Embed Size (px)
Citation preview

© 2011 Pearson Education, Inc.
Module 7.8: Fontanelles
• Fontanelles
• Large fibrous areas between cranial bones of infants and small children
• Ease passage of head through birth canal
• Allow for cranial growth to keep pace with brain growth and later fetal stages
• Over time, fontanelles are replaced with sutures
• Occipital, sphenoidal, and mastoid fontanelles disappear a month or two after birth
• All fontanelles replaced before age 5 when brain stops growing
© 2011 Pearson Education, Inc.Figure 7.8 3
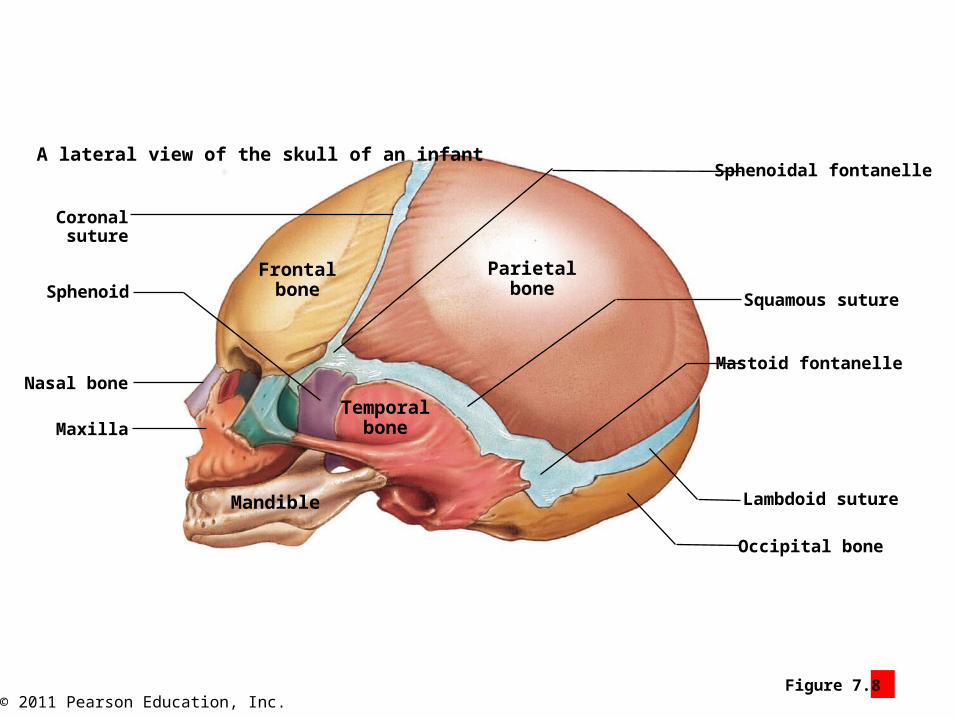
A lateral view of the skull of an infant
Parietalbone
Frontalbone
Temporalbone
Coronalsuture
Sphenoid
Nasal bone
Maxilla
Mandible
Occipital bone
Lambdoid suture
Sphenoidal fontanelle
Mastoid fontanelle
Squamous suture

© 2011 Pearson Education, Inc.
Module 7.8: Fontanelles
• Fontanelles
• Anterior
• Largest fontanelle
• At intersection of frontal, sagittal, and coronal sutures
• Sphenoidal
• Junction of squamous and coronal sutures
• Mastoid
• Junction of squamous and lambdoid sutures
• Occipital
• Junction of lambdoid and sagittal sutures

© 2011 Pearson Education, Inc.Figure 7.8 1
The anterior fontanelle (“soft spot”) and associated sutures in theskull of an infant
Rightparietal
bone
Leftparietal
bone
Sagittal suture
Anterior fontanelle
Coronal suture
Frontal suture
Frontal bone
Frontal suture

© 2011 Pearson Education, Inc.Figure 7.8 2
Sagittal suture
Rightparietal
bone
Leftparietal
bone
Lambdoid suture
Occipital fontanelle
Occipital bone
The occipital fontanelle and associated suturesin a posterior view of the skull of an infant

© 2011 Pearson Education, Inc.Figure 7.8 4
Frontal suture
A superior view of the skull of an infant
Frontalbone
Parietalbone
Frontalbone Parietal
boneCoronal suture
Anterior fontanelleSagittal suture Occipital fontanelle
Occipital bone
Lambdoid suture
What purposes do fontanelles serve

© 2011 Pearson Education, Inc.
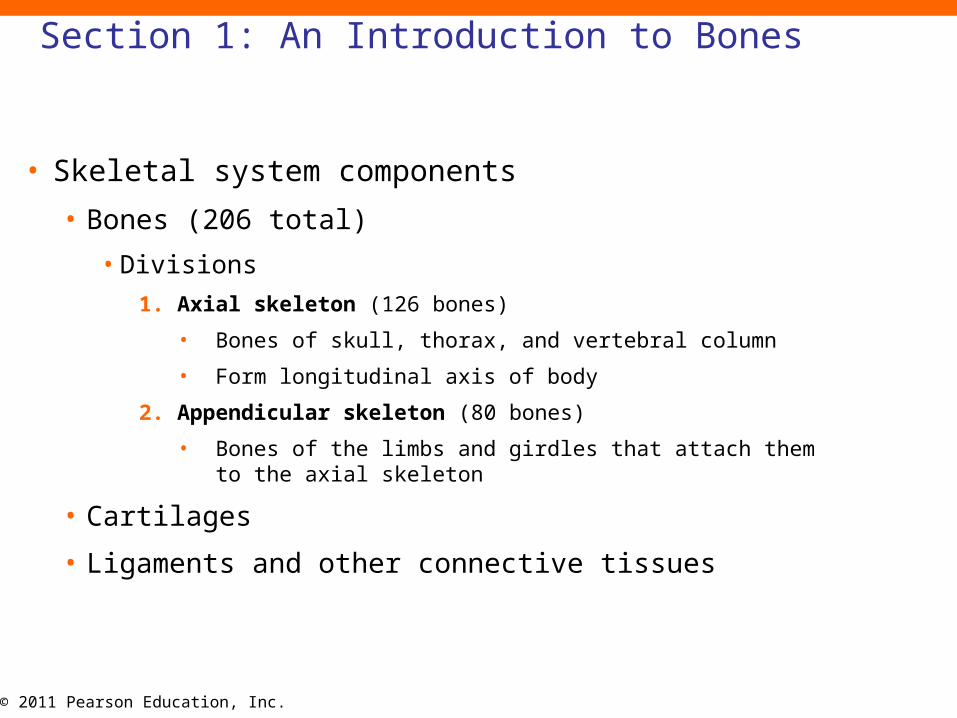
Section 1: An Introduction to Bones
• Learning Outcomes
• 6.1 Classify bones according to their shapes, identify the major types of bone
markings, and explain the functional significance of surface features.
• 6.2 Identify the parts of a typical long bone, and describe its internal
structures.
© 2011 Pearson Education, Inc.
• Skeletal system components
• Bones (206 total)
• Divisions
1. Axial skeleton (126 bones)
• Bones of skull, thorax, and vertebral column
• Form longitudinal axis of body
2. Appendicular skeleton (80 bones)
• Bones of the limbs and girdles that attach them to the axial skeleton
• Cartilages
• Ligaments and other connective tissues
Section 1: An Introduction to Bones

© 2011 Pearson Education, Inc.Figure 6 Section 1 1
Axial Skeleton(126 Bones)
The axial skeletonconsists of thebones of the skull,thorax, and vertebralcolumn. Theseelements form thelongitudinal axis ofthe body.
The adult skeletalsystem, which can bedivided into the axialskeleton and theappendicular skeleton
The appendicularskeleton includesthe bones of thelimbs and thepectoral and pelvicgirdles that attachthe limbs to theaxial skeleton.
AppendicularSkeleton (80 Bones)

© 2011 Pearson Education, Inc.
• Functions of the skeletal system
• Support (support for body, attachment for soft tissues)
• Storage of minerals (calcium and phosphate)
• Calcium most abundant mineral in body (~2–4 lb)
• 98% stored in bones
• Blood cell production (all formed elements of blood)
• Protection (delicate tissues and organs surrounded by bone)
• Leverage (act as levers with skeletal muscles to move body)
Section 1: An Introduction to Bones

© 2011 Pearson Education, Inc.
Module 6.1: Bone classification
• Six categories based on shape
1. Flat bones
• Thin, roughly parallel surfaces
• Examples: cranial bones, sternum
2. Sutural bones (Wormian bones)
• Irregular bones formed between cranial bones
• Number, size, and shape vary
3. Long bones
• Relatively long and slender
• Examples: various bones of the limbs

© 2011 Pearson Education, Inc.
• Six categories based on shape (continued)
4. Irregular bones
• Complex shapes
• Examples: vertebrae, bones of pelvis, facial bones
5. Sesamoid bones
• Small, flat, and somewhat shaped like sesame seed
• Develop in tendons of knee, hands, and feet
• Individual variation in location and number
6. Short bones
• Small and boxy
• Examples: bones of the wrist (carpals) and ankles (tarsals)
Module 6.1: Bone classification

© 2011 Pearson Education, Inc.
• Bone surface features
• Also known as bone markings
• External and internal features related to functions!!!!
• Elevations/projections for tendon and ligament attachment
• Depressions/grooves/tunnels for blood vessels or nerves to lie alongside or penetrate
Module 6.1: Bone classification

© 2011 Pearson Education, Inc.
• Skull surface features
• Canal or meatus (large passageway)
• Process (projection or bump)
• Sinus (chamber within bone, usually filled with air)
• Foramen (small rounded passageway)
• Fissure (elongated cleft or gap)
Module 6.1: Bone classification
© 2011 Pearson Education, Inc.
• Humerus surface features
• Head (expanded proximal end that forms part of joint)
• Tubercle (small, rounded projection)
• Sulcus (deep, narrow groove)
• Tuberosity (small, rough projection; may occupy broad area)
• Diaphysis (shaft; elongated body)
• Trochlea (smooth, grooved articular process)
• Condyle (smooth, rounded articular process)
Module 6.1: Bone classification

© 2011 Pearson Education, Inc.
• Femur surface features
• Trochanter (large, rough projection)
• Head
• Neck (narrow connection between head and diaphysis)
• Diaphysis
• Facet (small, flat articular surface)
• Condyle
Module 6.1: Bone classification
© 2011 Pearson Education, Inc.
• Pelvis surface features
• Crest (prominent ridge)
• Fossa (shallow depression or recess)
• Line (low ridge; more delicate than crest)
• Spine (pointed or narrow process)
• Ramus (extension that makes angle with rest of structure)
Module 6.1: Bone classification

© 2011 Pearson Education, Inc.
Module 6.2: Typical long bone structure
• Long bone features
• Epiphysis (expanded ends)
• Consist largely of spongy bone (trabecular bone)• Network of struts and plates
• Resists forces from various directions and directs body weight to diaphysis and joints
• Outer covering of compact bone• Strong, organized bone
• Articular cartilage• Covers portions of epiphysis that form articulations
• Avascular and receives resources from synovial fluid

© 2011 Pearson Education, Inc.
• Long bone features Metaphysis (connects epiphysis to shaft)
• Diaphysis (shaft)
• Contains medullary cavity (marrow cavity)
• Filled with marrow
• Red bone marrow (red blood cell production)
• Yellow bone marrow (adipose storage)
Bone vasculatureGrowth and maintenance requires extensive blood supplyVascular features
Nutrient artery/vein (commonly one each/bone)Nutrient foramen (tunnel providing access to marrow cavity)Also supplies osteons of compact bone with blood

© 2011 Pearson Education, Inc.Figure 6.2 1 - 2
Coronal sections through a right femur, showing the boundaries of a long bone’s majorregions, plus the bone’s internal organization and how it distributes the forces appliedto the bone
The epiphysis(e-PIF-i-sis) is anexpanded areafound at each endof the bone.
The metaphysis(me-TAF-i-sis; meta,between) is a narrowzone that connectsthe epiphysis to theshaft of the bone.
The diaphysis(shaft) is long andtubular.
The epiphysis consistslargely of spongy bone,also called trabecularbone. Spongy boneconsists of an open networkof struts and plates thatresembles latticework witha thin covering, or cortex, ofcompact bone.
The medullary cavity(medulla, innermost part), ormarrow cavity, is a spacewithin the hollow shaft. Inlife, it is filled with bonemarrow, a highly vasculartissue. Red bone marrowis highly vascular andinvolved in the productionof blood cells. Yellowbone marrow is adiposetissue important in thestorage of energy reserves.
Compressionon medial
side of shaft
Tensionon lateral
side ofshaft
Body weight(applied force)
The wall of the diaphysisconsists of a layer ofcompact bone.
Metaphysis
Epiphysis

© 2011 Pearson Education, Inc.Figure 6.2 3
A longitudinal section of the humerus, showing the extensive|network of blood vessels in long bones
Epiphyseal arteryand vein
Metaphysis
An articular cartilage covers portions ofthe epiphysis that articulate with other bones. The cartilage is avascular, and itrelies primarily on diffusion from thesynovial fluid to obtain oxygen andnutrients and eliminate wastes.
The metaphyseal artery (red) andmetaphyseal vein (blue) carry blood toand from the area of the metaphysis and tothe epiphysis through epiphyseal arteriesand veins.
Periosteum
Compactbone
Medullarycavity
Metaphysis
Metaphysealartery and vein
Most bones have only onenutrient artery (shown inred) and one nutrient vein(shown in blue), but a fewbones, including the femur,have more than one of each.
A nutrient foramen is a tunnel that penetrates thediaphysis and providesaccess for the nutrient arteryand/or vein. Branches ofthese large vessels supplythe osteons of thesurrounding compact bonebefore entering andsupplying the tissues of themedullary cavity.

© 2011 Pearson Education, Inc.

© 2011 Pearson Education, Inc.
• Bone Layers: Periosteum, Compact Bone, Medullary Cavity
• Periosteum features
• Smaller blood vessels (supply superficial osteons)
• Lymphatic vessels (collect lymph from bone and osteons)
• Sensory nerves (innervate diaphysis, medullary cavity, and epiphyses)
Module 6.2: Typical long bone structure

© 2011 Pearson Education, Inc.
Module 6.2 Review
a. List the major parts of a long bone.
b. Describe the function of the medullary cavity.
c. If articular cartilage is avascular, how is it nourished?

© 2011 Pearson Education, Inc.
• Four bone cell types
1. Osteocytes (osteo-, bone + cyte, cell)
• Mature bone cells that cannot divide
• Most numerous bone cell type
• Maintain protein and mineral content of adjacent matrix
• Occupy lacunae (pocket)• Separated by layers of matrix (lamellae)
• Connected with canaliculi
2. Osteoblasts (blast, precursor)Produce new bony matrix (osteogenesis or
ossification)Become osteocytes once surrounded by bony matrix

© 2011 Pearson Education, Inc.Figure 6.3 1 - 2
The layers of matrixare called lamellae(lah-MEL-lē; singular,lamella, a thin plate).
The structures of osteocytes and osteoblasts within along bone
Osteocytes account for mostof the cell population in bone.Each osteocyte occupies alacuna, a pocket sandwichedbetween layers of matrix.Osteocytes cannot divide,and a lacuna never containsmore than one osteocyte.
Narrow passagewayscalled canaliculipenetrate the lamellae,radiating through thematrix and connectinglacunae to one anotherand to various bloodvessels that supplynutrients.
Osteoblast
Osteoid

© 2011 Pearson Education, Inc.
3. Osteoprogenitor cells (progenitor, ancestor)
• Mesenchymal (stem) cells that produce cells that differentiate into osteoblasts
• Important in fracture repair
• Locations
• Inner lining of periosteum
• Lining endosteum in medullary cavity
4. Osteoclasts (clast, to break)Remove and remodel bone matrixGiant cells with 50+ nuclei
Derived from same stem cells as macrophagesRelease acids and proteolytic enzymes to dissolve matrix
and release stored minerals = Osteolysis (lysis, loosening)

© 2011 Pearson Education, Inc.Figure 6.3 3 - 4
Endosteum
Osteoprogenitor cell
Osteoclast
The structures of osteocytes and osteoblastswithin a long bone

© 2011 Pearson Education, Inc.
Module 6.3: Bone tissue
• Bone matrix
• Collagen fibers account for ~1/3 bone weight
• Provide flexibility
• Calcium phosphate (Ca3(PO4)2) accounts for ~2/3 bone weight
• Interacts with calcium hydroxide (Ca(OH)2) to form crystals of hydroxyapatite (Ca10(PO4)6(OH)2) salts
• Incorporates other salts (calcium carbonate, CaCO3) and ions (Na, Mg2, F)
• Provides strength

© 2011 Pearson Education, Inc.Figure 6.3 5

© 2011 Pearson Education, Inc.
Module 6.3 Review
a. Define osteocyte, osteoblast, osteoprogenitor cell, and osteoclast.
b. How would the compressive strength of a bone be affected if the ratio of collagen to hydroxyapatite increased?
c. If osteoclast activity exceeds osteoblast activity in a bone, what would be the effect on the bone?

© 2011 Pearson Education, Inc.
Module 6.4: Compact and spongy bone
• Compact bone
• Functional unit is osteon
• Organized concentric lamellae around a central canal
• Osteocytes (in lacunae) lie between lamellae
• Central canal contains small blood vessels
• Canaliculi connect lacunae with each other and central canal
• Strong along its length

© 2011 Pearson Education, Inc.Figure 6.4 1 - 2
The structure of compact bone, as shown inthe shaft of a long bone
Capillary and venule
Central canal
Concentric lamellae
Canaliculi radiatingthrough the lamellaeinterconnect the lacunaeof the osteons with oneanother and with thecentral canal.
Endosteum
Periosteum
Central canal
Vein
Artery
Osteon
Compact bone LM x 375
The osteocytes occupy lacunae that liebetween the lamellae. In preparing thismicrograph, a small piece of bone wasground down until it was thin enough totransmit light. In this process, the lacunaeand canaliculi are filled with bone dust, andthus appear black.
Circumferentiallamellae
Interstitiallamellae
Central canal
Perforating canal

© 2011 Pearson Education, Inc.
Module 6.4: Compact and spongy bone
• Typical long bone organization
• Periosteum (outermost layer)
• Compact bone (outer bone tissue layer)
• Circumferential lamellae (circum-, around + ferre, to bear)
• Outer and inner surfaces of compact bone layer
• Interstitial lamellae
• Fill spaces between osteons
• Osteons
• Contain central canals (parallel to bone surface)
• Connected by perforating canals (perpendicular)
• Spongy bone (innermost layer)

© 2011 Pearson Education, Inc.
• Spongy bone
• Located where bones not heavily stressed or in many directions
• Lamellae form struts and plates (trabeculae) creating an open network
• Reduces weight of skeleton
• No blood vessels in matrix• Nutrients reach osteons through canaliculi open to
trabeculae surfaces
Module 6.4: Compact and spongy bone

© 2011 Pearson Education, Inc.Figure 6.4 3 – 4
Trabeculae ofspongy bone
Canaliculiopening on
surface
Endosteum Lamellae
The structure of spongy bone, as shown in the head of the femur

© 2011 Pearson Education, Inc.Figure 6.5 1
Increase in bone diameter resulting from appositional growth
Additional circumferentiallamellae are deposited, andthe bone continues toincrease in diameter.
Periosteum

© 2011 Pearson Education, Inc.Figure 6.5 2
Enlargement of the medullary cavity with increased bone diameterresulting from appositional growth
Bone matrix is removedby osteoclasts
Bone deposited bysuperficial osteoblastsInfant Child Young adult Adult

© 2011 Pearson Education, Inc.Figure 6.5 4
Structure of the endosteum
Endosteum
Osteoclast
Circumferential lamella
Osteocyte
Osteoprogenitorcell
Osteoid
Osteoblast

© 2011 Pearson Education, Inc.
Module 6.6: Endochondral ossification
• Initial bone formation in embryo begins with cartilage
• Replaced by bone through endochondral (endo-, inside + chondros, cartilage) ossification
• Uses cartilage as small model
• Bone grows in diameter and length
• Diameter growth involves appositional bone deposition
Animation: Early Endochondral Ossification

© 2011 Pearson Education, Inc.
• Steps of endochondral ossification
1. In shaft, chondrocytes enlarge and matrix ossifies
• Chrondrocytes die, leaving cavities within cartilage
2. Blood vessels grow around cartilage edge and osteoblasts form to create a superficial layer of bone
3. Blood vessels penetrate central region
• Allow entering fibroblasts to change into osteoblasts• Spongy bone produced (primary ossification center)
and spreads toward bone ends
Module 6.6: Endochondral ossification

© 2011 Pearson Education, Inc.
• Steps of endochondral ossification (continued)
4. Medullary cavity created as cartilage replaced by osseous tissue
• Bone grows in length and diameter
5. Secondary ossification centers form as capillaries and osteoblasts migrate into epiphyses
6. Epiphyses fill with spongy bone
• Only articular cartilage (on epiphyses) and epiphyseal cartilage (in metaphysis) remain
Module 6.6: Endochondral ossification

© 2011 Pearson Education, Inc.Figure 6.6 1 – 6
The process of endochondral ossification
Enlargingchondrocytes within
calcifying matrix
Hyaline cartilage
Epiphysis
Diaphysis
Boneformation
Bloodvessel
Medullarycavity
Primaryossificationcenter
Superficialbone
Spongybone
Medullarycavity
Metaphysis
Enlargement ofchondrocytes
Formation of superficiallayer of bone
Production of spongy bone ata primary ossification center
Further growth in lengthand diameter
Hyaline cartilage
Epiphysis
Metaphysis
Periosteum
Compactbone
Secondaryossification
center
Formation of secondaryossification centers
Formation of an epiphysealcartilage between epiphysis
and diaphysis
Articular cartilage
Spongybone
Epiphysealcartilage
Diaphysis

© 2011 Pearson Education, Inc.
• Steps of endochondral ossification (continued)
7. Bone grows in length at epiphyseal cartilage
• Chondrocytes actively produce more cartilage on epiphysis side
• Osteoblasts actively replace cartilage with bone on shaft side
• As long as both processes are equally active, bone lengthening continues• At puberty, hormones increase bone growth and epiphyseal
cartilage is replaced
• Leaves epiphyseal line in adults
Module 6.6: Endochondral ossification

© 2011 Pearson Education, Inc.Figure 6.6 6 – 7
Formation of an epiphysealcartilage between epiphysis
and diaphysis
Articular cartilage
Spongybone
Epiphysealcartilage
Diaphysis
Medullarycavity
Osteoblasts Osteoid
Epiphysealcartilage matrix
Cartilage cells undergoingdivision and secreting
additional cartilage matrix
The ossifying surface of anepiphyseal cartilage
LM x 250

© 2011 Pearson Education, Inc.
Module 6.6 Review
a. Define endochondral ossification.
b. In endochondral ossification, what is the original source of osteoblasts?
c. How could x-rays of the femur be used to determine whether a person has reached full height?

© 2011 Pearson Education, Inc.
Module 6.7: Intramembranous ossification
• Begins as mesenchymal (stem) cells differentiate into osteoblasts within embryonic or fibrous connective tissue
• Normally occurs in deeper layers of dermis
• = Dermal bones (or membrane bones)
• Examples:
• Roofing bones of skull
• Lower jaw
• Collarbone
• Sesamoid bones such as patella

© 2011 Pearson Education, Inc.
• Steps of intramembranous ossification
• Mesenchymal cells secrete osteoid matrix• Differentiate into osteoblasts
• Osteoid matrix becomes mineralized• Forms ossification center
• Bone grows out in small struts (spicules)
• Osteoblasts become trapped and mature into osteocytes• Mesenchymal cells produce more osteoblasts
• Blood vessels enter and become trapped in developing bone
Module 6.7: Intramembranous ossification

© 2011 Pearson Education, Inc.Figure 6.7 1 – 3
Osteocyte in lacunaBone matrix
Osteoblast
Osteoid
Embryonic connective tissue
Mesenchymal cell
The process of intramembranous ossification
Bloodvessel
Osteocytesin lacunae
Osteoblastlayer
Blood vessel Osteoblasts Spicules Blood vessels
LM x 32 LM x 32
The growth of developing bone outward from the ossificationcenter in small struts called spicules
The growth and entrapment ofblood vessels within developingbone
Spongy bone, the initial form ofintramembranous bone

© 2011 Pearson Education, Inc.
• Further membranous bone development
• Spongy bone formed initially
• Remodeling around blood vessels forms osteons of compact bone
• Periosteum forms, lined with osteoblasts
• Begins at approximately 8th week of embryonic development
Module 6.7: Intramembranous ossification

© 2011 Pearson Education, Inc.Figure 6.7 4
Futurehip bone
Primaryossification
centers of thelong bones ofthe lower limb
Intramembranousossification centers
that produce theroofing bones of
the skull
Long bonesof the limbs
10 weeks of development Flat bonesof the skull
16 weeks of development
The extent of intramembranous andendochondrial ossification occurring between10 and 16 weeks of development

© 2011 Pearson Education, Inc.
Section 2: Bone Physiology
• Learning Outcomes
• 6.9 Discuss the effects of hormones on bone development, and explain the
homeostatic mechanisms involved.
• 6.10 CLINICAL MODULE Describe the types of fractures, and explain how
fractures heal.

© 2011 Pearson Education, Inc.
• Bones are important mineral reservoirs
• Mostly calcium but other ions as well
• Calcium
• Most abundant mineral in body
• 1–2 kg (2–4 lb)
• ~99% deposited in skeleton
• Variety of physiological functions
• Concentration variation greater than 30–35% affects neuron and muscle function
• Normal daily fluctuations are <10%
Section 2: Bone Physiology

© 2011 Pearson Education, Inc.Figure 6 Section 2 1
Composition of Bone Bone Contains …
99% of the body’s calcium
4% of the body’s potassium
35% of the body’s sodium
50% of the body’s magnesium
80% of the body’s carbonate
99% of the body’s phosphate
Calcium 39%
Potassium 0.2%
Sodium 0.7%
Magnesium 0.5%
Carbonate 9.8%
Phosphate 17%
67%Total inorganiccomponents
Organiccompounds
(mostly collagen)33%
The importance of bones as mineral reservoirs

© 2011 Pearson Education, Inc.
• Calcium (continued)
• Levels controlled by activities of:
• Intestines
• Absorb calcium and phosphate. Under hormonal control
• Bones
• Release Calcium in blood stream or Lay down calcium to make new bone. (Remodeling by osteoblasts and osteoclasts)
• Kidneys
• Calcium and phosphate loss in urine. Under hormonal control
Section 2: Bone Physiology

© 2011 Pearson Education, Inc.
Module 6.9: Hormonal control of calcium
• Factors that increase blood calcium levels
• Parathyroid hormone (from parathyroid glands)
• Responses
• Bones: Stimulates bone cells (osteoclasts) to release calcium
• Intestines: Increases calcium absorption
• Kidneys: Causes calcium reabsorption in kidneys

© 2011 Pearson Education, Inc.
• Factors that decrease blood calcium levels
• Calcitonin from thyroid gland C cells
• Responses
• Bone: decrease osteoclast activity (Bone cells keep calcium in bone therefore blood calcium levels are low)
• Intestines: decreased absorption
• Kidneys: inhibits calcium reabsorption
Module 6.9: Hormonal control of calcium

© 2011 Pearson Education, Inc.
• As a calcium reserve, skeleton has primary role in calcium homeostasis
• Has direct effect on shape and length of bones
• Release of calcium into blood weakens bones
• Deposit of calcium salts strengthens bones
Module 6.9: Hormonal control of calcium

© 2011 Pearson Education, Inc.
Module 6.9 Review
a. Identify the hormones involved in stimulating and inhibiting the release of calcium ions from bone matrix.
b. What effect would increased PTH secretion have on blood calcium levels?
c. How does calcitonin lower the calcium ion concentration of blood?

© 2011 Pearson Education, Inc.
Module 6.10 CLINICAL MODULE: Fractures
• Fracture
• Crack or break due to extreme mechanical stress
• Most heal as long as blood supply and cellular parts of periosteum and endosteum survive

© 2011 Pearson Education, Inc.
• Steps of fracture repair
1. Large blood clot (fracture hematoma) develops
2. Calluses form
• Internal callus (network of spongy bone uniting inner edges)
• External callus (cartilage and bone stabilizes outer edges)
Module 6.10 CLINICAL MODULE: Fractures

© 2011 Pearson Education, Inc.
Module 6.10 CLINICAL MODULE: Fractures
Animation: Steps in the Repair of a Fracture
• Steps of fracture repair (continued)
3. Calluses replaced and dead bone removed
• Spongy bone unites broken ends
• Cartilage of external callus replaced by bone
4. Remodeling of healed bone

© 2011 Pearson Education, Inc.Figure 6.10 1
The events in the repair of a bone fracture
Spongy boneof internal
callus
Cartilageof external
callus
Fracturehematoma
Deadbone
Bonefragments
Spongy bone ofexternal callus
Periosteum
Internalcallus
Externalcallus
Externalcallus
Formation of a fracturehematoma
Formation of an internalcallus and an externalcallus
Replacement of thecartilage of the externalcallus with bone
Remodeling overtime andcompletion ofrepair

© 2011 Pearson Education, Inc.Figure 6.10 5
Transversefractures, such asthis fracture of theulna, break a boneshaft across its longaxis.
Types of Fractures
Spiral fractures,such as thisfracture of thetibia, are producedby twistingstresses thatspread along thelength of the bone.
Displaced fracturesproduce new andabnormal bone ar-rangements;nondisplacedfractures retain thenormal alignment ofthe bones orfragments.
Compression fracturesoccur in vertebraesubjected to extremestresses, such as thoseproduced by the forces thatarise when you land on yourseat in a fall.
In a greenstickfracture, such as thisfracture of the radius,only one side of theshaft is broken, andthe other is bent. Thistype of fracturegenerally occurs inchildren, whose longbones have yet toossify fully.
Comminutedfractures, such asthis fracture of thefemur, shatter theaffected area into amultitude of bonyfragments.
Epiphyseal fractures, such as thisfracture of the femur, tend to occur wherethen bone matrix is undergoing calcificationand chondrocytes are dying. A cleantransverse fracture along this line generallyheals well. Unless carefully treated, fracturesbetween the epiphysis and the epiphysealcartilage can permanently stop growth atthis site.
A Pottfracture occursat the ankle andaffects bothbones of the leg.
A Colles fracture, abreak in the distalportion of the radius,is typically the resultof reaching out tocushion a fall.