Embed Size (px)
Citation preview

Sensitivity of duplex ultrasound in
evaluation of AV access with comparison to
digital substraction angiography
Department of Surgery, College of Medicine and Health Sciences, UAE University, Al- Ain, UAE.
Ali Jawas, Mohammed Murtuza, Trab Manar, Safi Basel, Fikri Abu-Zidan

Maintenance of AV access is essential for
patients on hemodialysis.
Monitoring of the access helps to detect stenosis
prior to complete occlusion.
Endovascular intervention for failing vascular
access could prolong the patency of the access.
Introduction
The gold standard to diagnose stenosis of AVF and
AVG is angiogram.

Duplex scan is non invasive, less expensive and
widely used for various vascular conditions.
Currently there are no well-defined
ultrasonographic criteria for evaluation of AVF
and AVG.
Many apply the duplex criteria of arterial
stenosis.
Introduction

To report on the Value and sensitivity of
duplex ultrasound for evaluation of AV
access with comparison to digital
substraction angiography
Objectives

• 121 patients were referred to our vascular laboratory
for evaluation of AV fistulas and AV grafts over 9
months (January 2013 to September 2013) .
Patients and methods
Tawam Hospital Al-Ain Hospital

• GE Logic 9 Duplex scanner with linear broadband
transducers of 12 MHz and 7 MHz for superficial and
deep vessels respectively.
Patients and methods

1. Reduced thrill or weak bruit on auscultation
2. Decrease dialysis flow rate. (KDOQI)
3. High venous pressure. (KDOQI)
4. Difficulty in access cannulation.
5. Excess post dialysis bleeding.
Criteria for referral for access duplex ultrasound

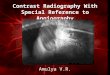
• Peak Systolic Velocity of >400 cm/sec.
• Peak Systolic Velocity Ratio >3.5 (between
the area of stenosis and pre-stenosis).
• Luminal narrowing on B mode image.
• Volume flow <400
Critical stenosis parameters and Endpoints

• Moderate stenosis Peak Systolic Velocity
Ratio (3.5-2), Volume flow (400-600)
• Mild stenosis Peak Systolic Velocity Ratio
<2, Volume flow (>600).
Stenosis parameters and Endpoints

• Anastomotic stenosis (at the anastomosis of
fistula or graft).
• Junctional stenosis (at the junction of
cephalic and subclavian veins).
• Venous outflow stenosis (stenosis in the
outflow vein or graft).
Location of Stenosis

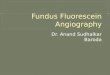
• Angiography was performed on all hemodynamically
significant stenosis diagnosed by Duplex scan.
• Percentage stenosis in angiogram was calculated by
measuring the stenotic vessel diameter in comparison
to pre- and post stenotic vessel.
• Angioplasty performed in the same setting if
significant lesion is confirmed on angiogram.
Angiography

Mean age (SD)
56.6 (17.3) years
Results
Male = 78 (64 %)
Female = 43 (36 %)

Type Number %
Normal 29 24%
Mild stenosis 12 9.9%
Moderate stenosis 19 15.7%
Severe stenosis 49 40.5%
Occlusion 12 9.9%
Total 121 100
Results

Normal Mild Moderate Severe
Kruskall Wallis test p < 0.0001

Normal Mild Moderate Severe
Kruskall Wallis test p < 0.0001

Normal Mild Moderate Severe
Kruskall Wallis test p < 0.0001

Site of stenosis Mild Moderate Severe Total
Anastomotic 12 (100%) 17 (89.5%) 40 (81.6 %) 69 (86.3%)
Junctional 0 (0%) 2 (10.5%) 7 (14.2%) 9 (11.3)
Venous outflow 0 (0%) 0 (0%) 2 (4%) 2 (2.5 %)
Total 12 (100%) 19 (100%) 49 80 (100 %)
Results
P = 0.64 , Fisher’s Exact test

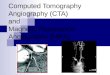
121 patients
Complete
occlusion
12
Mild-
moderate
Stenosis
31
Follow up
Severe
Stenosis
49
Angiography
Normal
29
46
44 (95.6 %)
Severe stenosis
Sensitivity
95.6 %



Pre-angioplasty

Post Angioplasty






• Ultrasound is a sensitive screening tool for
guiding decisions on interventions for vascular
accesses.
• Vascular laboratory and good vascular
technologist is an essential and important
service in the evaluation and management of
vascular access.
Conclusions

College of Medicine and Health Sciences,
UAE University