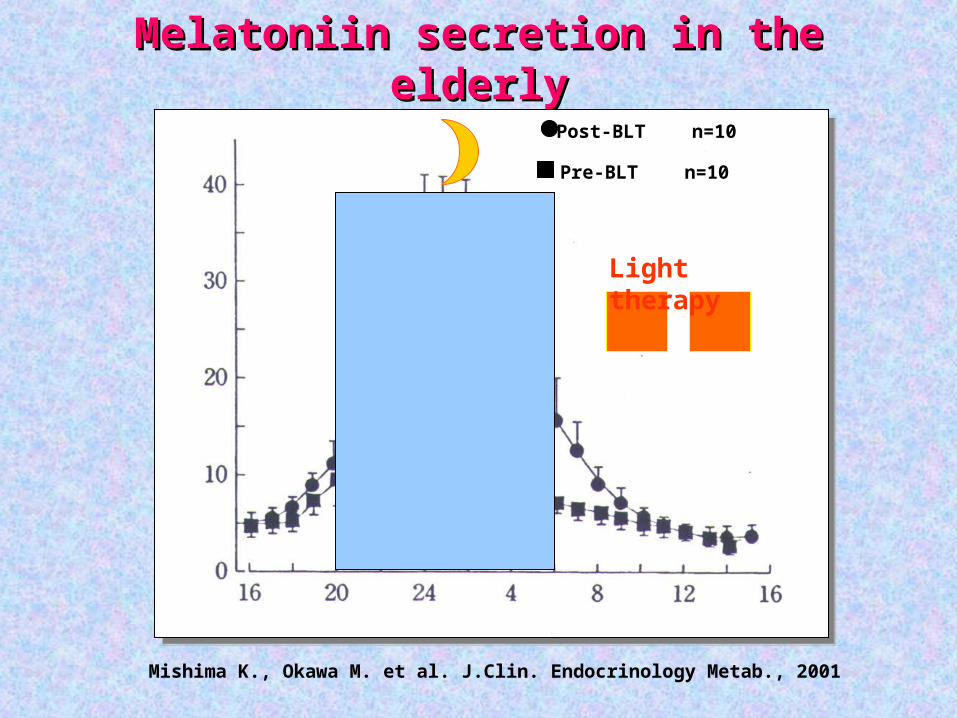
Melatoniin secretion in the elderlyMelatoniin secretion in the elderly
Post-BLT n=10
Pre-BLT n=10
Mishima K., Okawa M. et al. J.Clin. Endocrinology Metab., 2001
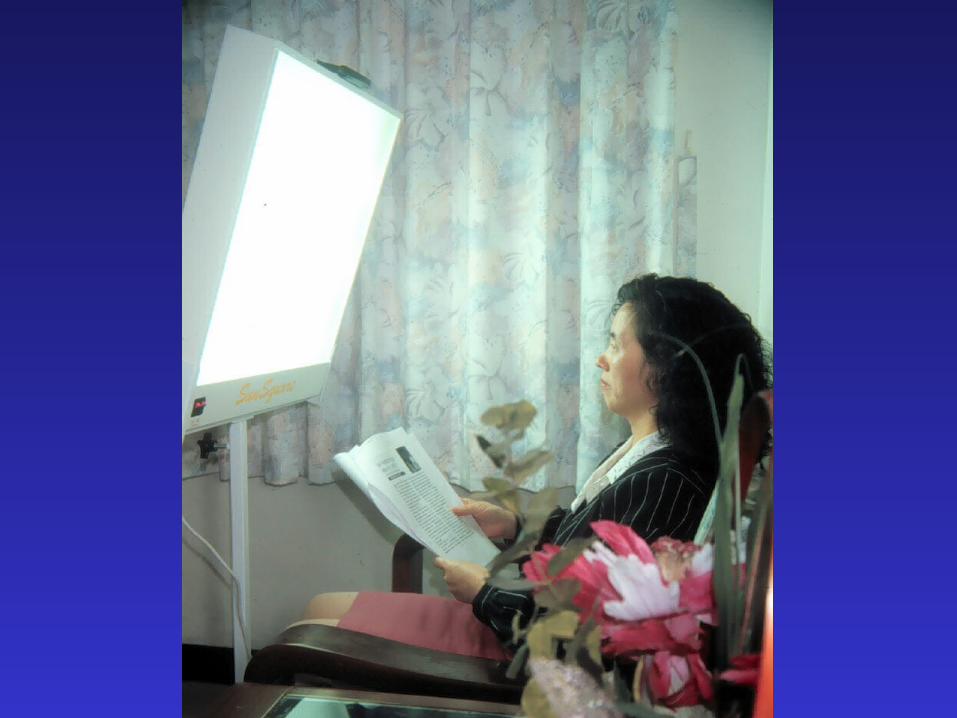
Light therapy
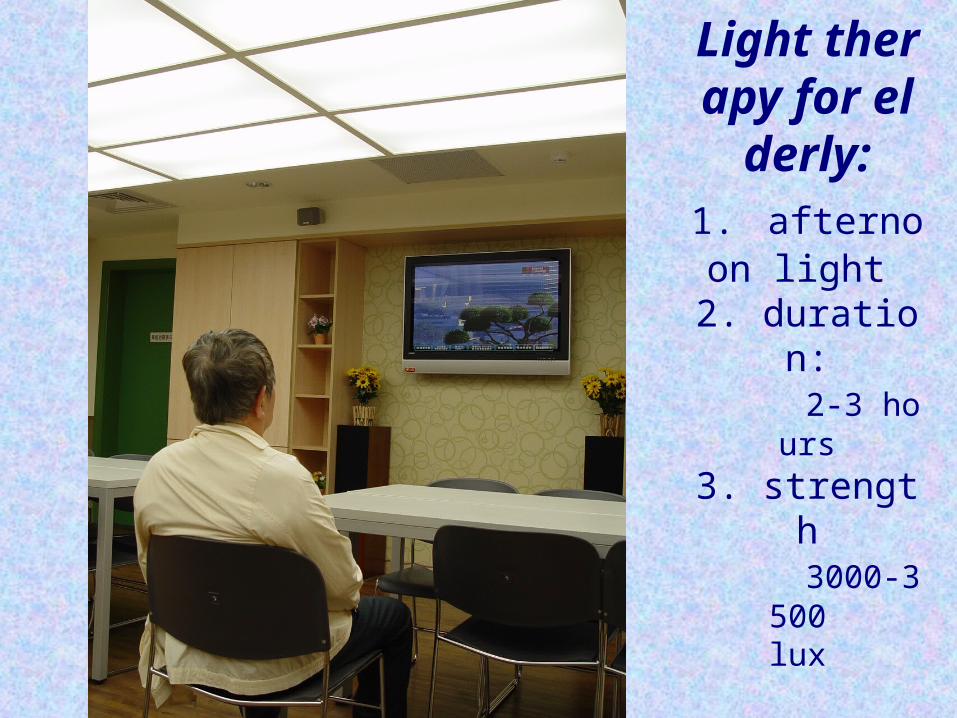
Light therapy for el
derly:1. afternoon li
ght 2. duration: 2-3 hours
3. strength 3000-3500
lux
Perpetuating Factors• Behavioral
– Irregular sleep-wake schedule– Excessive time in bed– Sleep-incompatible activities – Excessive caffeine use, stimulating activities close to
bedtime – Clock watching during the night
• Cognitive– Worry about sleep – Fear of not sleeping– Irrational beliefs concerning consequences of poor sleep
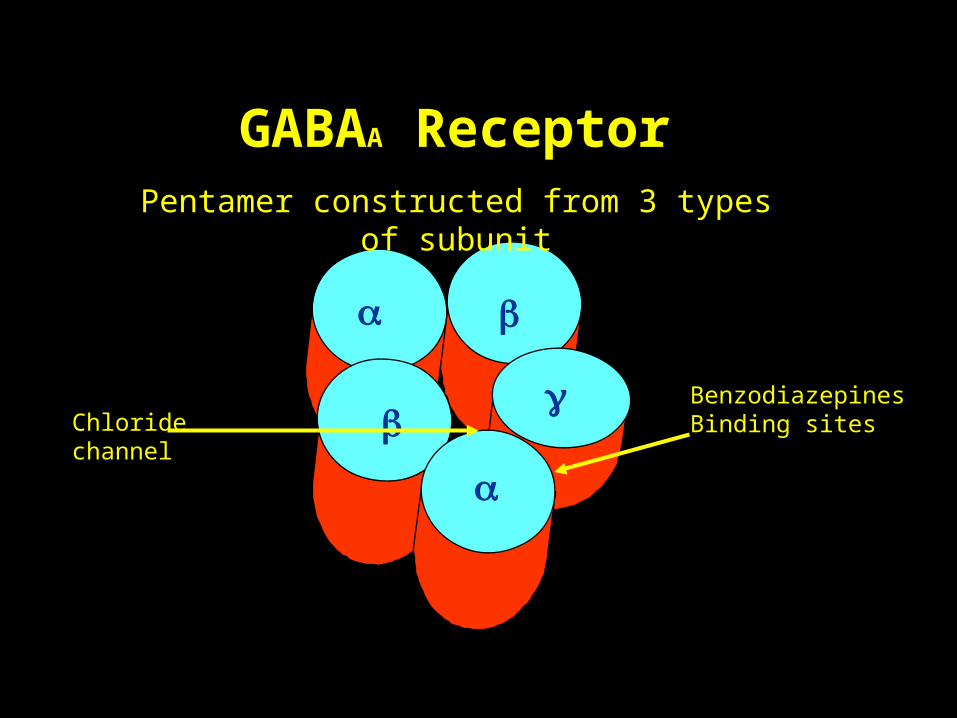
BenzodiazepinesBinding sitesChloride
channel
Pentamer constructed from 3 types of subunit
GABAA Receptor
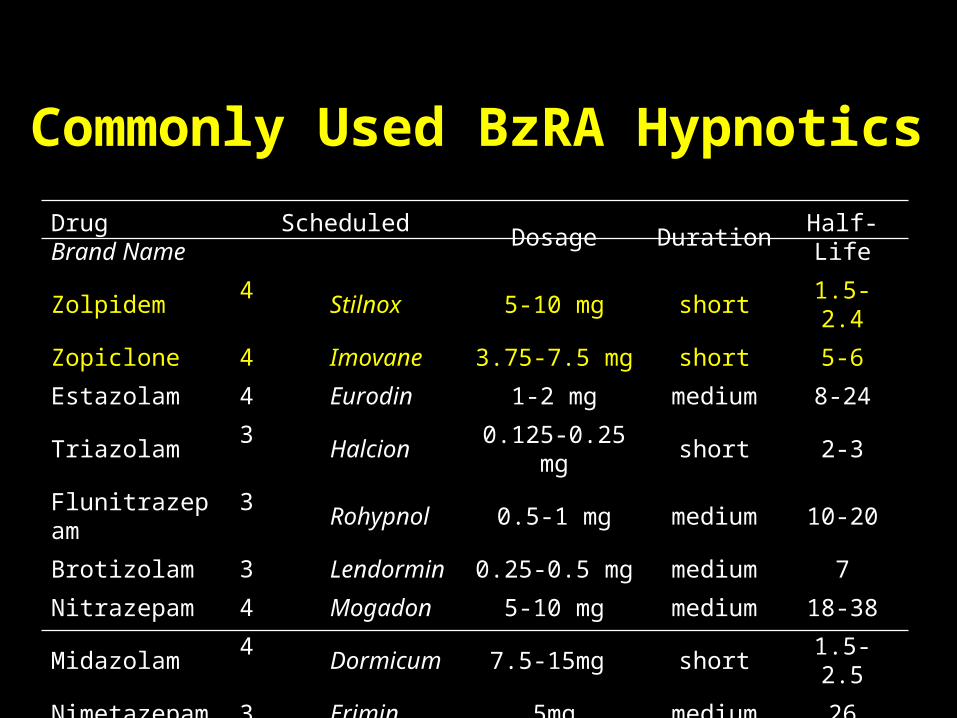
Commonly Used BzRA HypnoticsCommonly Used BzRA Hypnotics
Drug Scheduled Brand Name Dosage Duration Half-Life
Zolpidem 4 Stilnox 5-10 mg short 1.5-2.4
Zopiclone 4 Imovane 3.75-7.5 mg short 5-6
Estazolam 4 Eurodin 1-2 mg medium 8-24
Triazolam 3 Halcion 0.125-0.25 mg short 2-3
Flunitrazepam 3 Rohypnol 0.5-1 mg medium 10-20
Brotizolam 3 Lendormin 0.25-0.5 mg medium 7
Nitrazepam 4 Mogadon 5-10 mg medium 18-38
Midazolam 4 Dormicum 7.5-15mg short 1.5-2.5
Nimetazepam 3 Erimin 5mg medium 26
Flurazepam 4 Dalmadorm 15-30 mg long 40-100
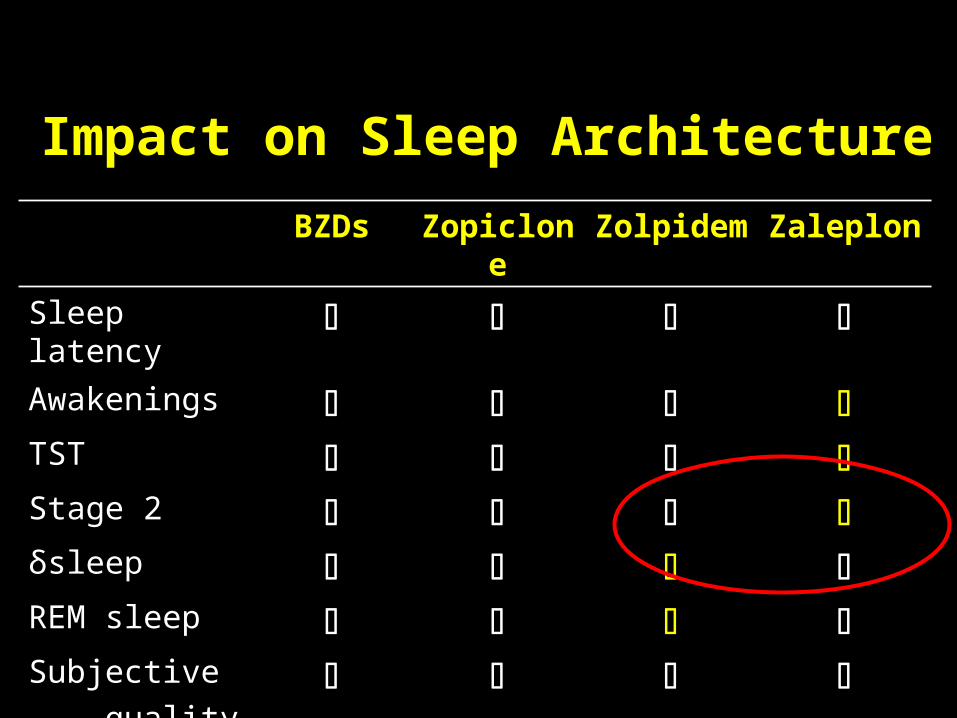
BZDs Zopiclone Zolpidem Zaleplon
Sleep latency Awakenings TST Stage 2 δsleep REM sleep Subjective
quality
Impact on Sleep Architecture
Adverse effect of BzRA
• Adverse effects:– Daytime sleepiness (reaction time, recall, vigilance)– Risk of falls & hip fractures in the elderly– MVA rate increased– But did not show elevated mortality risk (cancer coh
ort)
• Discontinuation phenomena– Rebound phenomenon– Withdrawal: 40-100% with chronic use– Recurrence of insomnia – Abuse of BzRA---uncommon
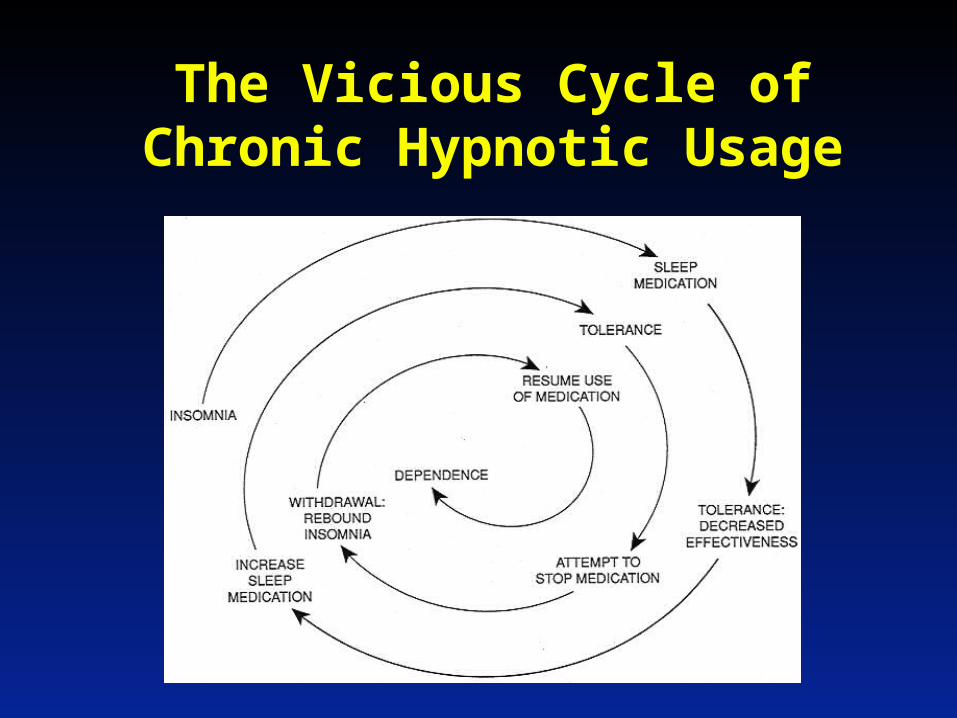
The Vicious Cycle of Chronic Hypnotic Usage
如何好好睡眠1. 認識睡眠2. 了解睡眠3. 把握好睡眠要訣4. 減少導致失眠之外在因素5. 如何放鬆自己、減少壓力6. 了解安眠劑之使用概況 (1) 以最少、最有效之劑量 (2) 必要時使用 (as needed use) (3) 不完全排斥藥物,然而要掌控藥物,不能讓藥物控制你7. 如有長期治療困難之失眠時,要尋找如何與失眠共處相
互生存8. 光線治療之重要性
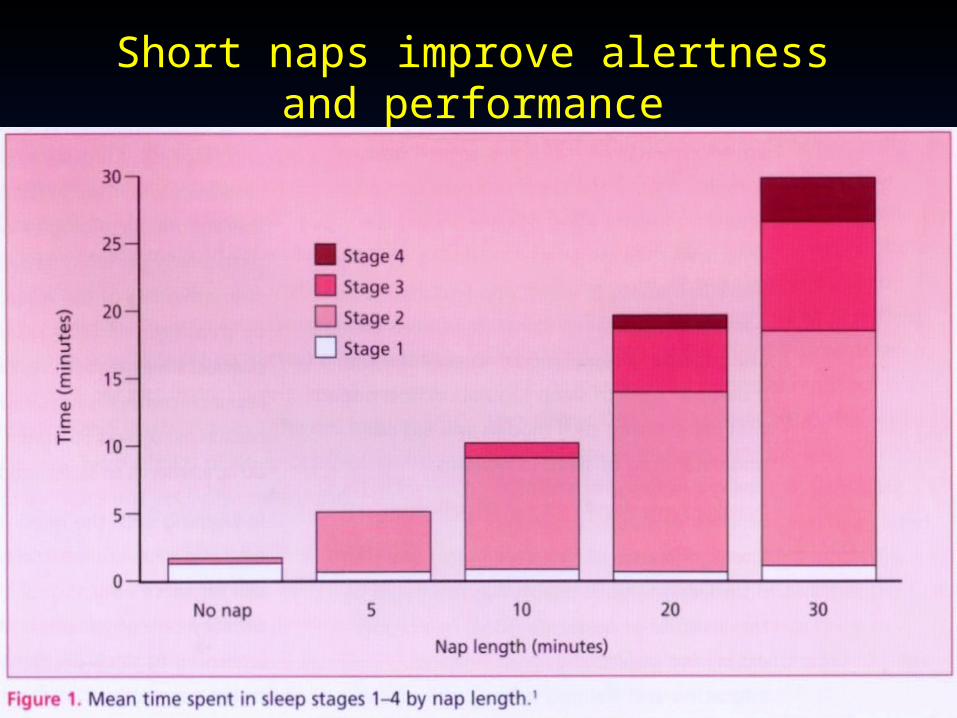
Short naps improve alertness and performance

Thanks forYour Attention
Pre-Sleep arousal Scale• 心跳加速、猛烈或不規則
• 身體內有緊張不安的感覺• 覺得呼吸短促費力• 肌肉繃緊或緊張• 手、腳或其他全身各處覺
得寒冷• 胃部不適 ( 如胃部糾結、胸
口灼熱、噁心等 )
• 手心或身體其他部位冒汗• 口舌喉嚨乾燥
• 會擔心能否入睡• 回想或去考量白天的事情• 有沮喪和焦慮的意念• 會擔心睡眠以外的問題• 神智處於清醒活躍狀態• 無法關閉自己的思維• 念頭持續穿過腦海• 被周遭的聲響、噪音所分心
( 如鐘錶聲、屋內的響動、車聲等 )

Assessment
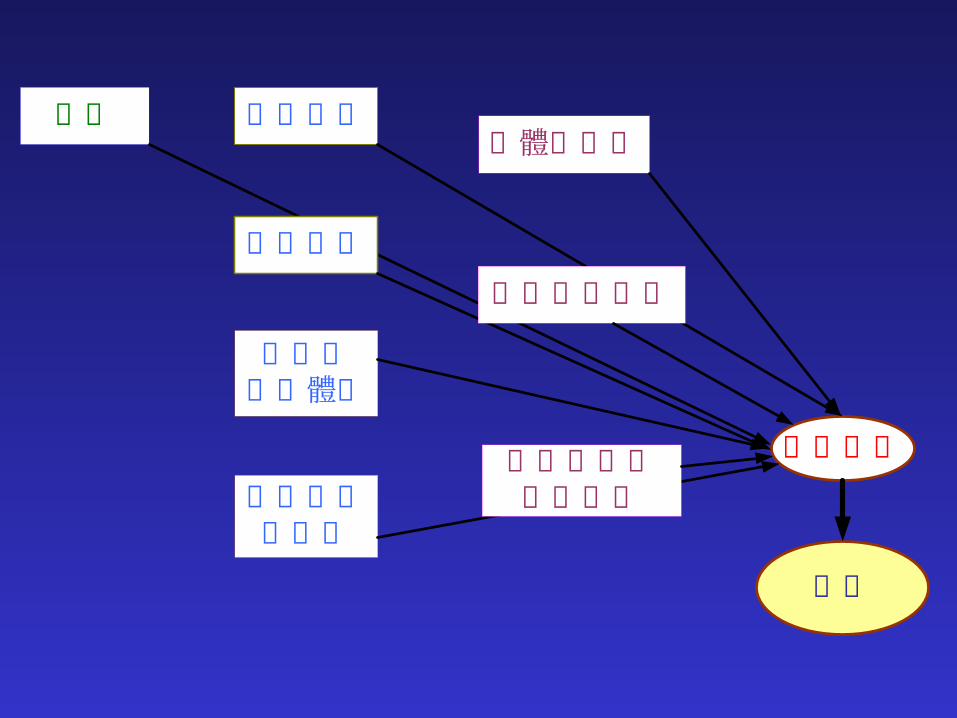
年紀
醒覺干擾
失眠
身體的疾病
生理時鐘的因素
敏感的失眠體質
藥物作用
急性壓力
精神上的疾病
環境或行為上的因素
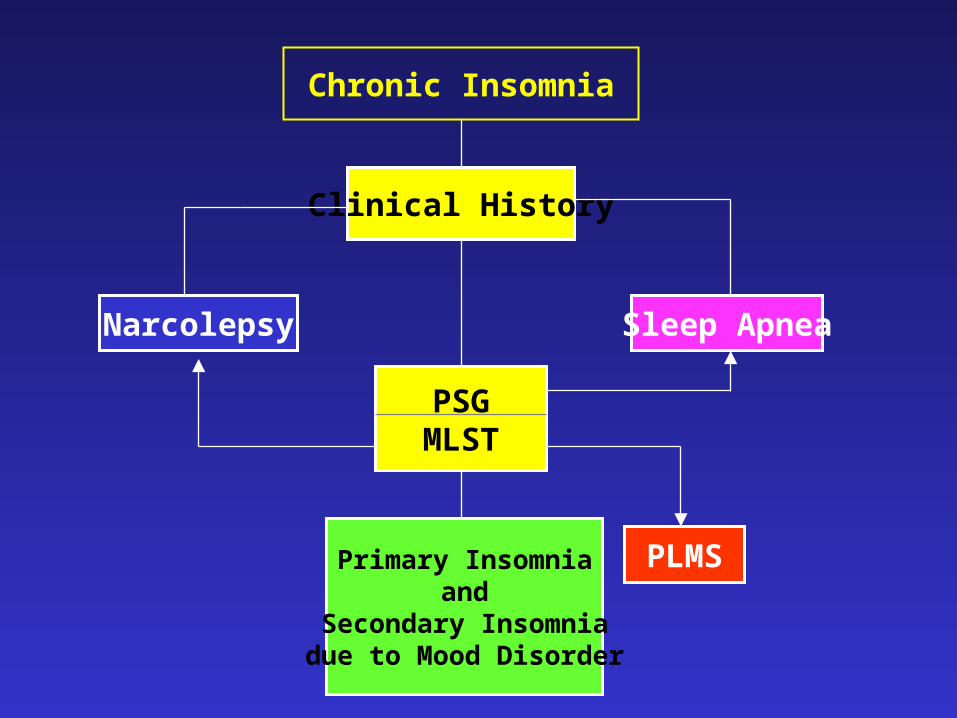
Chronic Insomnia
Clinical History
Sleep ApneaNarcolepsy
PSGMLST
PLMSPrimary Insomniaand
Secondary Insomniadue to Mood Disorder
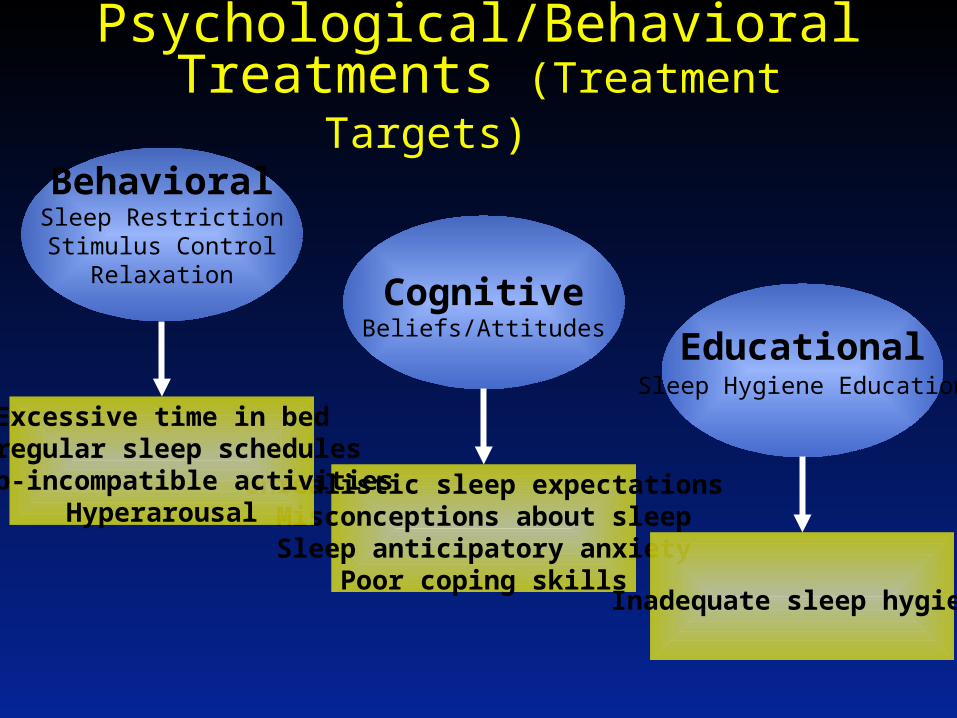
Psychological/Behavioral Treatments (Treatment Targets)
CognitiveBeliefs/Attitudes
Unrealistic sleep expectationsMisconceptions about sleepSleep anticipatory anxiety
Poor coping skills
BehavioralSleep RestrictionStimulus Control
Relaxation
Excessive time in bedIrregular sleep schedules
Sleep-incompatible activitiesHyperarousal
EducationalSleep Hygiene Education
Inadequate sleep hygiene



![Activity;7?actigraph.sakura.ne.jp/blog/wp-content/uploads/2012/01/...[1] 睡眠 ウォッチマン 2014年5月発売 日々の活動に必要な貴方の 必要な固有の睡眠時間測定に](https://img.pdfslide.us/doc/110x75/5f06a1ca7e708231d418f526/activity7-1-ccoe-fffff-20145oec-ee.jpg)

![Cortex-M0+ )和深度睡眠( 的功耗模式分为 ... · • 可选择性地保持外部参考时钟使能—osc_cr[erefsten]。 • 将在进入vlps 模式时的相同mcg 模式下退出vlps](https://img.pdfslide.us/doc/110x75/5f0a8ce27e708231d42c2f6c/cortex-m0-ioeccoei-ce-a-eoeoeefefeefaosccrerefsten.jpg)