Embed Size (px)
Citation preview

NCPO LaTrobe University
PREPARING AMPUTEE ATHLETES:
THE AUSTRALIAN APPROACH
compiled by Joellen McPhan

Page i
TABLE OF CONTENTS
TABLE OF FIGURES.............................................................................................. VI
ACKNOWLEDGEMENTS ....................................................................................VII
INTRODUCTION........................................................................................................1
SECTION 1 – BACKGROUND TO AMPUTEE RUNNING .....2
CHAPTER 1 - BIOMECHANICS OF AMPUTEE RUNNING............................3
RUNNING............................................................................................................3
TEMPEROSPATIAL CHARACTERISTICS......................................................4
KINEMATICS .....................................................................................................5
JOINT MOMENTS..............................................................................................8
ENERGETICS......................................................................................................8
CHAPTER 2 - AMPUTEE SPECIFIC CONSIDERATIONS.............................12
PHYSICAL CONSIDERATIONS.....................................................................12
PROSTHETIC CONSIDERATIONS ................................................................13
PSYCHOLOGICAL CONSIDERATIONS .......................................................13
CHAPTER 3 - AMPUTATION LEVEL CONSIDERATIONS............................14
CONGENITAL AND ACQUIRED AMPUTEES.............................................14
UPPER EXTREMITY AMPUTEES .................................................................14
THROUGH KNEE AMPUTEES.......................................................................15
ABOVE KNEE AMPUTEES.............................................................................15

Page ii
CHAPTER 4 - THE MULTI-DISCIPLINARY TEAM APPROACH .................17
DOCTOR............................................................................................................18
PHYSIOTHERAPIST ........................................................................................19
PROSTHETIST..................................................................................................19
COACH ..............................................................................................................19
SECTION 2 - THE MULTI-DISICPLINARY TEAM...................20
CHAPTER 5 - THE ROLE OF THE PHYSIOTHERAPIST .............................21
INITIAL ASSESSMENT...................................................................................21
GAIT ANALYSIS ............................................................................................22
PHYSICAL ASSESSMENT.............................................................................22
• Residual Limb.......................................................................................23
• Posture .................................................................................................23
• Strength ................................................................................................23
• Range Of Motion ..................................................................................24
• Core And Joint Stability And Activation ..............................................24
PHYSICAL UPGRADING................................................................................25
GAIT RE-EDUCATION.................................................................................25
CORE PROGRAM .........................................................................................26
MODIFIED GYM PROGRAM.......................................................................27
POOL WORK.................................................................................................29
SPORT SPECIFIC TRAINING ......................................................................29
ONGOING MANAGEMENT............................................................................29
LIASE WITH TEAM.......................................................................................29
INJURY PREVENTION AND MANAGEMENT ............................................29
ELIGIBILITY FOR A RUNNING PROSTHESIS............................................30
COMMON EXERCISES AND PROGRAMS...................................................30

Page iii
CHAPTER 6 - THE ROLE OF THE PROSTHETIST........................................31
INITIAL ASSESSMENT...................................................................................31
RUNNING PROSTHESIS .................................................................................32
BELOW-KNEE COMPONENTRY.................................................................32
• Foot ..................................................................................................32
• Liner .................................................................................................36
• Socket type .......................................................................................36
• Suspension........................................................................................38
• Trimlines ..........................................................................................40
BELOW KNEE ALIGNMENT........................................................................40
Below Knee Bench Alignment ...................................................................41
Below Knee Static Alignment ....................................................................42
Below Knee Dynamic Alignment...............................................................42
ABOVE KNEE COMPONENTRY..................................................................42
• Foot ..................................................................................................43
• Socket ...............................................................................................44
• Liner/suspension ..............................................................................45
• Knee Units........................................................................................46
ABOVE KNEE ALIGNMENT ........................................................................47
Above Knee Bench Alignment ...................................................................47
Above Knee Static Alignment ....................................................................48
Above Knee Dynamic Alignment...............................................................48
EDUCATION.....................................................................................................49
CHAPTER 7 - THE ROLE OF THE COACH .....................................................51
INITIAL ASSESSMENT...................................................................................52
DEVELOPING A TRAINING PROGRAM......................................................54
INDIVIDUALISM ..........................................................................................54
INJURY PREVENTION AND MANAGEMENT ............................................55
COMMUNICATION ......................................................................................55
SPORT SPECIFIC FITNESS .........................................................................56
SPORT SPECIFIC SKILL DEVELOPMENT ................................................57

Page iv
MODIFICATIONS TO EXERCISES................................................................60
STRENGTHENING PROGRAMS..................................................................60
PLYOMETRIC EXERCISES ..........................................................................60
SECTION 3 - TROUBLE SHOOTING .................................................62
CHAPTER 8 - INJURIES.......................................................................................63
RISK FACTORS................................................................................................63
INJURY MANAGEMENT................................................................................63
INJURY PREVENTION....................................................................................64
COMMON INJURIES .......................................................................................65
CHAPTER 9 - GAIT ANALYSIS: DEVIATIONS AND MANAGEMENT......69
GAIT ANALYSIS..............................................................................................69
PHYSIOTHERAPIST .....................................................................................70
PROSTHETIST ..............................................................................................71
COACH ..........................................................................................................72
GAIT DEVIATIONS .........................................................................................73
GENERAL DEVIATIONS ..............................................................................73
BELOW KNEE SPECIFIC DEVIATIONS .....................................................86
ABOVE KNEE SPECIFIC DEVIATIONS .....................................................87
REFERENCES...........................................................................................................88

Page v
SECTION 4 - APPENDICIES.....................................................................91
APPENDIX I – AMPUTEE CLASSIFICATIONS.................................................92
APPENDIX IIA – IMPAIRMENT SPECIFIC SCREENING FORM .................94
APPENDIX IIB – EXPLANTORY NOTES............................................................98

Page vi
TABLE OF FIGURES
Figure 1 - The Running Gait.. ........................................................................................4
Figure 2 - Joint Angle Times During Able-Bodied Running. .......................................5
Figure 3 - Knee Joint Angular Kinematics ....................................................................6
Figure 4 - Energy Absorption During Stance ..............................................................10
Figure 5 - Energy Generation During Stance ..............................................................11
Figure 6 - A Below Elbow Running Prosthesis ...........................................................15
Figure 7 - The Multi-Disciplinary Team .....................................................................18
Figure 8 - Gait Re-Education.......................................................................................26
Figure 9 - Core Strengthening......................................................................................27
Figure 10 - Modified Gym Program ............................................................................28
Figure 11 - Modified Gym Program ............................................................................28
Figure 12 - The Flex-Sprint III ....................................................................................33
Figure 13 - The Flex-Sprint III and Attachments ........................................................34
Figure 14 - Positioning and Attaching the Lamination Connector ..............................35
Figure 15 - Hydrostatic Sockets...................................................................................37
Figure 16 – Running Prosthesis Compenentry ............................................................39
Figure 17 - Running Prosthesis Componentry.............................................................39
Figure 18 - Bench Alignment of the Flex-Sprint III. ...................................................41
Figure 19 - The Flex-Sprint Series...............................................................................43
Figure 20 - The Quadrilateral and Ischial Containment Sockets.. ...............................44
Figure 21 - The Flex-Sprint I and Attachments ...........................................................46
Figure 22 - Bench Alignment of an Above Knee Running Prosthesis ........................47
Figure 23 - Strength Testing ........................................................................................53
Figure 24 - Relative Strength Training ........................................................................56
Figure 25 - Bend Running............................................................................................58
Figure 26 - Take-Off....................................................................................................59

Page vii
ACKNOWLEDGEMENTS
Harvey Blackney - Advanced Prosthetic Centre
David Howells – prosthetist, Advanced Prosthetic Centre
Cathy Howells – consultant physiotherapist, Advanced Prosthetic Centre
Colin Wright – coach of a number of successful Paralympians
Stephen Wilson – dual gold medallist and world record holder, Sydney 2000
Paralympic Games
Chris Nunn - head coach athletes with disabilities, Australian Institute of Sport
Dr Tim Bach – supervisor, Head of NCPO, Latrobe University.
Les Barnes – co-supervisor, NCPO, Latrobe University.
Staff at the Advanced Prosthetic Centre, Sydney
Fellow honours students
Sydney Athletics Centre, Homebush Bay

Page 1
INTRODUCTION Australian amputee runners have been extremely successful in international
competition. The training approach taken in the preparation of the athletes has been
identified as a major contributor in achieving such success. The ability to obtain
information relating to the Australian methods of training amputee runners is limited.
There are no current publications that investigate or discuss the training approach of
the Australian amputee track team.
The success of the Australian amputee track team was demonstrated at the
Sydney 2000 Paralympic games. As a result of the increased exposure of the abilities
and successes of amputee athletes it is anticipated this will inspire others to develop
their sporting skills. Increased participation provides a higher competition standard
and as a result produces more competitive athletes. It also increases the demand for
improvements in prosthetic and other disabled sport technology and increases the
demand for amputee running related resources, which are already limited.
The Australian method of training amputee athletes involves a multi-
disciplinary team approach. This provides expertise and specialist knowledge in every
aspect relating to amputee running. The multi-disciplinary team approach is
applicable in training disabled athletes in general, although this manual demonstrates
the approach in relation to amputee running.
The manual is aimed to educate and guide the multi-disciplinary team on ways
of managing amputee runners when they initially present. The manual includes sports
specific knowledge (biomechanics of amputee running), discusses the roles of each
member of the multi-disciplinary team and includes a trouble-shooting guide that
reviews gait deviations and amputee specific injuries. Case studies are also included
to provide examples of successful coaching and physiotherapeutic programs and
prosthetic management. The manual addresses the management of athletes at the early
stages of running, to the more experienced, elite athlete. It also caters for all levels of
amputation, with the main emphasises throughout the manual being the multi-
disciplinary team approach.
The manual will provide an updateable resource for people interested in any
aspects relating to amputee running. It provides guidelines to assessing athletes, the
basic principles of designing individual amputee specific training programs and
options for prosthetic prescription.

Page 2
SECTION 1
BACKGROUND TO AMPUTEE
RUNNING
BIOMECHANICS OF AMPUTEE RUNNING
AMPUTEE SPECIFIC CONSIDERATIONS
AMPUTATION LEVEL CONSIDERATIONS
THE MULTI-DISCIPLINARY TEAM APPROACH
It is important for the members of the multi-disciplinary team to have good
knowledge of the biomechanics of running as it provides an understanding of the
limitations and adaptations necessary to enable amputees to run. This section provides
a brief summary of below knee and above knee amputee running, discussing the
temperospatial characteristics, kinematics, joint moments, energetics and joint
powers.
This section also briefly discusses the amputee specific considerations that a
professional managing an amputee athlete should understand. This includes the
physical, prosthetic and psychological issues that the amputee faces.
The types of amputation (congenital and acquired) are reviewed as too the
basic considerations necessary for each amputation level. Finally, the multi-
disciplinary team is introduced as it forms the basis of the manual. The relationship
between the major contributors of the amputee running multi-disciplinary team (the
physiotherapist, prosthetist, coach and athlete) is identified.

Page 3
CHAPTER 1
BIOMECHANICS OF AMPUTEE RUNNING
Understanding the biomechanics of normal running is important in identifying
the limitations and compensations that occur during amputee running. Research is
further enhancing our understanding of the adaptations required of amputees to run
(Czerniecki, 1996). The adaptive processes of the amputee must coordinate prosthetic
limb motion with those of the intact limb. This increases the demand in muscle work
and increases the energy expenditure of amputee running gait (Sanderson and Martin,
1996). When discussing amputee running, it is important to distinguish between
swing and stance phases and the movement of the intact and the residual limbs.
The main biomechanical deficits of amputee running are insufficient power
generation at prosthetic push-off, increased impact forces on the intact limb and
interlimb asymmetry (Brouwer, Allard and Labelle, 1989; Smith, 1990; Czerniecki,
Gitter and Beck, 1996). Compensatory mechanisms are adopted to overcome these
limitations particularly on the intact limb during swing phase and the prosthetic limb
during stance phase (Czerniecki, 1996). It is important for each team member to
understand the biomechanics of running and the compensations and adaptations
employed to enable amputees to run as it influences the implementation of a training
program and the prosthetic prescription
RUNNING As a person increases their speed from walking to running, the proportion of
stance phase decreases, swing phase duration increases and double support is
eliminated. The running cycle consists of a stance phase and a swing phase, which
includes a period of flight where there is no contact with the ground (FIGURE 1). The
stance phase can be further divided into absorption and propulsion phases and the
swing phase into initial and terminal swing phases (Thordarson, 1997).

Page 4
Figure 1 - THE RUNNING GAIT. This figure illustrates the various positions of the body during
running gait at (A) take-off, (B) flight and (C) initial contact (as cited by Lees in Durward, Baer and
Rowe, 1999).
(A) (B) (C) (A)
TEMPEROSPATIAL CHARACTERISTICS The stride length, stride time and impact loads of the intact and prosthetic
limbs are common asymmetries (Macfarlane, Nielsen and Shurr, 1997). Interlimb
asymmetries result in an energy expensive gait compared to normal (Macfarlane,
Nielsen and Shurr, 1997).
In above knee prosthesis, excessive heel rise causes a delay in the forward
acceleration of the distal shank. This is a major contributor to interlimb asymmetry
and can cause a number of gait deviations (Sabolich, 1987). In an attempt to quicken
the follow through of the distal shank (foot) during running, the hop-skip method of
running was previously adopted by above knee runners. The hop-skip method
involves two intact stance phases to one prosthetic swing phase with a period of
double support (Mensch and Ellis, 1986). The feet are closer together at initial
contact and assist in decreasing the knee flexion moment and impact loads of the
intact limb at initial contact.
In recent years, through prosthetic componentry developments, particularly
knee units, has enabled above knee amputees to run with a more efficient step-over-
step style.

Page 5
KINEMATICS In able-bodied jogging, initial contact is with the heel. At heel contact,
dorsiflexion occurs and the foot pronates. Pronation and dorsiflexion, along with hip
and knee flexion, assists in absorbing impact loads (Thordarson, 1997). As speed
increases, initial contact occurs with the midfoot/forefoot. Consequently the foot is
plantarflexed at initial contact. The ankle then quickly dorsiflexes to reflect the
movement of the body over the foot and plantarflexes again for push-off (FIGURE 2)
(as cited by Lees in Durward, Baer and Rowe, 1999).
Figure 2 – JOINT ANGLE TIMES DURING ABLE-BODIED RUNNING. The ankle, knee and thigh
angle times during able-bodied running are shown below (as cited by Lees in Durward, Baer and Rowe,
1999).

Page 6
At initial stance during able-bodied running, the knee maintains a slightly
flexed position to absorb loads and assist in push-off. Alternatively, the transtibial
amputees often walk and run with a ‘locked-knee’ gait. This refers to a gait where the
amputee maintains their knee in extension or limits their knee flexion, particularly
during swing on the intact limb and initial –mid stance on the prosthetic limb (Miller,
1987; Sanderson and Martin, 1996). FIGURE 3 illustrates the limited flexion of the
prosthetic knee during initial-mid stance and the limited flexion of the intact knee
during swing.
Limited knee flexion on the prosthetic side occurs for a number of reasons.
Decreased quadriceps strength and manipulation of the knee joint moment to limit
knee flexion maintains the prosthesis in a vertical position. Maintenance of a vertical
position is an attempt to reduce the impact loads applied to the residual limb and is a
safety mechanism used to prevent the knee from collapsing (Brouwer, Allard and
Labelle, 1989; Sanderson and Martin, 1996).
Figure 3 - KNEE JOINT ANGULAR KINEMATICS. The knee angle during stride is illustrated for
‘normal’ (solid line), the intact (dotted line) and the prosthetic sides (broken line). Stance phase
comprises the first 40% of stride duration (Sanderson and Martin, 1996).

Page 7
As rapid acceleration occurs, during and after prosthetic push-off, the
prosthesis can give the amputee the sensation that their leg is pulling off. However, by
restricting knee flexion and maintaining the prosthesis in a vertical position the
elongation on the distal end of the residual limb is eliminated.
Knee flexion can also be limited as a result of the prosthesis’ design. The
patellar tendon bar in particular designs apply pressure on the patella ligament when
the knee is flexed. If this pressure is excessive, the amputee maintains their knee in
extension to avoid discomfort (Miller, 1987; Enoka, Miller and Burgess, 1982;
Brouwer, Allard and Labelle, 1989).
The intact limb limits the amount of knee flexion in an attempt to gain
symmetry with the prosthetic limb. The decreased knee flexion maintains the intact
foot close to the ground and as a result the step length is reduced (Sanderson and
Martin, 1996). It has been suggested that the reduced step length on the intact side is
in an attempt to match the step length of the prosthetic side and hence gain symmetry
between the intact and prosthetic limbs.
The knee flexion angle of the intact leg is also manipulated in an attempt to
gain symmetry between the prosthetic and intact limbs. By manipulating joint
moments, the sum of all the joint moments on the intact leg is similar to the sum of
those on the residual limb.
The rigidity of the extended knee at initial contact reduces the shock absorbing
characteristics of the limb and places further stress on the knees and hips of both legs
and the vertebral column (Enoka, Miller and Burgess, 1982; Brouwer, Allard and
Labelle, 1989). Such stresses can result in degenerative changes at these joints
(Czerniecki, 1996; Macfarlane, Nielsen and Shurr, 1997).
It is important for the above knee amputee to maintain knee stability and
prevent the knee buckling (Czerniecki, 1996). To achieve this, above knee amputees
use their hip extensors to maintain stability. The hip is maintained in extension for a
longer period compared to able-bodied athletes for stability reasons and is also held at
approximately 0o-5o extension to assist in maintaining a vertical limb for the reasons
mentioned previously. However, by maintaining the hip in extension, the impact
forces are not absorbed efficiently. To effectively absorb impact forces it is necessary
to have hip and knee flexion, although knee flexion encourages knee instability
(particularly in above knee athletes). Ideally, the prosthetic knee unit should replicate

Page 8
the quadriceps in early stance and the hamstrings in late stance in their energy
absorption roles and abilities (Czerniecki, 1996).
JOINT MOMENTS During swing in below knee amputee running there is an increased hip flexor
moment on the intact and prosthetic sides (Czerniecki and Gitter, 1996; Sanderson
and Martin, 1996). Sanderson and Martin (1996) found that both the intact and
prosthetic limbs have an increased hip flexor moment compared to normal. The intact
leg increases its hip flexor moment in an attempt to provide symmetry between the
limbs during running. As mentioned previously, this may be an attempt to gain
symmetry between the limbs by making the sum of the joint moments on each leg
similar values.
Czerniecki and Gitter (1996) found an increased hip flexor moment on the
intact side during swing contributes to energy transfer mechanisms. By increasing the
concentric hip flexor and eccentric knee extensor contractions during swing, there is
an increase in the mechanical work done and the energy available to transfer. Energy
transfer is adopted in amputee running to provide an alternate power source to
compensate for the insufficient push-off on the prosthetic side.
The knee and ankle moments are also manipulated on the intact side in an
attempt to gain symmetry between the intact and prosthetic limbs. The joint moments
are manipulated to allow the sum of the joint moments on the intact limb to equal the
sum of joint moments on the prosthetic limb (Sanderson and Martin, 1996). Although
the knee joint may contribute a different joint moment to the summed figure of each
limb, the addition of all the joint moments on each limb will be approximately the
same.
ENERGETICS At initial contact in able-bodied running, pronation and dorsiflexion, along
with hip and knee flexion, assists in absorbing impact loads (Thordarson, 1997). The
foot is dorsiflexed as the body moves over the foot and during the absorption phase,
following initial contact, the hip and knee extend and remain extended until just prior
to push-off (Throdarson, 1997). At push-off the ankle plantarflexes and the hip and

Page 9
knee flex to generate energy to propel the body forward (as cited by Lees in Durward,
Baer and Rowe, 1999).
In below knee amputee running, similarly to able-bodied running, all joints of
the lower limbs assist in energy generation and absorption. However, they each
contribute differently compared to able-bodied running and as a result of the loss of
the plantarflexors in the amputee. In comparison to able-bodied running, the intact leg
has increased impact loads and the prosthetic leg has decreased impact loads
(Brouwer, Allard and Labelle, 1989; Prince, Allard, Therrien and McFadyen, 1992;
Czerniecki and Gitter, 1996). There is also an overall reduction in the work done on
the prosthetic stance phase limb in below knee amputee running, irrespective of
prosthetic foot type (Czerniecki, Gitter and Munro, 1991). Some studies have found
that up to 50% less work is done on the prosthetic stance phase limb compared to
normal (Czerniecki and Gitter, 1992). This is attributable to the reduced energy
generation provided by both the plantarflexors and knee extensors. The prosthetic side
knee extensors absorb significantly less energy than normal and as a result the
prosthetic hip extensors absorb more energy than normal (FIGURE 4) (Czerniecki,
Gitter and Munro, 1991; Czerniecki, 1996). The hip extensors on the prosthetic side
actually have increased work demands and generate more energy than normal during
stance phase (FIGURE 5). Czerniecki and colleagues (1992) found that the prosthetic
side absorbed two-thirds the energy and the hip extensors generated three times more
energy than non-amputees. The intact limb in below knee athletes during stance does not increase muscle
work to compensate for the power deficits associated with prosthetic push off
(Brouwer, Allard and Labelle, 1989; Smith, 1990; Czerniecki, 1996). However,
during swing, the total mechanical work done on the intact limb is 69% more than
normal (Czerniecki and Gitter, 1992; Czerniecki, Gitter and Beck, 1996). This
influences the energy levels of the limb and energy transfer mechanisms.
Energy transfer assists in accelerating the prosthetic limb into swing and
accounts for more than 50% of the total work done (Gitter, Czerniecki and Miender,
1997). Typically, energy is transferred into the prosthetic limb in early swing and as
the limb decelerates toward the end of swing, energy is transferred out of the limb.
This energy transference co-insides with prosthetic push-off (Czerniecki, Gitter and
Beck, 1996).

Page 10
The intact limb of the transfemoral amputee experiences higher impact loads
and higher work demands compared to the prosthetic and normal limbs (Czerniecki,
1996). Increased mechanical work by the intact limb compensates for the inability of
the prosthesis to provide push-off power. The intact hip extensors, during the
concentric contraction phase in stance, produce 270% more mechanical work than
normal and the intact plantarflexors generate 30% more (Serroussi, Gitter, Czerniecki
and Weaver, 1996). The increase in mechanical work by the intact hip musculature
increases the energy levels of the limbs and contributes to energy transference. Energy
transfer mechanisms are incorporated into transfemoral running gait similarly to
transtibial amputees, to assist in prosthetic push-off and to assist the acceleration of
the prosthesis into swing (Gitter, Czerniecki and Beck, 1996).
There is also an increase in hip flexor power on the prosthetic side to
accelerate the transfemoral prosthesis into swing. The increased hip flexor power
produces a ‘pull-off’ effect, lifting the prosthesis into swing, rather than pushing off
with the prosthesis (Serroussi, Gitter, Czerniecki and Weaver, 1996). The value of the
prosthetic hip flexor power is similar to normal. However, the prosthetic limb weighs
approximately 30-40% of the normal limb. In context, more power is produced to
propel the lighter prosthetic limb into swing compared to a ‘normal’ leg (Serroussi,
Gitter, Czerniecki and Weaver, 1996).
Figure 4 - ENERGY ABSORPTION DURING STANCE. This figure illustrates the distribution of total
stance phase eccentric muscle work (energy absorption) of the hip extensors, knee extensors and ankle
plantarflexors (Czerniecki, Gitter and Munro, 1992).

Page 11
Figure 5 - ENERGY GENERATION DURING STANCE. This figure illustrates the distribution of
total stance phase concentric muscle work (energy generation) of the hip extensors, knee extensors and
ankle plantarflexors (Czerniecki, Gitter and Munro, 1992).

Page 12
CHAPTER 2
AMPUTEE SPECIFIC CONSIDERATIONS The recreational desires of the lower limb amputee are not entirely considered
during the initial rehabilitation stages (Enoka, Miller and Burgess, 1982; Czerniecki
and Gitter, 1992). The initial rehabilitation team should discuss the patient’s
expectations beyond gait re-education in regard to long-term functional outcomes.
Ideally, rehabilitation programs should not regard walking as the ultimate objective
for fit and active lower extremity amputees. Running forms the basis of many
recreational activities and running related issues should be addressed and incorporated
in the rehabilitation programs for active amputees, especially if they intend to pursue
recreational activities (Czerniecki and Gitter, 1992).
When managing an amputee athlete (either lower or upper extremity) there are
a number of factors to consider. The amputee pursuing recreational desires is faced
with various challenges including physical, prosthetic and psychological issues.
Clearly a multi-disciplinary team is required in the management and preparation of
these athletes to address each challenge.
PHYSICAL CONSIDERATIONS Physically, amputee athletes have increased work demands compared to able-
bodied athletes during walking and running. Amputee athletes often tire quicker due
to the increased work demands and have thermoregulatory issues. Amputees tend to
perspire more as there is less surface area for heat dissipation. As a result of wearing a
prosthesis, the perspiration cannot evaporate and the full cooling benefits associated
with evaporation are not gained.
Muscular imbalances may also be present as a result of surgical management.
Consequently, compensatory measures to overcome the original deficiencies may
further influence the development of other muscular imbalances.
Pain and phantom pain also requires consideration when managing amputee
athletes. Pain influences the ability of the athlete to fully weightbear and impairs their
ability to walk and run.

Page 13
PROSTHETIC CONSIDERATIONS Prosthetically, there is a need for a recreational or sporting prosthesis that is
designed for the particular sport chosen by the athlete. This will be discussed in the
prosthetist’s management of the athlete.
PSYCHOLOGICAL CONSIDERATIONS Congenital and acquired amputees must continuously attend to various
psychological issues, amongst many includes the acceptance of amputation, body
image, self-pity and frustration. It may be necessary to employ experts in psychology
to delicately handle the situation.
The amputee’s ability to cope with such issues and to maintain a healthy
psychological state is influenced by the amputee’s attitude and their ability to pursue
goals to control their negative feelings. Amputees often engage in sport as a result of
observing role models and to prove their abilities and functional capacity as an
athlete. Sport itself provides a number of psychological benefits including enhancing
self-confidence and increasing motivation.
The amputee athlete may find it difficult not only re-integrating back into
society but also into able-bodied sports. The commitment and effort required to
achieve an elite level of competitiveness is also difficult in amputee sports. The
athlete may face setbacks during their training and as a result need to be prepared to
modify their outlook, goals and performance expectations.
Most amputee athletes are active prior to their amputation and often believe
they are unable to further practice and develop their sporting abilities. Role models
indirectly encourage the amputee to pursue their sporting desires and are commonly
used as a tool for managing amputee psychological issues. Role models provide a
good resource in the area of amputee psychology however their contribution is often
underestimated.
Role models increase the awareness of the abilities of amputees and provide a
foundation from which other amputees can base themselves in terms of achievable
goals. They give the amputee perspective as they begin to consider their amputation in
‘relative terms’. That is, the amputee does not allow their amputation to provide an
obstacle in achieving their goals and objectives. Through this, the amputee learns the
ability to adapt their goals to certain conditions.

Page 14
CHAPTER 3
AMPUTATION LEVEL CONSIDERATIONS
CONGENITAL AND ACQUIRED AMPUTEES In most cases, congenital amputees have a shorter proximal section (i.e.,
humerus or femur) and therefore their lever arm is reduced. In particular lower limb
congenital pathologies (i.e., proximal femoral focal deficiency – PFFD), where a short
femur causes the knees to be at different heights, creates technical problems with leg
exercises and drills (e.g., squats).
The neuromuscular pathways that the congenital amputee athlete has
developed since childhood often make it difficult to modify the athlete’s style. For
example, congenital arm amputees naturally adopt their intact limb as their dominant
side. It is difficult to train the neuromuscular pathways of congenital arm amputees to
drive and propel with their affected side and to avoid compensating and balancing
with their dominant side.
UPPER EXTREMITY AMPUTEES The upper limbs provide balance, propulsion and drive during running. If only
one arm is present, often the athlete presents with decreased strength on their affected
side and associated scoliosis due to the difference in muscle strength.
Upper extremity amputees often hold their intact arm out as a compensatory
measure to maintain balance. Ideally, the arm should move straight up and down and
not swing out and around.
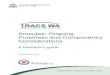
Prosthetic management of upper limb amputees is mainly to assist with a
crouch/block start (FIGURE 6). It allows the athlete to gain full momentum and drive
from the blocks. It is difficult for a congenital arm amputee to incorporate and use the
prosthesis in their running style, however traumatic below elbow athletes may utilise
and prefer weighting of their prosthesis.

Page 15
Figure 6 - A BELOW ELBOW RUNNING PROSTHESIS. This type of prosthesis assists crouch/block
starts for below-elbow amputees.
THROUGH KNEE AMPUTEES Knee disarticulation amputees have an advantage over transfemoral amputees
as a result of a longer residual limb length. The length of the lever arm means the
muscles are longer. Resulting in a powerful lever arm that increases the amputee’s
ability to generate power. The increased muscle mass also provides increased
proprioception, provides better control of the knee unit and provides the amputee with
a good idea of their foot placement. Through-knee athletes can often tolerate distal
weightbearing; as a result they have shorter sockets that do not require loading the
pelvis.
ABOVE KNEE AMPUTEES Above knee amputation surgery has a huge impact on the stability and strength
of the residual limb. Above knee amputees often lose muscle strength as a result of
reduced muscle mass, muscle atrophy and muscular imbalances.
Again, the stump length influences the lever arm, power and muscle
attachments of transfemoral athletes. The length of the femoral remnant determines
the attachment of the adductor musculature and hence their adducting ability and
strength. In most cases, the shorter the stump the more abducted it is. The reason for

Page 16
this is that the adductor musculature is not attached to its correct anatomical position.
The abductor musculature and the gluteus medius and minimus over power the
adductors of the residual limb and hold the limb in an abducted position. Often, with
shorter residual limbs, hip external rotation occurs as a result of no opposition of the
abductors and external rotators.

Page 17
CHAPTER 4
THE MULTI-DISCIPLINARY TEAM APPROACH
A multi-disciplinary team approach has assisted Australian amputees achieve
the successes of recent times. The team approach is successful in the rehabilitation
management of amputees immediately post-operatively and is also applicable to
training amputee athletes. A multi-disciplinary team approach provides the athlete
with expertise in every aspect related to amputee running. The success of the multi-
disciplinary team is dependent on the qualifications, interest and abilities of each team
member and their capacity to communicate and work within a team environment.
The immediate post-operative multi-disciplinary team educates and
rehabilitates the patient on all facets relating to their amputation. The basic team
involves; the doctor/orthopaedic surgeon, physiotherapist, prosthetist, social worker
and psychologist, although this may differ between hospitals and rehabilitation
facilities. The recreational desires are not entirely considered in the initial
rehabilitation phase, however the multi-disciplinary team approach is successful and
the principles can be applied to training amputee athletes.
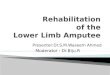
The amputee running multi-disciplinary team is similar to the immediate post-
operative rehabilitation team, however of particular interest and significance is the
relationship between the physiotherapist, the prosthetist, the coach and the amputee
athlete (FIGURE 7). With minor but important contributions from the biomechanist and
other sport related professionals (e.g., orthopaedic surgeon/sports physician, sports
psychologist etc). The goal of the ‘team’ is to work together to assist the athlete in
achieving their maximal functional potential, which in this situation, is to become a
competitive amputee runner. Each member plays an important role in assisting the
athlete to produce an efficient running style, in an attempt to minimise the energy
expenditure and metabolic cost associated with amputee running gait (Nunn, 1992). It
is essential each member understand their individual role as well as the roles of the
other members. It is important to note that each member of the multi-disciplinary
team plays an equally important role and the co-ordination of these disciplines
determines the success of the preparation of amputee athletes.

Page 18
Figure 7 - THE MULTI-DISCIPLINARY TEAM. This figure demonstrates the relationship of the
multi-disciplinary team involved in preparing amputee athletes.
DOCTOR The doctor/orthopaedic surgeon plays a small but important role in the multi-
disciplinary team. The doctor/surgeon supervises the medical and surgical
management of the athlete, monitors the general health of the athlete and plays an
important role in diagnosing injuries and injury management. Ideally they should have
sport specific knowledge and/or have previous experience in managing amputees.
COACH
AMPUTEE
PHYSIOTHERAPIST PROSTHETIST

Page 19
PHYSIOTHERAPIST The physiotherapist, through a physical assessment, determines the current
physical status of the athlete. In conjunction with the coach, the physiotherapist
develops and supervises a general fitness program. The physiotherapist focuses on the
general strength, flexibility, stability and endurance of the athlete and introduces and
provides basic education on sport specific skills. The physiotherapist must be satisfied
with the condition of the athlete, including their walking gait, before the athlete is
eligible for a running prosthesis.
PROSTHETIST The prosthetist determines the componentry for the running prosthesis
including the suspension and interface and fabricates and aligns the prosthesis to
running specifications. The prosthetist is concerned with the effects of the prosthesis
on movement and the athlete’s utilisation of the prosthesis’ characteristics.
COACH After the introduction of the basic sport specific skills by the physiotherapist,
the coach formulates a training program and technically evaluates the athlete’s
performance. Generally, the coach is interested in the general movement of the
athlete, their style and progress.
As demonstrated, the multi-disciplinary approach can be applied to any type of
amputee management. This may include other sports or other aspects relating to
rehabilitation and recreation. The success of the team is determined through the ability
of the team to work together and communicate.

Page 20
SECTION 2
THE MULTI-DISICPLINARY TEAM THE ROLE OF THE PHYSIOTHERAPIST
THE ROLE OF THE PROSTHETIST
THE ROLE OF THE COACH
This section discusses the roles and management of below-knee and above-
knee amputee runners by each multi-disicplinary team member. The physiotherapist
assesses the athlete as they initially present to a clinic. Based on the results of the
athlete’s walking gait and various tests the physiotherapist can design and determine
an individualised physical upgrading program. Once the athlete has improved in these
areas they are introduced to the sport specific skills necessary to run. The
physiotherapist also determines when the athlete is eligible for a running prosthesis
and plays a further role in the ongoing management of the athlete.
Once the athlete has fulfilled the criteria necessary, the running prosthesis can
be fabricated and aligned by the prosthetist. When determining the prosthetic
componentry, the prosthetist must consider the foot, socket-stump interface, socket
shape and type, suspension, trimlines and the relationship of the componentry.
Ultimately the athletes’ preference determines the prosthesis to be fabricated and the
prosthetist aims for the amputee to control the prosthesis, not the prosthesis control
the amputee.
Following the introduction of the sport specific skills by the physiotherapist,
the coach takes over to further define these skills. The coach moulds the athlete to run
to a technical model. To achieve this, the coach implements a sport specific training
program that encourages strengthening the cardiovascular system and the sport
specific musculature used in running.
The coaching strategies used to train able-bodied athletes are applicable to
training amputee athletes. However, there are a number of factors the coach needs to
consider when designing a training program for amputee athletes. These factors and
modifications to exercises will be discussed in this section.

Page 21
CHAPTER 5
THE ROLE OF THE PHYSIOTHERAPIST
The physiotherapist assesses the athlete in their ability to become a runner.
Generally, the role of the physiotherapist is to provide gait re-education and gait
training for amputees in both their everyday and sporting prostheses, maintain general
body condition and prevent and manage injuries (Nunn, 1992). To achieve this, the
physiotherapist implements a training program that involves general strengthening
and flexibility exercises, focussing on the weaknesses and deficiencies identified
when the amputee initially presents.
It is important that the physiotherapist has a full understanding of the
biomechanical principles of amputee running as it influences the information they
require during their initial assessment and also affects the implementation of an
appropriate training program.
The management of the physiotherapist involves a number of steps. They first
complete an initial assessment of the athlete including gait analysis and a physical
assessment. This provides the basis for the physical upgrading program. Physical
upgrading includes a core program, weights and pool programs and is implemented in
an attempt to gain general fitness, strength and endurance. This period also involves
gait re-education and the introduction of running skills.
Finally, the physiotherapist maintains an ongoing role in managing the athlete,
including injury management and must also liase with the multi-disciplinary team as
much as possible.
INITIAL ASSESSMENT The approach taken by the physiotherapist follows the same fundamental
principles at each amputation level. However, some modifications to testing
procedures and exercises are required to allow for the different amputation levels. In
any case, the basic procedures and protocols are the same.

Page 22
The initial assessment by the physiotherapist involves an in-depth analysis of
the individuals’ walking gait and a thorough physical assessment of the athlete’s
posture, mobility, strength and stability.
GAIT ANALYSIS
It is important to complete a thorough investigation of the athlete’s walking
gait. The athlete wears their walking prosthesis during the analysis, as their running
prosthesis is aligned to different specifications. These specifications are not suited to
walking and promote asymmetry, making it difficult to accurately assess the walking
gait and posture of the athlete.
The assessment identifies the functional strength, stability and mobility of the
athlete. The gait deviations present demonstrate the functional weaknesses of the
athlete and should be managed appropriately, as any deviations in walking gait will be
amplified in their running gait. A detailed report on the observations should be
documented, as it is a useful tool in gauging the progress of the athlete over a certain
period.
The physiotherapist should follow the same amputee gait analysis procedures
and guidelines as they would at any other time. They look at the basic pattern of
movement and determine the reasons for any compensations that are present.
PHYSICAL ASSESSMENT
A full physical assessment should be carried out on the athlete. This includes
assessing the residual limb condition, posture, joint ranges of motion, muscle strength,
muscle control and muscle activation and recruitment patterns. It is assumed the
physiotherapist has knowledge in the basic testing positions and procedures. There are
no amputee specific tests necessary to assess the strength, range of movement and
muscle control. Modifications may be necessary depending on stump length and
amputation level, however the same principles apply as for able-bodied patients. Of
particular interest is the strength, range of movement, stability and activation of the
hips and abdominals (the ‘core’). The core plays a critical factor in amputee running
in relation to posture, pelvic movement and energy generation and absorption.

Page 23
• Residual Limb
The condition of the residual limb is assessed and follows assessment criteria
as for the initial presentation for an everyday prosthesis. The stump characteristics
including musculature, scarring, length, shape, sensitivity, abrasions, redundant tissue,
pain and phantom pain should be considered.
The physiotherapist should also consider the impact and tolerance of sporting
activities on the level of pain and phantom pain experienced by the amputee.
• Posture
The postural assessment assists in management and prevention of back injuries
and reflects compensations adopted by the amputee to overcome the biomechanical
deficits they encounter during gait. Maintenance of a good posture influences the
performance and technique of the athlete (Nunn, 1995).
The posture of the athlete should be assessed with the walking prosthesis
donned. With the athlete looking straight ahead, ensure the feet are level and weight is
evenly distributed between both feet. If the weight is unevenly distributed, the
alignment of the prosthesis may need to be modified. There should be no need for the
athlete to exert effort to maintain a comfortable and symmetrical static alignment.
• Strength
Initial strength tests assist in identifying the weaknesses and imbalances the
athlete has. From this, the physiotherapist can establish the most appropriate training
program, taking into account these deficiencies. This includes designing a modified
gym program where the exercise is adapted to the amputee and is bias towards
strengthening weak musculature and avoids strengthening its strong antagonist. For
example, the program may be biased towards strengthening weak hip flexors and
exclude strengthening the overpowering hip extensors.
The procedures to follow are the basic strength tests used in everyday
physiotherapy management. However, some positions and tests may need to be
modified to assist in identifying the strengths of amputees.

Page 24
• Range of Motion
Range of motion tests provide information regarding the mobility of particular
joints. All joints of the lower and upper limbs should be tested as they all influence
the running ability of the athlete. Similarly to strength training, a stretching program is
prescribed to assist in stretching out tight muscles and joint structures (e.g., joint
capsule), increasing flexibility and increasing the movement of the joint.
Restrictions in joint movement influence the ability of the athlete to run
efficiently as compensations are usually adopted to overcome any limitations.
• Core and Joint Stability and Activation
Core and joint stability and activation are important as these influence the
athlete’s ability to recruit the appropriate muscles at particular times during the gait
cycle. Employing inappropriate muscles to do work during running gait is considered
a compensatory mechanism and should be addressed. The compensations adopted
influence the efficiency and energy expenditure of the athlete's running gait.
To test the posture, mobility, strength and stability of the athlete, two forms
have been developed to guide the assessor (the physiotherapist) through the process.
The tests should be performed at each joint on both the intact and prosthetic sides and
on the upper limbs.
The impairment specific screening form assists in identifying weaknesses and
provides examples of common deviations. However, it is still important to determine
the severity of the weakness. The results of the tests provide an insight of the
strengths and weaknesses of the athlete and provide the basis from which an
appropriate training program can develop. The forms are found in APPENDIX II A and
the explanatory notes in APPENDIX IIB.
Once the results of each test have been obtained, the information should be
analysed to determine the strengths and weaknesses of the athlete. This forms the
basis for the development of an individual physical upgrading program.

Page 25
PHYSICAL UPGRADING The physical upgrading component of the physiotherapist's management
includes gait re-education, core maintenance, general fitness work that comprises of a
core program, weights program and pool work and the introduction of basic running
skills. Achieving a satisfactory level of fitness (i.e., strength, mobility, stability and
endurance) is a criterion that must be fulfilled before the athlete is eligible for a
running prosthesis. It is vital the athlete has good hip and abdominal (core) strength,
stability and range of movement to maintain a good posture and to achieve the
benefits mentioned previously.
GAIT RE-EDUCATION
Gait re-education aims to attain a precise walking gait with no gait deviations,
as any deviations will be more pronounced in running gait. It involves a number of
steps including:
- Strengthening or activating weakened or inhibited muscle groups, usually the
hip extensors, abdominals and knee extensors.
- Inhibiting compensatory measures to overcome deficiencies and stretching of
tight structures as a result of these compensations, commonly the iliopsoas as
it influences hip and knee flexion throughout stance phase.
- Improving muscle control especially eccentrically; for example, in transtibial
athletes it is important to enhance the control of the knee extensors to ensure
shock absorption, or enhance control of the hip extensors in transfemoral
athletes.
- Re-introducing correct movement patterns into gait (i.e., activation of
appropriate muscle synergies, adequate upper body rotation (FIGURE 8) etc).

Page 26
Figure 8 - GAIT RE-EDUCATION. A Swiss ball is used in gait re-education for a number of reasons,
in this case to encourage adequate trunk movement.
CORE PROGRAM
The body core is the lumbopelvic-hip complex. Lumbopelvic-hip (core)
stability is an important component in rehabilitation and gait re-education. A core
stabilisation program aims to develop an optimal level of functional strength and
dynamic stabilisation (FIGURE 9). Core stabilisation also improves dynamic postural
control, neuromuscular efficiency and enhances the power and endurance of the core
musculature. A core program further facilitates muscle balance by encouraging the
activation and strengthening of functional synergies, whilst simultaneously inhibiting
inappropriate activity.

Page 27
Figure 9 - CORE STRENGTHENING. A Swiss ball can also be used to assist in core strengthening (as
seen here).
MODIFIED GYM PROGRAM
The weights program should: -
- Target weakened muscle groups as identified during testing, in an attempt to
decrease imbalances and prevent the adoption of compensations.
- Have a functional emphasis where most of the limb is against resistance
requiring stabilisation of the core and attention to joint positions in relation to
the activity you are training for (FIGURE 10). This strengthens the functional
range of the muscle while simultaneously recruiting core stability muscles to
reinforce and improve their roles in core stability.
- Include exercises that can be modified to adapt to the individual amputee (e.g.,
squats and bench press) (FIGURE 11). The program should be modified as the
athlete improves their sport specific strength and skills. Squats need to be
modified so the intact leg does not bear an increased proportion of the load.
Each limb should therefore be strengthened individually. Upper limb amputees
will find it difficult to maintain a horizontal bar in bench press. To overcome
this the Smith machine (assisted bench press) should be used to avoid injury
and allow for correct technique. It also permits the athlete to perform the
exercise independently.
- Be supervised and monitored to ensure the correct technique is used.

Page 28
Figure 10 - MODIFIED GYM PROGRAM. Exercises should have a functional emphasis with
simultaneous stabilsiation of the core (courtesy of the Australian Institute of Sport).
Figure 11 - MODIFIED GYM PROGRAM. Modifications to exercises are necessary to allow the
athlete to gain the maximum benefits from the exercise. This figure shows a modified squat (courtesy
of the Australian Institute of Sport).

Page 29
POOL WORK
Pool work is an important component in amputee training, particularly in
bilateral amputee management. It provides a non-weightbearing exercise and assists in
injury prevention, as the limb is not constantly loaded as in walking and running. It
enhances cardiovascular fitness and involves core stability work. Pool work may also
be used as an alternative training method if an injury has occurred.
No modifications to exercises are necessary as the water assists the amputee
maintain balance. This allows the athlete to gain the full benefits of each exercise. It is
important to monitor the exercise technique to ensure it is being executed
appropriately.
A pool program may also include the use of a specially designed aquatic
training prosthesis for the residual limb in an attempt to involve the residual limb in
the pool workout.
SPORT SPECIFIC TRAINING
The physiotherapist also assists the athlete in acquiring the basic skills of their
sport. The process of developing sport specific skills is similar to gait re-education. As
the athlete develops basic running skills the coach takes over the sport specific
training of the athlete.
ONGOING MANAGEMENT LIASE WITH TEAM
As the physiotherapist is a member of the ‘team’ they maintain contact with
the athlete throughout their prosthetic and athletic lives. The physiotherapist provides
further sporting analysis and monitors the progress of the athlete. The program
requires constant modifications as the athlete develops their sport specific strength
and skills.
INJURY PREVENTION AND MANAGEMENT
The physiotherapist also plays a major role in injury prevention and
management. They introduce the initial sport specific skills and techniques to the

Page 30
athlete and ensure that the exercises are practised correctly. Close monitoring of the
athlete's running style identifies any weaknesses in their technique. Prompt
identification and management of technical errors by the physiotherapist (and coach)
prevents injury development. The physiotherapist should also be aware of previous
injuries and the current status of the affected areas. It is important to monitor the
previously injured area for the recurrence of pain, limitations in movement, oedema
and heat.
The physiotherapist designs and implements a rehabilitation program that aims
to return the athlete to previous training levels as quickly and smoothly as possible.
During this period it is important to maintain the general fitness levels of the athlete
and to educate the athlete on injury management.
ELIGIBILITY FOR A RUNNING PROSTHESIS To be eligible for the fabrication of a running prosthesis, the amputee must
fulfil a number of criteria. The athlete should have:
- A sound gait with no deviations as any deviations in walking are more
pronounced during running
- Achieved a good level of general fitness, including strength, flexibility,
stability and endurance
- Demonstrated commitment through adhering to the initial fitness program for
a minimum of approximately three months.
- Joined a sporting association and have commenced competition at a local
level.
COMMON EXERCISES AND PROGRAMS It is difficult to define a ‘common’ training program from a physiotherapist’s
perspective. In the initial management of the athlete, the physiotherapist aims to gain
strength and endurance through the physical upgrading program. The prescription of
exercises is entirely based upon the findings of the initial assessment. The strengths
and weaknesses identified in the initial assessment may differ between athletes;
therefore the training program should be based on the athlete’s personal needs and
progression.

Page 31
CHAPTER 6
THE ROLE OF THE PROSTHETIST
The prosthetist plays a major role in the multi-disciplinary team approach
when managing amputee runners. It is necessary for the prosthetist to have sport
specific knowledge and current knowledge in prosthetics, as minor developments can
improve the athlete's performance.
The athlete will have an additional prosthesis for their recreational and
sporting activities. The prosthetist conducts an initial assessment to determine the
most appropriate componentry for the sporting prosthesis for the athlete. This requires
consideration of not only the prosthetic componentry but the demands of the sport,
componentry relationships, muscular imbalances and patient/athlete preference.
Ideally, when the athlete presents for their running prosthesis they will have fulfilled
the criterion for a running prosthesis as stipulated by the physiotherapist.
In the initial assessment, the prosthetist aims to determine the componentry to
be used in the running prosthesis, in particular the interface material. In any case all
the prosthetic options available should be presented to the athlete as inevitably their
personal preference plays a major role in determining the prosthesis to be fabricated.
The prosthetist then fabricates the prosthesis and aligns it to running
specifications. It should be emphasised that the maintenance of the prosthesis should
be attended to by the prosthetist.
The prosthetist plays a further role in education and it is important for the
prosthetist to remain in constant contact with the other members of the multi-
disciplinary team to discuss the management of the athlete.
INITIAL ASSESSMENT For the initial assessment to occur, the athlete will have fulfilled the eligibility
criteria for a running prosthesis as specified by the physiotherapist. This requires the
athlete to have a good walking gait, demonstrated commitment and has improved their
strength, range of motion and stability (for more detail refer to physiotherapy section).

Page 32
It should be noted that prior to this assessment, the amputee will have been
running on their everyday prosthesis, which is not aligned to running specifications.
The results of this maybe reflected in the stump condition of the athlete.
The initial assessment of the amputee for a running prosthesis follows the
same principles and guidelines as the assessment for a new walking leg. The
prosthetist will most likely have seen the athlete previously and has an understanding
of the athlete’s stump characteristics and individual alignment. In any case it is
important to examine the residual limb characteristics in relation to skin quality, scar
line and general stump condition. These characteristics influence the selection of
interface for the running prosthesis and the main aim of the initial assessment is to
determine the most appropriate interface for the athlete.
RUNNING PROSTHESIS With constant prosthetic developments it is important the prosthetist presents
the athlete with all the prosthetic options available. Emphasis must always be placed
on the athlete’s preference as they must be comfortable and secure with their
prosthesis.
BELOW-KNEE COMPONENTRY
• Foot
Energy storing feet are designed to more closely replicate the normal
biomechanics of the foot and ankle. They store energy upon loading and later release
this energy, as the foot is unloaded (push-off). During sprinting, the prosthetic foot is
in contact with the ground for a shorter period of time and can incur loads up to five
times bodyweight. The energy storing/releasing characteristics provide numerous
benefits to the athlete and are recommended for running prosthesis.
Other prosthetic feet, including the SACH, single axis and multi-axial feet are
based on different design principles. They do not return the energy absorbed at initial
contact as effectively as energy storing feet although this does depends on the type of
energy storing foot (e.g., Vari-Flex, Flex-Walk etc).
The Flex-Sprint series are energy-storing feet and are recommended for
running. They consist of a flexible, lightweight carbon fibre keel that runs the entire

Page 33
length from the socket to the ground (FIGURE 12). They have no heel counter and a
drop-toe design to promote toe running (FIGURE 13). The Flex-Sprint III keel has an
inverted question mark shape that allows the prosthesis to be aligned with the weight
line passing through the toe without plantarflexing the foot. The keel shape also
enables the foot to vertically compress and simulate dorsiflexion at initial contact.
This accounts for the symmetry seen in amputees running with these feet. It limits the
vertical displacement of the centre of mass and in turn decreases the impact loads
incurred by the intact limb.
Figure 12 - THE FLEX-SPRINT III. This figure shows the Flex-Sprint III runs the entire length from
the socket to the ground (courtesy of the Advanced Prosthetic Centre).

Page 34
The distal end of the Flex-Sprint III curves up and requires a build-up/filler
underneath. The build-up should extend from the distal tip of the toe to the point of
contact between the foot and the ground. This build-up aims to increase the surface
area of the ‘toe’ in contact with the ground. Attached to this build-up are running
spikes from a spiked running shoe to assist in traction etc.
To select the most appropriate Flex-Sprint III it is important to determine the
‘category’ of the foot. The category of the foot relates to the stiffness and the
compressibility of the carbon fibre keel and is determined by the individual
characteristics and preference of the athlete. The category of the foot is always a
consideration when using an energy storing foot in a prosthesis and it is necessary to
determine the correct category otherwise the athlete will be unable to utilise their
prosthesis effectively. Gait deviations including knee hyperextension (in both BK and
AK athletes) may result if the category selection is incorrect. The higher the category,
the stiffer the foot and the less compression.
Figure 13 - THE FLEX-SPRINT III AND ATTACHMENTS. The Flex-Sprint III can attach to the
socket by a pylon connector or a lamination connector (courtesy of Flex-Foot).

Page 35
The Flex-Sprint III can be attached to the transtibial socket in two ways, either
by a pylon connector (FIGURE 17 & 18B) or a lamination connector (FIGURE 14). The
pylon connector is the preferred method. It is laminated into the socket and the
connector is exposed distally (below the socket). The Flex-Sprint III is bolted to the
exposed portion of the attachment plate and this allows for easy adjustments to be
made. The position of the pylon connector to the socket is dependent on the athlete’s
stump characteristics (i.e., stump flexion, abduction/adduction). The pylon connector
should be strongly adhered to the socket and often requires carbon fibre
reinforcement.
The lamination connector is also laminated into the socket. However, there is
no distal section and the Flex-Sprint III attaches directly to this connector plate,
posterior to the socket (FIGURE 14). If alterations are necessary or if problems occur
with the lamination connector (i.e., screw cross-threading) the entire plate must be
removed from the socket.
The position of the adaptor plates should be as precise as possible before the
lamination. However, if a slight alignment adjustment is necessary, bias wedges are
available to adjust the position of the Flex-Sprint feet.
Figure 14 - POSITIONING AND ATTACHING THE LAMINATION CONNECTOR. It is important
to have the lamination connector in the correct position before it is laminated into the socket.

Page 36
• Liner
The interface between the residual limb and socket should protect the stump
from shear and frictional forces. Depending on the interface, the forces are either
absorbed and/or transferred from between the skin-liner to the liner-socket. The
ability of the interface to distribute or eliminate these forces is also determined
through the interface materials and the socket fit. Socket fit and the liners abilities are
highly inter-related. However, patient/athlete’s preference determines the interface as
their comfort and security is of the upmost importance.
Polyurethane and silicon liners are popular amongst active athletes (FIGURE
16). They are worn directly against the skin providing total contact. This minimises
shear and frictional forces as no movement can occur between the skin and liner.
As the amputee athlete runs, their stump shape changes. The urethane liner
adapt to this as the gel 'flows' from areas of high concentration to areas of low
concentration. Although silicon and polyurethane liners are indicated for highly active
(running) amputees, a pelite liner may still be preferred by some athletes. However,
the pelite can ‘bottom out’ and lose its shock absorbing characteristics. A pelite liner
also necessitates the use of stump socks. The frictional forces produced between the
sock and residual limb can cause skin breakdowns. It is also necessary to change
stump socks regularly as they absorb perspiration. Silicon impregnated stump socks
are also available and provide similar benefits to the silicon liners although to a lesser
magnitude.
Hard sockets with no liners are also contraindicated as forces are dissipated
directly to the residual limb causing skin breakdown and other overload injuries.
• Socket type
A good prosthetic socket should permit efficient energy transfer from the
residual limb to the prosthesis and not impinge on movement. The socket fit is
determined by casting techniques, socket design/shape and the socket materials.
Carbon fibre laminated sockets are lighter and stronger than fibreglass
laminated sockets. The socket lamination procedure follows the same guidelines as a
general lamination, however the position and direction of the carbon fibre influences
the strength characteristics of the socket.

Page 37
Patella tendon bearing sockets focuses loads on particular areas of the residual
limb. For example, the patella tendon bar loads the patella ligament. This can cause
discomfort during knee flexion if there is a large patella tendon shelf.
Similarly, the supracondylar suspending socket (PTK socket) loads proximally
to the femoral condyles for suspension. To achieve this, the mediolateral dimension of
the socket is reduced above the femoral condyles. Although this provides suspension
it causes the quadriceps to atrophy. The athlete then relies on the socket for stability
rather than their muscles alone. This can cause a vicious cycle where the tighter the
ML dimension the less control the muscles have over the prosthesis and the further
they atrophy, then the tighter the ML dimension.
A total surface-bearing, hydrostatic socket is necessary with the use of
urethane and silicon liners (FIGURE 15). Total surface bearing sockets reduce socket
forces as pressure is distributed over the entire residual limb with no specific weight
bearing areas. Hydrostatic socket designs utilises the compression of fluids in the liner
to distribute and eliminate forces. In any case the socket should not compensate for
muscle weakness or instability.
Figure 15 - HYDROSTATIC SOCKETS. Hydrostatic sockets apply pressure equally over the residual
limb (Fergason and Smith, 1999).

Page 38
• Suspension
The athlete’s confidence in the suspension of the prosthesis is important.
Athlete preference is emphasised in the choice of suspension, as the athlete needs to
feel assured that their prosthesis is secure and not going to detach.
As mentioned previously, supracondylar suspension causes the knee extensors
to atrophy and the athlete relies on the prosthesis for stability rather than their
muscles.
Negative pressure suspension requires an intimate fitting total surface bearing
socket. It necessitates a silicon sleeve to be donned over the socket to maintain the
negative pressure and to suspend the prosthesis (FIGURE 16). Unlike the supracondylar
suspending socket (PTK), it does not rely on high trimlines to maintain suspension or
stability. The suspension sleeve does not restrict knee movement and the knee
musculature is fully utilised for stability. This increases the knee muscle’s control of
the prosthesis. An expulsion valve is also necessary to evacuate/expel any air within
the system. Air within the socket/suspension sleeve causes the suspension to be
ineffective. Similarly, if there is a tear in the silicon sleeve the suspension will be
ineffective. Therefore, it is important that the prosthetist is educated on correct casting
and fabrication techniques and the athlete on the correct donning and maintenance
procedures.
Shuttle lock systems are used with silicon or urethane liners. However, they
can elongate on the distal end of the residual limb. This milking effect can be
uncomfortable and give the athlete a feeling of insecurity.
Suprapatellar straps are still used in running prosthesis (FIGURE 17). They are
not necessarily the most suitable suspension for running but athlete's using this type of
suspension have produced world records. The suprapatellar strap can be attached to an
elastic waistband for auxiliary suspension. The elastic strap only provides suspension,
particularly during swing and does not assist weak musculature.

Page 39
Figure 16 – RUNNING PROSTHESIS COMPENENTRY. A negative pressure suspending prosthesis
requires a urethane line, spikes, a Flex-Sprint III attached to a total contact socket via a lamination
connector, an explusion valve and a suspension sleeve).
Figure 17 - RUNNING PROSTHESIS COMPONENTRY. A pelite liner with a suprapatellar cuff
attached to a waistband (www.advancedprosthetic.com.au).

Page 40
• Trimlines
The suspension influences the trimlines of the socket. Ideally, they should be
kept to a minimum to avoid restricting movement, especially knee flexion.
The posterior trimlines of the socket should not impinge on knee flexion. If the
athlete has a reasonably long residual limb, the height of the posterior trimline can be
reduced. When treating athletes with shorter residual limbs the centre of the posterior
trimline should be maintained as proximal as possible without impinging on the
medial and lateral hamstrings.
The medial/lateral trimlines of a transtibial socket should also be kept to a
minimum. Prostheses using negative pressure suspension minimise the height of the
trimlines. This allows the athlete to have good muscle control over the prosthesis.
As the athlete’s knee musculature strengthens and the muscles have increased
control of the prosthesis, the trimlines can be lowered. Lowering mediolateral
trimlines further strengthens the knee musculature. Increased strength also results in
increased muscle control of the prosthesis.
BELOW KNEE ALIGNMENT
Alignment of the prosthesis describes the relationship between the socket and
foot. There are no exact optimal dynamic alignment specifications however the static
alignment of the prosthesis does provide a foundation for dynamic alignment.
Athletes have their own individual dynamic alignment that is influenced by their
personal running technique and stump characteristics. However the basic aim of
alignment is the same, to minimise gait deviations, to gain the maximum out of the
prosthesis and to produce an energy efficient gait
Core stability (as mentioned in the physiotherapy section) and prosthetic
alignment are significantly interrelated. The ability of the athlete to control their
lumbopelvic complex influences their prosthetic alignment. The better core stability
the athlete possesses, the more precise the alignment. This enables the athlete to
utilise the characteristics of the prosthesis more efficiently.

Page 41
Below Knee Bench Alignment (Flex-Sprint III)
• Position the socket in neutral (i.e., 0o flexion) in relation to the foot. This
allows the weightline to fall through the toe without plantarflexing the foot
(when the pylon connector is vertical).
• From the side (sagittal view) with the socket in neutral, the weightline
should fall from the midpoint of the socket through the midpoint of the
Flex-Sprint keel (FIGURES 11 a &b).
Figure 18 - BENCH ALIGNMENT OF THE FLEX-SPRINT III. This figure illustrates the bench
alignment of a Flex-Sprint III attached with a (A) lamination and (B) pylon connector (courtesy of
Flex-Foot). The weight line should fall from the mid-point of the socket through the mid-point of the
Flex-Sprint III keel.
weightline weightline
ground contact ground contact

Page 42
Below Knee Static Alignment
Static alignment provides a foundation from which dynamic alignment can be
determined. Generally, the height of the transtibial running prosthesis is
approximately ½” - ¾” longer than the intact side, depending on the category/stiffness
of the foot. This encourages toe running and allows for vertical compression of the
Flex-Sprint III in an attempt to achieve a level pelvis during stance. The height of the
prosthesis has a significant effect on the trunk movement/core stability of the athlete
and is discussed further in the gait deviations section of this manual.
Below Knee Dynamic Alignment
The dynamic alignment aims to eliminate gait deviations and achieve a
symmetrical running gait. Initial dynamic alignment is based on restoring symmetry
between the intact and prosthetic limbs during running. Depending on the adjustments
made, it may indicate muscle weakness. From this the physiotherapist and coach can
work on strengthening these particular muscles and return the athlete to a more
symmetrical running gait.
The dynamic alignment of the prosthesis changes significantly, as the athlete
becomes more efficient in using their running prosthesis. As their ability to control the
energy storing characteristics of the foot develops, the alignment is adjusted to force
the athlete to use their musculature for stability, rather than relying on the prosthesis.
To encourage the athlete to fully utilise their skills and the prosthesis’ characteristics,
the prosthesis is aligned to have as much foot in contact with the ground as possible.
This should enable the athlete to have total control of the energy stored without being
out of control.
As mentioned previously, if the alignment of the connector plate is incorrect or
alignment alterations are necessary, bias wedges are used to reposition the Flex-Sprint
III in relation to the socket.
ABOVE KNEE COMPONENTRY
In the above knee amputee athlete the stump characteristics have more of an
influence on prosthetic prescription. More components are required in above knee
prosthesis and as a result there is a stronger relationship between the componentry. An
increased number of components increases the chance of breakdown and increased

Page 43
maintenance needs, highlighting the need to maintain constant contact with the
prosthetist and have regular maintenance assessments.
• Foot
Based on athlete feedback and success, the foot used in above-knee amputee
runners is the Flex-Sprint I or II. The Flex-Sprint I is based on the Modular III, which
is an energy storing foot. It consists of a carbon fibre keel that extends from the knee
unit to the toe. However, the Flex-Sprint I has no heel counter and is more
plantarflexed than the Modular III design. The Flex-Sprint I and II have a straighter J-
shaped keel rather than the Flex-Sprint III’s inverted question mark shape (mentioned
in trantibial prosthetic feet options) (FIGURE 19).
As a result of their straighter shape, the Flex-Sprint I and II have less vertical
compression than the Flex-Sprint III. In above-knee running, if the category of the
foot is too soft it allows excessive compression of the foot. As the prosthesis is loaded
the athlete will hyperextend their knee. This produces interlimb asymmetry as the
athlete spends more time on their prosthetic side during stance phase. Compression
also causes malalignment of the height of the prosthetic and intact knee axes.
Figure 19 - THE FLEX-SPRINT SERIES. This figure shows (from left) the Flex-Sprint I, II and III.
The Flex-Sprint I and II are used in above-knee running and the Flex-Sprint III in below knee running
(courtesy of Flex-Foot).

Page 44
• Socket
Transfemoral amputees have the option of two sockets, the quadrilateral
socket and the more recent ischial containment socket design. The ischial containment
socket is preferred over the quadrilateral socket for a number of reasons; it is more
energy efficient at higher speeds, contours better to the residual limb, has a bony lock
that eliminates ischial rotation within the socket and lateral stabilises the femur in
adduction (FIGURE 20).
Figure 20 - THE QUADRILATERAL AND ISCHIAL CONTAINMENT SOCKETS. This figure
compares the ischial containment socket with its bony lock and counter force to the quadrilateral socket
that has no bony lock and pressure on the distal femur (Sabolich, 1985).
Flexible inner plastic sockets with a rigid outer socket framework are common
above knee socket designs. The inner socket provides the interface for suction
suspension while the outer socket provides the structural framework and is fabricated
from a more rigid plastic or carbon fibre laminate. Windows may also be cut in the
outer socket, providing the main structural support is maintained.
On the posterior distal aspect of the above-knee socket there is often a flexion
bumper (FIGURE 26 – Earle Connor). This is in an attempt to limit heel rise. The foot hits
the flexion bumper and returns the foot to extension earlier for initial contact. This
also assists in overcoming the delay of the prosthetic foot during swing phase.

Page 45
• Liner/suspension
Suspension is a major consideration in transfemoral athletes and is determined
by the athlete’s preference. It is important the athlete feels secure with their
prosthesis’ suspension. The suspension options for transfemoral athletes are shuttle
locks or suction suspension.
The forces the athlete uses to extend the knee can cause terminal impact and
when using the shuttle lock system, can disengage the shuttle lock. Replacing the
spring with a more robust spring assists in overcoming this problem. Using a shuttle
lock is also dependent on stump length. A shuttle lock is contraindicated for long
residual limbs, as the shuttle pin will lower the position of the knee unit.
Suction suspension requires a total contact socket that is completely contoured
to the athlete's stump. The athletes pull themself into the prosthesis and the negative
pressure suspends the prosthesis on the residual limb. As mentioned previously, this
form of suspension is used in combination with a flexible inner socket.
Suction suspension is also suitable for through-knee athletes, although it may
be necessary to provide a build up proximal to the femoral condyles so a more
cylindrical shaped socket can be produced. This allows for easier donning.
Through-knee athletes have an extra suspension option available. This is
supra-condylar suspension. The residual limb is loaded proximally to the femoral
condyles and benefits athletes who have distal weightbearing.
Similarly to transtibial suspension, transfemoral amputees may also use
auxiliary suspension for additional security. This can include the use of a neoprene
sleeve or TES (total elastic support). When using a silicon suction suspension system
a neoprene sleeve limits the amount of elongation of the silicon liner on the distal end
of the residual limb.

Page 46
• Knee Units
There is an increased demand on the knee as a result of the faster and
increased loading associated with increased speeds. As a result, the prosthetic knee
used should be more responsive in running than walking. Commonly, hydraulic four
bar linkage knees are used in above knee (and through knee) running prosthesis.
The hydraulic four-bar linkage knee unit provides stability in stance and good
toe clearance during swing. The hydraulic mechanism adapts to changes in speed and
the four-bar linkage component effectively creates a longer lever arm.
The knee units attach to the socket by a lamination adapter plate or a male
pyramid. An L-bracket is attached to the distal connector of the knee and is the
attachment for the foot (FIGURE 21).
The friction of the running knee joint is also increased, so when the athlete
walks they are unable to break the knee. However, with the forces produced during
running the knee should flex accordingly.
Figure 21 - THE FLEX-SPRINT I AND ATTACHMENTS (courtesy of Flex-Foot). The Flex-Sprint I
attaches to the knee unit via a L-bracket adapter.

Page 47
ABOVE KNEE ALIGNMENT
(using a hydraulic four bar linkage and Flex-Sprint I or II)
Initially, the dynamic alignment aims to gain symmetry between the intact and
residual limbs. As the athlete becomes more experienced and has improved control of
their prosthesis the alignment is adjusted. The new alignment is dependent on the
athlete's ability to control the hydraulics of the knee unit and the energy storing
characteristics of the foot.
Above Knee Bench Alignment
Figure 22 - BENCH ALIGNMENT OF AN ABOVE KNEE RUNNING PROSTHESIS. These figures
demonstrate the alignment of above-knee running prostheses using a four-bar linkage knee unit and
Flex-Sprint I (courtesy of Flex-Foot).

Page 48
Bench alignment guidelines of the above knee running prosthesis using a four
bar linkage knee unit and Flex-Sprint I;
• Position the socket in slight extension and anteriorly to the knee unit. As a
result, the instantaneous centre of rotation moves posteriorly and
proximally increasing knee safety.
• In a sagittal view, the weightline should fall from the midpoint of the
socket through the knee axis and approximately six centimetres behind the
distal tip of the toe (FIGURE 22).
• In a frontal view, the weightline should fall from the midpoint of the
socket through the midpoint of the toe (FIGURE 22).
Above Knee Static Alignment
The height of the prosthesis should be as close to normal as possible. The knee
centre should be at the same height as the intact knee and the knee axis should be
horizontal to the ground.
Above Knee Dynamic Alignment
The knee should be aligned so that it is stable in hip extension with as little
energy required as possible for hip flexion to occur.
The angle between the knee unit and the L-bracket adaptor controls the
direction of the ground reaction force and alters the instantaneous centre of rotation of
the knee. Angling the knee unit and L-bracket adaptor is a useful alignment method
when determining the safety of the knee. The angle between the knee unit and Flex-
Sprint I L-bracket adaptor should direct the ground reaction force to a position that
allows the knee to break easily while maintaining stability. The exact angle between
the Flex-Sprint and knee joint is left to the discretion of the prosthetist, taking into

Page 49
account the athlete’s feedback and their ability to utilise their musculature and lever
arm to control the knee unit.
Angling the knee unit and positioning the foot back under the athlete
effectively shortens the toe lever. By shortening the toe lever the stride length is also
reduced. This results in faster loading and unloading of the foot. Consequently the
prosthesis is more responsive and the characteristics of the Flex-Sprint are utilised
more effectively. Shortening the toe lever also decreases the hip flexion required to
lift the prosthesis into swing.
However, these are just theories and there has been no valid research
undertaken to identify and justify the benefits mentioned.
EDUCATION The prosthetist plays a major role in the athlete’s education. The athlete should
have a basic understanding of prosthetic and stump management and care through
previous experience with their everyday prosthesis. The following issues should be
further emphasised as complications may occur. Things to address: -
- Hygiene management. Generally, amputees perspire more during walking
and running as a result of increased work demands. There is decreased
surface area for heat dissipation and as a result of not being exposed to the
ambient air; evaporation of the perspiration is difficult. It is important to
wipe the residual limb dry during training as perspiration can lead to
bacterial development and associated problems (detailed in injury section).
If the athlete uses stump socks then these should be changed regularly as
the socks absorb the perspiration. Cleaning/washing the liner is important
from a hygienic aspect and to ensure the longevity of the liner.
- Monitoring of the stump and education of what to look for. It is important
for the athlete to monitor the stump in an attempt to avoid injuries. Skin
breakdown or irritations and pressure areas are detrimental and usually
affect the athletes’ mobility. The inability of the athlete to wear their
prosthesis as a result of these injuries restricts the athlete to walking aids
and an alternate training program (i.e., pool work). Redness, swelling,
irritations and blisters are signs and may indicate a prosthetic or hygiene
issue.

Page 50
- Prosthetic management. Educate the athlete on the correct donning
procedure and the correct position of the running prothesis. Malalignment
of the prosthesis constitutes an ill-fitting socket and causes stump
problems. If the socket fit is inadequate or alignment inappropriate, the
earlier it is rectified the more comfortable training will become. It should
also be emphasised that any maintenance that the prosthesis requires
should be carried out by the prosthetist. The prosthetist is qualified and
experienced in prosthetics; they know what they are looking for in relation
to prosthetic management, the effect of the prosthesis on movement and
the alignment of the prosthesis.

Page 51
CHAPTER 7
THE ROLE OF THE COACH
After the initial fitness program of the physiotherapist is complete and the
athlete has starting running on their running prostheses, the coach becomes involved
in further developing the sport specific skills required for running.
The coach trains the athlete based on a technical model, or their interpretation
of the ‘ideal’ technique of running. The coach aims to teach the athlete to replicate
this model as closely as possible. The athlete’s ability to imitate this model is the
athlete’s individual ‘style’. When coaching amputee athletes, the coach needs to be
flexible with their model as slight modifications may be necessary. This requires the
coach to have a good understanding of the biomechanics of amputee running to
determine whether any deviations that present are technically related or are influenced
by the amputation.
By observing and interpreting the running technique of the amputee, the coach
can identify areas for improvement in comparison to the model. Modification of
existing techniques and the introduction of new techniques aid in producing the
fastest, most energy efficient running style and maximises the athlete’s performance.
The techniques and training programs used in coaching able-bodied athletes
can be applied to coaching amputee athletes although some exercises may require
modifications. Training with able-bodied athletes also provides a number of benefits
for the amputee athlete including improved performance, greater motivation and
increased self-discipline (Nunn, 1992). Training and competing with able-bodied
athletes also gives the coach an indication of the amputee’s style compared to other
styles that more closely replicate the technical model. There are however a number of
considerations that should be taken into account when coaching amputee athletes.
These include the individual characteristics of the athlete, injury prevention and
management, communication and sport specific fitness and skill development.

Page 52
INITIAL ASSESSMENT Similar to the physiotherapist and prosthetist, the coach assesses the physical
condition of the athlete. The coach conducts a personal assessment of the athlete and
structures a personal training program from the information obtained.
To begin, the coach will discuss the athlete’s ability and medical history with
the athlete, including current general health, previous injuries and any other issues
(e.g., scoliosis).
The coach then focuses on the technical assessment of the athlete during
walking. Ideally, the athlete will have a precise walking gait as a result of the
physiotherapist’s treatment and management. The athlete’s walking style provides an
indication of the way they will run (particularly if they are lower limb amputees).
Upper extremity amputees walk well and often show no evidence of deficiencies that
may present during running. It is difficult to make any assumptions between upper
extremity amputee walking and running.
The coach views the overall skeletal movement of the athlete. Skeletal
movement demonstrates muscle control. The coach begins the analysis at the hips
(analysing core function and stability) and assesses down the legs, then returns to the
hips and analyses the upper body. The coach then returns to an overall review of the
athlete.
It is important to fully assess the hips, as any deviations may be a reflection of
deviations present at the ankle and knees. The analysis involves assessing the amount
of pelvic/hip movement. There is a certain level of pelvic movement necessary in
running, however exaggerated pelvic movement indicates a structural problem or a
weak, unstable core. To further confirm this, the athlete should lie down and the coach
will check the position/alignment of the body segments in relation to the naval. This
identifies the natural alignment and symmetry of body segments.
With the athlete walking towards them, the coach analyses the lateral hip
movement. Looking more distally the coach should assess the inversion and eversion
of the prosthesis and foot. Any deviations that are present which are not a result of
muscular weakness suggest prosthetic issues and should be assessed by the
prosthetist.

Page 53
The coach should then focus on the upper body movement. Identifying the arm
movement during walking indicates the possible deviations that will present during
running.
After the technical evaluation is complete, the coach should have an
approximate idea of the strengths and weaknesses of the athlete, as it is possible for
technical faults to indicate functional weaknesses and deficiencies.
The assessment then moves to the gym to determine the extent of the athlete’s
strength and indicates where a weights program should begin and focus. The
physiotherapist (with the coach's input) will previously have introduced a
strengthening and flexibility program. However as the athlete improves, the coach
introduces a more defined gym program that addresses sport specific skills and
fitness. Squats and bench press are used as measurement instruments to quantify the
strength of the athlete (FIGURE 23).
Figure 23 - STRENGTH TESTING. Squats and bench press provide an indication of the strength of the
athlete (courtesy of the Australian Institute of Sport).

Page 54
Arm and trunk strength, stability and control are vital elements in running and
their necessity is evident in amputee running. The emphasis of the initial
strengthening program of the coach is to maintain general fitness levels and
strengthen the arms and trunk. It is important to strengthen and accentuate the arm
movement, as the legs will follow the arms. As the arm technique improves the
posture should then become the focus. Following from this the legs become the focus
of the strengthening program.
After the coach has implemented a strengthening program and the athlete has
progressed, the physiotherapist should assess the strength of the athlete to determine
any improvement from their perspective.
DEVELOPING A TRAINING PROGRAM When developing a training program for amputees, there a number of basic
principles the coach should consider. These include; individualism, periodisation,
injury prevention and management, communication, employment of other
professionals, general fitness, sport specific fitness and skills and variation within the
program. Essentially, these principles are the same for able-bodied running. However,
there is increased emphasis on particular principles and there are amputee specific
considerations to address.
Individual Characteristics
In any case, it is important that the coach designs a program that is suited to
the individual athlete. The coach should have good knowledge and understand the
specific considerations that relate to amputee running. Modifications to exercises are
adapted into the training program to cater for the amputation and allow the athlete to
gain the most out of each exercise. To avoid constantly loading the limb, the program
may include non-weight bearing exercises to maintain fitness levels (i.e., pool
sessions). Simultaneously implementing non-weight bearing exercise and increasing
the amount of recovery sessions assists in injury prevention and management.
Amputees often have thermoregulatory difficulties. Generally, amputees
perspire more as a result of the increased work demands and the decreased surface

Page 55
area for heat dissipation. The residual limb is not exposed to the ambient air due to
prosthetic use and makes evaporation of the perspiration difficult. This limits the
cooling effect of evaporation and the body overheats.
Fatigue is also a major factor to consider in amputee training programs. The
increased work demands and the need for increased energy generation, increases the
energy required during gait and increases the cardiovascular demands of the athlete.
Amputees tire quicker as a result of the increased work done and the increased energy
cost associated with amputee running. It is important to increase the recovery times
within and between training sessions, as amputees require increased recovery time to
return their body to homeostasis.
Injury prevention and management
The design of a training program must also be based on the athlete’s individual
characteristics, strengths and weaknesses. This includes accounting for the amputation
(i.e., modifications to exercises) and allowing sufficient recovery times between and
within training sessions.
Throughout the program implemented by the coach, injury prevention should
be a major consideration. Injury to an amputee athlete (particularly lower limb) is
extremely detrimental to their independence and mobility. Injury disrupts the training
program and limits the amputee to walking aids. This should be a high priority in the
coach's mind as the training program is designed. The training program must also be
periodised and individualised. Periodisation is the structure of a training program so
that the athlete will achieve the peak of their season at a particular time.
Communication
Communication is extremely important between the coach and the multi-
disciplinary team and in particular with the athlete themselves. Communication within
the multi-disciplinary team is important in achieving the most from the athlete
together. One aspect of management may indirectly influence other aspects and is
therefore necessary to determine the overall approach to training the athlete.
Management by one member of the team may indirectly influence other aspects of the
athlete’s management. Therefore, it is important to discuss management methods
within the multi-disciplinary team.

Page 56
Constant feedback from the athletes on their condition and how they feel is
important in modifying training programs. If the athlete is feeling lethargic,
inadequate recovery between training sessions may be indicated as a possible cause
and can predispose the athlete to injury.
Sport Specific Fitness
Relative strength training programs have similar benefits between able-bodied
athletes and disabled athletes. However, relative strength training is the most effective
way of stimulating the nervous system and increasing the strength of disabled athletes.
Generally, in maximum strength training, amputee athletes cannot handle as
heavy weights as able-bodied athletes. Relative strength training uses lighter weights
with a controlled stimulus, where the timing of the concentric and eccentric
contractions of the exercise is the focus (FIGURE 24).
Figure 24 - RELATIVE STRENGTH TRAINING. Relative strength training requires timing the
concentric and eccentric contractions of the exercise (courtesy of the Australian Institute of Sport).

Page 57
If the athlete struggles with an exercise due to a particular weakness, the
physiotherapist will implement supplementary exercises. Supplementary exercises are
co-ordinated within the training program to assist in overcoming specific weaknesses.
They strengthen weak muscles in isolation and ensure the athlete gains the maximum
from each exercise of the relative strength program. As a result, the relative strength
training program becomes more beneficial to the amputated side. This demonstrates
the co-ordination necessary within the multi-disciplinary team.
Sport Specific Skill Development
Explosive and reactive strength is the ability of the athlete to produce the
greatest amount of force in the shortest amount of time. Plyometric exercises are used
in the training program to assist in producing explosive and reactive strength and if
implemented correctly will aid in injury prevention. Plyometric exercises require
modifications to allow amputees to gain the full benefit of each drill and exercise.
Rather than modifying the actual exercise and losing the full effect of the drill, the
number of repetitions and sets undertaken during the training session is manipulated.
Particular exercises may also be gradually introduced into the training program (e.g.,
box jumps). Alternatively, plyometric exercises can be beneficial in a pool. It is not
necessary to wear the prosthesis in the water as the water in effect, stabilises the
athlete while they practice.
• BEND RUNNING
Sport specific skills development also involves teaching the athlete to run
bends. The inside (left) side drives and propels the athlete around the bends and the
main thrust is from the hips. The hips are also vital in changing direction in bend
running.
Using the outside/right leg to provide the drive around the bend is
contraindicated. It increases the stride length on that side and as a result the inside
leg’s hip movement is limited and stride length reduced. Limiting the hip movement
means the athlete cannot fully utilise both hips for the thrust necessary to powerfully
get around the bend. Leaning into the curve also limits the hip movement and stride
length of the inside leg.

Page 58
Figure 25 - BEND RUNNING. The inside arm and leg drive and propel the athlete around the bend
(www.advancedprosthetic.com).
Left-sided amputees (either upper or lower extremity) must use their affected
side to propel and drive themselves around the bend. This is a huge disadvantage in
comparison to right-sided amputees, who have their intact side for the drive and
propulsion (FIGURE 25). However, when running bends, right lower limb amputees
tend to contact the ground in an inverted position. The inverted orientation of the
prosthesis means less of the prosthesis is in contact with the ground. The athlete
pushes off the side of their toe and as a result the hip drops off and energy expenditure
increases. In an attempt to overcome this, the amputee may introduce hip/lumbar
rotation to increase the amount of prosthesis in contact with the ground, however the
athlete will still push off the edge of the prosthesis if it has a rounded toe.
Above knee amputee athletes also have difficulty in running bends. External
rotation of the hip causes internal rotation of the socket. As a result the prosthetic foot
does not track well and follows through with a lateral whip. This requires
strengthening of the hip internal rotators and adductors, in an attempt to minimise the
degree of hip external rotation and the resultant socket internal rotation and lateral
whip. It is difficult to make prosthetic alterations, as the bends are only a small
portion compared to the straights of the track.

Page 59
• TAKE-OFF/START
As in able-bodied take-offs and starts, the individual determines the best
method or style they will adopt. There are benefits of having the prosthesis as the
back foot or the front foot. With no real studies in this area, it is difficult to discuss the
most appropriate methods of training relating to take-off and starts. It should be
entirely based on the athlete’s personal preference. FIGURE 26 shows Earle Connor, an
above knee sprinter who holds the 100m world record (12.61 secs) in the above knee
amputee class (T42) practicing his start, note that his prosthesis is used on the back
block.
Bilateral amputees have a number of considerations regarding their take-off
style. A standing start does not provide any benefits other than they are balanced
when they take off. The bilateral lower extremity amputee has less proprioception and
less power generation through their prosthesis onto the blocks. Current theories are to
have a ‘leap style’ start where the blocks are of equal length and the athlete leaps off
the blocks and jumps into their take-off.
Figure 26 - TAKE-OFF. Pictured is an above-knee sprinter in a crouched starting postition
(www.healthcare.ottobock.com).

Page 60
MODIFICATIONS TO EXERCISES Exercises for amputee athletes do not require drastic modifications. Usually, if
the exercise is modified to suit the athlete the benefits and effects of the exercise
change. If an exercise appears dangerous it should be excluded from the athletes
program.
Often, the only modification to the exercises prescribed by the coach is the
number of repetitions and sets the athlete must complete. As the athlete becomes more
experienced at the exercises, the intensity of the program is slowly increased.
Strengthening Programs
During resistance training, there are a number of major muscle groups to
strengthen and there is a vast range of exercises to achieve this. A running resistance
strength training program should emphasise working on the legs and should assist in
the cyclic action required in running. With increased resistance these types of
exercises become particularly difficult for lower extremity amputees. If the athlete has
difficulty executing an exercise, a similar exercise providing the same benefits should
be prescribed. The introduction of different exercises for each major muscle group
also provides variation within the training program. For example, alternate leg
exercises in training sessions between squats and leg press. This prevents the athlete
becoming bored with their strengthening program while gaining similar benefits from
each exercise.
Plyometric exercises
Plyometric exercises can also be practised in a pool without a prosthesis. The
water stabilises the athlete and the full effects of the exercise are achieved. The non-
weightbearing environment aids in injury prevention, as the limb is not constantly
loaded and simultaneously the athlete gains the benefits of the exercise.
Lower limb amputees may require alterations to jumping exercises. The
residual limb is not as tolerant of the impact loads associated with jumping and as a
result these types of exercises need to be modified and gradually introduced into the
athlete’s training program.
Box jumps require both modifications and should be slowly introduced into
the athlete’s training program. The amputee athlete should first commence with

Page 61
vertical jumps. As the athlete progresses they are introduced to a low height to jump
from. The intensity (number of sets and repetitions) increases, as the athlete becomes
stronger and more efficient.
Above knee athletes have larger restrictions on their capacity to practice
particular exercises. When designing a program for above knee athletes the coach
should consider the athlete’s safety and their knee unit. The knee unit can pose a
problem in relation to stability and the athlete’s ability to control the knee unit during
drills. Some exercises for above knee athletes are unsuitable (i.e., bounding or split
squat jumps) and others require modifications. Step-ups for above knee amputee
athletes are difficult. With a height of 10-15 centimetres the athlete can step onto the
shelf and continue the movement over the box to the other side where they step down
off the box. This provides the same benefits and is as effective as step-ups. It is also
safer for the above-knee athlete.
Modifications to plyometric exercises for upper limb amputees are necessary
if the exercise requires the athlete to hold something in both hands. This includes the
use of a medicine ball during particular exercises.

Page 62
SECTION 3
TROUBLE SHOOTING
INJURIES
GAIT DEVIATIONS This chapter reviews a number of injuries that effect amputee athletes. This is
only a basic review and other injuries related to running in general (i.e., shin splints
etc) can be found in other references specialising in this area.
Injury to the intact or prosthetic limb is disruptive to the competitive amputee
athlete. The mobility of the athlete is restricted and at times walking aids are
necessary. It is important to understand the mechanism of injury to prevent further
recurrence. The identification, diagnosis and management of an injury influences the
rehabilitation period and the recovery process. It is imperative that injuries are fully
rehabilitated before the athlete returns to full training and any prosthetic modifications
should be attended to by the prosthetist.
It is important to understand the cause of the gait deviation to allow for the
correct modifications and alterations to be implemented. Gait deviations can be
attributable to muscle imbalances, the prosthesis, technique or a combination of these
factors.
Any deviations during walking gait are amplified in the athlete’s running style
and it is important for the athlete to have an ‘ideal’ walking gait before the fabrication
of their running prosthesis. The management of running and walking gait deviations
are similar. The speed at which gait deviations occur during running is fast and
difficult to identify to the untrained eye. Video analysis is a common tool in
identifying gait deviations during running.
This chapter discusses the running gait analysis of the physiotherapist,
prosthetist and coach in relation to what they look for. It provides a list of common
gait deviations, their causes and possible management methods.

Page 63
CHAPTER 8
INJURIES
As a result of the biomechanical deficits and the compensations adopted to
enable amputee’s to run, the prosthetic limb is predisposed to injury and the intact
limb is more susceptible to common able-bodied running injuries including plantar
fasciitis, shin splints, muscular sprains and strains and joint problems (please refer to
other resources that specialise in this area).
Risk factors The risk factors associated with able-bodied athletes are applicable to amputee
athletes. Amongst many these risk factors include; fatigue, training frequency and
training surface. Amputee specific risk factors include prosthetic fit and alignment,
training intensity and gait deviations. Inadequate recovery within and between
training sessions often predisposes the amputee athlete to overload injuries, on either
the intact or prosthetic side and is a major consideration in the design of a training
program. The coach and physiotherapist implement injury preventative techniques as
a component of a training program. These techniques include ensuring adequate
recovery and pool work (a non-weightbearing exercise).
Injury management The period the athlete will be limited in their training is influenced by the
initial management (immediately after the trauma), correct and accurate diagnosis,
specific treatment methods to allow healing and an extensive rehabilitation program to
return the athlete to their previous training levels.
Prosthetic modifications may also be required to assist in overcoming injury or
eliminating possible causes. For example, frictional and shear forces can occur
between the liner and residual limb requiring consideration of the socket fit and the
actual interface.

Page 64
Increased perspiration, inadequate stump care, poor hygiene and poor
maintenance and management of the prosthesis all contribute to injury (e.g., skin
irritations). To overcome skin irritations the athlete should doff the prosthesis
throughout the training session to wipe the perspiration from their residual limb and
liner.
Incorrect donning and inadequate socket fit can produce pressure areas on the
residual limb. With constant loading in these areas it can cause the skin to break
down. Further complications can develop (i.e., infection), however if the athlete
maintains constant contact with their prosthetist, the prosthetic derived injuries can be
minimised.
Massage is commonly used as an injury preventative and management
method. It provides both psychological and physical benefits. It is used in soft tissue
injury management as it increases blood flow to the muscles. As a result, this
increases the nutrients and oxygen delivered to the musculature. It also assists in
breaking down adhesive scars. This is particularly applicable to athletes with
excessive scarring on their residual limbs.
Injury prevention Introducing preventative measures into the athlete’s training program is the
preferred method of injury management. There are a number of factors that contribute
to minimising injury development and are briefly discussed in the coaching section
(training program considerations) section of the manual.
A well-designed training program allows adequate recovery within and
between training sessions. Insufficient recovery encourages overload injuries to
develop, as the musculature has not had enough time to adapt and repair itself from
the workload of the previous training session.
Education of the preventative aspects of injury is a major contributor in injury
prevention and management. Knowledge of prosthetic management, correct donning
procedures, socket positioning, stump care and hygiene aspects can all reduce the
amount of injuries sustained through poor stump and prosthetic management. For
example, most skin irritations are a result of increased perspiration and the best way to
manage this is to constantly doff the prosthesis and wipe the residual limb dry. It is

Page 65
assumed the athlete will have basic knowledge in stump and prosthetic care and
management from their previous experience with their everyday leg. As mentioned
previously the prosthetist should emphasise hygiene management (perspiration
issues), stump monitoring (for redness, breakdown, irritations) and prosthetic
management (donning, prosthetic maintenance) when the running prosthesis is
initially provided.
Injuries on the intact limb can sometimes be avoided through orthotic
intervention. Foot orthoses play a role in impact absorption and assist in maintaining
the structural integrity of the foot.
Although not discussed in detail, it is essential to understand the nutritional
requirements of an athlete, not only from an injury preventative and management
perspective but also in relation to improving performance. The nutritional
requirements of an amputee athlete follow the same guideline as able-bodied athletes.
Common injuries Amputee specific injuries usually involve the prosthesis. Such injuries are a
result of the forces produced and their distribution, poor socket fit causing movement
of the residual limb within the socket (i.e., pistoning, shear and frictional forces) and
gait deviations.
Amputee runners commonly incur back pain as a result of their spinal position
and muscular weaknesses. The spine adapts a scoliotic position to adapt to their limb
loss and to maintain balance. As a result, gait deviations and muscular imbalances
develop. This further emphasises the need for core strength and stability.
The increased loads and inadequate shock absorption on the prosthetic side
increases the incidence of joint degenerative conditions on the prosthetic and intact
limbs. Poor technique and inadequate prosthetic fitting and alignment also contribute
to excessive joint loading and joint degeneration.
The table below summarises amputee specific running/athletic injuries. It is
important that any injury is correctly diagnosed and sufficiently rehabilitated before
the athlete returns to previous training levels.

Page 66
Injury Signs and symptoms Mechanism of injury Management
Skin Irritations Rash on stump
Flakey or peeling skin
Dermatitis/eczema
Itchy
Redness of affected areas
Perspiration/heat
Reaction to liner
Shear/frictional forces at stump-
socket interface
Dry skin
Creams and moisturisers
Emphasise stump and prosthetic
care and management
Skin breakdown Broken skin
Scab
Painful
Shear or frictional forces at
stump-socket interface
Adhesive scar pulls skin tight
causing friction
Pressure areas
Insufficient management of
skin irritation
Pistoning within socket
Rest until healed
Emphasise stump monitoring
Assess and modify socket fit
Assess alignment
Massage to break up scar tissue
Verrucose
hyperplasia
Distal skin appears
roughened and warty
Loss of distal contact with
socket, as a result the blood
pools distally in the residuum
and the vessels burst
Assess and modify socket fit
New total contact socket
Infected hair
follicle
Pimply
Rash
Perspiration
Hygiene
Allow to heal
Emphasise stump and prosthetic
care and management
Stump pain General stump soreness
Stump pain on loading and
after training
Discomfort on loading
Muscle soreness
Stump intolerance to pressure
and loading
Hypersensitivity
Insufficient shock absorption
Socket fit
Medication (legal)
Massage (for hypersensitivity and
scar adhesions)
Acupuncture
Assess liner characteristics
Decrease foot category
Assess socket fit
Phantom pain Pain in the portion of leg
that has been amputated
Nerve impulses continue
through cut nerve giving the
athlete pain sensations in their
amputated leg
Medication
Massage
Acupuncture
Blisters Liquid filled mass
Shear and/or frictional forces at
stump-socket interface
Avoid loading
Rest until healed

Page 67
Injury Signs and Symptoms Mechanism of Injury Management
Calluses
(stump or intact
foot)
Hard, toughened skin
Can be painful
Constant blistering
Adaptation to loading
Friction
Remove (podiatrist)
Don’t soften as it will cause
breakdown
Ulcers Deep wounds (especially
on bony prominences)
Friction and shear forces
(particularly if athlete has frail
or thin skin)
Pressure on bony prominences
Pressure on desensitised skin
Constant skin breakdown
Assess interface/liner
Socket fit
Assess loading of socket
Close monitoring of stump
condition
Posterior knee
capsule
Posterior knee swelling
Posterior knee pain
Knee instability
Genu recurvatum
Constant knee hyperextension
during loading
Stretching of the synovial
capsule of the knee
Physiotherapy (ultrasound)
Walking gait re-education
Technique modifications
Knee Orthosis
Increase foot category
Back pain Constant lower back ache
Restrictions in movement
Awkward gait pattern
Spinal malalignment
Musculature weakness
Core instability and weakness
Gait deviations
Compensatory adaptations
Previous injury
Prosthetic socket fit, alignment,
height
Lack of shock absorption
Core stability and strengthening
work
Walking gait re-education
Running technique modifications
Suffice rehab post-injury
Rest
Prosthetic modifications (height,
alignment, socket fit)
Decrease category of foot
Joint pain
(intact or
prosthetic side)
Soreness at joint/s
Avoid loading joint
Increased impact loads
Inability to absorb shock (ie,
shoes, prosthesis)
Training surface too hard
Gait deviations
Joint degeneration
Increase flexibility (ROM)
Get suitable shoes
Add shock-absorbing materials to
prosthesis
Decrease foot category
Change training surface (ie, grass)
Gait re-education (walking and
running)

Page 68
It is important to note these injuries can be avoided. This is through constant
stump monitoring, stump care and management, prosthetic care and management and
maintaining contact with the prosthetist to assess prosthetic fit and function. It also
emphasises the necessity of a perfect walking gait and an ideal running style to avoid
back pain and other structural and muscular injuries. Often the muscular injuries are
overload injuries and are a result of inadequate technique or in suffice recovery. The
compensatory measures are adapted to avoid loading the limbs for various reasons,
including pain. This influences the alignment of body segments and predisposes the
athlete to further injury.

Page 69
CHAPTER 9
GAIT ANALYSIS: DEVIATIONS AND MANAGEMENT
GAIT ANALYSIS Similarly to walking gait analysis, during running gait analysis it is important
to get both frontal plane aspects and a sagittal view. Gait deviations during running
are more difficult to identify because of the speed of movement. To assist in
identifying gait deviations, it is important to look at the compensatory mechanisms
that are employed. The compensations accentuate the original deviation and direct the
assessor to the underlying cause.
Ideally, the athlete will have a good walking gait, as any deviations present
during walking will be amplified during running. This is one of the criteria (as
stipulated by the physiotherapist) that must be fulfilled before the athlete is eligible
for a running prosthesis. It is vital to have a balanced and solid walking gait
foundation to achieve an efficient running style.
It is important to address and manage any gait deviations as soon as possible.
Excessive gait deviations may cause long-term problems for the amputee including
pain, structural deformities and degenerative changes. Managing these deviations is
usually achieved through a multi-disciplinary team approach. If an individual
manages the deviation they should pass on their findings and management methods to
the other multi-disciplinary team members, as changes in one aspect can often
influence other aspects of the athlete’s management.
When assessing the athlete’s running gait, the athlete should run
approximately sixty metres a maximum of eight times. Exceeding this will produce
gait deviations that are a result of fatigue.
High speed video analysis of the athlete’s running gait is a common tool used
in recognising deviations and their cause. The speed of the video can be decreased
during playback and the movement of the athlete can be assessed slowly and in more
detail. It also enables the viewer to focus on certain aspects of the athlete’s gait
including stride speed and length, symmetry and the functional joint range of
movement.

Page 70
Viewing the footage with other members of the ‘team’ may also be useful in
determining a management plan to overcome the deviation and prevent the adoption
of compensations. This further highlights the need for communication within the
multi-disciplinary team.
PHYSIOTHERAPIST
The physiotherapist is particularly interested in the muscle efficiency and
muscle recruitment during running.
• Assess upper body rotation is sufficient and symmetrical.
Look for stiffness of the athlete during running.
Look whether the athlete has excessive trunk movement and/or upper
body rotation.
Note whether the arms are being used for drive.
Review core strength and stability.
• Check posture.
Look for excessive lumbar lordosis, anterior trunk flexion or lateral
trunk bending.
Check core strength and stability.
• Assess pelvic movement is sufficient (not excessive) in each plane.
Look for anterior pelvic tilt, pelvic drop and excessive pelvic shift.
Check core strength stability.
• Check knee stability.
Look for varus/valgus during loading, hyperextension and drop off
(excessive flexion).
• Check the width of the base of support.
Feet should be underneath athlete running in one line. Too wide
indicates an abducted gait.
• Assess symmetry.
Note stride length and duration, joint angles, rotational movements and
check the limbs are following the same movement pattern.
• Note whether muscles are being recruited efficiently and used effectively.

Page 71
PROSTHETIST
The prosthetist is particularly interested on the athlete’s use of the prosthesis
and the prosthesis effect on movement.
• Check the foot is flat on the ground with good ground contact.
Look for inversion or eversion of the prosthesis.
Look at amount of toe on ground.
• Assess whether feet are evenly loaded and are fully weightbearing through
their prosthesis.
Ensure prosthesis is not being used as a prop and is being used
appropriately.
• Assess symmetry.
Check for symmetry (approximately) between stride length, stride
width, swing and stance phase duration, joint angles, rotational movements
etc.
• Assess knee stability during stance.
Look for varus/valgus, knee hyperextension or drop off (excessive
flexion).
• Check abduction/adduction of the socket.
Check for good, even, flat contact with the ground.
• Assess knee movement during swing (lateral view).
Check there is no limitations or restrictions in movement.
Check trimlines and suspension is not impinging on knee movement
(especially knee flexion).
Make sure there are no medial or lateral whips.
• Assure full hip movement.
Note whether any restrictions are prosthetically related (i.e., influence
of trimlines or suspension).
• Assess adequate trunk movement.
• Analyse degree of hip internal/external rotation.
Check prosthesis tracks/follows through straight during swing.
Check for whips (particularly in above knee athletes).
• Assess the movement of the foot in transfemoral and through knee athletes.
Check for whips and terminal swing impact.

Page 72
COACH
Initially, the coach takes a holistic approach to analysing the running gait of
the athlete. The coach will then analyse the athlete in parts (upper limb and lower
limb) and then review the athlete as a whole.
• Check the athlete’s balance and posture.
Ensure the athlete demonstrates core stability.
Check for a good posture – reasonably upright, symmetry between the
stomach and back muscles (i.e., not leaning back, not leaning forward).
• Look at the iliopsoas.
Check it provides the initial drive during take off.
• Look at the gluteals.
Ensure gluteals provide the drive.
• Watch the leg movement during recovery.
Ideally the foot should follow through the knee while maintaining hip
flexion and a horizontal thigh.
Ensure quadriceps are utilised during recovery and not the gluteals.
• Check the pelvic position.
Ensure pelvis and hips are forward and up (to an extent) with no
rotation.
Review core strength and stability.
• Assess trunk movement.
Look for adequate trunk movement - excessive trunk movement
indicates possible balance problems and core instability.
• Check arm movement is symmetrical and controlled.
Arm action should be controlled in action and drive.
• Assess symmetry.
Check stride speed is even between limbs.
Check arm and leg movements are similar on both sides (i.e., no
balancing compensations etc).
• Review the athlete as a whole. Check the arm and leg movements are
coordinated and symmetrical.

Page 73
GAIT DEVIATIONS
GENERAL DEVIATIONS
• Lateral Trunk Bending
Presentation - athlete leans towards their amputated side during prosthetic stance. The
athlete has difficulty stabilising on the prosthetic side.
CAUSE MANAGEMENT
MUSCULAR Difficulty in stabilising on
prosthetic side
Strengthen extensors and adductors
on prosthetic side
Prosthesis length Assess and adjust height. Prosthetic
side should be approximately ¾”
longer than the intact limb (BK). PROSTHETIC
Foot too outset Inset foot under the athlete to
enable good ground contact
Introduce proprioception and
balance enhancing exercises
Compromised balance
Strengthen core
Introduce co-ordination exercises
Strengthen shoulders and trunk
Strengthen core
Uncontrolled trunk and arm
movement
Postural maintenance
TECHNICAL
Fatigue Increase recovery within and
between sessions

Page 74
• Excessive Anterior Trunk Flexion
Presentation – some anterior trunk flexion is necessary for forward progression in
running. It is necessary for the foot to contact the ground behind the centre of gravity
and moving at the same or slower velocity. However, if the athlete excessively leans
forward during running it limits the hip range of movement and as a result the stride
length is reduced.
CAUSE MANAGEMENT
Tight hip flexors/anterior
capsule
Decreased flexor range
Stretch and strengthen flexors
MUSCULAR
Poor core stability Core stability and strengthening
exercises
Foot too anterior, athlete has
to lift to get over the toe
Move foot back under athlete
PROSTHETIC
Socket too flexed Modify alignment
Teach to strengthen and utilise
trunk and arms
Co-ordinated arm movement
exercises
Unbalanced style
Posture and core stability exercises
Overcompensating Teach to run more upright
TECHNICAL
Fatigue Increase recovery within and
between sessions

Page 75
• Pelvic Shift
Presentation – pelvic shift occurs in each plane. Pelvic shift occurs naturally during
running however can become excessive. Excessive pelvic movement is a result of the
athlete’s inability to stabilise the core. Pelvic movement causes a displacement of the
centre of gravity and increases energy expenditure. Excessive pelvic movement does
not allow the athlete to fully utilise the characteristics of the prosthesis as the foot is
ineffectively loaded and unloaded.
CAUSE MANAGEMENT
Pelvis tilts anterior to
ground
Strengthen abdominals and core
Poor stability of hip on
prosthetic side
Strengthen abdominals, core and
hip extensors MUSCULAR
Unable to stabilise the core Include more core stability work in
program
Excessive foot compression
(category too soft)
Use a stiffer category – refer to
selection form.
Prosthesis too short Prosthesis should be approx ¾”
longer than intact side during static
alignment PROSTHETIC
Inversion/eversion of foot at
push off
Reposition foot to allow as much of
the foot is in contact with the
ground as possible
Teach athlete to run with as much
ground contact as possible
Don’t allow athlete to favour
prosthetic side
Poor prosthetic contact with
ground
Encourage loading of the prosthesis
Stretch and strengthen hip flexors
TECHNICAL
Lumbar spine rotation
(partial core instability) Core stability exercises

Page 76
• Prosthetic Pull-Off
The athlete lifts the leg into swing rather than pushing off with the prosthesis.
Occurs in both below knee and above knee athletes. The hip muscles and the
proportion of the prosthetic foot in contact with the ground influences the amount of
push-off. Prosthetic pull-off does not use the power generated by the hip extensors
efficiently.
CAUSE MANAGEMENT
MUSCULAR Tight hip flexors/anterior
hip capsule
Stretch and strengthen hip flexors
PROSTHETIC
Ineffective use of prosthesis
In suffice ground contact ∴
ineffective push off
Position socket and align prosthesis
allowing good ground contact and
enabling an effective push-off
TECHNICAL
Ineffective use of hip
extensors and their energy
to assist push-off
Drills focusing on hip extensor
recruitment
• Uneven Stride Length
Presentation – the prosthetic or intact leg has an increased stride length compared to
the contralateral side.
CAUSE MANAGEMENT
MUSCULAR Limitations in the hip or
knee ROM
Stretch out tight structures
Prosthetic alignment Realign to allow full hip and knee
movement
Impinging suspension Assess suspension PROSTHETIC
Trimlines too high Lower trimlines
Poor gait Walking gait re-education
TECHNICAL Fatigue causes athlete to
overstride
Enhance cardiovascular fitness

Page 77
• Toe Drag
Presentation – during swing the toe drags as a result of inadequate toe clearance.
CAUSE MANAGEMENT
MUSCULAR Weak knee flexors Strengthen knee flexors
Prosthetic length Shorten prosthesis (pros should be
approx ¾” longer) PROSTHETIC
Ineffective suspension Modify suspension
PROSTHETIC
(transfemoral)
Knee flexion restricted Decrease knee resistance
Increase recovery times during and
between training sessions
Fatigue
Enhance cardiovascular fitness TECHNICAL
Unsuitable gait Modify walking gait pattern

Page 78
• Increased Knee Flexion (Drop Off)
Presentation – throughout the gait cycle, excessive knee flexion can present in a
number of ways. At initial contact the knee is excessively flexed and the athlete tends
to ‘drop off’, coming off their prosthetic toe and falling quickly to the sound side.
CAUSE MANAGEMENT
MUSCULAR Weak knee extensors Strengthen knee extensors
Toe lever too short / foot too
posterior
Reposition foot more anterior
Inability to control energy
storing characteristics of the
prosthetic foot
Align prosthesis with more stability
(ground reaction force anterior to
knee)
PROSTHETIC
Socket to flexed Assess and modify alignment
PROSTHETIC
(transfemoral)
Inadequate knee flexion
resistance in knee unit
Increase flexion resistance
TECHNICAL
Inability to use musculature
to stabilise and control
prosthesis.
Implement knee stability and
control exercises and drills

Page 79
• Knee Hyperextension
Presentation – the knee is fully extended throughout stance phase. Forces are not
absorbed through the eccentric quadriceps and as a result can cause a number of
injuries. Continuous joint loading can eventually lead to degenerative changes in the
lower limb joints.
CAUSE MANAGEMENT
MUSCULAR
Poor muscle control
(particularly vastus
medialis)
Strengthen knee musculature
(esp. eccentric quadriceps)
Insufficient socket flexion Assess and modify alignment
PROSTHETIC Foot too anterior / toe lever
too long
Reposition foot more posterior and
under the athlete
Increase foot category PROSTHETIC
(transfemoral)
Excessive vertical
compression in foot Use a Flex-Sprint I or II
Strengthen and utilise trunk and
arms TECHNICAL
Unbalanced running style Postural maintenance, core strength
and stability work

Page 80
• Lumbar Lordosis
Presentation – the lumbar lordosis of the athlete is accentuated during running and the
trunk leans posteriorly. It is a compensatory measure adopted to overcome poor pelvic
stability and inadequate abdominal strength and control. It limits the stride length of
the athlete as there is a decreased range of hip extension and is difficult to achieve a
good range of hip flexion. This deviation occurs in both below knee and above knee
athletes.
CAUSE MANAGEMENT
Tight iliopsoas Stretch out iliopsoas
Hip extensor weakness Strengthen extensors
Core weakness and
instability
Strengthen core especially
abdominals MUSCULAR
Restricted hip movement Stretch hip musculature to improve
flexibility
Loss of socket fit Assess socket fit and alignment
PROSTHETIC
(transfemoral)
Insufficient socket flexion Modify alignment
Walking gait re-education
introducing upper body rotation TECHNICAL
Limited arm movement and
upper body rotation
Core strength and stability work

Page 81
• Excessive Heel Rise
Presentation – the prosthetic foot rises higher than the sound side’s foot. The
prosthetic foot can even hit the posterior aspect of the socket. There is forceful hip
flexion and as a result the foot flicks up behind the athlete, increasing prosthetic swing
duration and producing interlimb asymmetry.
CAUSE MANAGEMENT
MUSCULAR Decreased hip extensor
movement
Stretch and increase hip extensor
flexibility and mobility
Insufficient knee unit
flexion resistance
Increase knee unit flexion
resistance
Prosthetic knee axis higher
than anatomical knee
Reposition and align knee unit PROSTHETIC
Flexion bumper on the posterior
distal aspect of the socket
TECHNICAL
Inability to push off with
prosthesis
Introduce a prosthetic push off
technique to limit the use of the hip
flexors

Page 82
• Medial/Lateral Whip
Presentation – the heel twists at toe off and follows a medial or lateral direction
throughout swing.
CAUSE MANAGEMENT
MUSCULAR
(transfemoral)
Flabby musculature causes
socket and musculature to
internally/externally rotate
around bony reminant
Strengthen and tone musculature
Internal or external socket
rotation in relation to line of
progression
Socket fit too tight or does
not accommodate contour of
muscles
Modify socket fit and suspension
Toe break not in line of
progression
PROSTHETIC
Insufficient foot contact
with ground
Assess and modify alignment
PROSTHETIC
(transfemoral)
Knee not horizontal with
ground (AK)
Assess and modify assessment
Insufficient contact with
ground causes foot to twist
during stance
Teach athlete to control and utilise
energy characteristics of the foot
TECHNICAL
Not fully weightbearing
through prosthesis
Determine why not fully
weightbearing (i.e., pain, insecure)

Page 83
• Abducted Gait
Presentation – the athlete has a wide running base where the legs do not follow a
single line underneath the athlete. It also involves excessive pelvic and trunk
displacement and is often associated with lateral trunk bending.
CAUSE MANAGEMENT
Weak hip extensors Strengthen extensors
MUSCULAR Hip muscular imbalances
(abductors and adductors)
Strengthen hip adductors
PROSTHETIC
(transtibial) Prosthesis too long
Pros approx ¾” longer
than intact
Stump not in socket
Medial wall to high
Socket does not support
femur in adduction
Assess and modify socket
fit PROSTHETIC
(transfemoral)
Prosthesis too long Prosthetic side approx
same height as intact
Running weave drills
(works adductors) TECHNICAL
Inability to control trunk
and maintain good posture
Core stability work

Page 84
• Circumduction
Presentation – the entire prosthesis tracks laterally in swing and returns to the correct
position for heel strike. This deviation can occur in both below knee and above knee
athletes, usually above knee unless otherwise stated).
CAUSE MANAGEMENT
MUSCULAR Weak hip extensors Strengthen hip extensors
PROSTHETIC Prosthesis too long Pros approx ¾” longer
than intact
Knee unit position / knee
too stable
Modify and adjust socket
and knee position
Excessive knee flexion
resistance
Decrease knee flexion
resistance
Medial socket wall too
high
Assess and modify socket
fit
PROSTHETIC
(transfemoral)
Prosthesis too long Pros approx same height
as intact (level knees)
Athlete lacks confidence
loading knee, does not use
knee effectively (AK)
Teach to trust knee unit
during loading
Knee lifts
TECHNICAL
Foot does not follow
through knee arc Increase hip flexibility

Page 85
• Vaulting
Presentation – rising up on the toe of the intact leg to accommodate for prosthetic
swing. Vaulting occurs in both below knee and above knee running gait. Management
is generally the same unless otherwise specified.
CAUSE MANAGEMENT
MUSCULAR Weak hip flexors Strengthen hip flexors
Prosthesis too long Shorten leg
PROSTHETIC Excessive knee flexion
resistance making it
difficult to break the knee
(AK)
Decrease knee flexion
resistance
Athlete not confident to
load knee (AK)
Teach athlete to trust knee
unit during stance (explain
exercises) TECHNICAL
Athlete does not utilise
prosthesis’ characteristics
Educate athlete on ways to
utilise foot and knee unit

Page 86
BELOW KNEE SPECIFIC DEVIATIONS
• Knee Mediolateral Instability
Presentation – knee adopts a varus or valgus position during stance. Prosthetically,
mediolateral knee movement relates to the amount of toe on the ground.
CAUSE MANAGEMENT
MUSCULAR Muscular weakness and
instability
Strengthen knee musculature
Foot too inset or outset Reposition foot
Socket position in frontal
plane
Adjust alignment PROSTHETIC
M/L diameter of socket too
wide
Assess and modify socket fit
Enhance endurance capacity of the
athlete TECHNICAL Fatigue
Increased recovery periods within
and between training sessions

Page 87
ABOVE KNEE SPECIFIC DEVIATIONS
• Terminal Impact
Presentation – at the end of swing the prosthetic shank hits full extension and bounces
back. This reduces the stride length because when the foot bounces back off the knee,
it is positioned back under the athlete when the foot is loaded.
CAUSE MANAGEMENT
MUSCULAR Lack of proprioception Proprioceptive development
exercises
Friction and extension bias
unbalanced
Modify friction and assistance of
knee unit PROSTHETIC
Absent knee extension
bumper
Replace bumper or entire knee unit
Teach athlete smooth technique
TECHNICAL Over-striding Teach athlete to increase stride
speed and frequency to run faster,
rather than over striding

Page 88
REFERENCES
• Bowker, J.H. and Michael, J. W. (1992) ‘Atlas of Limb Prosthetics: Surgical,
Prosthetic and Rehabilitation Principles, 2nd edn.’ American Academy of
Orthopaedic Surgeons.
• Brouwer, B.J., Allard, P. and Labelle, H. (1989) ‘Running Patterns of Juveniles
Wearing SACH and Single-Axis Foot Components’, Archives of Physical
Medicine and Rehabilitation; 70: 128-134.
• Czerniecki, J. M. (1996) ‘Rehabilitation in Limb Deficiency’, Archives of
Physical Medicine and Rehabilitation; 77: S3-S37.
• Czerniecki, J. M. and Gitter, A. (1992) ‘Insights into Amputee Running: A
Muscle Work Analysis’, American Journal of Physical Medicine and
Rehabilitation; 21: 209-218.
• Czerniecki, J. M. and Gitter, A. J. (1996) ‘Gait Analysis in the Amputee: Has it
Helped the Amputee or Contributed to the Development of Improved Prosthetic
Gait Components?’ Gait and Posture; 4: 258-268.
• Czerniecki, J. M., Gitter, A. J. and Beck, J. C. (1996) ‘Energy Transfer
Mechanisms as a Compensatory Strategy in Below Knee Amputee Runners’,
Journal of Biomechanics; 29(6): 717-722.
• Czerniecki, J. M., Gitter, A. and Munro, C. (1991) ‘Joint Moment and Muscle
Power Output Characteristics of Below Knee Amputees During Running; The
Influence of Energy Storing Prosthetic Feet’, Journal of Biomechanics; 24 (1): 63-
75.
• De Castella R. and Clews, W. (1996) ‘Smart Sport: The Ultimate Manual for
Sports People’, RWM Publishing Pty Ltd.

Page 89
• Enoka, R. M., Miller, D. I. and Burgess, E. M. (1982) ‘Below-Knee Amputee
Running Gait’, American Journal of Physical Medicine; 61(2):66-84.
• Fergason, J. and Smith, D. G. (1999) ‘Socket Considerations for the Patient With
a Transtibial Amputation’, Clinical Orthopaedics and Related Research; (361):76-
84.
• Gitter, A., Czerniecki, J. and Meinders, M. (1997) ‘Effect of Prosthetic Mass on
Swing Phase Work During Above-Knee Amputee Ambulation’, American Journal
of Physical Medicine and Rehabilitation; 74(2):114-121.
• Lees, A. (1999) ‘Running’ in Durward, B. R., Baer, G. D. and Rowe, P. J.
(editors) Functional Human Movement, Butterworth Heinemann.
• Macfarlane, P. A., Nielsen, D. H. and Shurr, D. G. (1997) ‘Mechanical Gait
Analysis of Transfemoral Amputees: SACH Foot Versus the Flex-Foot’, Journal
of Prosthetics and Orthotics; 9(4):144-151.
• Mensch, G. and Ellis, P.E. (1986) ‘Running Patterns of Transfemoral Amputees:
A Clinical Analysis’, Prosthetics and Orthotics International; 10:129-134.
• Miller, D. I. (1987) ‘Resultant Lower Extremity Joint Moments in Below Knee
Amputees During Running Stance’ Journal of Biomechanics; 20(5): 529-541.
• New York University: Postgraduate Medical School Prosthetics and Orthotics
(1982) ‘Lower Limb Prosthetics: including Prosthetists Supplement’.
• Nunn, C.J. (1992) ‘Coaching Amputee Athletes’, Goanna Print.
• Nunn, C. J. (1995) ‘Walk This Way’, Sport Health; 13(4) 6-7.

Page 90
• Prince, F., Allard, P., Therrien, R.G. and McFadyen, B.J. (1992) ‘Running Gait
Impulse Asymmetries in Below Knee Amputees’, Prosthetics and Orthotics
International; 16: 19-24.
• Sabolich, J. (1985) ‘Contoured Adducted Trochanteric-Controlled Alignment
Method (CAT-CAM): Introduction and Basic Principles’, Clinical Prosthetics
and Orthotics; 9(4): 15-26.
• Sabolich, J. (1987) ‘The O.K.C. Above-Knee Running System’, Clinical
Prosthetics and Orthotics; 11(3): 169-172.
• Sanderson, D. J. and Martin, P. E. (1996) ‘Joint Kinetics in Unilateral Below Knee
Amputee Patients During Running’, Archives or Physical Medicine and
Rehabilitation; 77: 1279-1285.
• Seroussi, R. E., Gitter, A. Czerniecki, J. M. and Weaver, K. (1996) ‘Mechanical
Work Adaptions of Above-Knee Amputee Ambulation’, Archives of Physical
Medicine and Rehabilaition; 77: 1209-1214.
• Smith, A. W. (1990) ‘A Biomechanical Analysis of Amputee Athlete Gait’,
International Journal of Sport Biomechanics; 6: 262-282.
• Thordarson, D. B. (1997) ‘Running Biomechnaics’, Clinics in Sports Medicine;
16(2) 239-247.

Page 91
SECTION 4
APPENDICIES
AMPUTEE CLASSIFICATIONS
IMPAIRMENT SPECIFIC SCREENING FORM
IMPAIRMENT SPECIFIC SCREENING EXPLANATORY NOTES

Page 92
APPENDIX I – AMPUTEE CLASSIFICATIONS
CURRENT
CATEGORY
PREVIOUS
CATEGORIES DESCRIPTION
F42 A2 & A9 single AK & combination
F43 A3 & A9 double BK & combination
F44 A4 & A9 single BK & combination
F45 A5 & A7 double AE & double BE
F46 A6 & A8 single AE & single BE
T42 A2 & A9 single AK & combination
T43 A3 & A9 double BK & combination
T44 A4 & A9 single BK & combination
T45 A5 & A7 double AE & double BE
T46 A6 & A8 single AE & single BE
LEGEND
Abbreviations AK – above or through the knee joint
BK – below the knee, but through or above the talo-crural joint
AE – above or through the elbow joint
BE – below the elbow, but through or above the wrist joint
Previous classifications A1 – double AK – both legs amputated above the knee
A2 – single AK – one leg amputated above the knee
A3 – double BK – both legs amputated below the knee
A4 – single BK – one leg amputated below the knee
A5 – double AE – both arms amputated above the elbow
A6 – single AE – one arm amputated above

Page 93
A7 – double BE – both arms amputated below the elbow
A8 – single BE – one arm amputated below the elbow
A9 – combination - upper and lower extremity amputations

Page 94
APPENDIX IIa – IMPAIRMENT SPECIFIC
SCREENING FORM
Name :
Sport :
Events :
Level of amputation
Walking prosthesis
Sporting prosthesis
Training prosthesis / aids / orthotics
• Residual Limb Diagram:
Length
Verrucose hyperplasia
Sensitivity / Pain
Redundant tissue
Sensation
Phantom pain
Scarring
Abrasions
• Posture
HEAD & CERVICAL SPINE
Normal
Lordosis
Pokeneck
Flat C/S
Side tilt Left Right

Page 95
Rotation Left Right
• THORACIC SPINE
Normal
Kyphosis
Flattened
Scoliosis
Shoulders level
Sloping
Rounded
• LUMBAR SPINE
Normal
Flattened
Lordotic
Scoliosis
Muscle bulk
Atrophied
Hypertrophied
• PELVIS
Normal
Shift Left Right
Anteriorly rotated
Posteriorly rotated
Check leg length – PSIS level
• FEMUR
Normal
Gluteal wasting Left Right
Internal rotation Left Right
External rotation Left Right

Page 96
• KNEE
Normal
Genu Recurvatum Left Right
Genu Varum Left Right
Genu Valgum Left Right
Quad wasting Left Right
Knee joint swelling Left Right
• PATALLAE
Normal
Lateral Left Right
Squinting Left Right
• FOOT POSITION
Normal Left Right
Hallux Valgus Left Right
High arch Left Right
Low arch Left Right
Evert Calcaneus Left Right
Invert Calcaneus Left Right
Foot turned in Left Right
Foot turned out Left Right
• Stability/Muscle Activation
7 stage abdominals
Activated abdominals Single leg Double leg
Resisted hip rotation Internal External
Hip capsule Left Right
Isolation of abdominal & gluteal activity
Unilateral hip extension Left Right
Unilateral knee flexion (activation sequence)
Eccentric quads

Page 97
Single leg stance
Step down
Single leg squats
Hops
Comments
• Gait analysis
Lateral trunk bending
Pelvic shift
Upper body rotation
Lumbar spine hyperextension
Knee hyperextension
Increased knee flexion (drop-off)
Uneven step length
Knee deviation
Whip medial/lateral
Terminal impact
Abducted gait
Circumduction
Vaulting
• Problems
• Recommendations

Page 98
APPENDIX IIb – IMPAIRMENT SPECIFIC
SCREENING EXPLANTORY NOTES
• Prosthesis type: documentation for both walking and sporting prostheses note:
- Socket type
- Suspension
- Liner
- Knee/elbow joint
- Foot/ankle complex or terminal device
• Residual limb: skin arising from suboptimal socket fit or prosthetic alignment
obviously will require prosthetic review.
Verrucous hyperplasia appears distally on the residual limb. The skin appears
roughtened and warty and this is due to loss of distal contact with the prosthetic
sockets.
Redundant tissues is an excessive amount of soft tissue tht extends beyone the bony
remanent. It may cause problems with socket fit and comfort which may respond to
different types of prosthetic liner.
Note whether the sporting activity has an impact on residual limb pain or phantom
pain.
Measurement of residual limb length:
- Transtibial – tibial tuberosity to distal tibia
- Tranfemoral – greater trochanter to distal femur
- Transradial – acromion process to distal humerus
- Transradial – olecranon to distal radius
• Posture: assess with the walking prosthesis donned. The sports specific
alignment of the sporting prosthesis usually does not allow the athlete to adopt a

Page 99
comfortable standing posture. The sporting prosthesis is designed and aligned
depending on the demands of the sport.
Ensure the feet are level and the weight is evenly distributed on both feet. The athlete
should look straigh ahead. If weight is taken unevenly on the prosthetic foot, an
alignment fault maybe indicated. The athlete should not have to exert effort to
maintain a comfortalble and symmetrical standing alignment.
• Stability and Activation:
1. Seven stage abdominals: in supine with the knees flexed to 90o. Walking
prosthesis is on.
2. Activated abdominals: measure the distance to the surface when abdominal
control is lost for single and double leg tests.
3. Resisted hip rotation: the athlete lies supine with the knees bent to 90o. Observe
deviation of the naval as they resist applied hip rotation force. Note any abdominal
muscle imbalances.
4. Hip capsule: determine any tightness in the hip capsule and iliopsoas muscle
independantly. The athlete is prone with the legs in a figure 4 position. Measure
the distance from the supporting surface to the raised ASIS.
5. Isolation of abdominal and gluteal activity: test in the above position. Also note
the ability to co-contract these muscles and any compensations evident.
6. Unilateral hip extension: in prone, time to fatigue bilaterally.
7. Unilateral knee flexion: note the activation sequence, i.e., activation of stabilisers
v’s hamstrings.
8. Eccentric quadriceps: test strength and control in standing. Pop onto prosthetic
toe. Note control of flexion/extension and where in range control is lost.
9. Single leg stance: Observe lateral pelvic tilt, rotation, lumbar spine lateral flexion.
Balance. Co-activation of abdominals and erector spinae.
10. Step down and single leg squat (trantibial athletes only - prosthetic side as able).
Note knee angle and deviation at fail, note any pelvic deviation at fail.
• Gait Analysis: if any of the mentioned gait deviations are present and considered
to be excessive then a prosthetic clinic review may be necessary to determine the

Page 100
cause and rectify the problem. A gait fault in walking will be magnified in running
or any other higher activity, which may predispose to injury. (Refer to gait
deviations in Chapter 8 – Gait deviations and management).
1. Lateral trunk bending – inadequate shift of the pelvis to the stance side with
compensatory trunk lateral flexion to the stance side. Upper body rotation is
lacking. Could indicate a problem with prosthesis and/or athlete.
2. Pelvic shift – excessive or inadequate?
3. Upper body rotation – is it equal on both sides?
4. Lumbar spine hyperextension – this is usually a compensation related to poor
pelvic stability and inadequate abdominal strength and control. Note hip range of
movement.
5. Knee hyperextension – in stance phase. This may indicate poor muscle control.
6. Increased knee flexion – is there drop-off before prosthetic toe-off?
7. Uneven step length – this will indicate a need for physiotherapeautic review and
gait training.
8. Knee deviation during stance phase – a varus or valgus deviation will indicate
either a malalignment or knee instability, requiring intervention.
9. Whip – medial or lateral. Is present when the foot has an altered course throughout
prosthetic swing phase. Indicates malalignment of knee axis and foot.
10. Terminal impact – occurs in a prosthetic knee joint when friction and extension
bias are not balanced. Requires knee adjustments.
11. Abducted gait – base is too wide. Could indicate prosthetic problems (e.g.,
discomfort in groin) or muscle imbalance.
12. Circumduction – the prosthesis tracks laterally in swing and is placed in the
correct heel strike position.
13. Vaulting – rising up on the toe of the intact eg to accommodate prosthetic swing.
Could indicate the prosthesis is too long.