Embed Size (px)
Citation preview

1

2
Arthur Dessi Roman MD MTM FPCP FPSMID
Internal Medicine – Infectious Diseases
Outline
• Basic Bacteriology– Structure and Characteristics– Bacterial Culture
• Host defenses• Cases
– Gram positive Pathogens– Gram negative Pathogens– Bonus(es)
• Question and Answer Portion• Sportswear Competition

3
Highschool recall: Eukaryotes
• Eukaryote - organism whose cells contain complex structures enclosed within membranes
– the defining membrane-bound structure is the nucleus, which contains the genetic material
– also contain other membrane-bound organelles: mitochondria, chloroplasts and the Golgi apparatus
– e.g. animals, plants and fungi
Highschool recall: Prokaryotes• Prokaryote - NO cell nucleus , or any other
membrane-bound organelles. – DNA and other sites of metabolic activity: openly
accessible, free-floating
– asexual reproduction, usually by binary fission or budding
– Genetic exchange and recombination still occur, but this is a form of horizontal gene transfer and is
NOT a replicative process, simply
involving the transference of DNA
between two cells, as in
bacterial conjugation.

4
Size comparison of cells
Bacterium
Bacterial cell structure

5
Prokaryotes Eukaryotes
Simple structure Membrane-bound structures (nucleus, mitochondria)
Plasmids
Peptidoglycan that strengthens bacterial cell wall
Bacterial morphology

6
Generalities
• Most cocci are gram positive
• Most bacilli are gram negative
Gram positive Bacilli/rods
• Bacillus sp.– Normal flora of the skin
– B. anthracis, B. cereus
• Lactobacillus (shirota strain et al)
• Corynebacterium
• Clostridium sp.
• Listeria
• Erysipelothrix

7
Gram negative cocci
• N. meningitides, N. gonorrhea
• Acinetobacter spp.
• Coccobacilli:
– Pasteurella multocida
– Bordetella pertussis
– Legionella
Identify

8
Identify
Identify

9
Bacterial morphology
Gram staining

10

11
The Gram Stain
• Quick procedure that reveals bacterial cell morphology (cocci vs. bacilli, G+ vs G-)
• Gram negative: red/pink
• Gram positive: violet/blue
• The color difference is based on the amount of the peptidoglycan layer (G+=thick = more dye uptake=blue/violet color)
• Results guide initial antibiotic therapy
The Prokaryotic genome has many plasmids.
• encode genes that carry specialized functions (eg. Resistance to bacteria)
• Also encode for genes that mediate their transfer from one organism to another as well as other genes associated with genetic acquisition or rearrangement of DNA.

12
Rise of the superbugs
Resistance of bacteria to antibiotics after their liberal use in hospitals may be assimilated by plasmids of other non-resistant bacteria
Gram-positive vs Gram-negative cell wall

13
Gram-positive & Gram-negative cell wall
Gram + Gram -
Cell wall made of thick peptidoglycan
Thin peptidoglycan
No outer membrane Outer membrane present
No endotoxin contains LPS/ Lipid A/ endotoxinresponsible for sepsis
More susceptible to penicillins(lysozymes, detergents, etc.) due to
absence of outer layer
Outer membrane provides barrier has porins for entry of
nutrients
NO periplasmic space Periplasmic space contains B-lactamase/other enzymes that may
degrade antibiotics
Possess teichoic acids NO teichoic acids

14
Bacterial cell wall peptidoglycan
PBPs
• Penicillin-binding proteins (PBPs) catalyze the synthesis of the PG in the cell wall
• B-lactam antibiotics work by inhibiting PBPs
• Some bacteria produce enzymes that alter the PBPs or inactivate the B lactam ring resistance

15
Beta-Lactams
Sulbactam
• A beta-lactamase inhibitor
• Binds to B-lactamase irreversible B-lactamasecanNOT deactivate the beta-lactam ring

16
Beta-Lactams
Meropenem

17
(Livermore and Woodford, Trends in Microbiol, 2006)
The Gram Negative Cell Wall
Porin
channels
PBPs
Efflux system
B-lactamases
Mechanism of Resistance to β-lactams
CELL WALL
PENICILLIN BINDING
PROTEIN (cell wall
synthesis)
S. aureus

18
BETA-LACTAM ANTIBIOTIC
S. aureus
mecA gene
DNA
SCC
PBP2A
MRSA

19
Anaerobic vs. aerobic bacteria
• Aerobic: need oxygen to grow
• Anaerobic: fail to grow in the presence of oxygen
• Obligate anaerobes: grow only in aerobic environment
• Facultative anaerobes: can grow with or without oxygen
• Microaerophilic bacteria: grow best in an environment with reduced oxygen
• Aerotolerant: can grow in the presence of air, but do NOT use oxygen
Important Bacterial Pathogens
Bacteria
Gram positive* Gram negative* Atypical
Cocci Bacilli Cocci Bacilli
*can be aerobic/anaerobic

20
Spot Quiz
What are single-celled, prokaryotic microorganisms that sometime produce disease in humans and are usually susceptible to antibiotics?
Answer: BACTERIA

21
What is the rigid structure outside the cell membrane which protects and maintains the shape of bacteria?
Answer: CELL WALL
What is the main component of bacterial cell walls?
Answer: PEPTIDOGLYCAN

22
What are the proteins that facilitate formation of peptidoglycans?
Answer: PENICILLIN-BINDING PROTEINS (PBPs)
What is the procedure that can help visualize bacteria under the microscope and differentiate them into gram-positive and gram-negative bacteria?
Answer: GRAM STAIN

23
Differentiate the call walls of gram-positive and gram-negative cell walls.
Answer: Gram-negative cell walls have an outer membrane made up of a thinner layer of peptidoglycan and an outer membrane, which is in turn made up of lipopolysacharide or endotoxin.
What is the enzyme that can degrade beta lactam antibiotics found in the periplasmic space of gram-negative bacteria?
Answer: BETA LACTAMASE

24
The outer membrane of gram-negative bacteria act as a barrier to some antibiotics, but antibiotics and other nutrients can enter the bacteria via “holes” called:
Answer: PORINS
Differentiate aerobes from anaerobes.
Answer: Aerobes are bacteria that need oxygen to grow, while anaerobes are bacteria that cannot grow in the
presence of oxygen.

25
Bacterial reproduction via binary fission
Bacterial culture

26
Bacterial Identification
• Subsequent bacterial identification is based from initial Gram staining results from bacteria from isolated colonies on agar plate
• Subsequent testing uses bacterial nutritional requirement and metabolic capacities
• Most bacteria will grow in 24-48 hours except for fastidious or anaerobes which may require more time.
• Culture/identification is performed so a physician can come up with a diagnosis and prescribe the most appropriate antibiotic.

27
Normal Flora

28
Bacterial growth curve
Pathogens
• Microorganisms causing disease
• Pathogenicity: ability to cause disease (increased by the presence of bacterial enzymes and bacterial toxins)
• Stages of infection: adherence, invasion, multiplication, dissemination in the host

29
Host Defenses
Types of Infection
Acute: Chronic:- develop rapidly - develop more slowly- usually associated with fever - milder symptoms- generally of short duration - longer-lasting Acute infections may become chronic, chronic infections may
become acute.
Local: Systemic:- Limited to one site - throughout the bodyLocal infections may occasionally cause systemic symptoms or
may serve as nucleus for spread of infection to other body areas (e.g. dental infection).

30
Types of Infection
• Bacteremia: presence of bacteria in the blood.
• Septicemia: blood poisoning; systemic disease associated with presence and persistence of pathogenic microorganisms or their toxins in the blood.
Phases of Infection
1. Invasion: Bacteria gain entry into the host, or host tissues, where it’s not part of normal flora.
2. Incubation: Period before any manifestation of illness. It represents the time required for pathogens to multiply to a critical population size. Patient can be infectious.
3. Prodrome: Period characterized by nonspecific symptoms (e.g. headache, malaise).
4. Clinical illness: Period when specific symptoms (fever) appear. Body damage may result due to toxin, death of host cells, actions of host’s immune system.
5. Convalescence or Resolution: Period of recovery, even without symptoms patient may still be infectious.

31
Symptoms of Infection
• Provide subjective information on patient’s condition.
• Inflammation: Process that occurs in tissues as a reaction to injury. It involves vasodilation, increased permeability of capillaries to fluid and large molecules, and attraction and accumulation of WBCs and other immune system components in injured area.- Results in pain, swelling, heat and throbbing.
• Fever: Not true in all infections. Microbes produce pyrogens (fever-causing substances) that cause release of cytokines that cause the fever.
• Symptoms depend on organs or systems affected and are helpful to MDs in diagnosing specific conditions.
Signs of Infection
• Provide objective measures of disease; vary depending on nature and severity of condition.
• Fever: Both a sign and symptom. • Increased number of neutrophils in blood.• Increased in proportion of immature WBC (shift to the left).
• Neutropenia or granulocytopenia: abnormally, low neutrophils in overwhelming, severe infections. (Normal value: 1,500-7,800 /mL). The incidence of infection rises as neutrophil count declines.
• Anemia: reduction below normal in number of RBCs per mm3,
hemoglobin, or volume of packed RBC per 100 ml of blood.• Increased ESR (erythrocyte sedimentation rate) which measures the
rate at which RBCs settle in uncoagulated blood – a non-specific measure of inflammation or disease activity.

32
Signs of Infection
• Elevated blood levels of C-reactive protein.
• Increase in pulse rate, respiration rate, anxiety, confusion, delirium, and other abnormalities in mental status.
• Hyperglycemia: elevated blood sugar levels, especially in diabetics.
• Changes in kidney and liver function.
Non-specific host defenses
• Directed against any pathogen
• Mechanical
• Chemical
• Phagocytes and complement system

33
Non-specific immunity: cilia
Non-specific immunity: phagocytes

34
Specific immunity: antibodies
Specific immunity: T cells

35
Spot quiz(zes)
What do you call the microorganisms that normally live in our bodies?
Answer: NORMAL FLORA

36
What do you call a microorganism that cause disease?
Answer: PATHOGEN
What do you have when bacteria invade body tissues, multiply in them, and cause damage to the host’s cells?
Answer: INFECTION

37
What do you call the body’s response to infection?
Answer: IMMUNITY
What is the importance of knowing the normal flora in terms of dealing with infections?
Answer: It helps in determining EMPIRIC THERAPY.

38
Antibiotic Classes
32
Case 1• 35/male who was admitted for severe
abdominal pain and fever.
• Took paracetamol but did not improveER
• PE: febrile, direct and rebound tenderness RLQ

39
32
Case 1• A> Acute appendicitis underwent OR
• He was discharged improved.
• On ff-up with the surgeon after 5 days,
STAPHYLOCOCCUS

40
Staphylococcus aureus
• frequently found in the human respiratory tract and on the skin
• NOT always pathogenic• Causes skin infections (e.g. boils), respiratory disease
(e.g. sinusitis), and food poisoning• Producing potent toxins• Common cause of device-related infections• Carriage in healthy individuals (nostrils)• The emergence of antibiotic-resistant forms of
pathogenic S. aureus (e.g. MRSA) is a worldwide problem in clinical medicine.
Staphylococcus aureus
• Virulence factors
– Coagulase
– Staphylokinase
– Hyaluronidase

41
Coagulase and Staphylokinase
Staphylokinase
Staphylokinase
Clotting protein
36
Hyaluronidase (Spreading factor)
Hyaluronidase digests hyaluronic acid,
the “glue” that holds cells together
37

42
Clinical manifestation of S. aureus infection
38
40

43
Staphylococcus aureus
1. Local Stap. Infection – drainage
> antibiotics –semi synthetic PCN
Cloxacillin Erythromycin
Cehalosporin (1st gen.)
2. Systemic Infection: Parenteral
Vancomycin Oxacillin
Methiallin Cephalosporin
QuestionWhat is the current MRSA rate in the Philippines according to the ARSP 2014?
A. <5%
B. 35%
C. 60%
D. 90%

44
QuestionWhat is the current MRSA rate in the Philippines according to the ARSP 2014?
A. <5%
B. 35%
C. 60%
D. 90%
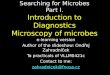
Percent resistance of S. aureus, (n=3,529), ARSP, 2014
ANTIMICROBIAL RESISTANCE SURVEILLANCE PROGRAM 2014 ANNUAL REPORT
30
FIGURE 32. Yearly penicillin, oxacillin and vancomycin resistance rates of S. aureus,
ARSP, 2005-2014
FIGURE 33. Yearly clindamycin, co-trimoxazole and tetracycline resistance rates of S.
aureus, ARSP, 2005-2014
ANTIMICROBIAL RESISTANCE SURVEILLANCE PROGRAM (ARSP) 2014 ANNUAL REPORT,
Research Institute for Tropical Medicine, Department of Health Philippines

45
Percent resistance of S. aureus, (n=3,529), ARSP, 2014
ANTIMICROBIAL RESISTANCE SURVEILLANCE PROGRAM (ARSP) 2014 ANNUAL REPORT,
Research Institute for Tropical Medicine, Department of Health Philippines
Percent resistance of S. aureus, ARSP, 2014
ANTIMICROBIAL RESISTANCE SURVEILLANCE PROGRAM 2014 ANNUAL REPORT
29
Antimicrobial Resistance
The 2014 resistance rate of S. aureus against the β-lactam oxacillin is at 60.3% (n=3,323; 95% CI: 58.6-62). The 2014 rate of methicillin-resistant S. aureus (MRSA) rates
increased significantly from 53.2% in 2013 to the 60.3% in 2014 (p value 0.0001). Resistance
rates against the antibiotics tested against S. aureus for 2014 and the past decade are see n
FIGURES 40-43. The 2014 resistance rates to the rest of the antibiotics tested did not differ
significantly from the reports from 2013 except for the significant increase in co-trimoxazole
resistance from 14% in 2013 to 22% for 2014 (p value 0.0001). Although there were 17 isolates
reported as vancomycin resistant, none of these S. aureus isolates were sent for confirmatory
testing at the reference laboratory.
FIGURE 30. Percent resistance against penicillins, vancomycin, clindamycin and
erythromycin of S. aureus, ARSP, 2014
FIGURE 31. Percent resistance against rifampin, ciprofloxacin, co-trimoxazole, linezolid and
tetracycline of S. aureus, ARSP, 2014
ANTIMICROBIAL RESISTANCE SURVEILLANCE PROGRAM (ARSP) 2014 ANNUAL REPORT,
Research Institute for Tropical Medicine, Department of Health Philippines
• Overall cumulative MRSA rate for 2014 was at 60.3%
(from 53.2%, p=0.0001)
• 85% were isolated from specimens taken from patients in
the OPD, emergency room and admission within their 1st
2 hospital days
• 60% MRSA rate from all blood isolates (n=570)

46
Enterococci
• Gram-positive cocci in chain
44
Enterococci
• Gram-positive cocci in chain
• Commensals of the GI tract of humans & animals
• Diseases :
• Consist of 16 species :- E. faecalis, E. faecium
- Urinary tract infection (UTI)
- Bacteremia, endocarditis
44

47
Vancomycin-Resistant
Enterococci (VRE)
46
• An emerging pathogen but none yet in PH
• Acquired via plasmids
• Cephalosporin use is a risk factor
• Can be carried by healthy people
32
Case 2• 65/male DM, HPN admitted for sudden left
sided weaknessER
• PE: no motor movement left UE and LE, shallow right NSLF, slurred speech

48
32
Case 2• Treated as stroke and underwent rehab after 5
days doing well
• On Day 6 cough and difficulty of breathing, high fever, auscultation revealed rales on right lung field
• Eventually intubated due to respiratory distress
Case 2• Started empirically on PipTazo
• ETA GS revealed many PMNs and many Gram _____________.

49
Pseudomonas aeruginosa
•Aerobic gram-negative bacilli, non-spore forming
•Produces cyanin pigment
•Produces grape-like odor
•Inhabitant of the GI tract
•Saprophytic (natural habitat: soil and water)
•An opportunistic pathogen
Pseudomonas aeruginosa
•

50
• MOST important hospital-acquired pathogen
• Other pseudomonads: Burkholderia mallei, Burkholderia cepacia
•High tendency to develop antibiotic resistance
Pseudomonas aeruginosa
21
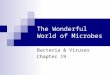
Resistance Pattern of P. aeruginosa, ARSP 2011

51
23
• Causes nosocomial infections- extensive burns, trauma to the skin or conjunctiva, urinary tract manipulations
• cystic fibrosis.
• Ear infections – swimmer’s ear
• Bacteremia in debilitated patients, accounts for 10% of all Gram(-) associated with a 50% mortality rate
Pseudomonas aeruginosa
21

52
Treatment
• Aminoglycosides
• Third and fourth generation cephalosporins(ceftazidime, cefepime)
• Carbapenems (imipenem, meropenem)
• Pip-tazo
• Colistin
Pseudomonas aeruginosa
Clinical manifestation of P. aeruginosainfections

53
32
Case 3• 15/male with cerebral palsy recurrently
admitted for pneumonia
• He already has a tracheostomy tube in place
• Developed progressive cough and respiratory distressER
32
Case 3• PE: drowsy, highly febrile, rales all over R>L
• Hooked to MV and started on Pip-Tazo

54
Case 3• After 3 days of antibiotics, he was still febrile
• Developed hypotension and further respiratory distress
Case 4
• EC = few PMN=moderate
• Gram negative diplococci-few
• Gram negative coccobacilli-many

55
Acinetobacter
• Aerobic gram-negative coccobacilli,
non-spore forming• > 25 species
•A common cause of ventilator-
associated pneumonia (VAP)
•Opportunistic pathogen
28
• Local isolates are very highly
resistant to antibiotics
A. baumannii
Clinical manifestation of A. baumanniiinfection1.Hospital-acquired pneumonia
especially VAP
2.Community-acquired pneumonia :The source of infection may be throat carriage, which occurs in 10% of community residents with excessive alcohol consumption
3.Bloodstream infection & endocarditis
4.Skin/soft tissue infection
5.UTI
6.Meningitis
29

56
A. baumannii
Persistence in the hospital
environment : 3 days to 5 months
1. Resistance to major antimicrobial
drugs
2. Resistance to desiccation
3. Resistance to disinfectant
Three factors contributing to the
persistence
31
A. baumannii
31

57
A. baumannii
Treatment:
• Meropenem
• Colistin
• Tigecycline
• Ampicillin-Sulbactam
31
Acinetobacter
• Aerobic gram-negative coccobacilli,
non-spore forming• > 25 species
•A common cause of ventilator-
associated pneumonia (VAP)
•Opportunistic pathogen
28
• Local isolates are very highly
resistant to antibiotics

58
A. baumannii
Clinical manifestation of A. baumanniiinfection1.Hospital-acquired pneumonia
especially VAP
2.Community-acquired pneumonia :The source of infection may be throat carriage, which occurs in 10% of community residents with excessive alcohol consumption
3.Bloodstream infection & endocarditis
4.Skin/soft tissue infection
5.UTI
6.Meningitis
29
A. baumannii
Persistence in the hospital
environment : 3 days to 5 months
1. Resistance to major antimicrobial
drugs
2. Resistance to desiccation
3. Resistance to disinfectant
Three factors contributing to the
persistence
31

59
A. baumannii
31
A. baumannii
Treatment:
• Meropenem
• Colistin
• Tigecycline
• Ampicillin-Sulbactam
31

60
Enterobactereaceae
• Gram-negative, nonspore-forming rods
• Facultative anaerobic
• Grow in simple media (MacConkey agar)
• Ferment glucose (LF)
• Motile with peritrichous flagella except Shigella
• Some possess capsule
Impt. Human pathogens
• Escherichia - E. coli
• Enterobacter (E. aerogenes, E. cloacae)
• Citrobacter - C. freundii
• Serratia - S. marcescens
• Hafnia - H. alvei
• Klebsiella

61
*Proteus Group
– P. mirabilis
– P. vulgaris
– Morganella – M. morganii
– Providencia – P. rettgeri
*Edwardsiella – E. hoshinae
Escherichia coli
• Escherichia coli and certain related bacteria (e.g., Klebsiella, Enterobacter, Citrobacter) form the group known as the coliforms
• presence in drinking water is considered evidence of fecal contamination
• used as an index of fecal pollution.

62
Epidemiology
• Fecal-oral transmission transmission among infants in hospital nurseries.
• Food-borne transmission of E. coli 0157:H7 -contaminated meat, from cattle; this serotype behaves as a zoonotic agent.
• UTI –perineum; In women, UTI is associated with sexual activity, hence the term "honeymoon cystitis".
Diseases associated with Escherichia coli:
• Diarrhea
• Meningitis – impt. cause of neonatal meningitis in the neonates
• Sepsis
• Urinary Tract Infection -most common cause

63
Gram’s Stain and Culture
Klebsiellae
• Encapsulated
• The species of Klebsiella include
- Klebsiella pneumoniae- most infections
-Klebsiella oxytoca
-Klebsiella ozaenae
-Klebsiella rhinoscleromatis

64
• Mucoid colony
• มแีคปซลูหนา
Klebsiella18
Diseases:
• Community acquired and nosocomial pneumonia w/ underlying medical problems such as alcoholism, COPD or diabetes mellitus
• Lung abscess may also develop.
• Urinary tract infection
• Wound infection
• Epidemic diarrhea - newborns
• Septicemia

65
• Hypermotile
• Swarming
growth
Proteus vulgaris

66
Enterobacteriaceae: Treatment
• Empiric therapy with aminoglycoside and third cephalosporin
Case 4
• 35/female who just delivered a baby boy via NSD 1 week ago rushed back to the ER for severe hypogastric pain
• PE: highly febrile, direct tenderness at the hypogastric area, purulent vaginal discharge
• Diagnosis?
• Started on meropenem and clindamycin(MRSA)

67
Case 4
• She underwent EL on Day 3
• Doing well
• Day 10 of meropenem and clinda, developed high fever
• No cough. No dysuria but she was having LBM 5-7x/day
• Diagnosis?
Clostridium Difficile• Gm (+) bacillus, obligate anaerobe
• Spore forming contact precautions
• Causes pseudomembranous colitis and antibiotic-associated diarrhea

68
Laboratory Diagnosis
• Culture of stool specimens
• Cytotoxin Assay
– Tissue culture assay
– immunoassays
• Colonoscopy or Signoidoscopy with Biopsy Endoscopic findings – pseudomembranes and hyperemic rectal mucosa
Treatment• Antimicrobial therapy should be
discontinued
• Maintenance of fluid & electrolyte balance
• Avoid drugs which intestinal motility

69
• Drug of choice
– Metronidazole (30 mg/day in 4 divided doses) – drug of choice in the initial treatment of most patients with colitis
– Oral Vancomycin (40 mg/kg/day in 4 divided doses) – indicated only for seriously ill patients or those who do not respond to vancomycin
– Bacitracin – ssecond alternative therapeutic choice
Case 5
• 70/female post stroke and chronically bed ridden was admitted for decreased sensorium
• Because of urinary incontinence, has been on foley catheter and PEG for episodes of aspiration
• PE: drowsy, T 37 C BP 70/50 HR 100
• Clear breath sounds, no nuchal rigidity

70
Case 5
• Labs done: WBC 20 Neut 90%
• Chest xray: normal
• Urinalysis: WBC 50 RBC 0-3 EC few yeast cells few
• Started on Ceftriaxone 1g IV q24h
• FC was changed
• Urine GS CS requested
Case 5
• Urine GS: PMN many yeast cells few G+cocciin clusters many

71
Candida spp.
• normal flora of the skin, mucous membranes, and gastrointestinal tract
• colonize the mucosal surfaces of all humans during or soon after birth
• Candida albicans – the most common pathogen
• Others: C albicans, C tropicalis, C parapsilosis, C glabrata, C guilliermondii, and C dubliniensis)
• The widespread use of fluconazole has precipitated the emergence of more azole-resistant species, such as C kruseiand C lusitaniae.
Cutaneous & Mucosal Candidiasis
• The risk factors: AIDS, pregnancy, diabetes, young or old age, birth control pills, and trauma (burns, maceration of the skin), corticosteroids or antibiotics, hyerglycemia, and cellular immunodeficiency
• Cutaneous candidiasis- when the skin is weakened by trauma, burns, or maceration.
Vulvovaginitis - irritation, pruritus, and vaginal discharge;
often preceded by factors such as diabetes, pregnancy, or
antibacterial drugs that alter the microbial flora, local acidity,
or secretions.

72
Systemic Candidiasis (Candidemia)
• Causes:
– indwelling catheters, surgery, intravenous drug abuse, aspiration, or damage to the skin or gastrointestinal tract
• most often associated with:
– chronic administration of corticosteroids or other immunosuppressive agents; with hematologic diseases such as leukemia, lymphoma, and aplastic anemia; or with chronic granulomatous disease
Candidiasis: Treatment
• Systemic candidiasis: amphotericin B with/without oral flucytosine, fluconazole, or caspofungin

73
Outline
• Basic Bacteriology
– Structure and Characteristics
– Bacterial Culture
• Host defenses
• Gram positive Pathogens
• Gram negative Pathogens
• Bonus(es)
감사합니다!!!! ㅋㅋㅋ