Embed Size (px)
Citation preview
--
Introduction To PumpingIntroduction To PumpingStart For SuccessStart For Success
Children With Diabetes – Orlando – July 24, 2008Children With Diabetes – Orlando – July 24, 2008John Walsh, PA, CDEJohn Walsh, PA, CDE
Advanced Metabolic Care Advanced Metabolic Care + Research + Research
700 West El Norte Pkwy 700 West El Norte Pkwy
Escondido, CA 92126Escondido, CA 92126
(760) 743-1431 (760) 743-1431
The Diabetes Mall The Diabetes Mall
(619) 497-0900(619) 497-0900
[email protected]@diabetesnet.com

Highlights
• Reasons To Use A Pump
• Who’s A Candidate?
• Pump Basics
• Brands And Features
• Infusion Set Tips
• Pump Start Tips
• Pump Settings
• Wrap Up
--
Reasons To Consider A Pump

Better Control –> Fewer Complications
•55.0
29.8
•23.9
•5.1
•13.413.0
7.9
16.4
5.02.50
10
20
30
40
50
60
RetinopathyProgression1
Laser Rx1 Micro-albuminuria2
Albuminuria2 ClinicalNeuropathy3
Conventional
Intensive
76%76%Risk ReductionRisk Reduction
59%59%Risk ReductionRisk Reduction
39%39%Risk ReductionRisk Reduction
54%54%Risk ReductionRisk Reduction
64%64%Risk ReductionRisk Reduction
Cu
mu
lati
ve In
cid
ence
(%
)
1. DCCT Research Group, Ophthalmology. 1995;102:647-661
2. DCCT Research Group, Kidney Int. 1995;47:1703-1720
3. DCCT Research Group. Ann Intern Med. 1995;122:561-568.

Surprise Findings From EDIC Study
Lower Glucose Reduces Heart Attacks & Nerve Damage
After DCCT ended in 1993, the EDIC study followed participants.
In 12 year followup, A1c levels in intensive and conventional control groups have been nearly identical at 7.9% (was 7.4% and 9.1%).
Heart attacks and strokes have been twice as high (98 vs 46) in original conventional compared to intensive group, even though A1c levels were identical since the DCCT trial ended.
The tight control group also had 51% less neuropathy.
• Take Home: Improve control and always aim for normal on your next reading
1. EDIC Study Group presentation at 2005 ADA, K.M. Venkat Narayan: Clinical Diabetes 24:88-89, 20062. Diabetes Care, Vol 29, No. 2, pp. 340-344
Avg A1c = 7.9%

The Challenge Of DiabetesBringing the A1c down smoothly takes effort
……for this you need ADVANCED therapyfor this you need ADVANCED therapy
100 (5.5)
200 (11.1)
300 (16.7)
Normal A1C 4%–6%
BG
in
mg
/dL (
mm
ol)
0800 1200 1800 0800
Uncontrolled A1C ~9%
A1C ~6%
“Controlled” A1C <7%
Time of Day

Exposure And Variability
40
60
80
100
120
140
160
180
200
220
240
260
280
300
320
340
360
380
400
2:00 PM 3:00 PM 4:00 PM 5:00 PM 6:00 PM 7:00 PM 8:00 PM 9:00 PM 10:00
PM
11:00 PM 12:00
AM
1:00 AM 2:00 AM 3:00 AM 4:00 AM 5:00 AM 6:00 AM 7:00 AM 8:00 AM 9:00 AM 10:00
AM
11:00
AM
12:00
PM
1:00 PM 2:00 PM
glucose (mg/dl)
One day – BG checks every 30-60 min.
Exposure or Average =
Variability or Swing =
A1c or avg. BG from meter
Standard deviation or GlycoMark test

Glucose Goals Not Met HbA1c
10%
9%
8%
7%
6%
ADA
EASD/AACE
ADA = American Diabetes Assoc., IDF = Inter. Diabetes Federation, EASD is European Assoc. for the Study of Diabetes, AACE = American Association of Clinical Endocrinologists
Novo Nordisk Type 2 diabetes market research, Roper StarchWright A., Burden et al, Diabetes Care 2002; 25:330–336Turner RC, Cull et al, JAMA 1999; 281:2005–2012
2/3 with diabetes including most pumpers remain in poor control Avg. A1c in
TYPE 1sAvg. A1c on Pumps
Goal
5%

Talk The Talk
• TDD – total daily dose of insulin (all basals and boluses)
• Basal –background insulin released slowly through the day
• Bolus – a quick release of insulin Carb bolus – covers carbs Correction bolus – lowers high readings
• Bolus On Board (BOB) – bolus insulin still active from recent boluses
• Duration of Insulin Action (DIA) – time that a bolus will lower BG – used to measure BOB
--
Who Is A Pump Candidate?

Advantages
• More reliable insulin action, better control, lower TDD
• Precise basal delivery – 0.05 u compared to 0.5 u
• Automatic dose calculations with accurate boluses
• Avoids common problem of insulin stacking
• Fewer missed/skipped doses

People Choose Pumps For
• Convenience
• Better lifestyle
• Less hypoglycemia
• Improved sense of well being
• Flexible insulin delivery – exercise, skipping meals
• Less hassle and anxiety with erratic schedule, shiftwork, travel, time zones

Poor control, high A1c, wide BG excursions
Nocturnal or frequent lows, hypo unawareness
Frequent hospitalization/DKA
Increased insulin sensitivity
Varied or intense exercise/activity
Dawn phenomenon, gastroparesis, pregnancy
Varied work or school schedule, travel
Insulin resistance, Type 2 diabetes
Physicians Recommend Pumps For

Requirements
• Realistic expectations
• Willing to check BG 4 or more times a day and keep records
• Count carbs or quantify food intake
• Able to solve problems
• Willing to adjust basals and boluses
• Keep clinic visits for follow up

Expectations
Unrealistic Realistic
The pump will cure my diabetes I will feel better
I won’t have to test as much I must monitor frequently
I can eat anything I want I will have more freedom with my food choices
My blood sugar will be perfect I will have better control with fewer lows
It will be as easy to learn as a meter
It will take time to learn and adjust to the pump
Infants & Toddlers
• Little ones are ideal pump candidates
• Able to delay or split boluses for fussy eaters
• Fast insulin change for erratic activity
• Precise doses – 0.025 basal and 0.05 bolus – assists infants who cannot convey hypoglycemia symptoms and have frequent illnesses
Back Buddy
Place between shoulder blades and use lock-out to avoid self dosing

Kids & Teens
• Better for growth spurts, hormone changes in puberty, Dawn Phenomenon
• Easy to cover snacks
• TDD and bolus history available to ensure consistent dosing
• Fast adjustments of basals and boluses for activity and exercise
• Lessens impact of BG swings on top of peer pressure, struggle for independence, mood swings, college, and issues with alcohol, sex, drugs

A pump’s basals and boluses provide a better match
Bolus
Flexible basal from pump
Basals And Boluses From Pump
Flat basal from Lantus or Levemir

Basals And Boluses
A pump’s basal delivery provides a better match for life’s needs
Temp basal reductionfor exercise

4
5
6
7
8
9
10
11
12
0 2 4 6 8 10 12 14SMBG Frequency (BG per day)
HbA1c
HbA1c=5.99+5.32 / (BGpd+1.39)
Atlanta Diabetes Associates study:378 patients sorted from a database of 591 Pumps=MM 511 or earlierBG Target=100C peptide <0.1
ADA:< 7%% AACE:
< 6.5%
P. Davidson et al: Diabetes 53 (suppl 2): abstract 430-P, 2004
Checking/Monitoring Still Required

--
Brands And Features

Things To Consider
• Look, feel, color, wearability
• Reminders, child block, waterproofing
• Basal and bolus increments
• Infusion set options
• Customer support
• History, ease of data download and analysis
• Meter and CGM integration, remote bolusing, covers, cases, PDA, smart phone

Insulin Pumps – 2008
• Accu-Chek Spirit
• Animas 2020
• Deltec CozMore 1800
• Insulet Omnipod
• Medtronic Paradigm x22
• Sooil Dana Diabecare IIS
Pump info at www.diabetesnet.com/diabetes_technology/

Accu-Chek Spirit
• Boluses based on BG, not BOB
• Strong motor and delivery +
• 300 units
• 0.1 u basal & bolus increments
• Reversible display +
• Side-mounted tactile buttons
• Accu-Chek Pump Configuration Software with fast download
• IR (direct line) control from optional Palm PDA or smart phone
• Database of 1,000 Calorie King foods in PDA

Animas 2020
• High contrast color screen +
• Smallest mainstream pump +
• Smallest basal increment – 0.025 u – great for kids +
• 200 units
• Waterproof – 12 ft for 24 hrs
• ezCarb meal bolus calculator
• ezBG correction bolus calculator
• ezBolus shortcut to give bolus
• Carb/food database in pump
Dexcom

Lifescan Ping
Dexcom
• One Touch meter with direct BG entry into new Animas pump
• Bolus delivery directly from meter

Deltec Cozmo
• Most features: +
HypoManager, Weekly Schedule, Missed Meal Bolus, Disconnect Bolus, Basal Test, Therapy Effectiveness
• Most setup options +
• Direct BG entry from Freestyle +
• Accurate bolus calculations +
• 300 units
• 0.05 unit basal & bolus increments
• Easy and accurate BOB access +
• CozFoods Meal Maker carb database
Navigator

Special Features
Feature: Pumps
Cont Monitor readout Paradigm
No tether Omnipod
Lowest basal rate Animas
HypoManager Cozmo
Weekly Schedule Cozmo
Missed Meal Bolus Cozmo
Bolus Not Completed Cozmo
Disconnect Bolus Cozmo
Food/Carb List Animas, CozmoOmnipod,
Spirit
Therapy Effectiveness Cozmo, Paradigm
Glucose SD (Variability) Cozmo

Insulet Omnipod
• No tubing, easy wear +
• Fewer infusion set problems +
• Automatic cannula insertion and priming +
• Remote bolusing from controller or smart phone +
• Direct BG entry from Freestyle +
• 200 units
• Limited to 72hrs (+8 hrs basal)
• Watertight
• 1000 food database
• Smaller startup, larger overall cost
DexcomNavigator

Medtronic Paradigm
• Built-in CGM display eliminates one device +
• Simple
• Direct BG entry from One Touch meter +
• Proprietary infusion sets
• History via CareLink online software +
• 176 or 300 unitsParadigm RT

Continuous Monitor Benefits
• Increased sense of security
• Immediate feedback – look and learn
• Trend lines help adjust basals and boluses
• Improves control
• Worth out of pocket cost for many
• Insurance reimbursement gradually catching on

Trends Versus Stasis
CGM reading shows the wearer only a few carbs may be needed. Meter reading gives no clue.

CGM Look And Learn
Excess night basal or bedtime bolus
Breakfast bolus too small or too late
Lunch bolus too small or afternoon basal too low

CGM–Pump Combos
Animas
Cosmo
Omnipod
Medtronic
Dexcom
Navigator
Paradigm RT

Only Pumps Track BOB
CDA1 StudyOf 201,538 boluses,
64.8% were given within 4.5 hours of a previous bolus
This means BOB is present in nearly 2 out of every 3 boluses
Time between boluses in hrs
J. Walsh, D. Wroblewski, and TS Bailey: Disparate Bolus Recommendations In Insulin Pump Therapy. AACE Meeting poster, 2007, www.diabetesnet.com/pdfs/AACE2007Poster.pdf

BOB Helps Prevent Lows
• Better bolus accuracy
• Less insulin stacking as BOB is tracked after each bolus
• A BG check reveals the current carb or insulin deficit
• Faster reduction of insulin for exercise
• Smaller pool of insulin under skin lessens risk of a large release in hot tub or weather
• More predictable insulin action

Helpful Reminders
Reminders (alarms) to
Check BG after a bolus
Check BG after a low reading
Check BG after a high reading
Warn when bolus delivery was not completed *
Warn when bolus not given at designated time of day *
Change infusion site
Warn of low reservoir (20, 10, 5 and 0 units) (Extra 10 “hidden” units for basal delivery in Cozmo and Omnipod)
* Cozmo 1800

Infusion Sets
#1 cause for “unexplained” highs
and pump problems

Infusion Sets And Inserters
Rapid-D/ContactRapid-D/Contact
Animas InsetAnimas Inset MM Quik-serterMM Quik-serter
Comfort/Silhouette/TenderComfort/Silhouette/Tender
Deltec CleoDeltec Cleo
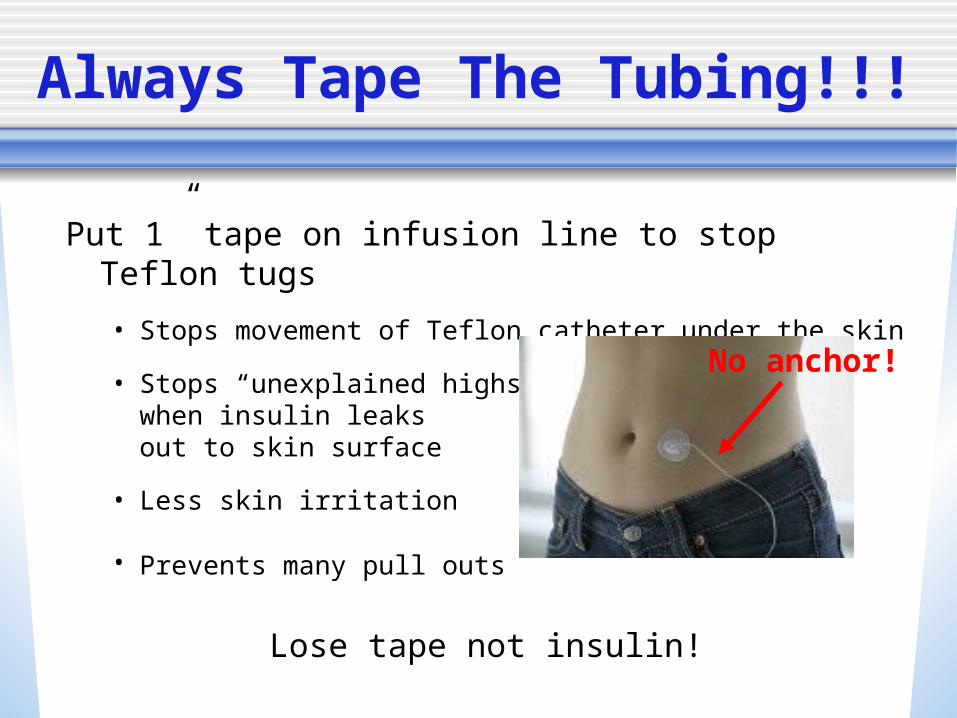
Always Tape The Tubing!!!
Put 1” tape on infusion line to stop Teflon tugs
• Stops movement of Teflon catheter under the skin
• Stops “unexplained highs” when insulin leaksout to skin surface
• Less skin irritation
• Prevents many pull outs
Lose tape not insulin!
No anchor!

Lose Tape Not Insulin!!!
Most insulin is lost when the Teflon comes loose, not from a complete pullout
Photo courtesy of [email protected]

Tapes
Some 1” tapes that work well Micropore
Durapore
Hypafix
Blenderm

Tackies
Toupee glue Skin-Tac Mastisol
Remove with Goo B Gone or Detechol

Use Sterile Technique For Site Prep
Methicillin-resistant staph aureas (MRSA) is now common.
PREVENT infection:
• Wash your hands
• Sterilize skin with IV Prep
• Place bio-occlusive IV3000 over site
• Insert infusion set through IV 3000
Extra steps for staph carriers: • Use antiseptic soap all over body once every 1-2 weeks
• Periodically, apply bacitracin ointment to inside of nose
30% of people are constant and 25% intermittent staph carriers

--
Pump Start
Preparation
• Use basal/bolus approach first with injections
• Count carbs accurately
• Read Pumping Insulin & manual
• Practice with pump as soon as it arrives
• View DVD as you practice with your pump
• Get training in operation andtroubleshooting

Preparation
• Ask how to discontinue your long-acting insulin
• Determine start-up settings for TDD, basal/bolus balance, carb and correction factors, and DIA
• Get prescriptions for insulin, test strips, IV Prep, IV 3000 dressings, etc.
• Have contacts for MD, CDE, pump company, pump rep, other pumpers

Steps To Success
• Test often
• Keep a record (Smart Charts, download, etc)
• Take a bolus for every bite except for carbs used to treat a low BG
and carbs used to compensate for exercise
• Bolus early
• Write down a reason for each high and low BG
• Change infusion sets on schedule and whenever unexpected highs occur

Steps To Control
• Stop lows first
• Find your optimum TDD
Start basals as half of optimized TDD
Determine starting carb factor with 450 Rule (450/TDD) and correction factor with 2000 Rule (2000/TDD)
• Use a realistic DIA – 4 to 6 hrs
• Periodically check basal/carb bolus balance
• Look for and correct unwanted patterns

Stop Lows FirstBetter control, more stability
• Mild lows cause followup lows
• Small epinephrine release makes muscles sensitive to insulin
• Can lead to another low as much as 36 hours after the first
• More carbs than usual are needed
Severe lows cause highsHigher stress hormone release makes glucose rise for 6-10 hrsExcess carb intake leads to highs Boluses may be reduced/skippedMore insulin than usual needed

A Critical Question
The question “Are lows or highs your main problem?” is not answered correctly by many.
The answer is critical to solving control problems.
Base your answer on BG data and other’s observations, not on your feelings or fears.

Find Your Optimal TDD
Determine your current TDD
1. Lower it:
• For frequent lows
• For highs AND lows – which comes first?
2. Raise it:
• For a high A1c or a high average BG on your meter
3. Keep basal rates and the daily carb bolus total balanced
TDD – too low
or too high?

Raise TDD For High Avg. BG or A1cExample: someone’s TDD = 35 units, few lows, and A1c = 9%.
© Pumping Insulin, 2006© Pumping Insulin, 2006

Change Your TDD For
• Changes in diet
• Loss or gain of weight
• Seasons
• Changes in activity
• Starting/stopping sports
• Vacations
• Growth spurts, puberty
• Menses
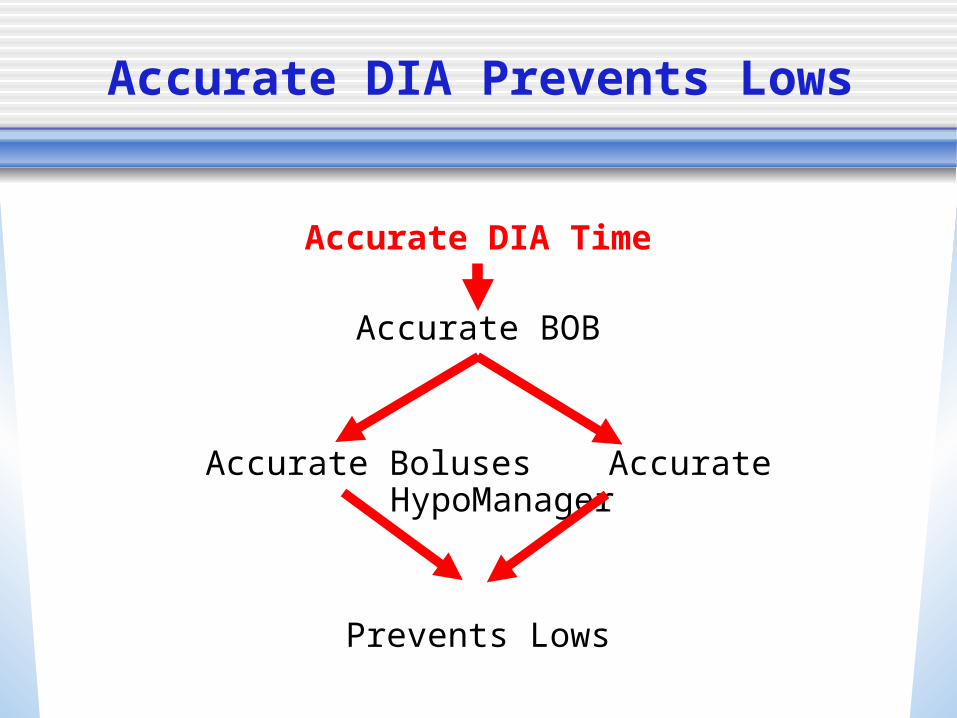
Accurate DIA Prevents Lows
Accurate DIA Time
Accurate BOB
Accurate Boluses Accurate HypoManager
Prevents Lows

Duration Of Insulin Action (DIA)
4 hrs 6 hrs2 hrs0
Accurate boluses require an accurate DIA
Glu
cose
-lowe
ring
Activ
ity
DIA times shorter than 4 to 7 hrs will hide BOB and its glucose lowering activity

More DIA
Large doses (0.3 u/kg = 15 u for 110 lb. person) of “rapid” insulin in 18 non-diabetic, obese people
Med. doses (0.2 u/kg = 10 u for 110 lb. person)
Apidra product handout, Rev. April 2004a
Regular

DIA Tips
• DIA times NOT different between children and adults
• If your pump does not “give enough bolus insulin”, do NOT shorten the DIA to get larger boluses
• Look for the real reason:
a basal rate too low
or a carb factor too high
that makes your DIA SEEM SHORT!

DIA Recommendations
Modified from Mudaliar et al: Diabetes Care, 22:
1501, 1999
DIAs on current pumps can be set from 2 to 8 hours.
An accurate DIA can significantly improve control.

--
Basal RatesShould keep the glucose flat overnight
or when a meal is skipped
Relatively easy to check (don’t eat)
See See Pumping InsulinPumping Insulin for detailsfor details

How Many Basals?
0
5
10
15
20
25
Number of Basals
1 2 3 4 5 6 7 8 9 10
Percentage of pumpers who use 1 to 10 basals per day from self reports of several hundred pumpers at insulin-pumpers.org%
One basal rate may work in children, while the complex metabolism of puberty often requires multiple rates

• 50% Rule: basals usually make up 40 to 65% of an accurate TDD
• Basal rates will be similar through the day, such as between 0.45 and 0.7, or between 1.0 and 1.4
• When basal rates need to change, modify them in small steps – usually 0.05 or 0.1 u/hr
• Change basals 3 to 8 hours before need arises
Basal Tips

Duration Of Carb Action
Most carbs affect the BG only 1 to 2.5 hoursMore delay with complex carbs, more fiber, more fat, etc
0 hrs 1 hr 2 hrs 3 hrs 4 hrs
High GI
Med GI
Low GI
Thanks to Gary Scheiner, MS, CDEThanks to Gary Scheiner, MS, CDE

Most Carbs Faster Than Insulin
Time over which a bolus lowers the BG
From From Pumping InsulinPumping Insulin
Take Home: Bolus 15 to 30 minutes before meals Use extended boluses sparingly.
Meal’s impact on BG
One hour after a meal, half a meal’s glucose rise is gone, but 80% of the “rapid” insulin’s activity remains

Bolus Timing
Figure shows rapid insulin injected 0 min, 30 min, and 60 minutes before a meal
Normal glucose and insulin profiles are shown in the shaded areas

Carb Factor
• Carb factor – how many grams of carb are covered by 1 unit
• Carb boluses determined from:
Your carb factor
How many grams of carbs you plan to eat
Your BG allows a correction bolus determination
Amount of BOB still active determined from BG
• Pump determines the bolus needed for a meal IF the carb count and the carb factor are accurate
Visit your dietician to learn!

How To Find Carb & Correction Factors
Determine starting carb factor with the 450 Rule:
450/TDD = Carb Factor
Check it: Carb Factor X TDD = 450?
Determine starting correction factor with the 2000 Rule:
2000/TDD = Carb Factor
Check it: Correction Factor X TDD = 2000?

20 u 0.42 u/h 22 grams 100 mg/dl
25 u 0.52 u/h 18 grams 80 mg/dl
30 u 0.63 u/h 16 grams 67 mg/dl
35 u 0.73 u/h 13 grams 57 mg/dl
40 u 0.83 u/h 11 grams 50 mg/dl
50 u 1.04 u/h 9 grams 40 mg/dl
60 u 1.25 u/h 7.5 grams 33 mg/dl
80 u 1.67 u/hr 5.6 grams 25 mg/dl
Find Basals And Boluses From TDD
Starting Carb Factor Corr. Factor TDD 50% Basal 450 Rule 2000 Rule
An accurate TDD solves most control problems!
3.1 mmol

Check Your Carb Factor
Check how close you are to the 450 Rule:
Multiply your average TDD for the last 14 days times your carb factor.
Example:
Avg TDD X Carb Factor = Carb Factor Rule Number
30 u/day X 12 = 360 (lower = more aggressive)

Regular Taken immediately –MOST meals
Combo / dual wave Some now, some later –burrito,
some pastas and pizzas, Symlin, precose
Extended / square wave Extended over time – gastroparesis
Carb Boluses

Missed Boluses Lead To High A1cs
• One missed bolus a week raises the A1c almost 0.5%
Prevent missed boluses:
• Give a bolus for every bite!
• Use pump reminders
• Review pump history to increase number of boluses given each week
• Solutions without blame
8.38.48.58.68.78.88.9
99.19.29.39.4
Before 6 mos
Control
+Rmindr
48 youth in poor control (A1c > 8%). All put on a Deltec Cozmo pump, with half using reminders. Significant reduction for reminder at 3 mos but no difference after 6 mos.
H. Peter Chase et al: Diabetes Care 29:1012-1015, 2006

Carb Bolus Tips
• Does your carb factor work for LARGE carb meals, such as for a carb intake = half your weight in lbs?
• Do you count carb accurately?
• Do you give boluses 20 min before meals when your glucose is normal?
For frequent lows after meals –> raise carb factor #
For frequent highs after meals –> lower carb factor #

Check For Patterns
• Frequent highs
• Frequent lows
• High at B/L/D/Bed
• Low at B/L/D/Bed
• Low to high
• High to low
Keep:
• TDDs similar from day to day
• Basals and boluses balanced
• Correction bolus below 8% of TDD
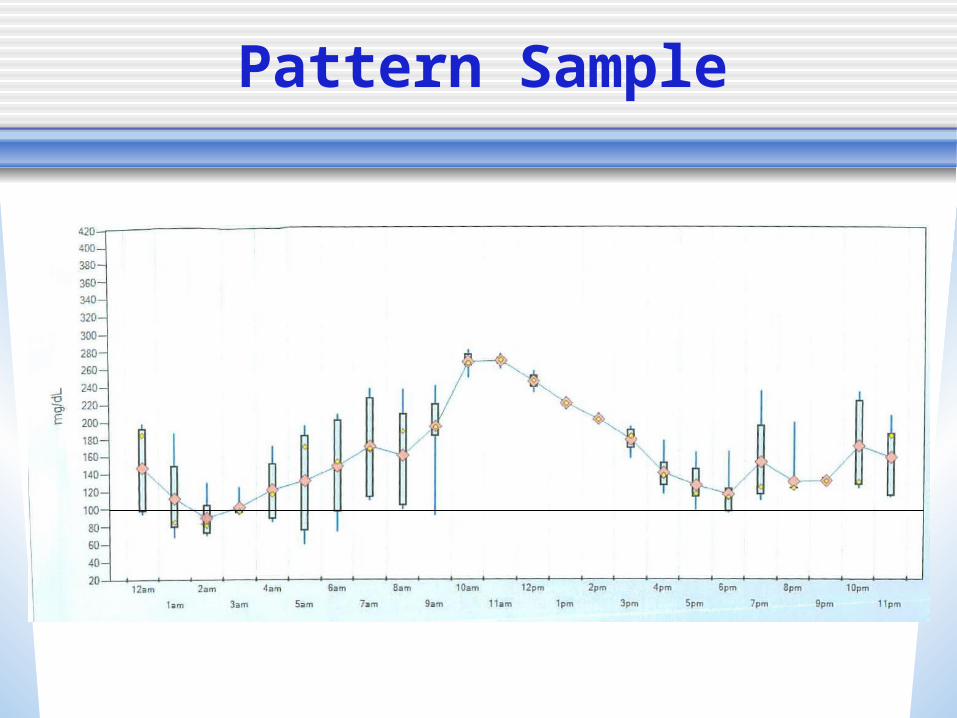
Pattern Sample

Bottom Line
If your smart pump is not giving you great control, check your
pump settings and infusion sets.

High BGs? Keep Usual Suspects In Mind
Bad infusion set or site
Inaccurate carb counts
Missed boluses
Bad insulin
Stress hormone rebound
Empty refrigerator syndrome
Stress, pain, steroid meds
I ate
too much

Wrap Up
• Pumps offer best technology for precise insulin delivery
• A more flexible and healthier life with less hypoglycemia
• Requires commitment, responsibility
• Good training and follow-up requiredfor an effective outcome
• Make the commitment to good health and pump well!

Questions – Discussion