Embed Size (px)
Citation preview

J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 0 , N O . 1 2 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 8 . 0 0 3
LEADERSHIP PAGE
Diversity Matters
Pamela S. Douglas, MD, MACC, Past President, American College ofCardiology; Chair, ACC Task Force on DiversityKim Allan Williams, SR, MD, MACC, Past President, American College ofCardiology; Vice-Chair, ACC Task Force on DiversityMary Norine Walsh, MD, FACC, President, American College of CardiologyD iversity and inclusion are increasinglyrecognized as requirements for optimalorganizational performance as they have
proven to (1):
� Improve financial performance� Leverage talent� Reflect the marketplace and build reputation� Increase innovation and group performance
In medicine, the case for diversity also includes: tobetter serve diverse patients, to promote healthequity, to provide diverse mentors at all levels, tobring different points of view to debates and problemsolving, to better engage our communities, and toinclude investigators with a broad range of perspec-tives in their scholarly activities.
CARDIOLOGY IS NOT A
DIVERSE PROFESSION
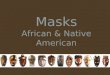
In comparison to the U.S. population, cardiology isfar less diverse (Figure 1). Data from the AmericanMedical Association and the American Council onGraduate Medical Education show that 5.4% of car-diology trainees were African American and 6.8%were Hispanic, compared with 5.8% and 7.8%,respectively, in internal medicine in the 2015 to 2016academic year (2). Overall, <10% of medical studentsand <3% of medical school faculty are AfricanAmerican (3). Although American College of Cardiol-ogy (ACC) member racial/ethnic demographicdata are incomplete, and we do not have robustoverall data on African-American and Hispanic
representation, the ACC 2016 Professional LifeSurvey suggests that these groups each represent 3%to 6% of our membership (4). Specifically, extrapo-lating respondents’ data suggests that there areapproximately 300 African-American men and 100African-American women Fellows of the AmericanCollege of Cardiology.
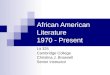
The ACC’s own data show that 9.8% of Fellowswho are U.S. board certified in adult cardiovasculardisease are women. American Association of MedicalColleges workforce reports show an improvementfrom 9.7% women in 2007 to 13.2% in 2015, but thisis still far below the 37% of women in generalinternal medicine (Figure 2) (5,6). In fact, regardingthe percentage of women in the specialty, cardiol-ogy ranks 36th out of 44 specialties tracked, andinterventional cardiology ranks 42nd, followed onlyby thoracic and orthopedic surgery. The proportionof women in cardiology fellowships has held steadyat 21% for the past 6 years, although internal med-icine residents, our talent pool, are 43% female.This strongly suggests that the under-representationof women is not a pipeline issue, and may ulti-mately have a negative effect on our ability toattract and retain the best and brightest to ourprofession.
IMPROVING PATIENT CARE
Diversity is not just an issue for cardiologists; it isan issue for quality patient care. The SullivanReport, Missing Persons: Minorities in the HealthProfessions: A Report of the Sullivan Commission on

FIGURE 1 Diversity in Cardiology Versus the U.S. Population
USA Cardiology
White/Asian HispanicAfrican American
Men Women
Data from U.S. population 2010 census data; Lewis et al. (4);
and Laslett et al. (9).
Douglas et al. J A C C V O L . 7 0 , N O . 1 2 , 2 0 1 7
Leadership Page S E P T E M B E R 1 9 , 2 0 1 7 : 1 5 2 5 – 9
1526
Diversity in the Healthcare Workforce (7), notedthat diversity plays an important role in thenation’s health: “The fact that the nation’s healthprofessions have not kept pace with changingdemographics may be an even greater cause ofdisparities in health access and outcomes than thepersistent lack of health insurance for tens ofmillions of Americans.” Similarly, the AmericanAssociation of Medical Colleges has called onpolicymakers to “prioritize research and initiativesfor increasing diversity in the physician work-force” (8).
ESSENTIAL TO OUR MISSION
Diversity and inclusion are essential to the ACC’smission, values, patients, and strategic business goalsas a profession and as a professional society. Thereasons for this include:
� Diversity drives better business decisions andfinancial performance, making it essential for ACCgovernance/leadership excellence.
� The ability to recruit from the entire available poolis critical to ensure continued excellence andmaximize the talent in our profession.
� Diversity and inclusion are important elementsof achieving the “Quadruple Aim” of clinician
wellness, leading to enhanced job performance andwork life, reduced harassment and burnout, andimproved job satisfaction. This, in turn, improvescare and patient satisfaction.
� A more diverse cardiovascular workforce will bet-ter address the health needs of our increasinglydiverse patient populations, and make progresstoward health equity.
� The movement toward team care requires clinicianhealth, communication, and trust—qualities thatare promoted by diversity and inclusion.
� Innovation requires diversity of background, ideas,and experience.
� Diversity and inclusion provide the ACC with achance to lead among medical professionalsocieties.
MOVING TOWARD SOLUTIONS
To address these issues, the ACC Task Force onDiversity was formed in early 2017 and was chargedwith providing recommendations to the Board ofTrustees to enable the achievement of the followinggoals:
1. To ensure that both cardiovascular medicine ingeneral, as well as the ACC itself, attract and providerewarding careers for the full range of talentedindividuals in medicine.
2. To ensure that both cardiovascular medicine ingeneral, as well as ACC itself, benefit from a diversityof backgrounds, experiences, and perspectives inleadership, cardiovascular health care delivery,education, and science.
3. To ensure that the diverse needs of cardiovascularpatients are met by cardiovascular clinicians sensi-tive to and respectful of their sex, cultural, racial,and ethnic diversity.
ACC Task Force on Diversity members (Table 1)were divided by preference into 5 work groups withthe following objectives:
� Data and benchmarking: To provide the informa-tion required to fully assess the problem, bench-mark the cardiology field and ACC, and devisesolutions, as well as to create feasible and mean-ingful progress indicators/metrics.
� Deep pipeline: To increase the talent pool of under-represented minorities and women selectingmedicine and cardiology as a career.
� Internal medicine residency to fellowship “cliff”: Toensure access to available talent: recruitment andretention among cardiologists.

prbe
ov
FIGURE 2 Percentage of Women in Cardiology Relative to 44 Other Specialties Over Time
Pediatrics
2007
Internal Medicine/Pediatrics
Child & Adolescent Psychiatry
Geriatric Medicine
Obstetrics and Gynecology
Neonatal-Perinatal Medicine
Dermatology
Endocrinology, Diabetes & Metabolism
Physical Medicine and Rehabilitation
Infectious Disease
Rheumatology
Psychiatry
Internal Medicine44.0%
9.7%
Anatomic/Clinical Pathology
Family Medicine/General Practice
Allergy and Immunology
Preventive Medicine
Hematology and Oncology
Radiation Oncology
Neurology
Anesthesiology
Emergency Medicine
Nephrology
Radiology and Diagnostic Radiology
Ophthalmology
Pulmonary Disease and Critical Care Medicine
General Surgery
Plastic Surgery
Otolaryngology
Gastroenterology
Cardiovascular Disease
Vascular Surgery
Neurological Surgery
Urology
Thoracic Surgery
Orthopedic Surgery
0% 10% 20%
Primary Care
30% 40% 50% 60%
PediatricsObstetrics & Gynecology
Pediatrics Hematology/OncologyChild & Adolescent Psychiatry
Internal Medicine/PediatricsGeriatric Medicine
Neonatal-Perinatal MedicineDermatology
Endocrinology, Diabetes & MetabolismRheumatology
Infectious DiseaseFamily Medicine/General Practice
PsychiatryInternal Medicine
Anatomic/Clinical PathologyAllergy & Immunology
Physical Medicine & RehabilitationAll specialties
Pediatric CardiologyPreventive Medicine
Hematology & OncologyNeurology
NephrologyRadiation Oncology
Emergency MedicineCritical Care Medicine
AnesthesiologyRadiology & Diagnostic Radiology
OphthalmologyNeuroradiologyGeneral Surgery
Pain Medicine & Pain ManagementGastroenterology
OtolaryngologyPlastic Surgery
Cardiovascular DiseaseVascular Surgery
Pulmonary DiseaseVascular & Interventional Radiology
UrologyNeurological Surgery
Interventional CardiologyThoracic Surgery
Orthopedic Surgery
2015
36.8%
7.4%
13.2%
Average = 28.3%
0 10 20 30 40 50 60 70
Reprinted, with permission, from the Center for Workforce Studies, Association of American Medical Colleges (5,6).
J A C C V O L . 7 0 , N O . 1 2 , 2 0 1 7 Douglas et al.S E P T E M B E R 1 9 , 2 0 1 7 : 1 5 2 5 – 9 Leadership Page
1527
� Cardiology field: To purposefully create a culture ofinclusion in the cardiology community throughadvocacy and through championing and commu-nicating diversity.
� Overarching concerns: To ensure that efforts to in-crease diversity and inclusivity are sustainable andimplemented throughout the organization so thatthey will maximally benefit the ACC and the field ofcardiology.
Each group has identified a series of strategic ini-tiatives to address its goal, along with tactics, asso-ciated benchmarks and progress indicators/metrics,and enduring accountabilities. This includes identi-fying and recommending changes in policies, pro-cesses, education, structure, culture, and applicationof resources to foster a culture of inclusion andensure the entry and advancement of women andunder-represented minorities in the field of
cardiology. The recommendations of each group werepresented to the entire Task Force, after which, ob-jectives and recommended strategic initiatives(including action items and progress/success metricsfor each) were substantially revised and prioritized.
The ACC Task Force on Diversity presented aninterim report to the Board of Trustees at its AugustStrategic Planning Retreat, including a detailedbackground document, draft Diversity and InclusionStrategic Plan, and prioritized recommendations foractivities to launch in 2018. The following 3 broadobjectives were identified:
Objective 1: Enhance the culture within the cardiology
ofession and the perceptions of the field tomore inclusive, professional, equitable, andlcoming. weObjective 2: Realize and sustain the value of diversity
er the long term by implementing structures and
co
byinenan
TABLE 1 ACC Task Force on Diversity Members
Name and Title ACC/Other Society Role Home Institution and Role
Pamela Douglas, MD, MACC Task Force Chair ACC President 2005–2006 Geller Professor of Research inCardiovascular Disease, Duke University
Kim Allan Williams Sr., MD, MACC Task Force Co-Chair ACC President 2015–2016 Chief of Cardiology, Rush University
David Acosta, MD Chief Diversity Officer, American Associationof Medical Colleges
Kim Burns, MD Medical Officer, National Heart, Lung, andBlood Institute
Quinn Capers, MD, FACC Co-Chair, ACC Training Directors Working Group onDiversity
Associate Dean for Admissions, AssistProfessor, The Ohio State UniversityCollege of Medicine
Barbara Casadei, MD, PhD President-Elect, European Society of Cardiology BHF Professor of Cardiovascular Medicine,University of Oxford
Anna Lisa Crowley, MD, FACC Co-Chair, ACC Training Directors Working Group onDiversity
Associate Professor of Medicine, DukeUniversity
Claire Duvernoy, MD, FACC Chair, ACC Women in Cardiology Chief of Cardiology, Ann Arbor VA Universityof Michigan
Robert Harrington, MD, MACC Member, ACC Academic Council, Women in CardiologyCouncil, Lifelong Learning Oversight CommitteeFormer Member, ACC Board of Trustees
Bloomfield Professor and Chair, Departmentof Medicine, Stanford University
Sharonne Hayes, MD, FACC Chief Diversity Officer, Mayo Clinic
Gerald Johnson II Chief Diversity Officer, American HeartAssociation
Lauren Kane, MD, FACC Member, ACC Surgeons’ Council Assistant Professor of Surgery, CongenitalHeart Surgery, University of Texas HealthScience Center at San Antonio
Elizabeth McNally, MD, PhD Director, Center for Genetic Medicine,Northwestern University
Laxmi Mehta, MD, FACC Member, ACC Board of Governors Steering CommitteePresident, ACC Ohio Chapter
Director of the Women’s CardiovascularHealth Program, Associate Professor ofMedicine, Ohio State University WexnerMedical Center
Hena Patel, MD Member, ACC.org Editorial Board Fellow-in-Training, Rush University MedicalCenter
Felix Sogade, MD, FACC Chair, Association of Black Cardiologists Georgia Arrhythmia Consultants
Mary Norine Walsh, MD, FACC ACC President 2017–2018 Medical Director, Heart Failure and CardiacTransplantation, St. Vincent Heart Center
Roberta Williams, MD, MACC Former Member, ACC Board of Trustees Professor and Chair Emerita of Pediatrics,University of Southern California, Schoolof Medicine
Clyde Yancy, MD, FACC Past President, American Heart Association Vice Dean for Diversity and Inclusion, Chief ofCardiology, and Magerstadt Professor,Northwestern University Medical School
Cathleen Gates ACC Chief Operating Officer and Executive VicePresident
Stephanie Mitchell ACC Staff Liaison, Task Force on Diversity
Douglas et al. J A C C V O L . 7 0 , N O . 1 2 , 2 0 1 7
Leadership Page S E P T E M B E R 1 9 , 2 0 1 7 : 1 5 2 5 – 9
1528
ntinuous improvement programs within the ACCaccountable execution.
forObjective 3: Engage and leverage all available talent
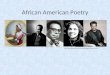
providing value to under-represented groupscardiology across the “career life-span,” fromsuring a deep pipeline to recruitment, retention,d leadership development.These objectives are illustrated in Figure 3.
NEXT STEPS
The ACC Diversity Task Force will continue tomeet regularly throughout the summer and fallto further refine and prioritize its recommendations;add specific tactics; and derive more robust esti-mates of feasibility, impact, and expense. The finalrecommendations will be presented to the Board ofTrustees in January 2018. With the extraordinary

FIGURE 3 Central Illustration of the ACC Task Force on Diversity
Key objectives from the interim report of the ACC Task Force on Diversity to the Board of Trustees.
J A C C V O L . 7 0 , N O . 1 2 , 2 0 1 7 Douglas et al.S E P T E M B E R 1 9 , 2 0 1 7 : 1 5 2 5 – 9 Leadership Page
1529
work of the Task Force, the ACC can envision afuture College and specialty of cardiology that ismore diverse and inclusive, and thus more able toserve our mission.
ADDRESS FOR CORRESPONDENCE: Dr. Mary NorineWalsh, American College of Cardiology, 2400 NStreet NW, Washington, DC 20037. E-mail:[email protected].
RE F E RENCE S
1. Catalyst. Why diversity matters. Available at:http://www.catalyst.org/system/files/why_diversity_matters_catalyst_0.pdf. Accessed August 3,2017.
2. Brotherton SE, Etzel SI. Graduate medicaleducation, 2015-2016. JAMA 2016;316:2291–310.
3. Merchant JL, Omary MB. Underrepresentationof underrepresented minorities in academicmedicine: the need to enhance the pipeline andthe pipe. Gastroenterology January 2010;138:19–26.e3.
4. Lewis SJ, Mehta LS, Douglas PS, et al., forthe American College of Cardiology Women
in Cardiology Leadership Council. Changesin the professional lives of cardiologistsover 2 decades. J Am Coll Cardiol 2017;69:452–62.
5. Center for Workforce Studies, Association ofAmericanMedical Colleges. 2016physician specialtydata report. Available at: https://www.aamc.org/data/workforce/reports/458712/1-3-chart.html.Accessed August 3, 2017.
6. Center for Workforce Studies, Association ofAmerican Medical Colleges. 2008 physicianspecialty data. Available at: http://www.aamc.org/download/47352/data/specialtydata.pdf. AccessedAugust 7, 2017.
7. American Association of Colleges of Nursing.Missingpersons:minorities in thehealthprofessions:a report of the Sullivan Commission on Diversity inthe Healthcare Workforce. Available at: https://www.aamc.org/download/47352/data/specialtydata.pdf. Accessed August 23, 2017.
8. Xierali IM, Castillo-Page L, ZhangK, Gampfer KR,Nivet MA. AM last page: the urgency of physicianworkforce diversity. Acad Med 2014;89. 1192–52.
9. ACC’s Board of Trustees’ Environmental Scan-ning Work Group (ESWG) Members, Laslett L1,Anderson HV, et al. American College of Cardiol-ogy: Environmental Scanning Report Update 2015.J Am Coll Cardiol 2015;66 19 Suppl:D1–44.