Embed Size (px)
Citation preview

Twenty Years of EVAR in the USThe Procedure that changed a Specialty
Michel Makaroun MD
Co-Director UPMC Heart and Vascular Institute
Professor and Chief, Division of Vascular Surgery
University of Pittsburgh School of Medicine

Consultant in AAA field: WLGore, Medtronic, Cordis
Grant/research support in AAA field from Cook, WLGore, Cordis, Medtronic, Bolton, Trivascular, Lombard
Faculty Disclosure
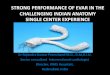
The Transformation of Vascular Surgery:Published Articles with “Endovascular” in Title
0
200
400
600
800
1000
1200
1400
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 281985 1990 1995 2000 2005 2010

Nov 23,1992 First EVAR in North America
Montefiore Hospital, Bronx, New York
Juan Parodi, Michael Marin, Frank Veith…

Juan Carlos Parodi MDBuenos Aires, Argentina
First EVAR in a human Sept 7, 1990
Reported the first 5 cases in 1991 in the
Annals of Vascular Surgery 5:491-499

The First EVAR Devices

Nicholas Volodos (Kiev, Ukraine) performed a similar
procedure for a thoracic traumatic aneurysm in 1987.
Reported in Russian only in 1988
Harrison Lazarus filed for a patent on an “Intraluminal graft
device, system and method” in December 1986
Granted US Patent number 4,787,899 on Nov 29,1988
Endovascular Technologies Inc.
The first study of a commercial device
Alexander Balko 1986
Animal work on Sheep
Precursor of the Talent Device
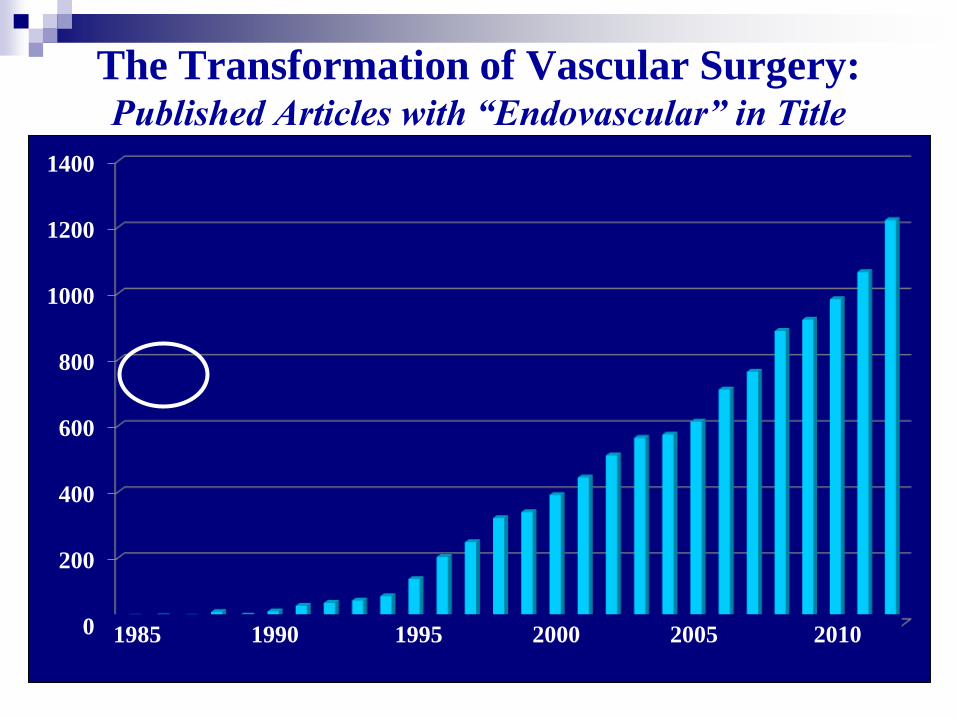
Michael Dake started working on Thoracic endografts
in 1992 and reported on 13 patients in 1994
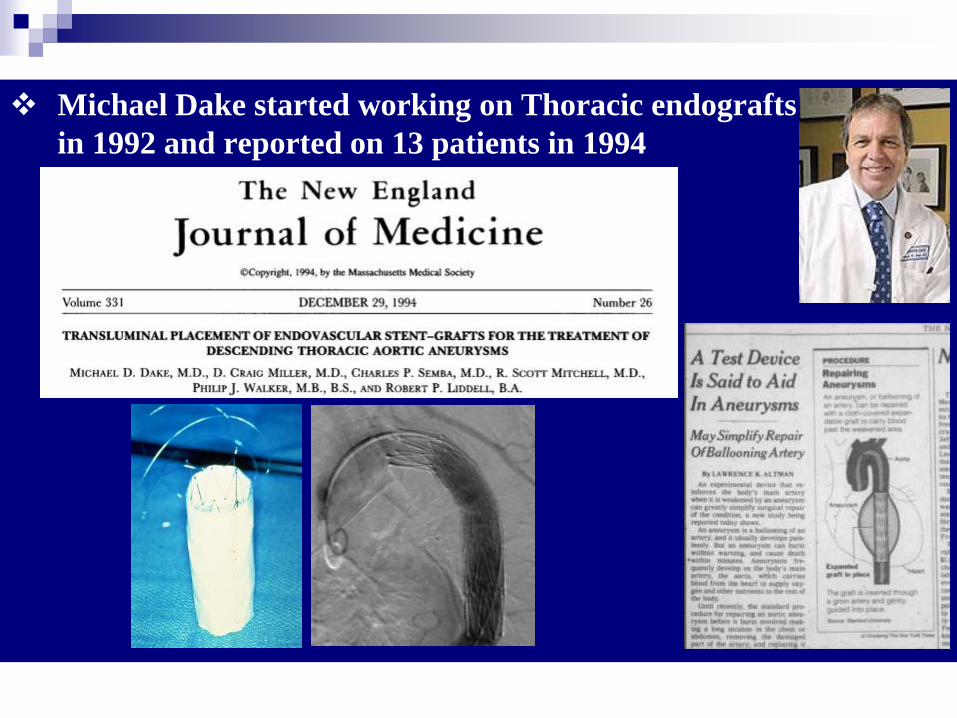
In 1993 Timothy Chuter (as a fellow) started
promoting bifurcated grafts as a more viable solution
Lancet 1994;343:413

J Vasc Surg 1994;20:855-60
….But what if these devices do work ..?…. My present best guess is
that 35% to 70% of current vascular prosthetic grafts could be
replaced by TPEGs. That potential and the fact that insertion of
these devices requires catheter-guidewire-imaging skills, which we
generally do not have, in addition to our vascular surgical skills,
explains why vascular surgeons are so interested in and yet agitated
by TPEGs. These devices could make vascular surgeons as we
currently know them largely obsolete…

4 Randomized Clinical Trials
EVAR trial in the UK
DREAM trial in Holland
OVER trial:VA Cooperative Study
ACE trial in France
Early Results of EVAR
Are Superior to Open Repair
Several
Industry
Regulatory
Trials

EVAR: Many Early Advantages
Local or Regional Anesthesia
Lower Morbidity and Mortality
Lower Blood Loss
Shorter Hospital and ICU Stays
Feasible in Higher-Risk patients
Patient Comfort

EVAR for AAA
first approved in 1999
86 year old
Significant CAD
Large 6 cm AAA
16 hours post procedure
The Far Reaching Impact of EVAR
Forced Retraining of the Vascular Workforce
Blurred Traditional Specialty Relationships
Changed our Operating Rooms and our Practice
Doubled the length of our Training Requirements
Promoted the Special Identity of Vascular Surgery
Prompted the Formation of a Vascular Surgery Board
Primary Specialty: Integrated Vascular Residencies
Increased the demand for Vascular Surgeons
Increased Compensation for our Specialty

J Vasc Surg 1999;29:177-86

70%

31%

34%
Steppacher R et al. J Vasc Surg 2009;49:1379-86
Vogel TR et al. J Vasc Surg 2009;49:1166-71
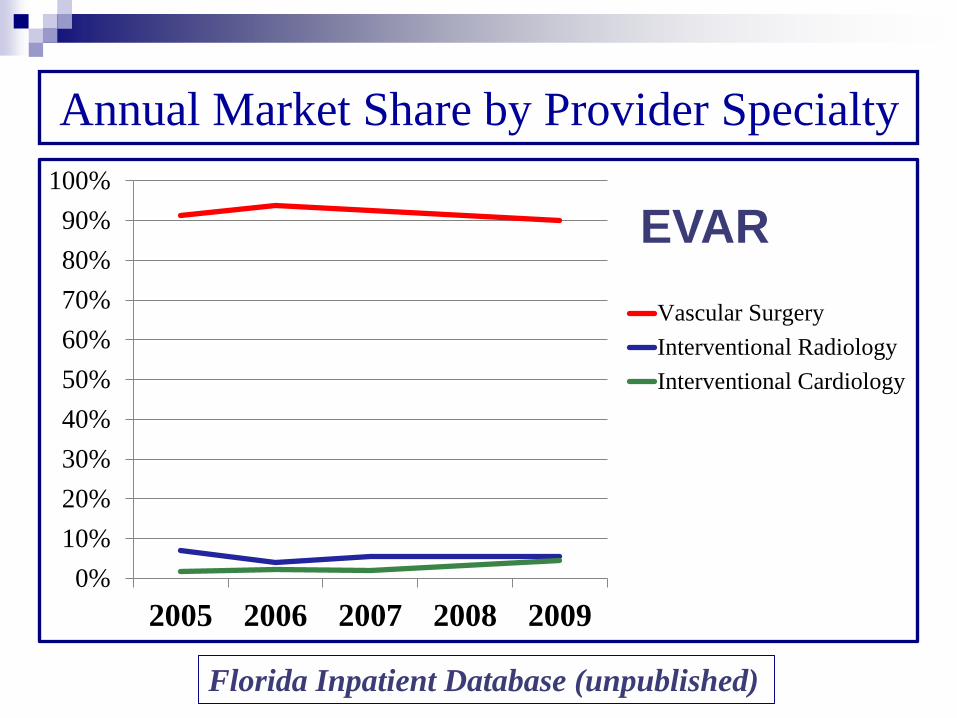
Annual Market Share by Provider Specialty
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009
Vascular Surgery
Interventional Radiology
Interventional Cardiology
EVAR
Florida Inpatient Database (unpublished)

-10%
0%
10%
20%
30%
40%
50%
60%
2005 2006 2007 2008 2009
Pro
po
rtio
n
Year
Vascular Surgery
Interventional Radiology
Interventional Cardiology
Annual Market Share by Provider Specialty
LE Int.
Florida Inpatient Database (unpublished)

0%
10%
20%
30%
40%
50%
60%
70%
2005 2006 2007 2008 2009
Vascular Surgery
Interventional Radiology
Interventional Cardiology
Annual Market Share by Provider Specialty
CAS
Florida Inpatient Database (unpublished)

The Far Reaching Impact of EVAR
Blurred traditional Specialty Relationships
Forced Retraining of the Vascular Workforce
Changed our Operating Rooms and our Practice
Doubled the length of our Training Requirements
Promoted the Special Identity of Vascular Surgery
Prompted the Formation of a Vascular Surgery Board
Primary Specialty: Integrated Vascular Residencies
Increased the demand for Vascular Surgeons
Increased Compensation for our Specialty


The Far Reaching Impact of EVAR
Blurred traditional Specialty Relationships
Forced Retraining of the Vascular Workforce
Changed our Operating Rooms and our Practice
Doubled the length of our Training Requirements
Promoted the Special Identity of Vascular Surgery
Prompted the Formation of a Vascular Surgery Board
Primary Specialty: Integrated Vascular Residencies
Increased the demand for Vascular Surgeons
Increased Compensation for our Specialty

J Vasc Surg 2009;49:1339-44

2008 2009 2010
Endovascular Diagnostic131 132 124
Endovascular Therapeutic355 440 307
EVARs and TEVARs 55 83 73
UPMC Average Caseload per Graduating Fellow 2008-2010
Endovascular Cases

The Far Reaching Impact of EVAR
Blurred traditional Specialty Relationships
Forced Retraining of the Vascular Workforce
Changed our Operating Rooms and our Practice
Doubled the length of our Training Requirements
Promoted the Special Identity of Vascular Surgery
Prompted the Formation of a Vascular Surgery Board
Primary Specialty: Integrated Vascular Residencies
Increased the demand for Vascular Surgeons
Increased Compensation for our Specialty

J Vasc Surg 1998;27:195-202

The Far Reaching Impact of EVAR
Blurred traditional Specialty Relationships
Forced Retraining of the Vascular Workforce
Changed our Operating Rooms and our Practice
Doubled the length of our Training Requirements
Promoted the Special Identity of Vascular Surgery
Prompted the Formation of a Vascular Surgery Board
Primary Specialty: Integrated Vascular Residencies
Increased the demand for Vascular Surgeons
Increased Compensation for our Specialty

Semin Vasc Surg 19:165-67
The Integrated Vascular Training Program
Directly from Medical School
5 Years: 24 months Core Surgery
36 months Vascular Surgery

Integrated Vascular Positions in match / Year
0
10
20
30
40
50
1 2 3 4 5 6 7
2007 2008 2009 2010 2011 2012 2013

Integrated
Programs in
Vascular
Surgery:
April 2013
46 programs
50 positions
5 new
programs
approved in
February
2013 Match:
39 Programs participated
46 Positions offered

The Far Reaching Impact of EVAR
Blurred traditional Specialty Relationships
Forced Retraining of the Vascular Workforce
Changed our Operating Rooms and our Practice
Doubled the length of our Training Requirements
Promoted the Special Identity of Vascular Surgery
Prompted the Formation of a Vascular Surgery Board
Primary Specialty: Integrated Vascular Residencies
Increased the demand for Vascular Surgeons
Increased Compensation for our Specialty


Vascular Surgery has quickly become one of the most difficult
recruitment efforts among all specialties.
60% increase in recruitment efforts the last 5 years

The Far Reaching Impact of EVAR
Stimulated Investments in Endovascular Technology
Far Beyond AAA affecting ALL Vascular Procedures
Thoracic and Thoraco-Abdominal Aneurysms
Thoracic Dissections
Vascular Trauma and Thoracic Aortic Transection
Popliteal Aneurysms
Aorto-Iliac and Lower Extremity Revascularization
Mesenteric Revascularization
Carotid Stenting

Abdominal EVAR
devices
Peripheral devices Thoracic
devices
Single Branch Device

The Far Reaching Impact of EVAR
Stimulated Investments in Endovascular Technology
Far Beyond AAA to affect ALL Vascular Procedures
Thoracic and Thoraco-Abdominal Aneurysms
Thoracic Dissections
Vascular Trauma and Thoracic Aortic Transection
Popliteal Aneurysms
Aorto-Iliac and Lower Extremity Revascularization
Mesenteric Revascularization
Carotid Stenting

EVAR
Two Decades later
Good Results and Improving!

Br J Surg 2001;88:1281-1282

August 25 2004
Initial Report of the UK EVAR Trial
October 14, 2004
Initial Report of the Dutch DREAM Trial
June 12, 2009
Initial Report of the VA OVER Trial
Randomized Trials EVAR vs OSR
Unequivocal Proof : EVAR HAS SUPERIOR EARLY RESULTS

UK EVAR 1 Trial
Randomized comparison of EVAR vs Open Repair
GOOD RISK CANDIDATES Suitable for both
From 1999 to 2003
1082 patients
41 Hospitals
AAA > 5.5 cm
> 60 Years old
Greenhalgh et al. EVAR 1 Trial. Lancet 2004;364:843-48

UK EVAR 1 Trial
EVAR Open p
30 day Mortality 1.7% 4.7% 0.01
Secondary Procedures 9.8% 5.8% 0.02
Greenhalgh et al. EVAR 1 Trial. Lancet 2004;364:843-48
EVAR OPENPer ProtocolIn Hospital Mortality 1.6% 6.0%

OVER Trial
Randomized comparison of EVAR vs Open Repair
GOOD RISK CANDIDATES Suitable for both
From 2002 to 2007
881 patients
42 VA Hospitals in the US
AAA > 5.0 cm
Mean age : 70 Years old
JAMA 2009;302:1535-1542
EVAR Open p
30 day Mortality 0.2% 2.3% 0.006
2 Yr Mortality 7.0% 9.4% 0.19

OVER Trial
NEJM 2012;367:1988-97

EVAR Open p
Initial Costs $37,068 $42,970 .04
@ 2 Years $75,325 $80,344 .35
EVAR is a cost effective alternative to open repair in the
US VA Health Care System for at least the first two years
Eur J Vasc Endovasc Surg 2012;44:543-8

1. Enthusiastic Adoption
of EVAR in the US
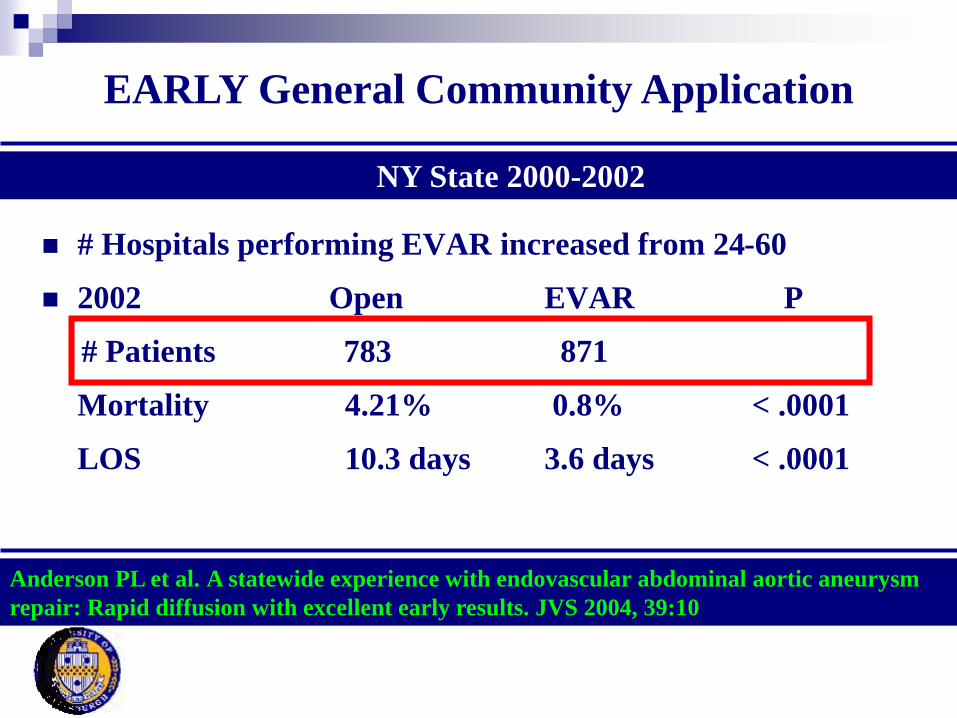
# Hospitals performing EVAR increased from 24-60
2002 Open EVAR P
# Patients 783 871
Mortality 4.21% 0.8% < .0001
LOS 10.3 days 3.6 days < .0001
NY State 2000-2002
Anderson PL et al. A statewide experience with endovascular abdominal aortic aneurysm
repair: Rapid diffusion with excellent early results. JVS 2004, 39:10
EARLY General Community Application

US Administrative Databases: Medicare
Dillavou et al. J Vasc Surg 2006;43:446-52
Dillavou et al. J Vasc Surg 2006;43:230-8 36.1%*41.4%*
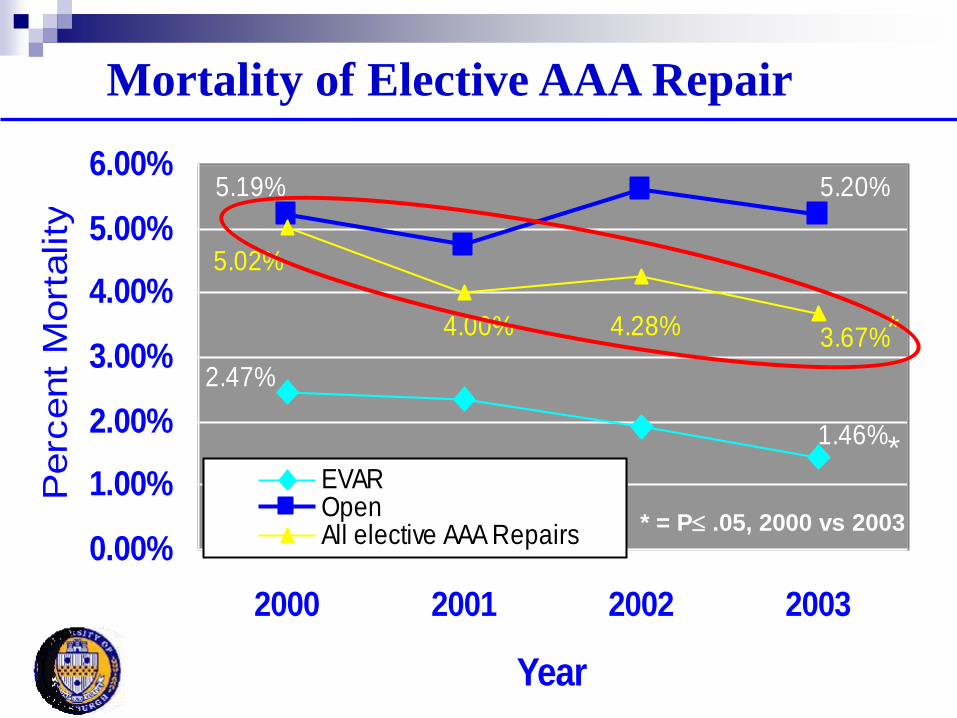
2.47%
1.46%
5.19% 5.20%
5.02%
4.00% 4.28% 3.67%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
2000 2001 2002 2003
Year
Perc
ent
Mort
ality
EVAROpenAll elective AAA Repairs
*
* = P .05, 2000 vs 2003
*
Mortality of Elective AAA Repair

2001 2002 2003
Open 79.2% 78.5% 75.4%*
EVAR 90.7% 92.2% 90.9%
Overall 82.8% 83.4% 81.7%
* = P .05 2001 vs 2003
Discharge to Home

J Vasc Surg 2009;50:722-9

J Vasc Surg 2009;50:722-9

50-64 y 65-74 y 75-84 y > 85 y
EVAR OAR EVAR OAR EVAR OAR EVAR OAR Hospital LOS, mean, d 2.5 7.3 2.9 8.2 3.2 9.5 3.5 9.9In-hospital mortality, % 0.3 1.2 0.8 2.5 1 5.6 1.5 9.5Discharge to home, % 98.1 94.9 96.1 88 92.3 71.5 85.6 50.2
complications, % 8.8 27.3 11 34.1 15.7 41 17.9 48.9
J Vasc Surg 2009;50:722-9
Mortality is reduced by EVAR in ALL AGE GROUPS

Strong Patient’s Preference for EVAR

J Vasc Surg 2009;49:576-81
Preference
EVAR Open Surgery Undecided
84% 13% 3%

Many Factors Impact the Decision To Use
EVAR in Hostile Anatomy
Individual patient
factors
impact the decision
to offer EVAR in
challenging
Anatomy
99
26
EVAR
79.2%
Open
Personal UPMC Experience 2002
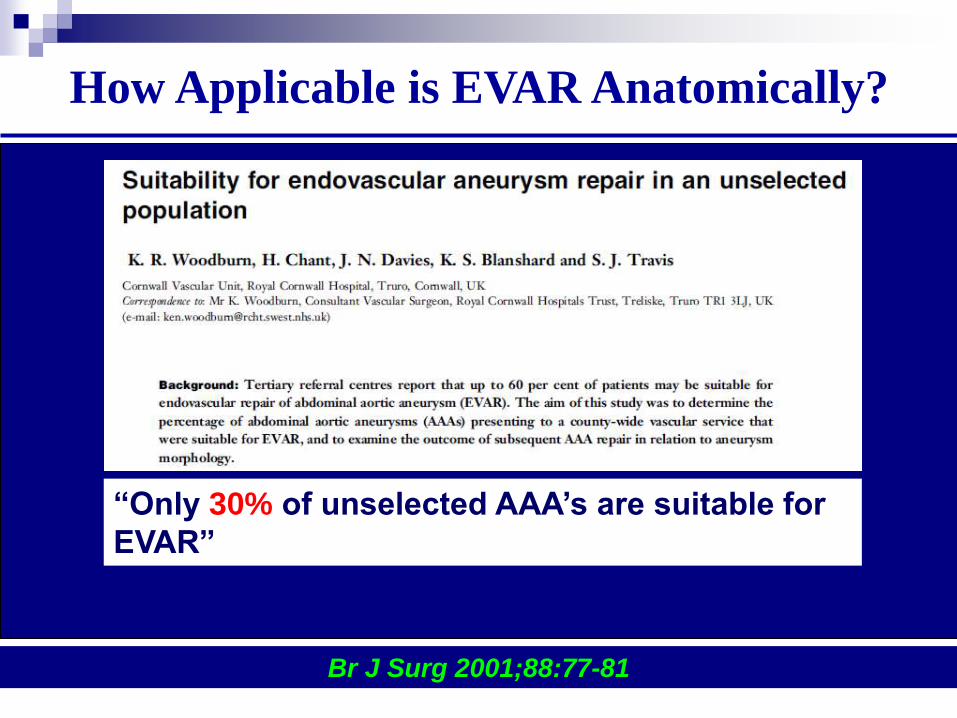
How Applicable is EVAR Anatomically?
Br J Surg 2001;88:77-81
“Only 30% of unselected AAA’s are suitable for
EVAR”

Moise MA et al. Vasc Endovasc Surg 2006;40:197-203
Anatomic challenges that cause Exclusion
1997-2000
2000-2003
Change over time

10228 patients (1999-2008)
59% <5.5 cm
41% had Sac enlargement @ 5 years
ONLY 42% of EVAR’s had anatomy that fit guidelines
Circulation 2011;123;2848-2855

2. Widespread application of EVAR resulted in
Many Operators being Less experienced !
Personal volume
2000-2004: 250 EVAR / year
2012-2013: 70 EVAR / year

Severe Oversizing !
32 mm
Zenith
1 month
later
Neck
Rupture
19 mm
Narrowing
Open Conversion
Cause of Complication: Severe Oversizing
Poor planning and Inexperience

Poor Planning: Multiple Complications
Bilateral Accessory
Renal Arteries
Small
Distal
Aorta
Coiled
Accesories
Covered
R Renal
Early Renal
Bifurcation

Multiple Complications
Rt Hepato-Renal
Bypass for renal
salvage

Recovery Room: Paraplegia and No femoral Pulses
Complete Thrombosis and Severe Ischemia
Multiple Complications
Narrow Distal Aorta

Multiple Complications
Ax Bifem Bypass
Wound breakdown
exposed Graft
6th Operation:
Conversion with Aorto-BiIliac bypass
and
removal of Ax-Bifem

3. Increasing Application of EVAR to
Rupture AAA

EVAR for Ruptured AAA
MP 87 yr old woman Hypotensive
Home in 4 days

J Vasc Surg 2008
6%7%
8%
11%
0%
2%
4%
6%
8%
10%
12%
2001 2002 2003 2004
NIS
Percent of
Ruptured
AAA Rx with
EVAR in NIS
40%43%45%
35%
41%
31%
43%
29%
0%
10%
20%
30%
40%
50%
60%
2001 2002 2003 2004
Open
EVAR
39%
21%
46%
55%
0%
10%
20%
30%
40%
50%
60%
Teaching Non Teaching
Open
EVAR

Ann Surg 2012;256:651-658
Medicare Results
2008 rates of EVAR
Intact AAA 77 %
Rupture AAA 31%
4. Revision of Surveillance Regimens
With more reliance on Ultrasound

EVAR has Possible Late Complications
Endoleaks
Migration
Material Fatigue
Endoleak
Life Long Surveillance
Migration

J Vasc Surg 2009;50:1538
29 Ruptures
After EVAR
22 (76%)
were lost to
Follow-Up
after the
initial EVAR

The issue of life long surveillance
and repeated CT scans
especially in young patients
is a significant consideration:
Radiation + Costs
There is plenty of evidence however
this can be simplified with the use of Duplex US

J Vasc Surg 2009;49:845-50

Can Duplex Ultrasound Completely Replace
CT in Certain Patients?
No Ruptures
No Graft Occlusions
No diagnosed Migrations
7 non aneurysm related deaths
1 Graft Infection and explantation Death
Results of New Policy in 2007 (187 Patients)
It IS SAFE to replace CT with a Duplex
Ultrasound after 1 yr if AAA is stable!

5. Decreasing Secondary Intervention Rate
Increased Experience
Improving Endograft Technology
Less interventions on Type II Endoleaks

Ann Surg 2009;250:383-389
11% of patients Undergo Reinterventions
Majority for endoleaks mostly Type II
76% of Reinterventions endovascular
>80% successful reinterventions except for type II
Low Mortality and Morbidity

486 Patients with 90 Type II Endoleaks (18.5%)
61% sealed spontaneously in 6 months
Only 6% experienced enlargement > 5mm
J Vasc Surg 2004;39:306-13

More Appreciation of Reinterventions for
Open Repair
Small bowel obstruction
Impotence and Retrograde Ejaculation
False aneurysms
Incisional Hernias
Graft Infection
Aortoduodenal fistulas
And Yes Endoleaks !!!

Open Repair Complications
Incisional
Hernias

Incisional Hernias after Open AAA Repair:
Quite common!
Author Year Incidence
Liapis 2004 16.2%
Raffetto 2003 28.2%
Papadirmitriou 2002 11.1%
Musella 2001 31.4%
Adye 1998 31%
Holland 1996 38.2%
Hall 1995 10.2%
Combined 21%
Takagi et al Eur J Vasc Endovasc Surg 2007 33;177-181

Anastomotic
or
New Aneurysms
Open Repair Complications

Aorto-duodenal Fistulas
Open Repair Complications

Open Repair Complications
Surgical Graft
Endoleak:
Reperfused aneurysm
Endoleak !!
After Open
Repair
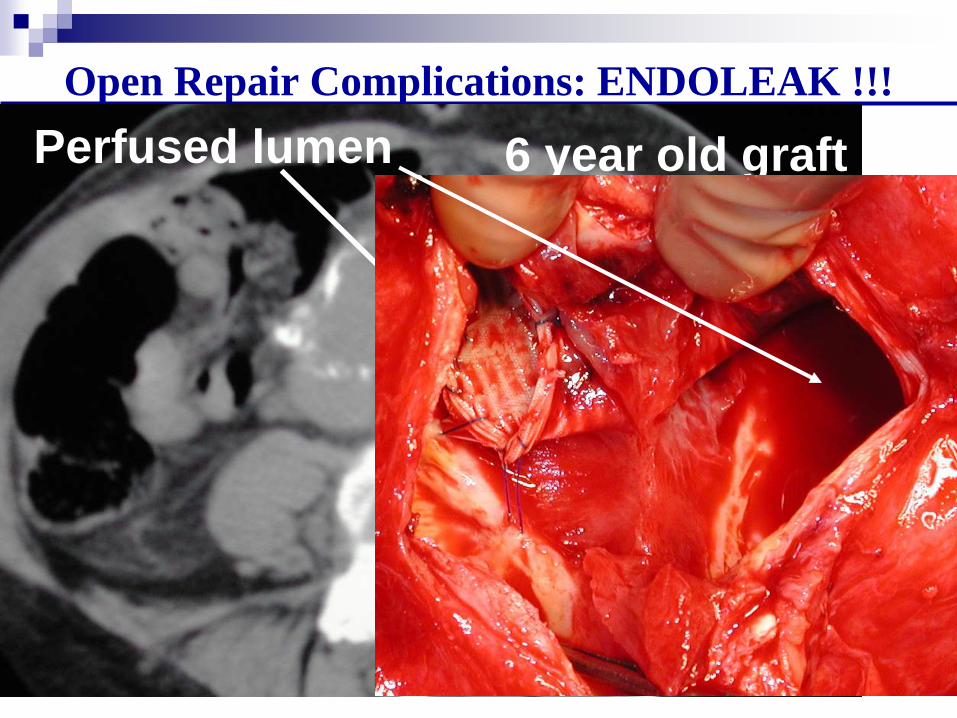
Open Repair Complications: ENDOLEAK !!!
Perfused lumen 6 year old graft

N Engl J Med 2008;358:464-74.
2830 matched patients in each group @ 4 Years
EVAR Open Surgery p
Reintervention 9.0% 1.7% <0.001
AAA related
Laparotomy related
Procedures 4.1% 9.7% <0.001
Hospitalization for
SBO or Inc Hernia 8.1% 14.2% <0.001

6. New Device Development
Focused on Tailoring Graft to Anatomy !

Available Commercial Choices in 2013Talent AneuRx Zenith Excluder Powerlink Endurant Ovation Aorfix
Zenith
FenestratedEndurant AUI

Devices in 2013 have
Expanded the Anatomic Limits of EVAR Decreasing device profile makes access a non issue:
13-14 Fr devices (Incraft** / Ovation….)
More Size offerings can now treat neck diameters of
16-32 mm (Ovation / Zenith / Excluder / Endurant…)
Improved Accurate deployment systems can now treat
shorter necks. (C3 Excluder / Endurant / Incraft**…)
Fenestrated Grafts can treat very short to non existent
necks ( Fenestrated Zenith / Ventana**…)
Innovative seals in diseased necks (Ovation…) or
endostaplers for better fixation (HeliFX..)
Very Flexible design to treat very angulated necks (Aorfix)
**Caution : Investigational Device / Limited by United States Law to Investigational Use

Biggest Effort: Reducing Profile
Talent AneuRx Zenith Excluder Powerlink Endurant Ovation Aorfix
2013 Ovation
Sheath 14 F OD1999 Ancure
Sheath 27 F OD

Lower Profile: Use smaller iliacs, Expand use in
Women, Decrease vascular complications
AFX Endologix Zenith LP** Ovation InCraft **
**Caution : Investigational Device / Limited by United States Law to Investigational Use
17 French 16 French 14-15 French 13-14 French

Excluder: Thinner constraining Sleeve
Reduced profile 2-4 Fr size
31 and 35 mm Main body down to 18 Fr Profile ID
16,18 and 20 mm contra leg down to 12 Fr ID
23 contra leg down to 14 Fr / 27 mm down to 15 FR ID
23-28.5 Aortic Extenders down to 16 Fr ID
32 mm Aortic Extender 17 Fr and 36 mm down to 18 Fr ID
Same Implant but ePTFE
sleeve made stronger,
denser and thinner to
constrain components at
smaller diameter
Future Design Target includes much lower profile
Released early 2013

Zenith LP: Nitinol Replaces Stainless Steel
Nitinol instead of Stainless
New suprarenal stent design
New capless constraint
New Stent configuration
Woven polyester fabric
New Dilator tip and Cannula
Mostly New Device Still in Trials in US
18-22 Fr ID 16 Fr ID
**Caution : Investigational Device / Limited by United States Law to Investigational Use

MC:82 y woman with AAA + severe iliac disease
6mm Balloons

14 Fr Device
MC:82 y woman with AAA + severe iliac disease
Increased Adoption of Percutaneous Approach:
Preclose Technique
Most Modern EVAR devices have a low enough profile
for percutaneous use!!
Personal Percutaneous Use since 2003 > 98%
New 14 Fr devices will encourage more users

Active Fixation: Reduce Migration
Endurant
**Caution : Investigational Device / Limited by United States Law to Investigational Use
Aorfix
Incraft**
Zenith ExcluderOvation
Aptus HeliFX

Flexible Construction: Accommodate Anatomy
Excluder Endurant Zenith-flex Aorfix
Most Flexible is the Aorfix: Both Iliacs and Necks
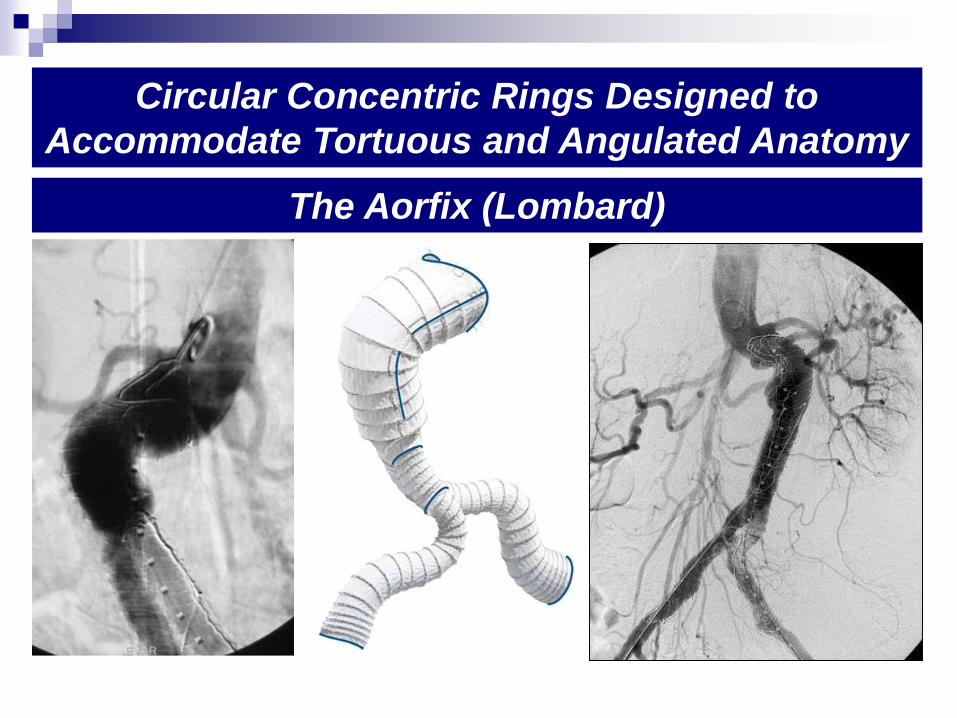
Circular Concentric Rings Designed to
Accommodate Tortuous and Angulated Anatomy
The Aorfix (Lombard)

Very Accurate and Controlled Deployment:
Improve Seal Zones + Use Shorter Necks
The Endurant (Medtronic)Based on delayed release of fixation until final position
IFU: Neck length > 10 mm

RO: Accurate Deployment in Very Short Neck
Adequate Seal and Good Comformability
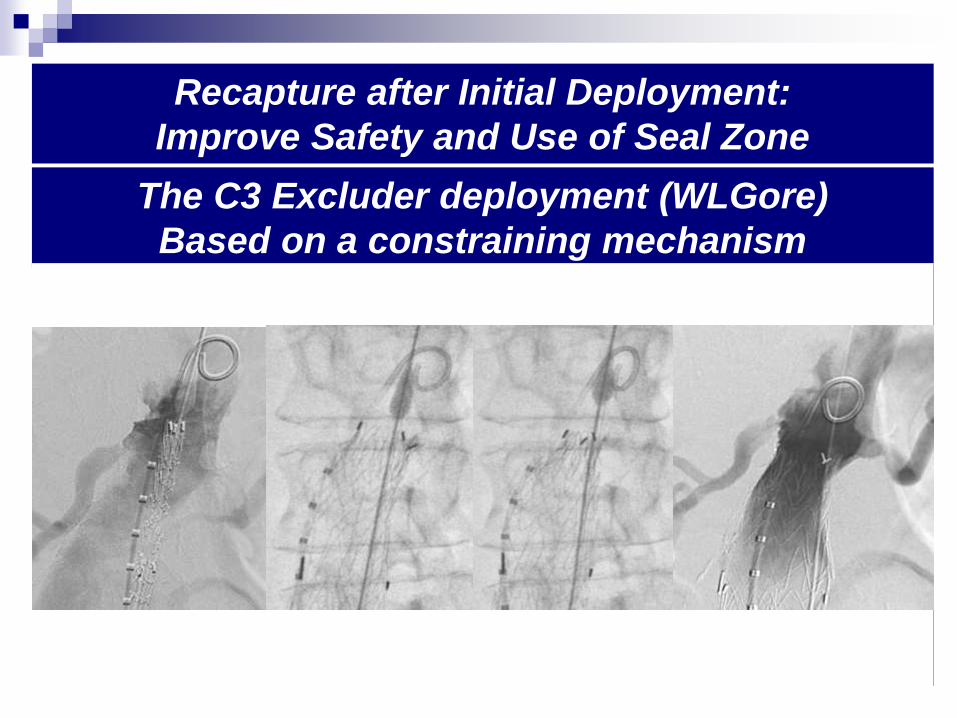
Recapture after Initial Deployment:
Improve Safety and Use of Seal Zone
The C3 Excluder deployment (WLGore)
Based on a constraining mechanism
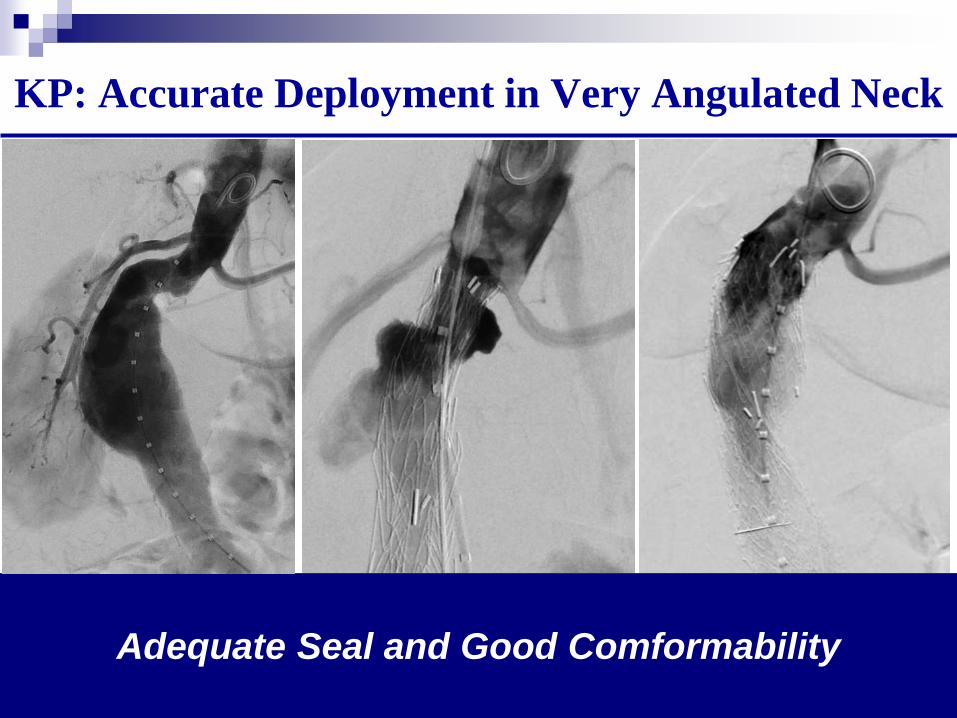
KP: Accurate Deployment in Very Angulated Neck
Adequate Seal and Good Comformability

Molds to irregularities in Sealing Zone
The Ovation Endograft (Trivascular)
Based on Biopolymer fill

TM: Reverse Taper Neck with Thrombus
Must Understand Behavior of particular Devices
Diam@ Renals: 22mm
13 mm lower: 31 mm

Allows Extension over Branches
The Zenith Fenestrated Graft
Custom Made

MV 85 year old F: Very Short Neck
Type II endoleak treated at 3 years / well at 6 years (92y)
1 month:51 x 55 mm
1 year : 38 x 46 mm

How to pick an Endograft
Clinical data
Familiarity and expertise
Ease of use
Stock and availability
Price
2013
Anatomy: Match Device to Anatomy

How to pick an Endograft
Workhorse Standard graft for most: Excluder
New devices have special characteristics to handle
difficult anatomy better
Short Necks 10-14 mm: New more accurate
deployment systems: C3 Excluder, Endurant..
Very Short Necks: Fenestrated Zenith graft
Non Cylindrical necks or small <17 mm: Ovation
Very poor Iliac access: ovation
Severe Neck angulation: Aorfix
Occluded Iliac or very complex iliac aneurysms: AUI
Narrow distal aorta: Endologix or AUI

Branched Grafts on the Horizon
Courtesy of R Greenberg
Branched TAAA Grafts
Courtesy of J Anderson
Branched Arch Grafts
Caution: Investigational device

Summary
EVAR has Excellent early results and good late
outcomes that continue to improve with new devices
that are also expanding its applicability
EVAR has largely replaced Open Repair in the US
in anatomically suitable candidates. This has been
associated with a decrease in total AAA mortality
EVAR had a profound effect on our specialty and
changed the face of Vascular Surgery as we knew it