Embed Size (px)
Citation preview

HEMOGLOBINOPTAHIES IN AFRICA
Léon Tshilolo, MD, PhDUNESCO HVP meeting
30-31 May 2016

WHO recommended the implementation of national SCA programs in Sub-Saharan Africa region with a focus on widespread awareness-raising, early identification, early access to adequate preventative care, and training of medical professionals.

Main focus of SCD

Geographical distribution and haplotypes
Coïncidence with malaria map
4 main focus(haplotypes)• Bénin• Sénégalais•Cameroun• Bantu (CAR)

Genetic diversity
A map of African language family distributions and hypothesized migration events within and out of Africa. (Campbell, Tishkoff 2009)

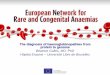
Prevalence of Hemoglobinopathies in Africa
0
5
10
15
20
25
30
35
40
Burkina Fas
o Benin
Nigeria
Guine
a
S Le
one M
ali
Ango
la
Con
go
D R
Con
go
Gab
on
Gha
na
Niger
C d'Iv
oire
Equ Guine
a
Libe
ria Togo
Gam
bia
G-B
issa
u
S T & Prin
cipe
Sene
gal
Uga
nda
Cam
eroo
n
Tanz
ania
Zambia
C Afr Rep
Mad
agas
car
Burund
i
Cha
d
Moz
ambiqu
e
Malaw
i
Rwan
da
Keny
a
Cap
e Ve
rde
Mau
ritius
Mau
retania
Zimba
bwe
Com
oros
May
otte
Reu
nion
Alge
ria
Seyc
helles
S Afric
a
Carriers, %
of the
pop
ulation
a0 thal
AE
Beta thal
AS
AC

Environmental and genetics factors• Tropical climate:
– malaria endemic, – High prevalence of HIV (4-15%)
• Socio economic conditions:– Poverty– independence since 50 years– Very rare Comprehensive SCA programs
• Homogenous population in DRC– Bantu haplotype: > 80%– Alpha-thal deletion: 10-50%– G6PD deficiency: 20-40%

EXPRESSION OF SCD in CENTRAL AFRICA

High morbidity and mortality
• Frequent VOC and high frequency of blood transfusion n (0.4U/yr)
• Severe complications

Early manifestationsHand Foot SyndromeAcute anaemiaSplenic SequestrationSepsis and pneumoniae (fever)

Septicemiae and meningitis•High mortality in very young children < 2 yrs•Str. Pneumoniae, Haemophilus Infl.

Respiratory infections: pneumoniae
Sreptocccus pneumoniae

Bone infectionsSalmonella sp : mainly in SCA patients
fistula

infections of international interestTuberculosis
• lung• bones
Malaria• Anemiae• CVO• Malnutrition• High risk Pregnancy• Mortality

Hepato-splenomegaly
• Large spleen• Persistent after 5yrs of age• Related to malaria?• Alpha –thalassemia
• Hepatomegaly• Viral infectious?• Iron hyperloading?

NTE manifestations
Nose bleeding
Hypertrophic tonsillitis Upper air obstruction
Dental abnomarlities

EARLY DIAGNOSIS

• Newborns and Children < 5yrs
• Samples : Dry blood and/or EDTA (Cord blood)
• IEF or HPLC: basic system (fisrt line method)
• Solubility test (Itano) in children > 1yr
• Capillary Electrophoresis (CE) : confirmation test
• Rapid diagnostic tests

Danielle Lena, PharmD
Hôpital d'enfants de la Timone, Marseille, France Monacord program
Dépistage et prise en charge des enfants atteints de syndrome drépanocytaire majeur dans les pays en développementScreening and management of children with sickle cell syndromes in developing countries
Kampala, UgandaMay 25-27, 2015

80’s Justification of newborn screening
Effective intervention in children with sickle cell disease provides a major impetus for neonatal screening
Prophylactic penicillin therapy has been found to significantly reduce the morbidity and mortality of patients with pneumococcal sepsis 1986
Antipneumococcal/haemophilus immunization
Antimalarial prophylaxis
Reliable, simple, and cost-effective techniques for mass screening of neonates are available.

Conditions of newborn screening
To be effective, neonatal screening must be part of a comprehensive program for the care of sickle cell patients and their families, including:
- a network of providers who ensure optimal medical care
- psychosocial support and genetic counseling.
Such follow-up capabilities should be in place before or coincidentally with screening implementation

Benin
1993: Pioneer programs in Africa
Ghana

2007: Pilot study Léna et al.
5 Countries - Morocco - Tunisia - Senegal - Mali - R Congo
Feasability
Enrolment in a follow-upProgram
5,000 samples

Results Léna et al. 2007
SS
SS

Results Léna et al. 2007
SS
SS
SS + SCSbThalSS + SbThal

Results Léna et al. 2007
SS
SS
SS + SCSbThalSS + SbThal
SOArab

Results Léna et al. 2007
SS
SS
SS + SCSbThalSS + SbThal
SOArab
Only 50% of the affected could be retrieved and enrolled in a follow-up program

30 questionnaires 19 answers
2016: What is the status today?

Most often 1 center or more 2-4 in capital cityPointe Noire
In some countries centersin different cities 2 in Angolato 11 in Nigeria
Newborn screening

.. .. . .. ... . .
Multiple centers
Angola 2Benin 1 + 2Mali 1 + 2Nigeria 8DRC: 4
Specialized centers
56% to 100% of the affected children have been enrolled in a follow-up program

Preventive measures
Peni VFolic ac.Immunization PneumoOpioids
TCD
93%100%100%80%
80%

Conclusions of the survey
impressive increase in the number of screening programs and specialized centers
BUT
most are pilot projects
no universal screening
difficulties in retrieving the affected children
Limited management of SCA patients

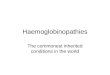
Exemple of Newborn screening in DRC
HET-EROZY-
GOTE AS; 16.8% HO-
MOZY-GOTE S;
1,7%
NORMAL A; 81,5% 81,5% AA, 16,8% AS, and 1.7% SS. No βSthal have been found but only few Bart’s Hb suggesting the co-existence of α-thal deletion

Clinical manifestations in Sickle cell trait patients: interest for genetic studies
• Splenic infarction at high altitudes
• Essential hematuria
• Loss of renal concentration ability
• Sudden death after extreme exertion
• Thromboembolism disease

Impact of genetic and environmentfactors
• Genetic factors determining clinical and laboratory heterogeneity in Sickle Cell Disease.
• The focus will be on clinical-laboratory outcomes (anaemia, haemolysis, foetal haemoglobin, infections, and neurological events)
• Pharmacogenomic response to treatment (hydroxyurea and antibiotics).

What we need
SCD
Healthcare
Training
Advocacy
Research

Genomic Research
Health benefits
GenotypingLaboratory capacity
Phenotyping Haemolysis, HbF, infections,
inflammation, Stroke
Statistical and Epidemiological Analysis
Bioinformatics Clinical Studies

The need of a Regional Collaboration and North-South parternership
Thank you/ Merci
Dank U/Aksanti