Embed Size (px)
DESCRIPTION
MD Buyline, the leader of healthcare supply chain management solutions, presented Transitioning to Digital Radiography at the AHRA 2014 Annual Meeting in Washington, DC. http://www.mdbuyline.com/research-library/articles/transitioning-to-digital-radiography-2/
Citation preview

Transitioning to Digital Radiography
Clinical, Financial and Operational Considerations

Presented By
Lori Webb, R.T. (R)Clinical Analyst, MD Buyline
Katie Regan, M.A.Clinical Publications Manager, MD Buyline
• Joined MD Buyline in 2008• 20 years experience in the clinical healthcare field • Practicing clinician at a local freestanding ER• Registered Radiology Technologist, American
Registry of Radiology Technologists
• Joined MD Buyline in 2012• Seven years of clinical and research experience • Responsible for clinical, financial and general
healthcare publishing projects at MD Buyline • Member of Healthcare Finance Management
Association

The Digital Age
• The medical imaging market is expected
to reach over $35 billion by 2019– The global digital radiology market is
forecasted to pass $13 billion by 2018
• Medical imaging moved away from
analog technology toward digital
solutions – Flat-panel detectors (FPDs) offer better image
quality, faster processing time and greater
dose reduction over analog predecessors
“Studies have shown that implementation of PACS, EHR and digital imaging shorten
turnaround times and increase medical imaging
department volume without a subsequent staffing increase.”
Health Care Industry Advisory Council 2013 (HCIAC)

The Shift from Analog to Digital• First implemented in cardiology
and mammography due to clinical improvements – Workflow efficiency– Image quality– Lower radiation dose potential
• General radiography units transitioned last due to the volume of equipment and presence of computed radiography (CR) systems– CR allowed images to be digitized– Acted as a bridge into the digital age
for general radiography
X-ray film used for imaging, must be developed
Imaging plate is used and digitized by optical scanner
Digital image acquired by direct or indirect flat panel detector (FPD)
Analog
Computed Radiography
Digital Radiography

Digital Cardiology• Conversion of cardiac imaging to digital flat-panel detectors (FPDs) was
driven by several considerable advantages – Faster patient turnaround time and higher productivity– Ability to record dynamic and static X-ray images at a high-image quality– Faster acquisition of images and greater flexibility with post processing of the
images– Better contrast and spatial resolution that allows greater visualization of small
guide wires, markers and stents– Lower radiation dose to patients and staff

Evolution of Digital Mammography• Full field digital mammography
(flat-panel detectors) offer– Lower radiation dose to patients– Greater image quality– Shorter exam times– Broader dynamic range– Digital CAD– Breast tomosynthesis
• Clinical improvement and its effect on public opinion have made the move necessary for providers to stay competitive
• Initial capital investment for digital mammography is substantial
• Most facilities are 100% digital(DR or CR mammography)
System Average Purchase Price
Service Contract
Analog $80,000 to $140,000 $7,000
Digital $210,000 to $450,000
$25,000 to $48,000

Digital Mammography
• Breast cancer prevention, detection and treatment is highly profiled – Compelling clinical results have left patients demanding and expecting digital
mammography • Digital Mammographic Imaging Screening Trial (DMIST) established benefits of
digital mammography over film-screen, particularly for women younger than age 50 with dense breasts
• FPD offers shorter exam times and the ability to increase throughput
• As hospitals compete for patients, volume is a key factor to the successof any service line
Clinical and Patient Drivers
System Patient Volume Exam Length
Analog 3 to 4 per hour 15 to 20 minutes per exam
Digital ~6 per hour 10 minutes per exam

Digital Mammography
Financial• Separate reimbursement levels
for mammography– Analog system exams: $81.66
(CPT 77057 bilateral screening)– Digital system exams: $138.81
(HCPCS G0202 screening)
Legal• The “digital divide” is when a
facility offers both digital and analog mammography– Creates patient, legal and
productivity issues
Financial and Legal Considerations

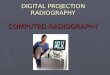
Evolution of Digital General Radiology
X-RAY 51.72%
NUCLEAR MEDICINE
4.28%
OTHER X-RAY 12.5%
ULTRASOUND14.26%
MR 4.99%
CT 12.02%PET 0.23%
Source: Frost & Sullivan, 2004, #A630-50, 1-7
• General radiology exams are the “bread and butter” of medical imaging– 74% of general radiologic exams, such as
X-ray and radiography/fluoroscopy (R/F)– The volume of R/F studies skyrocketed
from 25 million in 1950 to 293 million in 2006*
• The focus on converting general radiology to digital, FPD technology increased due to– The need to bring all equipment to digital
standards for communication with PACS and EMRs– The availability of budgetary dollars for technology upgrades– The need for a more efficient workflow, better image quality and lower radiation dose
*Source = American Society of Radiologic Technologists

Digital General Radiology Cost• Pricing associated with digital systems is complicated by the number of
possible system combinations and the “digital retrofit” upgrade path System Price Range
Fixed X-rays
Analog • $50,000 to $125,000 • Additional cost of $33,000 to $85,000 for a CR system
Retrofit • $100,000 to $150,000
Digital• $165,000 to $550,000 • Low-end price for a single-panel system • Higher price for a dual-detector system that is capable of advanced applications
Portable X-ray
Retrofit • $100,000 to $130,000
Digital • $150,000 to $200,000
R/F
Image Intensifier • $325,000 to $425,000
Digital • $500,000 to $800,000

Digital Retrofit Costs
• A “digital retrofit” upgrade path allows facilities to use an existing analog fixed X-ray or a mobile system with an FPD
• Retrofitting an older unit is considerably less costly than investing in a new digital system
• Pricing for retrofit FPDs
Vendor Size of Detector Plates Cost of Detector Plates1 14” x 17” Cesium Iodide $80,000 - $100,0002 14” x 17” Cesium Iodide $92,000 - $106,000
3 • 14” x 17” Gadolinium• 14” x 17” Cesium Iodide
• $65,000 - $94,000• $87,000 - $104,000
4 14” x 17” Cesium Iodide $76,000 - $87,000
X-ray and R/F

Digital RetrofitBridging the Gap Between Analog and Digital
2012 2013 2014 2015 2016 20170%
5%
10%
15%
20%
25%
IHS Forecast: Global Market for General Radiography X-ray Equipment
Mobile Retrofit Other GR X-ray Equipment
(Revenue Growth Profile)

R/F: Image Intensifier vs. FPD
• Price point advantage• Technology is still considered
viable• Better spatial resolution
Dynamic FPD: Pros• Smaller size• Easier to position• Sleek system appearance• Less geometric distortion and
glare• Less degradation of image quality
from flare or veiling
Image Intensifier: Pros

R/F: Image Intensifier vs. FPD
• Larger size• Harder to maneuver/position
for exams• Limitations in dynamic range• More glare and geometric
distortion
Dynamic FPD: Cons• Higher cost• Less spatial resolution
Image Intensifier: Cons

Evolution of Digital Mobile C-arms• Cost of mobile c-arms
• Digital, FPD mobile c-arms offer improved clinical performance and workflow over image intensifier systems – Improved image quality– Reduced dose– Extended dynamic range– Reduced distortion and image clarity for anatomical areas of interest
System Capital Price Range Service Contract Price Range
Image Intensifier-based Mobile C-arm $165,000 to $226,000 $8,400 to $10,200
Digital, FPD-based Mobile C-arm $260,000 to $399,000 $13,500 to $15,580

X-ray System Configurations and Pricing
• High-volume exam setting ($225,000 to $600,000)– Triple-Detector
• Uncommon• Pricey • Highly efficient• Has a fixed-wall FPD, fixed-table
FPD and wireless, portable FPD– Dual-Detector
• Involves a fixed-wall FPD and separate portable, wireless FPDs
A dual-detector in the form of two portable, wireless detectors

X-ray System Configurations and Pricing
• Medium to low volume ($150,000 to $275,000)– Single-Detector
• A single wireless, portable FPD that can be moved from wall stand to table and can be used for table-top exams
• Very cost effective and the most common configuration
A single-detector configuration or analog that can be retrofitted

X-ray System Configurations and Pricing
• Retrofit upgrade ($106,000 to $140,000)– One or two wireless FPDs are retrofitted using
an existing X-ray tube, wall stand and table– Retrofit panels can be mixed to some degree
with other vendors’ X-ray systems
• Small FPD panels ($62,000 to $85,000)– Used to retrofit analog systems or with new
fixed/portable X-ray system– Used in NICUs, pediatric wards, children’s
hospitals and for orthopedic exams– Appropriate for imaging smaller anatomy
Previous generation analog portable retrofitted with an FPD

Sole Sourcing vs. Mixing Vendors
Sole Source: Pros• Bundle systems together for
optimal pricing on purchase and service/support
• User interfaces/operating systems are uniform across modalities, decreasing learning curve
• Panel sharing
Mixed Vendors: Pros• Ability to customize and tailor
solution for workflow• Greater negotiation power

Sole Sourcing vs. Mixing Vendors
Sole Source: Cons• Vendor complacency• Loss of negotiation leverage• Risk of missing new or innovate
technology or features• Chosen vendor may not have the
top product in every category• Panel sharing
Mixed Vendors: Cons• Issues related to learning and
operating multiple vendor’s user interfaces is decreasing
• Loss of leverage in bundling support

Service Cost
• Increased cost of ownership when moving from analog to digital
• Facilities often elect for more full-service agreements due to– Complexity associated with supporting digital systems
– Lack of digitally-trained biomedical engineer (BME) staff
– “Software keys” required to diagnose and repair equipment
System Service Price Range
Analog $8,000 to $12,000
Digital $30,000 to $55,000

Service Cost• FPDs are moderately fragile and expensive• FPDs are portable and at a greater risk of being damaged• Many manufacturers offer or require separate service coverage for the
panel known as “drop-panel” coverage– Deductible per occurrence ($5,000)– Additional annual premium – Vendors may require sites that wave drop-panel coverage to sign a waiver
• Replacing the FPD will be market value ($80,000 to $125,000)

Service Recommendations• Suggestions for coverage hours
– Facilities with multiple systems: Monday through Friday from 8 a.m. to 5 p.m. – High-volume settings/dedicated ER X-ray rooms: Monday through Friday from
8 a.m. to 9 p.m. (extended coverage)
• When determining coverage amount– Consider the service history of existing systems in your facility– Assess how critical equipment is to your workflow and backup system
availability
• Service coverage for retrofitted systems– Typically service contracts are already in place for existing analog systems– Retrofit panel vendors should offer coverage and drop/damage protection

Service Recommendations• Types of coverage
– In-House or BME• Original Equipment Manufacturers (OEMs) offer biomedical training classes on
digital X-ray and R/F systems • Switching to an in-house service will depend on biomedical staff’s level of expertise• First-call agreement is a viable savings opportunity• Vendors do not always provide seamless access to proprietary “software keys”
– Third-Party Vendors• High-risk review on a case-by-case basis• Parts availability and replacement detectors can be difficult for third-party vendors
to obtain• Often unable to provide loaner panels as readily as OEMs

Clinical Considerations of “Going Digital”
• Clinical advantages of FPDs – Higher image quality– Less distortion– Potential for dose reduction– Greater anatomical coverage area– Immediate view of the image – Additional advantages for R/F systems
• Better penetration of anatomy • Additional room within the unit for
patient positioning and movement

Financial Considerations and Soft Dollar Benefits
• Financial considerations– “Going digital” requires a substantial investment by providers– Currently no separate reimbursement for digital and analog exams– Film and film processing costs are eliminated
• Measureable soft dollar benefits of switching to digital– Increased workflow efficiencies and time savings
• Immediate image preview and availability– Increased room utilization– Better turnaround times and increased patient satisfaction
• Increased patient safety and “touch” time– Maintaining the competitive edge
• Referring physicians are more likely to recommend or refer to hospitals

Increased Workflow Efficiencies and Time Savings
• Increased workflow efficiencies– A digital room can take the place of two or
more analog rooms– Some systems allow radiology administrators
to track usage and workflow performance of different users• Determine which technologists are the most
efficient and identify problem areas
• Time savings– View images immediately equates to saving
10 minutes per patient– Reduce the average report turnaround time – Allow radiologists/physicians immediate
access to images wirelessly

Maintaining a Competitive Edge• An informed patient
– The information age is changing how patients seek out care • Patients are becoming
increasingly well informed about the advantages of digital systems
– Hospitals are increasingly faced with the challenge of competing for patients
• Digital technology creates confidence for referring physicians• Gaining more referrals, in areas where multiple hospitals are competing for the
same patients is difficult

Prioritizing the Digital Transition• High-volume areas, such as the ER, are converted first
– The largest impact comes from improved turnaround times – Items to consider when prioritizing
• What are patient volumes, types and programs?• Which rooms do you use for outpatient referrals? • Which room(s) are used for inpatient routine exam traffic? • Do you have areas in your department that are not centralized that needs workflow
efficiency improvement?
• Mobile c-arms, lower volume rad rooms and R/F rooms are converted last• Fleet management and inventory review
– Move early, digital generation systems to facilities and clinics with lower exam volumes – Review inventory with clinical engineering or BME departments
• Age of CR and analog systems• Repair histories: replace the oldest and problem units first

When and Where Analog Is Still Appropriate
• CR is still appropriate in low-volume exam scenarios – CR has longer processing and exam times for patients
• When to go digital in general radiography?– All in or one at a time are both viable approaches– Concerns associated with handling conversions one at a time
• Continuity in technology for staff and physicians• Questions over discrepancies in image quality for analog vs. digital
– End of life decisions• Easier to purchase digital systems during end of life scenarios

The Cost of “Going Digital”• General radiology can have a significant impact on patient volumes and
the bottom line• Clinical and soft dollar benefits can offset the financial investment of
“going digital”– Clinical advantages: higher image quality, less distortion, greater anatomical
coverage area and potential for dose reduction– Soft dollar benefits: increased workflow efficiencies and patient satisfaction
along with time savings

Questions and Answers