Embed Size (px)
Citation preview

Presented By : Aamina Naseer
Seminar 30 Oct 2015

Boron Neutron Capture Therapy of cancer

Uses of Boron
Borosilicate glass
Detergents
Make alloys
nuclear rods for controlling the fast moving neutrons
Cancer Treatment
Development of BNCT
Therapie
s
Surgical Resection,
chemotherapy and
immunotherapy
BNCTDevelo
p molecular
strategies
Brief History of Boron Neutron Capture Therapy
The first study of charged particles from slow neutron irradiation of boron was completed at Cambridge University in December 1934
USA used irradiated Boron for cancer treatment 10B + 1n → 7Li + 4He In 1938, first radiobiological study was carried out by using neutron-10B
reaction at the University of Illinois. In 1960, Hatanaka in Japan confirmed that BNCT has advantages for patient’s
treatment of certain cancers by comparing between BNCT and conventional chemo-immuno –radiotherapy
History of BNCT
In 1980, a clinical trial was started which concentrated on glioblastoma multiforme
In 2001, an experiment using BNCT irradiated an explanted liver suffering from diffuse metastases took place in Italy
In 2003, BNCT used to treat skin melanoma (Nievaart 2007).
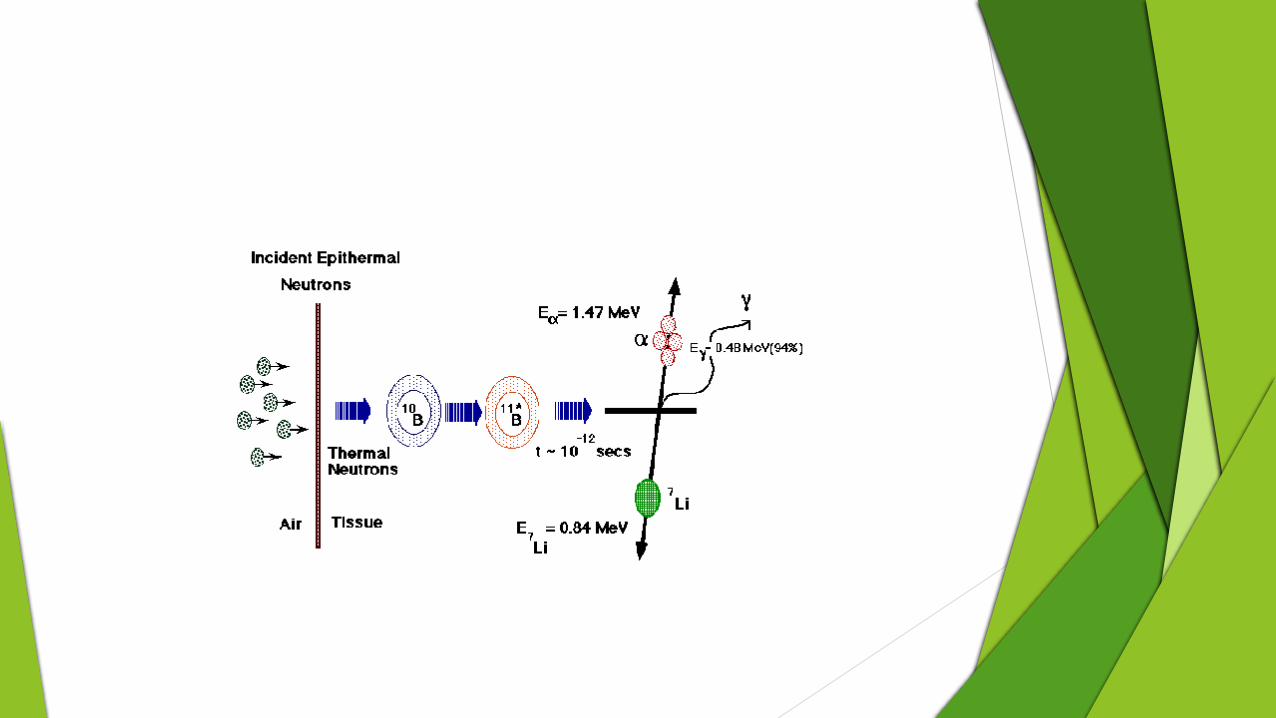
Basic Principle
Boron is injected to the patient. The uptake of Boron to tumor 20 g of B/g of tumor cell
Irradiation of boron through neutron Non-radioactive B-10 converted in to radioactive B-11 B-11 form Li and He (High LET particles) He and Le, particle range within the tumor cells are 9µm and 4µm (diameter
of tumor cells ) respectively (Coderre et al., 2004)
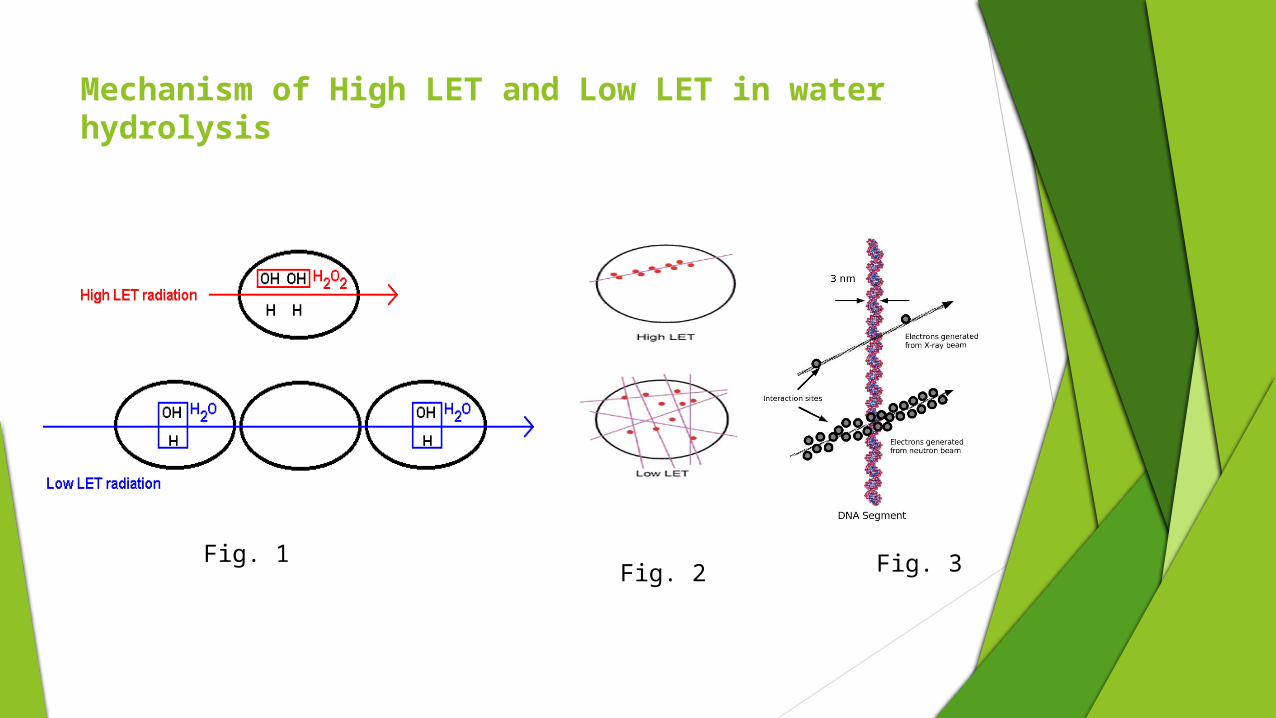
Mechanism of High LET and Low LET in water hydrolysis
Fig. 1Fig. 2 Fig. 3
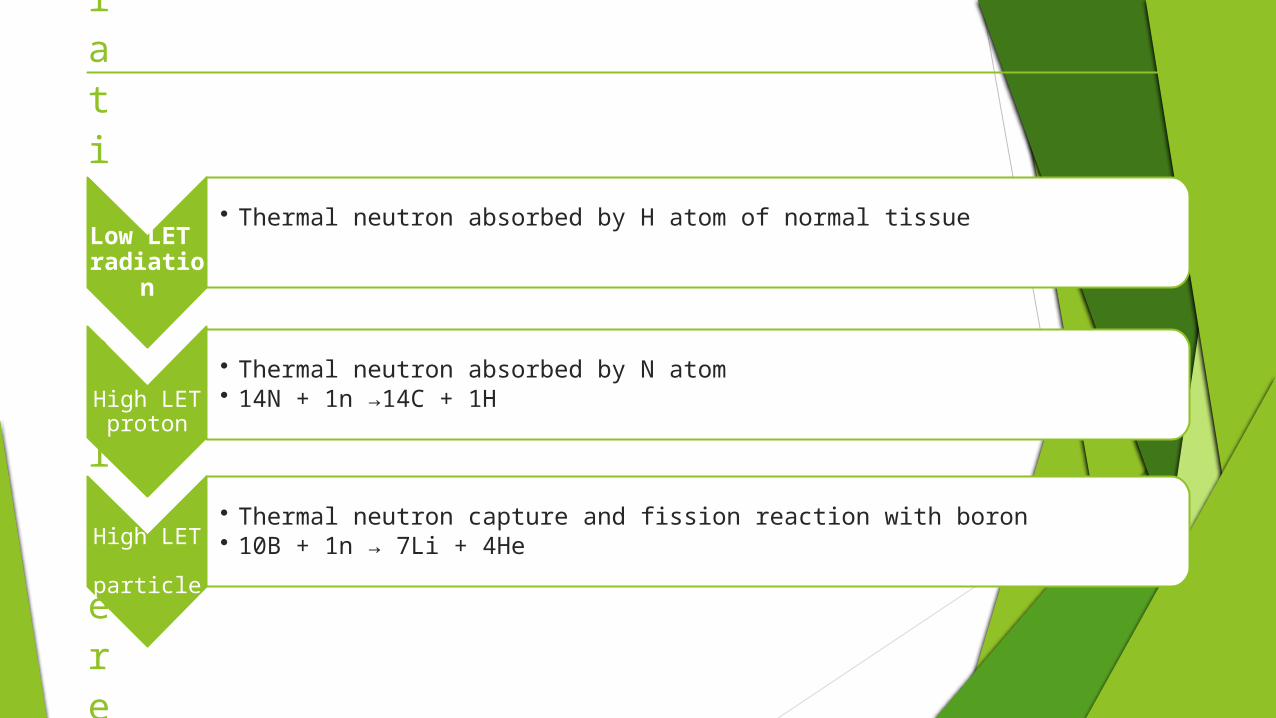
Types of Radiation Delivered
Low LET radiation
• Thermal neutron absorbed by H atom of normal tissue
High LET proton
• Thermal neutron absorbed by N atom• 14N + 1n →14C + 1H
High LET particle
• Thermal neutron capture and fission reaction with boron• 10B + 1n → 7Li + 4He
Requirements for a successful boron delivery agent
low systemic toxicity and normal tissue uptake with high tumor uptake and concomitantly high tumor/brain and tumor/ blood concentration ratios
B-10 concentration 20g /g tumor Rapid clearance from blood and normal tissues Retain ability of boron in tumor than normal cells (Barth et al., 2009)

Boron delivery agent
Optimizing Delivery of Boron-Containing Agents
Delivery of boron agents to brain tumors is dependent on the plasma concentration profile of the drug, which depends on the amount
and route of administration the ability of the agent to cross the Blood brain barrier (Lipophilicity) blood flow within the tumor (Barth et al., 2005)
Neutron Source for Boron Neutron Capture Therapy
Nuclear reactor Reactor produced different energy neutron
a) Thermal Neutron E 0.5ev
b) Epithermal Neutron E 1kev
c) Fast Neutron E 1Kev
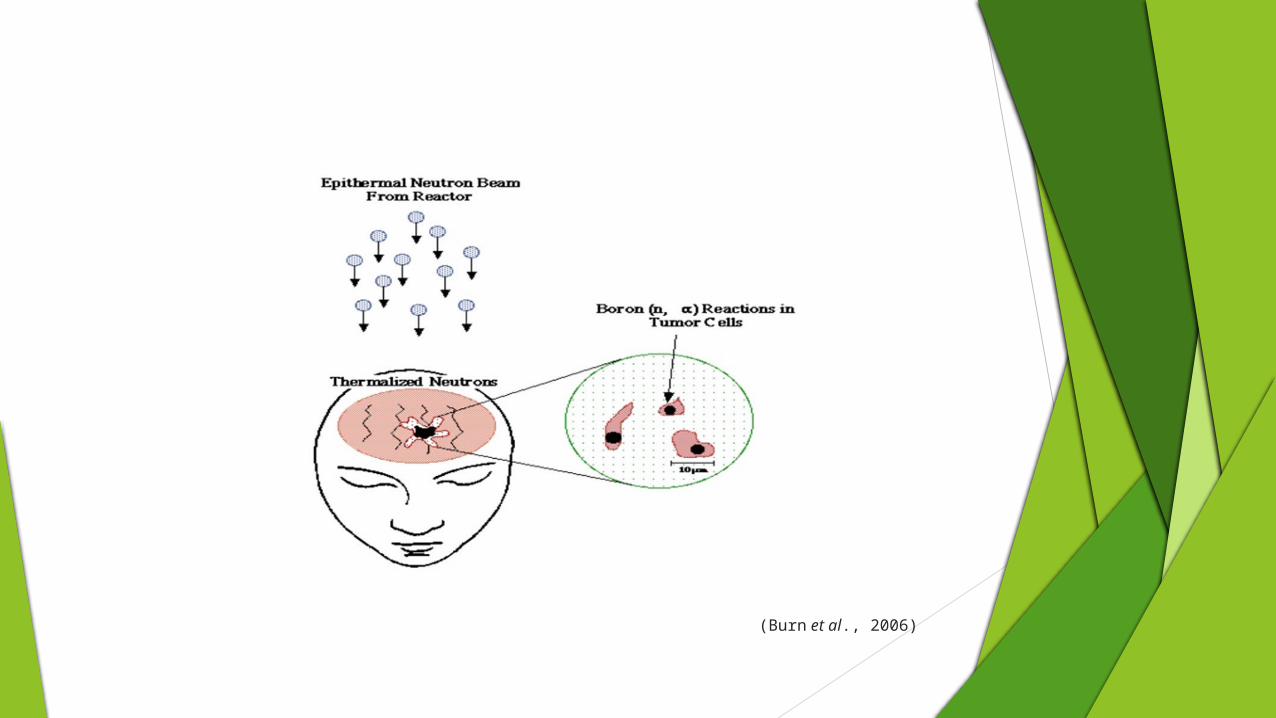
(Burn et al., 2006)
BNCT uses
Liver cancer• Hepatic tissue morphology preserved from radiotherapy• Require heavy operation(auto-transplantation), difficulty of determine
procedure length, fast system for infusion of blood, well trained surgeonBrain Tumor (Gliomas, Glioblastoma) and Skin cancer (melanomas)
• In Japan BNCT treatment equipment present (50% patient survive)
Lung disease
• Lung tissue are radio-sensitive so conventional therapies are not effective for its treatment (Barth et al.,
2005).
Advantages and Disadvantages
Clinical interest in BNCT has focused primarily on the treatment of high-grade gliomas and melanoma, most recently, head and neck and liver cancer
There are no boron compounds which have a sufficiently high tumor to healthy tissue ratio, to ensure that healthy tissues will not be affected by BNCT treatment
Undesirable dose components produced as an unavoidable side-effect (like gamma rays)
Well trained surgeon (Barth et al., 2009)
Cost Analysis
Factors which effect the cost Cost of nuclear source Construction of building Cost of equipment(dosimetry system and CT scan) Institutional maintenance Personal cost (depends on number of staff hired)
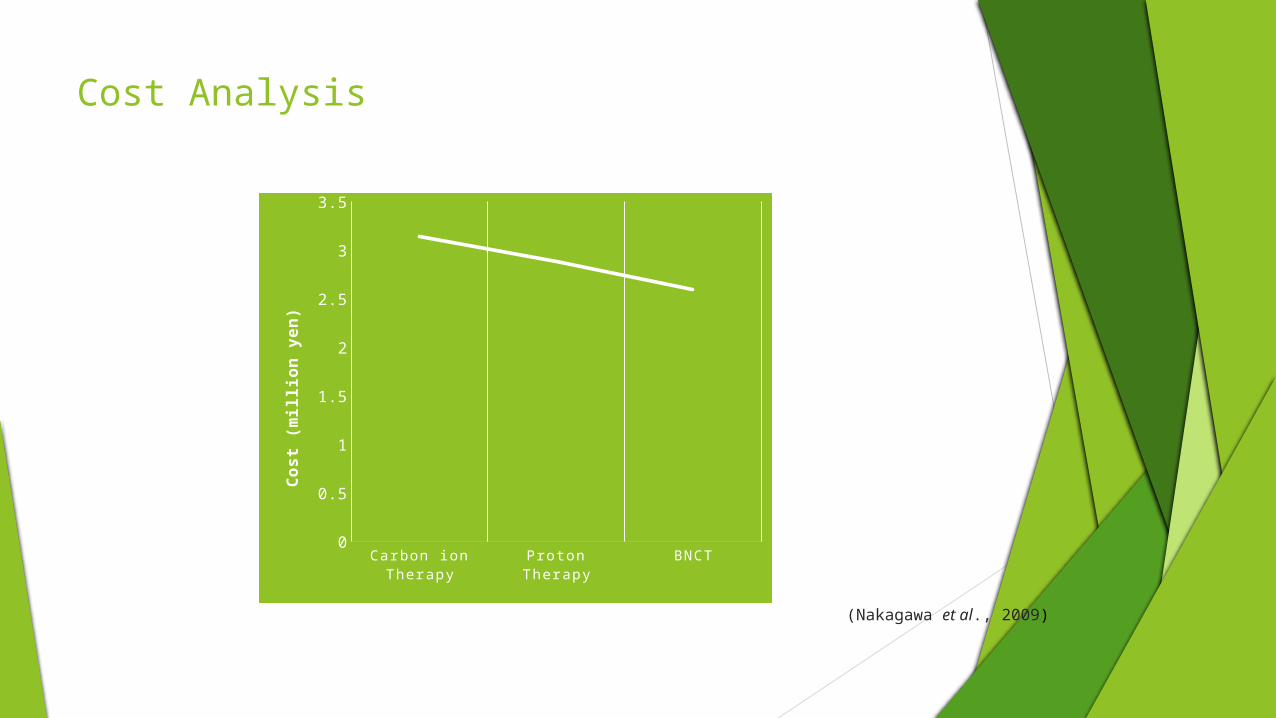
Cost Analysis
Ca rbo n io n T he ra py
Pro to n T he ra py
B NCT0
0.5
1
1.5
2
2.5
3
3.5
Cost
(m
illio
n ye
n)
(Nakagawa et al., 2009)
Critical Issues which require improvement
Require more selective and effective boron delivery agents Radiation dosimetry depends on uptake of boron concentration. Measurement
of accurate, real time dosimetry to better estimate the radiation doses delivered to the tumor and normal tissues
Need for randomized clinical trial
Conclusion
BNCT represents an extraordinary joining together of nuclear technology, chemistry, biology, and medicine to treat cancer.
The lack of progress in developing more effective treatments for high-grade gliomas has been part of the driving force that continues to propel research in this field.
BNCT may be best suited in combination with other modalities, including surgery, chemotherapy, and external beam radiation therapy, which, when used together, may result in an improvement in patient survival.
References
Bakeine, J. G., M. D. Salvo, S. Bortolussi, S. Stella, P. Bruschi, A. Bertolotti, R. Nano, A. Clerici, C. Ferrari, C. zonta, A. Marchetti and S. Altieri. 2009. Feasibility study on the ultilization of boron neutron capture therapy (BNCT) in a rat model of diffuse lung metastases. Applied radiation and isotopes, 67: 332-335.
Barth, F. R., A. Jeffrey, M. Coderre, H. Graa. Vicente, and B. E. Thomas. 2005. Boron Neutron Capture Therapy of Cancer: Current Status and Future Prospects. A review. Clinical Cancer Research, 11:3987-4002.
Burn, K. W., L. Casalini, E. Nava and R. Tinti. 2006. The epithermal neutron beam for BNCT under construction at Taprio. Journal of Physics: Conference Series, 41: 187-194.
Coderre, J. A., J. M. Rivard, H. Patel and G. R. Zamenhof. 2004. Topics in Neutron Capture Therapy: Proceedings of the11thWorld Congress on Neutron Capture Therapy. Applied Radiation Isotopes, 61.
Hentschel, S. J and F. F. Lang. 2005. Current surgical management of glioblastoma. In: Market J, Devita V T, Rosenberg SA, Hellman S, editors. Glioblastoma multiforme.1sted. Sudbury: Jones and Bartlett Publishers, 108-30.
Nakagawa, Y., H. Yoshihara, T. Kageji and R. Matsuoka. 2009. Cost analysis of radiotherapy, carbon ion therapy, proton therapy and BNCT. Applied radiation and isotopes, 67: 80-83.
Nievaart, V.A. 2007. Spectral Tailoring for Boron Neutron Capture Therapy. IOS Press, ISBN 978-1-58603-762-8.
Parney, I. F and M. S. Chang. 2005. Current chemotherapy for glioblastoma. In: Market J, Devita V T, Rosenberg S A, Hellman S, editors. Glioblastoma multiforme. 1st ed. Sudbury: Jones and Bartlett Publishers, 161-77.
Parney, I. F., C. Hao and K. Petruk. 2000. Glioma immunology and immunotherapy. Neurosurgery, 46:778-92.
Turiqi, A. A. 2009. Neutron activation boron therapy for cancer treatments. University of Surrey Thesis.
Zonta, T., U. Pinelli, L. Prati, C. Roveda, M. A. Ferrari, C. Clerici, G. Zonta, P. Mazzini, S. Dionigi, S. Altieri, P. Bortolussi, F. Bruschi and Fossati. 2009. Extra-corporeal liver BNCT for the treatment diffuse metastases. Applied radaiation and isotopes, 67: 67-75.

THANK YOU










![Precision determination of absolute neutron ux › pdf › 1801.03086.pdf · uence to determine doses to patients, particularly boron neutron capture therapy treatments [2, 3, 4]](https://img.pdfslide.us/doc/110x75/5f04db827e708231d4100ed9/precision-determination-of-absolute-neutron-ux-a-pdf-a-180103086pdf-uence.jpg)