Embed Size (px)
Citation preview

Extra oral examination 1
رابعة حديث
Semester 7

The extra oral examination By
Dr. Mohamed Abd-Elmoniem prof. Oral medicine ,
periodontology and oral diagnosis
Vice dean faculty of dentistry Minia University

•Patient examination is a systematic, detailed, anatomic &functional evaluation of the
patient. It does not require any complex technical devices &is mostly carried out by inspection &palpation. It includes:-

Stages of Clinical Examination
Stage 1 Overall assessment of the patient.
Stage2 Recording of vital signs.
Stage 3 Extra oral examination of head and neck
Stage 4 Intra oral examination of soft tissues and
teeth
General requirements of good examination:
1- Examination must be carried out in the dental clinic.
2- The patient must be seated on dental chair where the trunk, head and neck are at one line in an upright position.
3- If it possible, it will be helpful to have an assistant to record the findings.
4- Adequate light must be present.

Stage 1:-
overall assessment of the patient
(General appraisal of the patient) It is the impression concerning the patients health status that
can be gained by inspection from a comfortable distance.
The general appraisal usually starts while the patient is
entering the clinic or while he is standing or walking or
during the diagnostic interview.. It is performed casually
without stopping the patient by observing his gait, stature
, bodyweight….etc.

Overall assessment comprises the assessment of the following:-
1- patient age and gender.
2- Psychological assessment of the patient.
3- The physical constitution of the patient.

1- Patient age and gender:-
Old patients may suffer from atherosclerosis or cardiovascular diseases.
2- Psychological assessment of the patient:-
Patients may be afraid from
having severe disease,
infectious disease or
afraid from losing his teeth
The dentist must eliminate the fear of the patient and assure him.

3- The physical constitution of the patient:-
A- Patient stature.
B- Patient habitués.
C- The gait of the patient.
D- Patient tremors.
E- Weight of the patient.
F- patient behavior.
G- patient speech.
H- Skull and cranium.
I- Face and facial
expression.
J- Facial asymmetry.


i- Smaller stature or dwarfism a- Achondroplastic dwarf:
Defect in endochondral bone (membranous bone are normal).
Retruded maxilla ( growth base of the skull).
Mandibular prognathism.
Malocclusion.
Congenital absence of teeth.
b- Pituitary dwarf:-
Hypopituitarism.
All parts of the body are short and proportionate.
Small mandible and maxilla leads to teeth crowding.
Delayed eruption and shedding of teeth

i- Smaller stature or dwarfism c- Cretin dwarf:
Congenital hypothyroidism.
Over developed maxilla..
Under developed Mandible.
Retraction of the bridge of the nose ( growth base of the skull).
Delayed eruption and delayed shedding of the teeth.
Tongue is enlarged by edema leading to malocclusion.
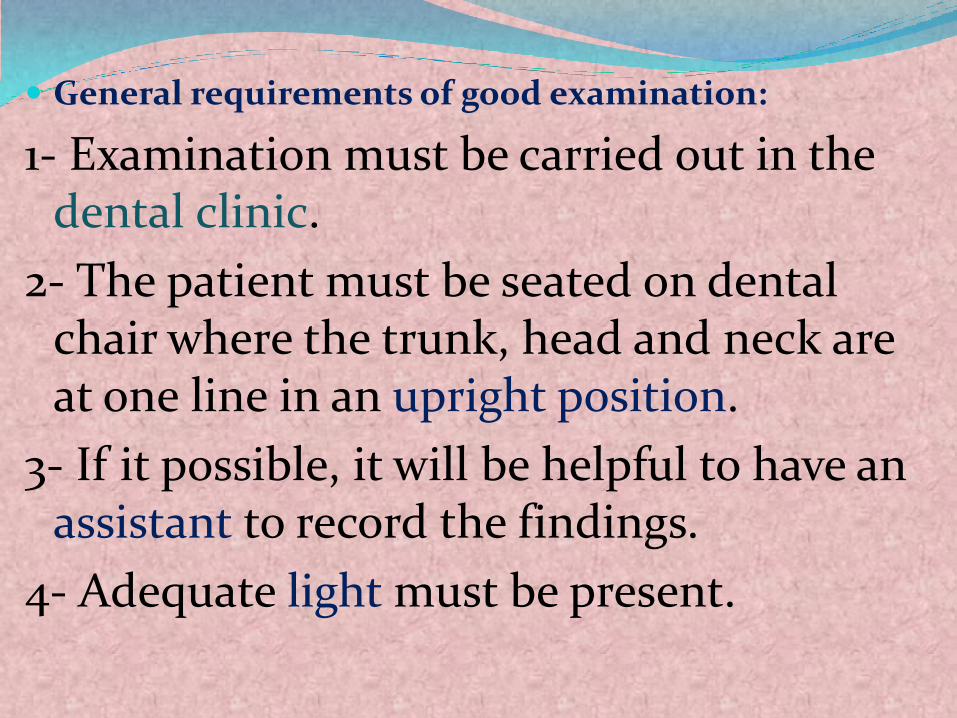
ii- Large stature a- Gigantism:-
Caused by hyperpitutarism.
Teeth are proportional to the size of the jaw.
Roots may be longer.
The body parts are proportionate but huge.
b- Acromegaly:- Hyperpitutarism in adults
Large hands, feet, malar bone, tongue, lip.
Large mandible.
Teeth spacing and root hypercementosis.
Difficulty in teeth extraction.

3- The physical constitution of the patient:-
A- Patient stature.
B- Patient habitues.
C- The gait of the patient.
D- Patient tremors.
E- Weight of the patient.
F- patient behavior.
G- patient speech.
H- Skull and cranium.
I- Face and facial expression.
J- Facial assymmetry.

B-Physical structure( habitués or body type):-
Sthenic bulky, muscular, strong individual with
short neck.
-

Asthenic tall, slender or
slim, under weight.

Hypersthenic or atheletic
heavy bone
&thick muscular proportions.
-

Obesity great fat tissues.
-Pyknic heavy, soft
& rounded due to excess body fat.

Cachexic decreased tissue mass resulting from malnutrition or debilitating disease, markedly weak person.

3- The physical constitution of the patient:-
A- Patient stature.
B- Patient habitues.
C- The gait of the patient.
D- Patient tremors.
E- Weight of the patient.
F- patient behavior.
G- patient speech.
H- Skull and cranium.
I- Face and facial expression.
J- Facial assymmetry.

C- Patient Gait Way of walking.
Altered by disorders or psychomotor problems which may affect the diagnosis and treatment plan.
Types of gaits:-

1- Circumduction gait (semicrcular lateral swing)
as in hemiplagia.

2- Ataxic gait
(irregular wide distanced, the patient tend to watch his feet) in alcoholic intoxication, tabes dorsalis and cerebral dysfunction

3- Scissors gait:- short steps,
one foot crosses over in front
of the other.

4- Hemiplagic gait:- semicrcular lateral swing of the affected leg
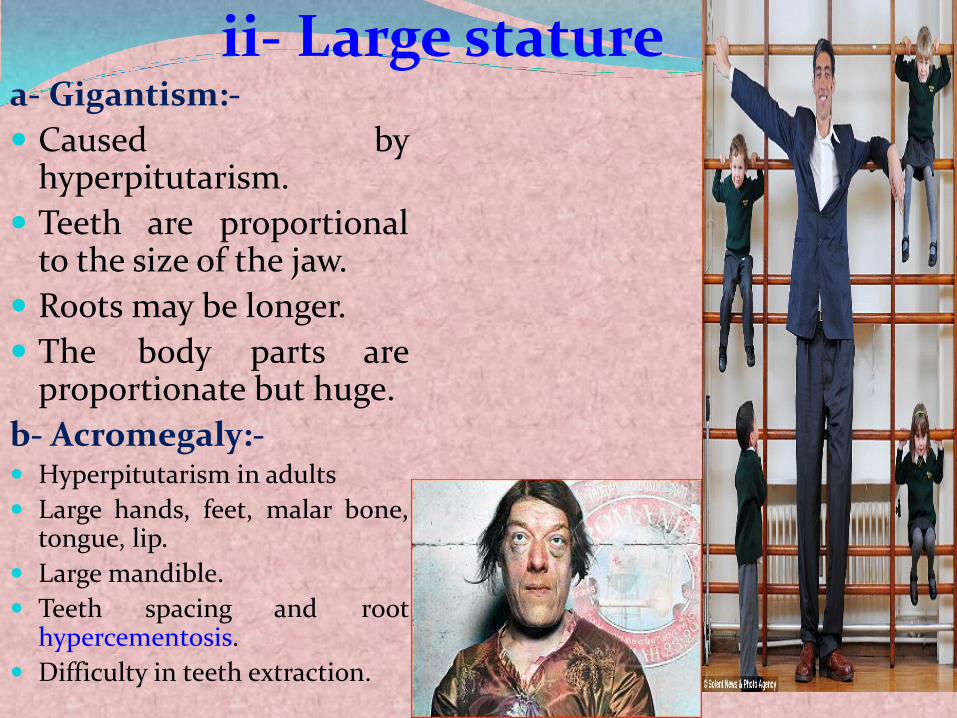
5- Parkinsonian gait:- hanging arms and rapid steps

D- Patient tremors
Movements of the patient extremities should be noted as it may indicate the
presence of systemic disease;
Movement of the thumb and index in a rolling movement characteristic of
parkinsonsm.
Tremors occurs with hyperthyroidism.
E-Body weight:-
The patient's weight in relation to height is called (body mass index).
Either gain or loss in weight should be recorded.
Obesity is associated with abnormal function of the thyroid or pituitary
glands.
Rapid loss of weight is suggestive of malignancy, hormonal or metabolic
dysfunction as, hyperthyroidism, diabetes M or chemotherapy.

F-Behavior and mental orientation:-
Patient behavior may be :-
Nervous, lazy. Alert, fearful or distressed.
Mental orientation:-
Is assessed on the basis of the patient's awareness of
identity,
place
&time.
G-Speech
normal speech implies
healthy function of the organs that produce the sound,
coherent mental status
&the ability to hear.

3- The physical constitution of the patient:-
A- Patient stature.
B- Patient habitues.
C- The gait of the patient.
D- Patient tremors.
E- Weight of the patient.
F- patient behavior.
G- patient speech.
H- Skull and cranium.
I- Face and facial expression.
J- Facial assymmetry.

H- Skull or cranium
a- Size small skull(microcephalus) may be due to brain hypoxia due to
developmental anomaly
or early brain damage by anoxia,
trauma, infection or radiation
Large head(macrocephalus) -Paget disease (frequent remodeling)
-Hydrocephalus( cerebrospinal fluid)
-Acromegalic( growth hormone)
-Achondroplasia(large head in contrast to body)
Failure of the fontanels to close at the proper time
The two conditions are accompanied with low intellectual development and convulsions.

b. Skull Shape 1- Prenatal or congenital syphilis
The frontal bones are prominent, the height& breadth of forehead are exaggerated.
2- Hydrocephalus:- It is abnormal accumulation of fluid in the
cranial cavity. Caused by excessive production or failure of
absorption of the fluid by arachnoid villi. 3- Achondroplasia:- due to defective endochondral ossification,
the head appears large in contrast to the body.
4- Rickets:- the skull is boxy due to prominence of the
frontal eminencies and the posterior parietal areas.
5- Paget’s disease and osteopetrosis:- Causes enlargement of the skull.





![تفسیر سورۃ الفاتحۃ - books-library.online · ، ص هعماج في يذمترل هجرخو ؛ ] [ مقر ثيدح ،ةعكر لك في ةتحافل¦ ... کر ھپڑ](https://img.pdfslide.us/doc/110x75/5fc59e00cb05983c804783b8/oe-f-f-books-oe-.jpg)