Embed Size (px)
Citation preview
Listen to this manuscript’s
audio summary by
Editor-in-Chief
Dr. Valentin Fuster on
JACC.org.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 3 , N O . 6 , 2 0 1 9
ª 2 0 1 9 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
JACC REVIEW TOPIC OF THE WEEK
Diagnosis and Treatment of Lyme CarditisJACC Review Topic of the Week
Cynthia Yeung, BSC, Adrian Baranchuk, MD
ABSTRACT
ISS
Fro
rel
Ma
The incidence of Lyme disease, a tick-borne bacterial infection, is dramatically increasing in North America. The
diagnosis of Lyme carditis (LC), an early disseminated manifestation of Lyme disease, has important implications for
patient management and preventing further extracutaneous complications. High-degree atrioventricular block is the
most common presentation of LC, and usually resolves with antibiotic therapy. A systematic approach to the diagnosis of
LC in patients with high-degree atrioventricular block will facilitate the identification of this usually transient condition,
thus preventing unnecessary implantation of permanent pacemakers in otherwise healthy young individuals.
(J Am Coll Cardiol 2019;73:717–26) © 2019 by the American College of Cardiology Foundation.
L yme disease (LD), an infection that can mani-fest in a multisystem nature, is gainingincreasing recognition. The causative Gram-
negative spirochete bacteria is acquired from rodenthost reservoirs and transmitted by the hard-bodiedIxodes tick (1). Although the sole bacterial species inNorth America is the Borrelia burgdorferi sensustricto, LD is also caused by B. garinii, B. afzelii, andB. spielmanii (2). During the early disseminated phaseof LD, hematogenous spread and organotropismresult in extracutaneous manifestations includingcardiac, neurological, and joint (2).
Our review focuses on early dissemination Lymecarditis (LC) and its most frequent manifestation,high-degree atrioventricular (AV) block (AVB).
DISEASE BURDEN
EPIDEMIOLOGY OF LD. LD is the most commonlyreported vector-borne disease in North America (3).The United States had 26,203 confirmed cases(incidence ¼ 8.1 cases/100,000 population) and36,429 probable cases of LD reported in 2016 (4);however, estimates suggest that the true incidenceis approximately 300,000 cases annually (5). The
N 0735-1097/$36.00
m the Department of Cardiology, Queen’s University, Kingston, Ontario, C
ationships relevant to the contents of this paper to disclose.
nuscript received October 11, 2018; revised manuscript received Novemb
incidence of reported LD has dramatically increasedin Canada, from 144 cases in 2009 to 2,025 casesin 2017 (6). Risk modeling suggests that the casenumbers will continue to increase rapidly asI. scapularis, carried by migratory birds that areaffected by climate change, invades further into theheavily populated southern parts of Canada (7).
EPIDEMIOLOGY OF LC. The incidence of cardiacinvolvement in LD has historically been as high as10% in earlier studies, but more recent studies havereported lower incidences at 0.3% to 4% (8–11). High-degree AVB is estimated to occur in approximately80% to 90% of LC (11,12). LC is much less common inEurope, which may be explained by different bacte-rial strains and virulence of European and NorthAmerican isolates (8). Myocardial involvement maybe more prevalent in pediatric patients with LD,at approximately 30% with electrocardiographicchanges (13).
LYME CARDITIS
PATHOPHYSIOLOGY OF LC. The pathophysiology ofLC involves the direct myocardial invasion by thebacteria and the subsequent immunologic and
https://doi.org/10.1016/j.jacc.2018.11.035
anada. Both authors have reported that they have no
er 13, 2018, accepted November 26, 2018.
ABBR EV I A T I ON S
AND ACRONYMS
AV = atrioventricular
AVB = atrioventricular block
CLD = chronic Lyme disease
DCM = dilated cardiomyopathy
IV = intravenous
LC = Lyme carditis
LD = Lyme disease
PTLDS = post-treatment Lyme
disease syndrome
SILC = Suspicious Index in
Lyme Carditis
Yeung and Baranchuk J A C C V O L . 7 3 , N O . 6 , 2 0 1 9
Diagnosis and Treatment of Lyme Carditis F E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6
718
autoimmunologic processes leading toan exaggerated inflammatory response. Au-topsies show a marked tropism of spirochetesfor cardiac tissues (14). The spirocheteinfiltrates the connective tissue associatedwith collagen fibers at the base of the heart,basal interventricular septum, perivascularregions, outer or inner membranes, and morerarely, blood vessels or valves (10,15,16).B. burgdorferi may persist in the extracellularmatrix (17), but does not produce any knownexotoxins or endotoxins (18). Studies innonhuman primates demonstrate a relation-ship between conduction disturbances, in-tensity of myocardial inflammation, andnumber of spirochetes in the cardiac tissue (15).
Unlike the neutrophil-predominant inflammationof Lyme arthritis, the band-like endocardial ortransmural inflammation in LC is mostly composed ofmacrophages and lymphocytes (15). The myocardiummay be affected either independently, simulta-neously with the pericardium, or within pancarditis(19,20). Lyme myocarditis is generally mild, short-term, and self-limited (19–22). The discrepancy be-tween the only sporadically identified spirochetesand the extent of lymphocytic infiltration indicatesthe importance of an immunologic component in theetiology of LC (23,24). Cross-reactive antibodiesinduced by the initial exposure to the bacteria mayreact with self-components, resulting in autoimmuneinjury (24).
The pathophysiology of AV node involvementin LC may be explained by its anatomic location,histology, and metabolic mechanisms (25,26). Elec-trophysiological case reports note a mainly supra-Hisian/intranodal AVB and AV junctional escaperhythm, with only occasional documentation of infra-Hisian blocks (12,27).
MANIFESTATIONS OF LC. Steere et al. (10) firstdescribed LC in 1980 and that it is an early manifes-tation of Lyme disease, appearing within 1 to2 months (range <1 to 28 weeks) after the onset ofinfection (12). AVB is the most common presentationof LC (90%), with high-degree AVB accounting forapproximately two-thirds of the cases (11,12). LCmanifests similarly in both adults and children, with alower prevalence of AVB in children and higherprevalence of first-degree AVB (28). The degree ofAVB can fluctuate over minutes, hours, or days(9,12,22,27). The progression to third-degree AVB canbe rapid and potentially fatal if untreated (14,29–32).Notably, AVB in LC is often transient in nature,particularly with antibiotic treatment (25,33,34). The
electrocardiographic progression of a patient withAVB in LC treated with antibiotics is shown inFigure 1. The signs, symptoms, and electrocardio-graphic presentations of patients with AVB in LCare summarized in Table 1 (35). Besides AVB, othermanifestations of LC include sinus node disease,intra-atrial block, atrial fibrillation, supraventriculartachycardia, sinus node dysfunction, bundle branchblock, and ventricular tachycardia and fibrillation(8,11,20,28,36–39).
LC can also present with acute myocarditis, peri-carditis, myopericarditis, endocarditis, and pan-carditis (11,19,21,22,36,37). Symptomatic myocarditismay contribute to the reversibly decreased left ven-tricular cardiac function found in some patients withsymptoms attributable to conduction disease (12).Lyme myopericarditis has been reported to mimicacute coronary syndrome (40). ST-segment depres-sion or T-wave inversion, especially in the infero-lateral leads, present in 60% of patients with LC,reflect diffuse myocardial involvement and disappearcompletely with clinical remission (10,41). Rarely,Lyme myopericarditis can present with ST segmentelevations and elevated peripheral blood cardiacbiomarkers (9).
Infrequently, LC may be associated with valvularheart disease (36), causing acute heart failure andcardiogenic shock (42). These presentations are notdifferent from those caused by other infectiousagents, and the diagnosis of LC is based on clinicalhistory triggering serological investigations. Clini-cally, patients may report symptoms such as light-headedness, pre-syncope/syncope, shortness ofbreath, palpitations, and chest pain, but also may becompletely asymptomatic (8,32,38). It is not infre-quent for patients to seek medical attention severaltimes in the emergency department before LC issuspected (39,43).
LC PROGNOSIS. The prognosis for treated earlydisseminated LC is very favorable, with completerecovery occurring in most patients who receivedantibiotics (10,18,44,45). High-degree AVB typicallyresolves within the first 10 days of antibiotictreatment (range 3 to 42 days) and other lesssevere conduction disturbances within 6 weeks(8–10,12,25,27,33,34,46). A marker of high risk forprogression to complete AVB is an initial PR interval>300 ms at presentation (10). Brief asystole, escaperhythm with a wide QRS complex, and fluctuatingbundle branch blocks are associated with poorerprognosis (44). Although there are case reports ofdeaths attributable to LC, mortality is exceedinglyrare if the presentation is high-degree AVB and the
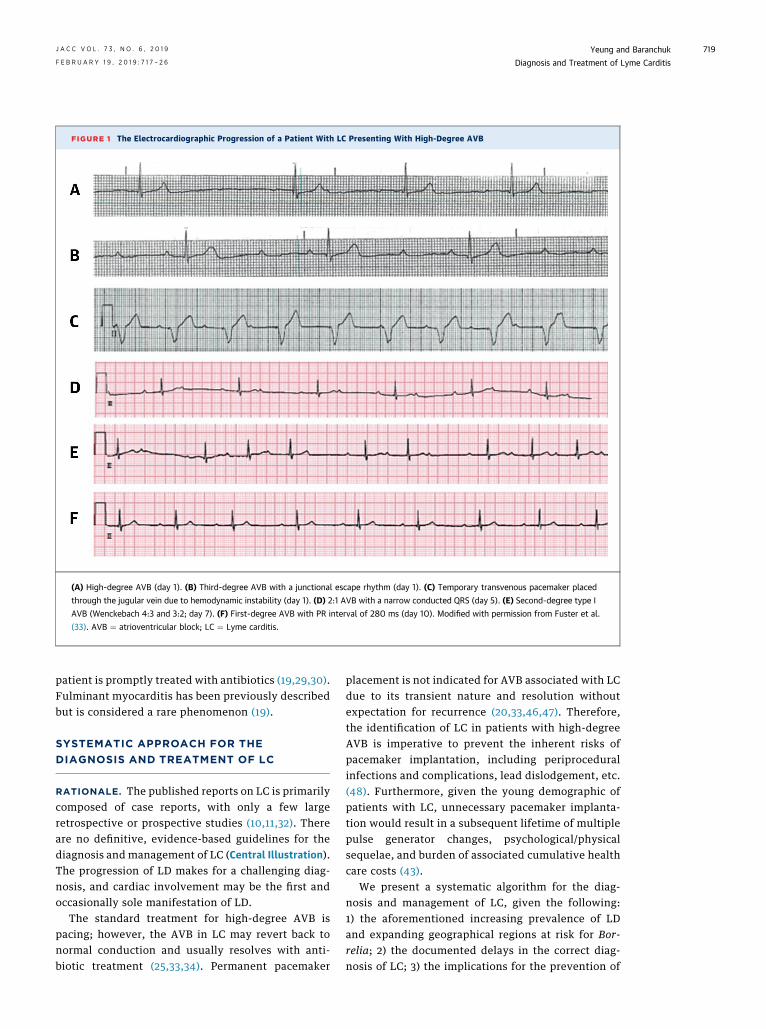
FIGURE 1 The Electrocardiographic Progression of a Patient With LC Presenting With High-Degree AVB
(A) High-degree AVB (day 1). (B) Third-degree AVB with a junctional escape rhythm (day 1). (C) Temporary transvenous pacemaker placed
through the jugular vein due to hemodynamic instability (day 1). (D) 2:1 AVB with a narrow conducted QRS (day 5). (E) Second-degree type I
AVB (Wenckebach 4:3 and 3:2; day 7). (F) First-degree AVB with PR interval of 280 ms (day 10). Modified with permission from Fuster et al.
(33). AVB ¼ atrioventricular block; LC ¼ Lyme carditis.
J A C C V O L . 7 3 , N O . 6 , 2 0 1 9 Yeung and BaranchukF E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6 Diagnosis and Treatment of Lyme Carditis
719
patient is promptly treated with antibiotics (19,29,30).Fulminant myocarditis has been previously describedbut is considered a rare phenomenon (19).
SYSTEMATIC APPROACH FOR THE
DIAGNOSIS AND TREATMENT OF LC
RATIONALE. The published reports on LC is primarilycomposed of case reports, with only a few largeretrospective or prospective studies (10,11,32). Thereare no definitive, evidence-based guidelines for thediagnosis and management of LC (Central Illustration).The progression of LD makes for a challenging diag-nosis, and cardiac involvement may be the first andoccasionally sole manifestation of LD.
The standard treatment for high-degree AVB ispacing; however, the AVB in LC may revert back tonormal conduction and usually resolves with anti-biotic treatment (25,33,34). Permanent pacemaker
placement is not indicated for AVB associated with LCdue to its transient nature and resolution withoutexpectation for recurrence (20,33,46,47). Therefore,the identification of LC in patients with high-degreeAVB is imperative to prevent the inherent risks ofpacemaker implantation, including periproceduralinfections and complications, lead dislodgement, etc.(48). Furthermore, given the young demographic ofpatients with LC, unnecessary pacemaker implanta-tion would result in a subsequent lifetime of multiplepulse generator changes, psychological/physicalsequelae, and burden of associated cumulative healthcare costs (43).
We present a systematic algorithm for the diag-nosis and management of LC, given the following:1) the aforementioned increasing prevalence of LDand expanding geographical regions at risk for Bor-relia; 2) the documented delays in the correct diag-nosis of LC; 3) the implications for the prevention of
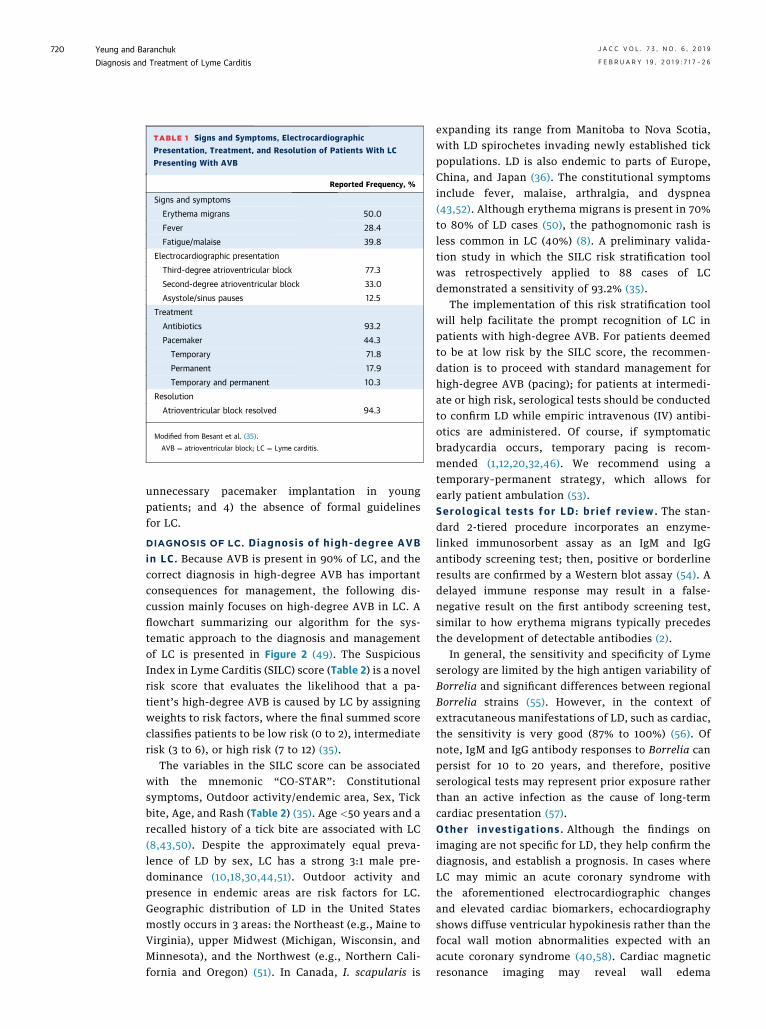
TABLE 1 Signs and Symptoms, Electrocardiographic
Presentation, Treatment, and Resolution of Patients With LC
Presenting With AVB
Reported Frequency, %
Signs and symptoms
Erythema migrans 50.0
Fever 28.4
Fatigue/malaise 39.8
Electrocardiographic presentation
Third-degree atrioventricular block 77.3
Second-degree atrioventricular block 33.0
Asystole/sinus pauses 12.5
Treatment
Antibiotics 93.2
Pacemaker 44.3
Temporary 71.8
Permanent 17.9
Temporary and permanent 10.3
Resolution
Atrioventricular block resolved 94.3
Modified from Besant et al. (35).
AVB ¼ atrioventricular block; LC ¼ Lyme carditis.
Yeung and Baranchuk J A C C V O L . 7 3 , N O . 6 , 2 0 1 9
Diagnosis and Treatment of Lyme Carditis F E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6
720
unnecessary pacemaker implantation in youngpatients; and 4) the absence of formal guidelinesfor LC.
DIAGNOSIS OF LC. Diagnos is of h igh-degree AVBin LC . Because AVB is present in 90% of LC, and thecorrect diagnosis in high-degree AVB has importantconsequences for management, the following dis-cussion mainly focuses on high-degree AVB in LC. Aflowchart summarizing our algorithm for the sys-tematic approach to the diagnosis and managementof LC is presented in Figure 2 (49). The SuspiciousIndex in Lyme Carditis (SILC) score (Table 2) is a novelrisk score that evaluates the likelihood that a pa-tient’s high-degree AVB is caused by LC by assigningweights to risk factors, where the final summed scoreclassifies patients to be low risk (0 to 2), intermediaterisk (3 to 6), or high risk (7 to 12) (35).
The variables in the SILC score can be associatedwith the mnemonic “CO-STAR”: Constitutionalsymptoms, Outdoor activity/endemic area, Sex, Tickbite, Age, and Rash (Table 2) (35). Age <50 years and arecalled history of a tick bite are associated with LC(8,43,50). Despite the approximately equal preva-lence of LD by sex, LC has a strong 3:1 male pre-dominance (10,18,30,44,51). Outdoor activity andpresence in endemic areas are risk factors for LC.Geographic distribution of LD in the United Statesmostly occurs in 3 areas: the Northeast (e.g., Maine toVirginia), upper Midwest (Michigan, Wisconsin, andMinnesota), and the Northwest (e.g., Northern Cali-fornia and Oregon) (51). In Canada, I. scapularis is
expanding its range from Manitoba to Nova Scotia,with LD spirochetes invading newly established tickpopulations. LD is also endemic to parts of Europe,China, and Japan (36). The constitutional symptomsinclude fever, malaise, arthralgia, and dyspnea(43,52). Although erythema migrans is present in 70%to 80% of LD cases (50), the pathognomonic rash isless common in LC (40%) (8). A preliminary valida-tion study in which the SILC risk stratification toolwas retrospectively applied to 88 cases of LCdemonstrated a sensitivity of 93.2% (35).
The implementation of this risk stratification toolwill help facilitate the prompt recognition of LC inpatients with high-degree AVB. For patients deemedto be at low risk by the SILC score, the recommen-dation is to proceed with standard management forhigh-degree AVB (pacing); for patients at intermedi-ate or high risk, serological tests should be conductedto confirm LD while empiric intravenous (IV) antibi-otics are administered. Of course, if symptomaticbradycardia occurs, temporary pacing is recom-mended (1,12,20,32,46). We recommend using atemporary–permanent strategy, which allows forearly patient ambulation (53).Serolog ica l tests for LD: br ie f rev iew. The stan-dard 2-tiered procedure incorporates an enzyme-linked immunosorbent assay as an IgM and IgGantibody screening test; then, positive or borderlineresults are confirmed by a Western blot assay (54). Adelayed immune response may result in a false-negative result on the first antibody screening test,similar to how erythema migrans typically precedesthe development of detectable antibodies (2).
In general, the sensitivity and specificity of Lymeserology are limited by the high antigen variability ofBorrelia and significant differences between regionalBorrelia strains (55). However, in the context ofextracutaneous manifestations of LD, such as cardiac,the sensitivity is very good (87% to 100%) (56). Ofnote, IgM and IgG antibody responses to Borrelia canpersist for 10 to 20 years, and therefore, positiveserological tests may represent prior exposure ratherthan an active infection as the cause of long-termcardiac presentation (57).Other invest igat ions . Although the findings onimaging are not specific for LD, they help confirm thediagnosis, and establish a prognosis. In cases whereLC may mimic an acute coronary syndrome withthe aforementioned electrocardiographic changesand elevated cardiac biomarkers, echocardiographyshows diffuse ventricular hypokinesis rather than thefocal wall motion abnormalities expected with anacute coronary syndrome (40,58). Cardiac magneticresonance imaging may reveal wall edema
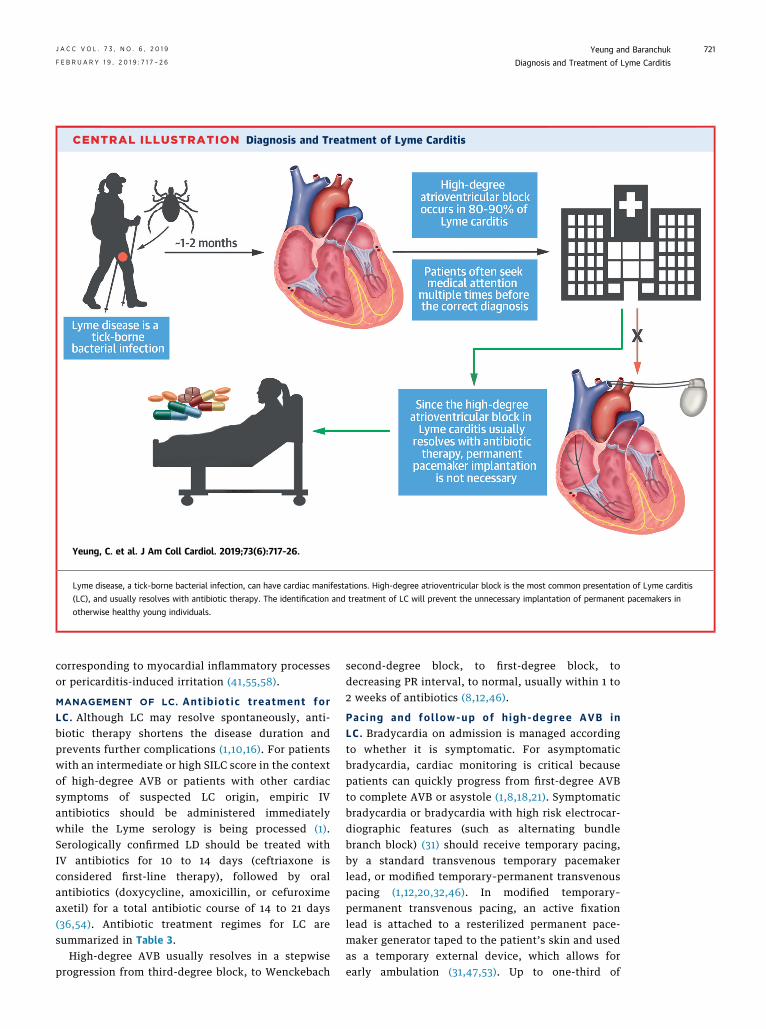
CENTRAL ILLUSTRATION Diagnosis and Treatment of Lyme Carditis
Yeung, C. et al. J Am Coll Cardiol. 2019;73(6):717–26.
Lyme disease, a tick-borne bacterial infection, can have cardiac manifestations. High-degree atrioventricular block is the most common presentation of Lyme carditis
(LC), and usually resolves with antibiotic therapy. The identification and treatment of LC will prevent the unnecessary implantation of permanent pacemakers in
otherwise healthy young individuals.
J A C C V O L . 7 3 , N O . 6 , 2 0 1 9 Yeung and BaranchukF E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6 Diagnosis and Treatment of Lyme Carditis
721
corresponding to myocardial inflammatory processesor pericarditis-induced irritation (41,55,58).
MANAGEMENT OF LC. Ant ib iot i c t reatment forLC . Although LC may resolve spontaneously, anti-biotic therapy shortens the disease duration andprevents further complications (1,10,16). For patientswith an intermediate or high SILC score in the contextof high-degree AVB or patients with other cardiacsymptoms of suspected LC origin, empiric IVantibiotics should be administered immediatelywhile the Lyme serology is being processed (1).Serologically confirmed LD should be treated withIV antibiotics for 10 to 14 days (ceftriaxone isconsidered first-line therapy), followed by oralantibiotics (doxycycline, amoxicillin, or cefuroximeaxetil) for a total antibiotic course of 14 to 21 days(36,54). Antibiotic treatment regimes for LC aresummarized in Table 3.
High-degree AVB usually resolves in a stepwiseprogression from third-degree block, to Wenckebach
second-degree block, to first-degree block, todecreasing PR interval, to normal, usually within 1 to2 weeks of antibiotics (8,12,46).
Pac ing and fol low-up of h igh-degree AVB inLC. Bradycardia on admission is managed accordingto whether it is symptomatic. For asymptomaticbradycardia, cardiac monitoring is critical becausepatients can quickly progress from first-degree AVBto complete AVB or asystole (1,8,18,21). Symptomaticbradycardia or bradycardia with high risk electrocar-diographic features (such as alternating bundlebranch block) (31) should receive temporary pacing,by a standard transvenous temporary pacemakerlead, or modified temporary–permanent transvenouspacing (1,12,20,32,46). In modified temporary–permanent transvenous pacing, an active fixationlead is attached to a resterilized permanent pace-maker generator taped to the patient’s skin and usedas a temporary external device, which allows forearly ambulation (31,47,53). Up to one-third of
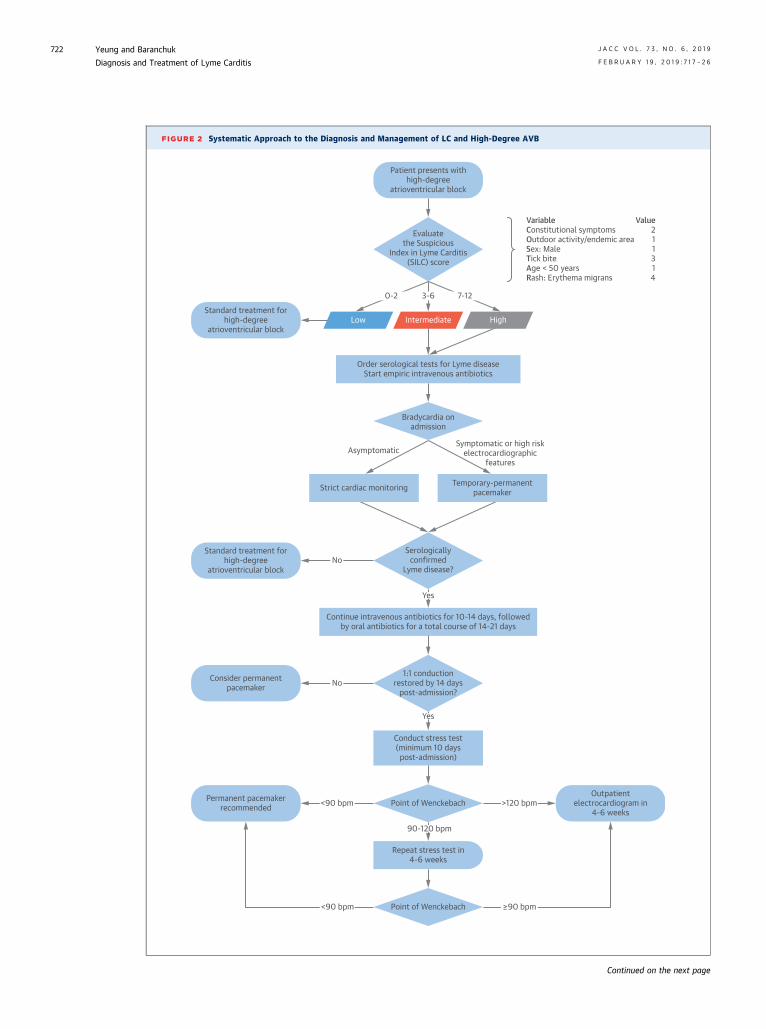
FIGURE 2 Systematic Approach to the Diagnosis and Management of LC and High-Degree AVB
Patient presents withhigh-degree
atrioventricular block
Evaluatethe Suspicious
Index in Lyme Carditis(SILC) score
Standard treatment forhigh-degree
atrioventricular blockLow Intermediate
Order serological tests for Lyme diseaseStart empiric intravenous antibiotics
Bradycardia onadmission
AsymptomaticSymptomatic or high risk
electrocardiographicfeatures
Strict cardiac monitoring Temporary-permanentpacemaker
Serologicallyconfirmed
Lyme disease?
Standard treatment forhigh-degree
atrioventricular block
Consider permanentpacemaker
Permanent pacemakerrecommended
Outpatientelectrocardiogram in
4-6 weeks
Repeat stress test in4-6 weeks
Point of Wenckebach
Point of Wenckebach
<90 bpm
<90 bpm
≥90 bpm
>120 bpm
Yes
No
0-2 3-6 7-12
1:1 conductionrestored by 14 days
post-admission?
Conduct stress test(minimum 10 dayspost-admission)
Continue intravenous antibiotics for 10-14 days, followedby oral antibiotics for a total course of 14-21 days
High
VariableConstitutional symptomsOutdoor activity/endemic areaSex: MaleTick biteAge < 50 years Rash: Erythema migrans
Value211314
90-120 bpm
Yes
No
Continued on the next page
Yeung and Baranchuk J A C C V O L . 7 3 , N O . 6 , 2 0 1 9
Diagnosis and Treatment of Lyme Carditis F E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6
722
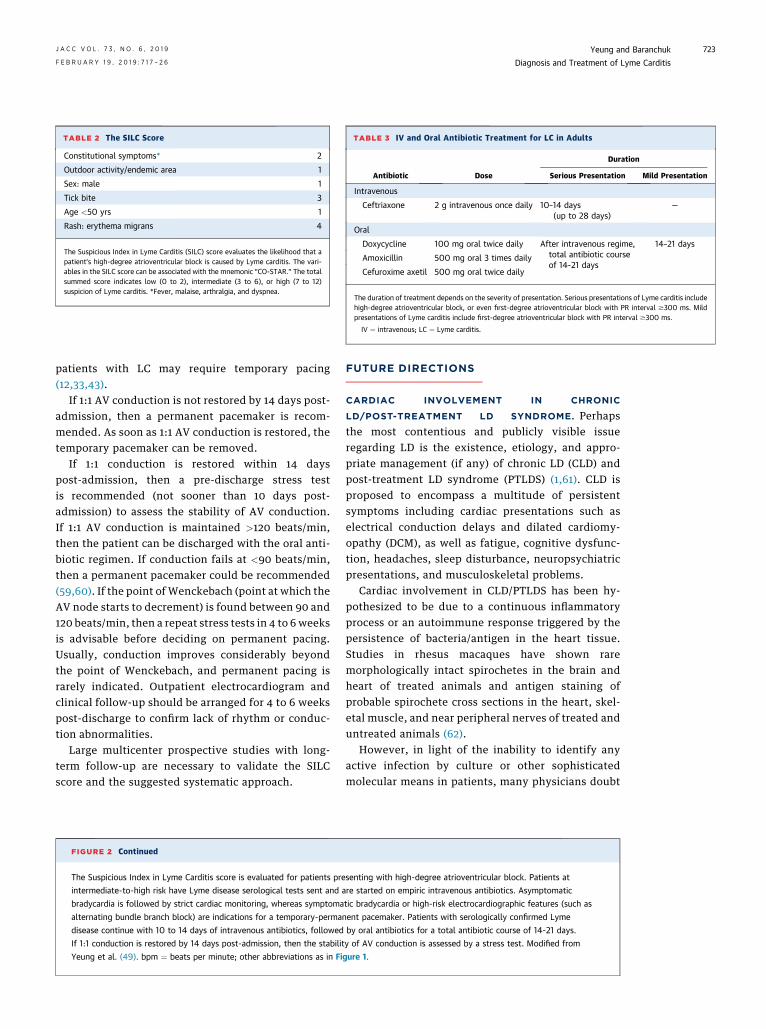
TABLE 2 The SILC Score
Constitutional symptoms* 2
Outdoor activity/endemic area 1
Sex: male 1
Tick bite 3
Age <50 yrs 1
Rash: erythema migrans 4
The Suspicious Index in Lyme Carditis (SILC) score evaluates the likelihood that apatient’s high-degree atrioventricular block is caused by Lyme carditis. The vari-ables in the SILC score can be associated with the mnemonic “CO-STAR.” The totalsummed score indicates low (0 to 2), intermediate (3 to 6), or high (7 to 12)suspicion of Lyme carditis. *Fever, malaise, arthralgia, and dyspnea.
TABLE 3 IV and Oral Antibiotic Treatment for LC in Adults
Antibiotic Dose
Duration
Serious Presentation Mild Presentation
Intravenous
Ceftriaxone 2 g intravenous once daily 10–14 days(up to 28 days)
—
Oral
Doxycycline 100 mg oral twice daily After intravenous regime,total antibiotic courseof 14-21 days
14–21 days
Amoxicillin 500 mg oral 3 times daily
Cefuroxime axetil 500 mg oral twice daily
The duration of treatment depends on the severity of presentation. Serious presentations of Lyme carditis includehigh-degree atrioventricular block, or even first-degree atrioventricular block with PR interval $300 ms. Mildpresentations of Lyme carditis include first-degree atrioventricular block with PR interval $300 ms.
IV ¼ intravenous; LC ¼ Lyme carditis.
J A C C V O L . 7 3 , N O . 6 , 2 0 1 9 Yeung and BaranchukF E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6 Diagnosis and Treatment of Lyme Carditis
723
patients with LC may require temporary pacing(12,33,43).
If 1:1 AV conduction is not restored by 14 days post-admission, then a permanent pacemaker is recom-mended. As soon as 1:1 AV conduction is restored, thetemporary pacemaker can be removed.
If 1:1 conduction is restored within 14 dayspost-admission, then a pre-discharge stress testis recommended (not sooner than 10 days post-admission) to assess the stability of AV conduction.If 1:1 AV conduction is maintained >120 beats/min,then the patient can be discharged with the oral anti-biotic regimen. If conduction fails at <90 beats/min,then a permanent pacemaker could be recommended(59,60). If the point of Wenckebach (point at which theAV node starts to decrement) is found between 90 and120 beats/min, then a repeat stress tests in 4 to 6 weeksis advisable before deciding on permanent pacing.Usually, conduction improves considerably beyondthe point of Wenckebach, and permanent pacing israrely indicated. Outpatient electrocardiogram andclinical follow-up should be arranged for 4 to 6 weekspost-discharge to confirm lack of rhythm or conduc-tion abnormalities.
Large multicenter prospective studies with long-term follow-up are necessary to validate the SILCscore and the suggested systematic approach.
FIGURE 2 Continued
The Suspicious Index in Lyme Carditis score is evaluated for patients pre
intermediate-to-high risk have Lyme disease serological tests sent and a
bradycardia is followed by strict cardiac monitoring, whereas symptoma
alternating bundle branch block) are indications for a temporary-perma
disease continue with 10 to 14 days of intravenous antibiotics, followed
If 1:1 conduction is restored by 14 days post-admission, then the stabilit
Yeung et al. (49). bpm ¼ beats per minute; other abbreviations as in Fi
FUTURE DIRECTIONS
CARDIAC INVOLVEMENT IN CHRONIC
LD/POST-TREATMENT LD SYNDROME. Perhapsthe most contentious and publicly visible issueregarding LD is the existence, etiology, and appro-priate management (if any) of chronic LD (CLD) andpost-treatment LD syndrome (PTLDS) (1,61). CLD isproposed to encompass a multitude of persistentsymptoms including cardiac presentations such aselectrical conduction delays and dilated cardiomy-opathy (DCM), as well as fatigue, cognitive dysfunc-tion, headaches, sleep disturbance, neuropsychiatricpresentations, and musculoskeletal problems.
Cardiac involvement in CLD/PTLDS has been hy-pothesized to be due to a continuous inflammatoryprocess or an autoimmune response triggered by thepersistence of bacteria/antigen in the heart tissue.Studies in rhesus macaques have shown raremorphologically intact spirochetes in the brain andheart of treated animals and antigen staining ofprobable spirochete cross sections in the heart, skel-etal muscle, and near peripheral nerves of treated anduntreated animals (62).
However, in light of the inability to identify anyactive infection by culture or other sophisticatedmolecular means in patients, many physicians doubt
senting with high-degree atrioventricular block. Patients at
re started on empiric intravenous antibiotics. Asymptomatic
tic bradycardia or high-risk electrocardiographic features (such as
nent pacemaker. Patients with serologically confirmed Lyme
by oral antibiotics for a total antibiotic course of 14-21 days.
y of AV conduction is assessed by a stress test. Modified from
gure 1.

Yeung and Baranchuk J A C C V O L . 7 3 , N O . 6 , 2 0 1 9
Diagnosis and Treatment of Lyme Carditis F E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6
724
any causal relationship between treated LD and thesubsequent reported array of vague, nonspecificsymptoms. Serological tests are not useful in inves-tigating PTLDS because various levels of IgG and IgMantibodies are known to remain detectable severalyears after adequate antibiotic treatment (57). More-over, no strain of B. burgdorferi has been describedthat is resistant to the recommended antibiotics (63).Therefore, practice guidelines from numerous NorthAmerican and European medical societies discouragethe diagnosis of CLD and recommend against treatingpatients with prolonged or repeated antibiotic cour-ses, which have been demonstrated by randomizedcontrolled trials to not show a sustained benefit(64,65).
Furthermore, the possible link between Borreliainfection and the development of DCM is alsocontroversial (20). The correlation between increasedBorrelia antibodies in patients with DCM was initiallysuggested by Stanek et al. (66,67), but was notconfirmed by subsequent studies (44,68,69).Although some research employing polymerase chainreaction found a significantly higher genome preva-lence of B. burgdorferi in patients recently diagnosedwith DCM compared with controls (23,70), left ven-tricular function did not improve with antibiotictreatment in patients who tested positive for theBorrelia genome (23).
VACCINATION. There is no preventative vaccinecurrently available for LD. Two OspA-based vaccines,LYMErix (SmithKline Beecham, Brentford, UnitedKingdom) and ImuLyme (Pasteur Mérieux-Con-naught, Lyon, France), have demonstrated efficacy inclinical trials, and a multivalent OspA vaccine (BaxterBioscience, Deerfield, Illinois) has been tested inPhase I/II clinical trials (71–73). In the United States,
LYMErix (SmithKlineBeecham, Pittsburgh, Pennsyl-vania) demonstrated 80% effectiveness and wasreleased for commercial use in 1998 until 2002 (74).However, the manufacturer voluntarily withdrew thevaccine in the midst of extensive media coverage,ongoing litigation, and falling sales—notwithstandingunanimous approval by the Food and Drug Adminis-tration and studies indicating that the vaccinerepresented a cost-effective public health interven-tion (74,75).
The high variability of Borrelia antigen proteinsimplies that a novel vaccine may require a combina-tion of several antigens or multiple epitopes based onvector-borne proteins and several outer membraneproteins to be effective. Many studies have concen-trated on antigenic subunits such as OspA, OspB,OspC, DbpA, and Bbk32 (36). The application of omicsand bioinformatics analysis to vaccine developmentrepresents a promising avenue for the identificationof vaccine targets against Borrelia with increasedimmunogenicity (76).
CONCLUSIONS
LC is an early manifestation of LD that has a veryfavorable prognosis with appropriate antibiotictreatment. A systematic approach to the diagnosisand treatment of LC will facilitate the identification ofLC in patients with high-degree AVB, thus preventingunnecessary implantation of permanent pacemakers.
ADDRESS FOR CORRESPONDENCE: Dr. Adrian Bar-anchuk, Department of Cardiology, Kingston GeneralHospital, Queen’s University, 76 Stuart Street, Kingston,Ontario K7L 2V7, Canada. E-mail: [email protected]. Twitter: @adribaran, @yeung2020.
RE F E RENCE S
1. Wormser GP, Dattwyler RJ, Shapiro ED, et al.The clinical assessment, treatment, and preven-tion of Lyme disease, human granulocyticanaplasmosis, and babesiosis: clinical practiceguidelines by the Infectious Diseases Society ofAmerica. Clin Infect Dis 2006;43:1089–134.
2. Shapiro ED, Wormser GP. Lyme disease in 2018:what is new (and what is not). JAMA 2018;320:635–6.
3. Rosenberg R, Lindsey NP, Fischer M, et al. Vitalsigns: trends in reported vectorborne diseasecases - United States and Territories, 2004-2016.MMWR Morb Mortal Wkly Rep 2018;67:496–501.
4. Centers for DiseaseControl andPrevention. LymeDisease: Data and Surveillance. Available at: https://www.cdc.gov/lyme/stats/index.html. AccessedSeptember 4, 2018.
5. Hinckley AF, Connally NP, Meek JI, et al. Lymedisease testing by large commercial laboratoriesin the United States. Clin Infect Dis 2014;59:676–81.
6. Public Health Agency of Canada. Surveillanceof Lyme disease. Available at: https://www.canada.ca/en/public-health/services/diseases/lyme-disease/surveillance-lyme-disease.html. Accessed September3, 2018.
7. Ripoche M, Gasmi S, Adam-Poupart A, et al.Passive tick surveillance provides an accurate earlysignal of emerging Lyme disease risk and humancases in southern Canada. J Med Entomol 2018;55:1016–26.
8. Krause PJ, Bockenstedt LK. Cardiology patientpages. Lyme disease and the heart. Circulation2013;127:e451–4.
9. Cox J, Krajden M. Cardiovascular manifestationsof Lyme disease. Am Heart J 1991;122:1449–55.
10. Steere AC, Batsford WP, Weinberg M, et al.Lyme carditis: cardiac abnormalities of Lyme dis-ease. Ann Intern Med 1980;93:8–16.
11. van der Linde MR. Lyme carditis: clinical char-acteristics of 105 cases. Scand J Infect Dis Suppl1991;77:81–4.
12. McAlister HF, Klementowicz PT, Andrews C,Fisher JD, Feld M, Furman S. Lyme carditis: animportant cause of reversible heart block. AnnIntern Med 1989;110:339–45.
13. Woolf PK, Lorsung EM, Edwards KS, et al.Electrocardiographic findings in children withLyme disease. Pediatr Emerg Care 1991;7:334–6.
J A C C V O L . 7 3 , N O . 6 , 2 0 1 9 Yeung and BaranchukF E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6 Diagnosis and Treatment of Lyme Carditis
725
14. Muehlenbachs A, Bollweg BC, Schulz TJ, et al.Cardiac tropism of Borrelia burgdorferi: an autopsystudy of sudden cardiac death associated withLyme carditis. Am J Pathol 2016;186:1195–205.
15. Cadavid D, Bai Y, Hodzic E, Narayan K,Barthold SW, Pachner AR. Cardiac involvement innon-human primates infected with the Lyme dis-ease spirochete Borrelia burgdorferi. Lab Invest2004;84:1439–50.
16. Haddad FA, Nadelman RB. Lyme disease andthe heart. Front Biosci 2003;8:s769–82.
17. Cabello FC, Godfrey HP, Newman SA. Hiddenin plain sight: Borrelia burgdorferi and the extra-cellular matrix. Trends Microbiol 2007;15:350–4.
18. Steere AC. Lyme disease. N Engl J Med 2001;345:115–25.
19. Yoon EC, Vail E, Kleinman G, et al. Lyme dis-ease: a case report of a 17-year-old male with fatalLyme carditis. Cardiovasc Pathol 2015;24:317–21.
20. Robinson ML, Kobayashi T, Higgins Y,Calkins H, Melia MT. Lyme carditis. Infect Dis ClinNorth Am 2015;29:255–68.
21. Pinto DS. Cardiac manifestations of Lyme dis-ease. Med Clin North Am 2002;86:285–96.
22. Manzoor K, Aftab W, Choksi S, Khan IA. Lymecarditis: sequential electrocardiographic changesin response to antibiotic therapy. Int J Cardiol2009;137:167–71.
23. Kubanek M, Sramko M, Berenova D, et al.Detection of Borrelia burgdorferi sensu lato inendomyocardial biopsy specimens in individualswith recent-onset dilated cardiomyopathy. Eur JHeart Fail 2012;14:588–96.
24. Raveche ES, Schutzer SE, Fernandes H, et al.Evidence of Borrelia autoimmunity-inducedcomponent of Lyme carditis and arthritis. J ClinMicrobiol 2005;43:850–6.
25. Sharma AK, Almaddah N, Chaudhry K,Ganatra S, Chaudhry GM, Silver J. Without furtherdelay: Lyme carditis. Am J Med 2018;131:384–6.
26. Imai DM, Feng S, Hodzic E, Barthold SW. Dy-namics of connective-tissue localization duringchronic Borrelia burgdorferi infection. Lab Invest2013;93:900–10.
27. van der Linde MR, Crijns HJ, Lie KI. Transientcomplete AV block in Lyme disease. Electrophys-iologic observations. Chest 1989;96:219–21.
28. Kostic T, Momcilovic S, Perisic ZD, et al.Manifestations of Lyme carditis. Int J Cardiol 2017;232:24–32.
29. Centers for Disease Control and Prevention.Three sudden cardiac deaths associated with Lymecarditis - United States, November 2012-July2013. MMWR Morb Mortal Wkly Rep 2013;62:993–6.
30. Forrester JD, Meiman J, Mullins J, et al. Notesfrom the field: update on Lyme carditis, groups athigh risk, and frequency of associated suddencardiac death–United States. MMWR Morb MortalWkly Rep 2014;63:982–3.
31. Khalil S, Padala SK, Hui CM, Steckman DA,Sidhu MS, Torosoff MT. Lyme carditis in the fastlane: from alternating bundle branch block toasystole in 12 hours. Conn Med 2015;79:517–20.
32. Forrester JD, Mead P. Third-degree heart blockassociated with Lyme carditis: review of publishedcases. Clin Infect Dis 2014;59:996–1000.
33. Fuster LS, Gul EE, Baranchuk A. Electrocar-diographic progression of acute Lyme disease. AmJ Emerg Med 2017;35:1040. e5–e6.
34. Fu Md J, Bhatta L. Lyme carditis: early occur-rence and prolonged recovery. J Electrocardiol2018;51:516–8.
35. Besant G, Wan D, Yeung C, et al. SuspiciousIndex in Lyme Carditis (SILC): systematic reviewand proposed new risk score. Clin Cardiol 2018;41:1611–6.
36. Bush LM, Vazquez-Pertejo MT. Tick borneillness-Lyme disease. Dis Mon 2018;64:195–212.
37. Ciesielski CA, Markowitz LE, Horsley R,Hightower AW, Russell H, Broome CV. Lyme dis-ease surveillance in the United States, 1983-1986.Rev Infect Dis 1989;11 Suppl 6:S1435–41.
38. Chaus A, Kazmi FN, Adil A, Pavlovic T,Hertsberg A. Lyme carditis: a case of reversiblecomplete heart block and atrial flutter (abstr).J Am Coll Cardiol 2018;71:A2540.
39. Banga G, Temple J. Sudden cardiac arrest andelectrical storm: an unusual presentation of Lymecarditis (abstr). J Am Coll Cardiol 2018;71:A2559.
40. Horowitz HW, Belkin RN. Acute myoper-icarditis resulting from Lyme disease. Am Heart J1995;130:176–8.
41. Munk PS, Orn S, Larsen AI. Lyme carditis:persistent local delayed enhancement by cardiacmagnetic resonance imaging. Int J Cardiol 2007;115:e108–10.
42. Koene R, Boulware DR, Kemperman M, et al.Acute heart failure from Lyme carditis. Circ HeartFail 2012;5:e24–6.
43. Wan D, Blakely C, Branscombe P, Suarez-Fuster L, Glover B, Baranchuk A. Lyme carditis andhigh-degree atrioventricular block. Am J Cardiol2018;121:1102–4.
44. Lelovas P, Dontas I, Bassiakou E, Xanthos T.Cardiac implications of Lyme disease, diagnosisand therapeutic approach. Int J Cardiol 2008;129:15–21.
45. Costello JM, Alexander ME, Greco KM, Perez-Atayde AR, Laussen PC. Lyme carditis in children:presentation, predictive factors, and clinicalcourse. Pediatrics 2009;123:e835–41.
46. Sangha M, Chu A. Permanent pacemakeravoided in high grade atrioventricular block(abstr). J Am Coll Cardiol 2018;71:A363.
47. Epstein AE, DiMarco JP, Ellenbogen KA, et al.ACC/AHA/HRS 2008 guidelines for device-basedtherapy of cardiac rhythm abnormalities: a reportof the American College of Cardiology/AmericanHeart Association Task Force on Practice Guide-lines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation ofCardiac Pacemakers and Antiarrhythmia Devices).J Am Coll Cardiol 2008;51:e1–62.
48. Wan D, Baranchuk A. Lyme carditis and atrio-ventricular block. CMAJ 2018;190:E622.
49. Yeung C, Baranchuk A. Systematic approach tothe diagnosis and treatment of Lyme carditis and
high-degree atrioventricular block. Healthcare(Basel) 2018;6:E119.
50. Nagi KS, Joshi R, Thakur RK. Cardiac mani-festations of Lyme disease: a review. Can J Cardiol1996;12:503–6.
51. Bacon RM, Kugeler KJ, Mead PS, Centers forDisease Control and Prevention. Surveillance forLyme disease–United States, 1992-2006. MMWRSurveill Summ 2008;57:1–9.
52. Steere AC, Malawista SE, Hardin JA, Ruddy S,Askenase W, Andiman WA. Erythema chronicummigrans and Lyme arthritis. The enlarging clinicalspectrum. Ann Intern Med 1977;86:685–98.
53. Wang C, Chacko S, Abdollah H, Baranchuk A.Treating Lyme carditis high-degree AV block usinga temporary–permanent pacemaker. Ann Nonin-vasive Electrocardiol 2018:e12599.
54. Stanek G, Wormser GP, Gray J, Strle F. Lymeborreliosis. Lancet 2012;379:461–73.
55. Scheffold N, Herkommer B, Kandolf R, May AE.Lyme carditis–diagnosis, treatment and prognosis.Dtsch Arztebl Int 2015;112:202–8.
56. Moore A, Nelson C, Molins C, Mead P,Schriefer M. Current Guidelines, Common ClinicalPitfalls, and Future Directions for LaboratoryDiagnosis of Lyme Disease, United States. EmergInfect Dis 2016;22:1169–77.
57. Kalish RA, McHugh G, Granquist J, Shea B,Ruthazer R, Steere AC. Persistence of immuno-globulin M or immunoglobulin G antibody re-sponses to Borrelia burgdorferi 10-20 years afteractive Lyme disease. Clin Infect Dis 2001;33:780–5.
58. Maher B, Murday D, Harden SP. Cardiac MRI ofLyme disease myocarditis. Heart 2012;98:264.
59. Andersen HR, Nielsen JC, Thomsen PE, et al.Atrioventricular conduction during long-termfollow-up of patients with sick sinus syndrome.Circulation 1998;98:1315–21.
60. Kristensen L, Nielsen JC, Pedersen AK,Mortensen PT, Andersen HR. AV block andchanges in pacing mode during long-term follow-up of 399 consecutive patients with sick sinussyndrome treated with an AAI/AAIR pacemaker.Pacing Clin Electrophysiol 2001;24:358–65.
61. Feder HM Jr., Johnson BJ, O’Connell S, et al.A critical appraisal of “chronic Lyme disease”.N Engl J Med 2007;357:1422–30.
62. Crossland NA, Alvarez X, Embers ME. Latedisseminated Lyme disease: associated pathologyand spirochete persistence posttreatment in rhe-sus macaques. Am J Pathol 2018;188:672–82.
63. Hunfeld K-P, Ruzic-Sabljic E, Norris DE,Kraiczy P, Strle F. In vitro susceptibility testing ofBorrelia burgdorferi sensu lato isolates culturedfrom patients with erythema migrans before andafter antimicrobial chemotherapy. AntimicrobAgents Chemother 2005;49:1294–301.
64. Lantos PM. Chronic Lyme disease. Infect DisClin North Am 2015;29:325–40.
65. Klempner MS, Hu LT, Evans J, et al. Twocontrolled trials of antibiotic treatment in patientswith persistent symptoms and a history of Lymedisease. N Engl J Med 2001;345:85–92.

Yeung and Baranchuk J A C C V O L . 7 3 , N O . 6 , 2 0 1 9
Diagnosis and Treatment of Lyme Carditis F E B R U A R Y 1 9 , 2 0 1 9 : 7 1 7 – 2 6
726
66. Stanek G, Klein J, Bittner R, Glogar D. Isolationof Borrelia burgdorferi from the myocardium of apatient with longstanding cardiomyopathy. N EnglJ Med 1990;322:249–52.
67. Stanek G, Klein J, Bittner R, Glogar D. Borreliaburgdorferi as an etiologic agent in chronic heartfailure? Scand J Infect Dis Suppl 1991;77:85–7.
68. Sonnesyn SW, Diehl SC, Johnson RC, Kubo SH,Goodman JL. A prospective study of the seropre-valence of Borrelia burgdorferi infection in pa-tients with severe heart failure. Am J Cardiol 1995;76:97–100.
69. Sangha O, Phillips CB, Fleischmann KE, et al.Lack of cardiac manifestations among patientswith previously treated Lyme disease. Ann InternMed 1998;128:346–53.
70. Palecek T, Kuchynka P, Hulinska D, et al. Pres-ence of Borrelia burgdorferi in endomyocardial
biopsies in patients with new-onset unexplaineddilated cardiomyopathy. Med Microbiol Immunol2010;199:139–43.
71. Sigal LH, Zahradnik JM, Lavin P, et al., Re-combinant Outer-Surface Protein A Lyme DiseaseVaccine Study Consortium. A vaccine consisting ofrecombinant Borrelia burgdorferi outer-surfaceprotein A to prevent Lyme disease. N Engl J Med1998;339:216–22.
72. Steere AC, Sikand VK, Meurice F, et al.,Lyme Disease Vaccine Study Group. Vaccina-tion against Lyme disease with recombinantBorrelia burgdorferi outer-surface lipoproteinA with adjuvant. N Engl J Med 1998;339:209–15.
73. Wressnigg N, Pollabauer EM, Aichinger G,et al. Safety and immunogenicity of a novelmultivalent OspA vaccine against Lyme borreliosis
in healthy adults: a double-blind, randomised,dose-escalation phase 1/2 trial. Lancet Infect Dis2013;13:680–9.
74. Plotkin SA. Correcting a public health fiasco:the need for a new vaccine against Lyme disease.Clin Infect Dis 2011;52 Suppl 3:s271–5.
75. Meltzer MI, Dennis DT, Orloski KA. The costeffectiveness of vaccinating against Lyme disease.Emerg Infect Dis 1999;5:321–8.
76. Bencurova E, Gupta SK, Oskoueian E, Bhide M,Dandekar T. Omics and bioinformatics applied tovaccine development against Borrelia. Mol Omics2018;14:330–40.
KEY WORDS atrioventricular block,Borrelia, Lyme carditis, Lyme disease






















![[Normas APA, 7.ª edición] Estilo de la American](https://img.pdfslide.us/doc/110x75/6169bde111a7b741a34ad970/normas-apa-7-edicin-estilo-de-la-american-.jpg)
![[the American Journal of Cardiology] the American (Bookos.org)](https://img.pdfslide.us/doc/110x75/55cf9c89550346d033aa2ae3/the-american-journal-of-cardiology-the-american-bookosorg.jpg)





