Embed Size (px)
Citation preview

Vision Health – An Integral Part of Public Health
*C.A.E Emereole1, C.A.Ogugua1and C.L. Amuneke1
1. Department of Optometry Imo State University, Owerri.
*Corresponding Author Email: [email protected] Phone: +234-803-540-7341
ABSTRACT
As our populations continue to live longer, the challenge of maintaining good vision is
increasing. Vision disorders and eye diseases are major public health problems, both nationally
and internationally. Optometrists with training and experience in public health need to assess
community needs for vision care services, to determine which factors contribute to treatment
and prevention of visual system anomalies, to develop and apply quality assurance systems, to
participate and provide leadership in health-related agencies, and to foster public awareness
of the need for vision care. Optometrists in public health are expected to have the capability to
develop, administer, and evaluate eye and vision health programs in research projects; design
and conduct epidemiological field studies, and use statistical methods for these data analyses;
develop and implement vision health education programs; and develop occupational health
and eye safety programs. The Nigeria national blindness and visual impairment survey
conducted in 2005-2007 showed that of a total of 13,599 persons aged 40+ who were
examined across the country, the prevalence of blindness in the sample using presenting vision
(PVA) of <3/60 in the better eye was 4.2% (95% CI: 3.8 to 4.6%) and the prevalence of severe
visual impairment (SVI) was 1.5% (95 % CI: 1.3 to 1.7%). Using best corrected vision (BCVA) in
the better eye, 3.4% (95% CI: 3.0 to 3.8%) were blind, 0.8% (95% CI: 0.7 to 1.0%) had SVI, 5.3%
(95% CI: 4.9 to 5.8%) had moderate visual impairment, 4.5% (95% CI: 4.1 to 4.9%) had mild
visual impairment while 86% (95% CI: 85.2 to 86.8%) were categorized as normal/near normal.
Preventable blindness is one of our most tragic and wasteful global problems.
Keywords: Vision health, Preventable blindness, Epidemiology, Public awareness.

VISION HEALTH – AN INTEGRAL PART OF PUBLIC HEALTH:
THE OPTOMETRISTS ROLE IN PUBLIC–PRIVATE PARTNERSHIP FOR THE DELIVERY OF
QUALITY EYE CARE SERVICES.
INTRODUCTION:
As our populations continue to live longer, the challenge of maintaining good vision is
increasing. Vision disorders and eye diseases are major public health problems, both nationally
and internationally. Optometrists with training and experience in public health need to assess
community needs for vision care services, to determine which factors contribute to treatment
and prevention of visual system anomalies, to develop and apply quality assurance systems, to
participate and provide leadership in health-related agencies, and to foster public awareness
of the need for vision care. Optometrists in public health are expected to have the capability to
develop, administer, and evaluate eye and vision health programs in research projects; design
and conduct epidemiological field studies, and use statistical methods for these data analyses;
develop and implement vision health education programs; and develop occupational health
and eye safety programs. Hence, Optometry plays a great role in the attainment of Public
health objectives.
WHAT IS PUBLIC HEALTH?
Public health is "the science and art of preventing disease, prolonging life and promoting health through the organized efforts and informed choices of society, organizations, public and
private, communities and individuals. It is concerned with threats to health based on population health analysis. The population in question can be as small as a handful of people
or as large as all the inhabitants of several continents. The dimensions of health can
encompass "a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity", as defined by the United Nations . Public health incorporates the interdisciplinary approaches of epidemiology, health informatics, biostatistics, sociology and demography, health education and promotion, management, and other health services. Environmental health, community health, behavioral health, health economics, public policy, insurance medicine and occupational health (respectively occupational medicine) are other important subfields.
The focus of public health intervention is to improve health and quality of life through the prevention and treatment of disease and other physical and mental health conditions, through surveillance of cases and health indicators, and through the promotion of healthy behaviors.
Modern public health practice requires multidisciplinary teams of professionals including physicians specializing in public health/community medicine/infectious disease,
epidemiologists, biostatisticians, public health nurses, medical microbiologists, environmental health officers / public health inspectors, pharmacists, dental hygienists, optometrists,
dietitians and nutritionists, veterinarians, public health engineers, public health lawyers, sociologists, community development workers, communications experts, and others .
Another focus of a public health intervention is to prevent and manage diseases, injuries and
other health conditions through surveillance of cases and the promotion of healthy behaviors,
communities and environments. Many diseases are preventable through simple, non-medical
methods. Public health surveillance has led to the identification and prioritization of many
public health issues facing the world today, including HIV/AIDS, diabetes, waterborne diseases,
zoonotic diseases, preventable blindness, and antibiotic resistance .
The World Health Organization (WHO) identifies core functions of public health programs to include:
Providing leadership on matters critical to health and engaging in partnerships where joint action is needed;
Shaping a research agenda and stimulating the generation, translation and dissemination of valuable knowledge;
Setting norms and standards and promoting and monitoring their implementation; Articulating ethical and evidence-based policy options; Monitoring the health situation and assessing health trends.
In particular, public health surveillance programs can:
Serve as an early warning system for impending public health emergencies; Document the impact of an intervention, or track progress towards specified goals; and
Monitor and clarify the epidemiology of health problems, allow priorities to be set, and inform health policy and strategies.
Diagnose, investigate, and monitor health problems and health hazards of the community
OVERVIEW OF THE VISION HEALTH SITUATION IN NIGERIA In 2002 the World Health Organization (WHO) revised estimates of the global magnitude and causes of blindness which revealed a paucity of recent data for most countries in the African region. Though Nigeria is the most populated country in Africa, with a population of 135 million, no national data on the prevalence and causes of blindness exist. Most data used for planning eye care services are generated either from urban areas where the large eye hospitals are situated or from small, focal surveys. These small studies indicate that blindness is likely to
be a public health problem but such data cannot be extrapolated to the entire country as the population is culturally, ethnically and geographically diverse. Similarly, national survey results from other West African countries (e.g. Benin, 1990; The Gambia, 1986, 1996, Cameroon,
1996) may not be readily comparable to present day Nigeria. Differences in population size, demographic profiles, climate and eye care service accessibility and provision contribute in
determining the frequency and distribution of conditions such as trachoma and onchocerciasis as well as other causes of visual loss (e.g. cataract, glaucoma).
The National Blindness and Visual Impairment Survey in Nigeria was conducted in 2005-2007
(30 months of field work). A total of 13,599 persons aged 40+ were examined across the country (response rate 89.9%). The prevalence of blindness in the sample using presenting
vision (PVA) of <3/60 in the better eye was 4.2% (95% CI: 3.8 to 4.6%) and the prevalence of severe visual impairment (SVI) was 1.5% (95 % CI: 1.3 to 1.7%). Using best corrected vision
(BCVA) in the better eye, 3.4% (95% CI: 3.0 to 3.8%) were blind, 0.8% (95% CI: 0.7 to 1.0%) had SVI, 5.3% (95% CI: 4.9 to 5.8%) had moderate visual impairment, 4.5% (95% CI: 4.1 to 4.9%) had

mild visual impairment while 86% (95% CI: 85.2 to 86.8%) were categorized as normal/near
normal.
Associations of blindness and visual impairment with socio-demographic factors revealed that the prevalence of blindness among those aged – 50 years was 5.5% (476/8702) and 9.3%
(476/5125) among those aged - 60 years (PVA <3/60 in the better eye) The prevalence of blindness (PVA) increases significantly with increasing age, from 0.8% (95% CI: 0.5 to 1.1%) at
40-49 years to 23.3% (95% CI:20.2 to 26.7%) among those aged _ 80 years (p =<0.001) Females had a higher prevalence of blindness than males (4.4% vs 4.0%) (p =<0.001). Illiterate
participants had far higher prevalence of blindness than those who could read and write (5.8% vs 1.5%) (p = <0.001) The South West GPZ had the lowest prevalence of blindness (2.8%; 95%
CI: 2.2 to 3.5%) and the North East GPZ had the highest (6.1%; 95% CI: 4.7 to 7.9%) (p = <0.001) The prevalence of blindness and SVI did not differ by urban/rural place of residence (p=0.18).
In multivariate analysis, age, gender, GPZ and literacy remained significantly associated with blindness after adjusting for age and gender differences. It is estimated that 1,130,000
individuals aged – 40 years are currently blind in Nigeria (95% CI: 1.03-1.25 million). The North West geo-political zone (GPZ) has the largest number of blind adults (28.6%) being the zone with the largest population. A further 2,700,000 adults aged - 40 years are estimated to have moderate visual impairment and an additional 400,000 adults are severely visually impaired. Thus a total of 4.25 million adults aged - 40 years in Nigeria are visually impaired or blind. The prevalence of blindness varied across the different ecological zones being highest in the sahel (6.6%) and the lowest in the delta (3.3%). The prevalence of blindness in people of all ages was estimated to be 0.78%.
Amongst the Causes of blindness and visual impairment cataract was the commonest cause of severe visual impairment and blindness being responsible for 45.3% and 43.0% respectively.
The prevalence of cataract blindness was 1.8% (95% CI: 1.57-2.05). Glaucoma was the second commonest cause of blindness (16.7%) (prevalence 0.7%; 95% CI:0.6-0.9). Corneal scarring
from all causes was responsible for 7.9% of blindness. 84% of blindness was due to avoidable causes. Uncorrected refractive errors were the commonest cause of mild and moderate VI
(77.9% and 57.1% respectively) being responsible for visual impairment in 2.46 million adults in Nigeria (i.e. acuity of <6/12-6/60). “Operable” cataract (i.e. visual acuity of <6/60) affects
400,000 people and glaucoma has caused blindness in a further 150,000 adults. By the year 2020 the number of adults with operable cataract will increase by 43% to 600,000 assuming that the incidence of SVI and blindness due to cataract and cataract surgical coverage remain essentially unchanged over the next 12 years.
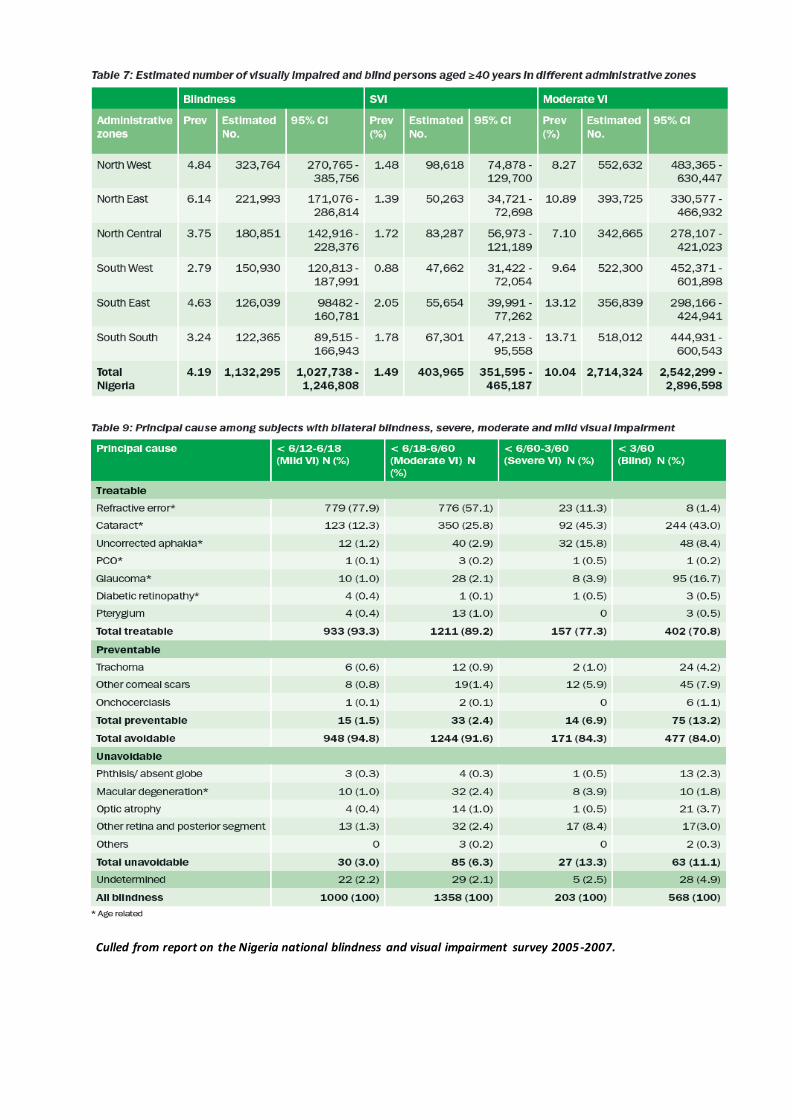
Culled from report on the Nigeria national blindness and visual impairment survey 2005-2007.
BLINDNESS IN NIGERIA: A PUBLIC HEALTH CHALLENGE – THE OPTOMETRISTS’ VOCATION
In 1999, in response to the observed trend in blindness data available the World Health
Organisation (WHO) and International Agency for Prevention of Blindness (IAPB), showed that unless active action is taken, a total 75million persons (based on projectio ns from available
blindness prevention data) would be blind worldwide by the year 2020. To this effect a movement called VISION2020: The Right-to-Sight was launched, and annually on the second
Thursday of every month of October, an advocacy day for this movement is observed.
The World Council of Optometry joined the VISION 2020 Task Force with Official Relations in 2003. The mission of the World Council of Optometry as written in its constitution is to facilitate the enhancement and development of eye and vision care world-wide. The World Council of Optometry, being the world-wide organization for the professionals working in the field of optometry, their associations and institutions, can facilitate the expansion of eye care providers, improve quality and access to eye and vision care, inform and educate the public regarding the importance of eye and vision care. Optometry’s responsiveness to the changing demographics and epidemiology of ocular and visual conditions complements the goals of the original VISION 2020 initiative. While contributing to all aspects of VISION 2020, Optometry will seek to make a major contribution to the alleviation of blindness and impaired vision due to Refractive Error and Low Vision.
By the year 2010, that is, 10 years down the lane, the impact of the activities mounted up had revealed a 10 to 13 percent reduction in visual impairment across board. Put simply, the
initiative and all it entails has proven to be “effective”!
According to the published reports of the recently conducted first National Survey on Blindness in Nigeria (between 2005-2007), at least 4 Nigerians out of a hundred (4.2 percent) are blind,
and even after issuing spectacles for best correction, the rate still remains as high as not less than 3 of 100. It also revealed that in every 100 blind Nigerians, Cataract was accountable for
43 of them, while Glaucoma accounted for another 17, Corneal Scars due to the triad of Vitamin A Deficiency, Measles and use of Traditional Eye medicines accounted for another 8,
while the remaining 32 would be due to Uncorrected Refractive Error, Aphakia, Trachoma, and
several Non-communicable disorders. Furthermore, the study implied that at least 1 million Nigerians are blind, and another 3 million are visually impaired.
Similar findings were true of such surveys by India (2005), and Pakistan (2003). In fact, the
International Agency for Prevention of Blindness (IAPB) in collaboration with World Health Organization (WHO) embarked on the activities of VISION2020: The Right-to-Sight in view of
such data. And till date, 90 percent of all visually impaired worldwide live in developing countries, 65 percent of them are aged above 50 years, 19 million children are visually
impaired, but the earth-shaking reality is: 80-90 percent Of Visual Impairment are avoidable or amenable To Control. Why is blindness Such a Burden then?
FACTORS AFFECTING THE REALIZATION OF VISION2020 OBJECTIVES IN NIGERIA.
The 3 Cardinal resources in any system are Manpower, Material and Money, and a proper
application of all these has always held the promise of achieving whatever goals set by such a system. A look at our total Health Care Sector, within which the eye care system can be found,
has a lot to say about such a burden as ours.
Manpower for Eye Health:
The survey revealed a human resource for eye health that is inadequate, ineffective and maldistributed. Not less than 80 percent of the total population of ophthalmologists and optometrists are based in the urban areas, while 70 percent Nigerians live in rural areas. There is a further geopolitically inequitable distribution of manpower as there could be up to 4 times the number of health workers in one zone as compared to another. There is also manpower underutilization leading to low productivity of ophthalmologist, optometrists, and other eye care team members.
Ignorance of available services, fear due to poor information on eye health issues, and poverty which is responsible for inability to make out-of-pocket payments for care services, as well as a
misplaced value system continues to enhance the gloomy statistics above. Hence as stated by the Federal government, on Service delivery “Health care services are fragmented, skewed in
distribution, limited in coverage and of poor quality. Also, there is a dearth of resources and referral systems are weak.” (FMoH, 2004)
Material Resources for Eye Health:
There is a minimum level of infrastructure needed to achieve the onerous task of VISION2020: The Right-to-Sight, by any national government and what we have on ground suffers from quality as well as quantity. Eye care is one field that is highly dependent on technology, with the rate of equipment engineering and procedural innovations on the international scene so
rapid that even the average eye care practitioner is kept on his/her toes just to keep abreast of the changes. The lack of optimal enabling environment for this is a major cause of low productivity. The services available at our centres may not be acceptable to the people due to socio-cultural issues, and it may be the reason that the survey detected that only about 47 out
of 100 eyes treated for straight forward cataract had formal cataract surgery, while another 43 eyes had the traditional cataract surgery (couching) which is usually of poor outcome, and the
rest 10 eyes had complicated cataracts necessitating the choice for formal care often times. We have outdated equipments sitting down in many of our secondary and tertiary centres,
thus making training of eye care human resource an arduous task for the trainers; retention strategies are poorly elucidated, giving room for continuous brain drain, and unending attrition, hence the rich venture often into Health Tourism Schemes in foreign lands, to sort
out their needs, while the 80 percent continue to languish in darkness and ‘pain’.
The present scenarios beg for a public-private partnership in order to achieve these objectives as the present situation is a far cry from the paintings on the VISION2020 blueprint given that
we are only 7 years away from the target year.
Funding For Eye Health:
Health Financing: At the national level the estimated per capita expenditure on health is $131
which falls very much short of the global average of $863. At the state level, where most secondary and primary care are provided, the health per capita spending is hardly up to $4. In
2010, federal budget allocation to health was 3.4 percent, and eyecare received less than 0.005 percent of that. The results of such underfunding can only be a weak health care s ystem,
helplessly watching the worsening trend in blindness.
THE NATIONAL HEALTH POLICIES and its Provisions for Vision health in the Public Health Scope in Nigeria.
One of the major weaknesses in the health sector currently is the non-existence of some important health legislations and the outdatedness, contradictions and ambiguities of some existing health laws. For example, the 1999 Constitution fell short of specifying what roles the various levels of government must play in the national health care delivery system. In formulating, updating and disseminating the laws and regulates as well as enforcing them, effective collaboration is to be maintained with the relevant stakeholders which include: the Federal and State Ministries of Health, the Federal and State Ministries of justice, Professional
Regulatory Bodies and the National and State Assemblies. An effective Information, Education and Communication system was therefore provided for in the Revised Health Policy of the
Federation, by the Eyitayo Lambo’s administration which saw to the inclusion of Eye health as part of the Nation’s utmost public health challenges.
“…vi. prevention and control of epidemic and endemic diseases indicators
shall specify disease specific incidence and prevalence rate; mortality for selected number of diseases; proportion of mortality rates from
communicable and non-communicable diseases; eyesight and lastly vector indices…”
(Revised National Health Policy, FMoH, September 2004)
NIGERIA’S FIGHT AGAINST BLINDNESS - The National Prevention of Blindness Programme
The National Programme for the Prevention of Blindness (NPPB) is the policy making organ of the Nigerian government, which also serves to coordinate activities and all matters relating to prevention of blindness and the rehabilitation of the blind. It was inaugurated in 1990 by the then Minister of Health, Late Professor Olikoye Ransome-Kuti. In setting up the NPPB, it was charged with a long-term goal of reducing the overall prevalence of blindness in the nation to 0.5% and to no more than 1% in any individual community. The short-term goals included
o Determination of causes and prevalence of blindness o Reduction of extent and nature of major blinding conditions
o Development of eye health manpower at all levels o Provision and strengthening of eye care facilities and ensuring access to referral
services etc.
It is chaired by the Director of Public Health of the FMOH, with the Vice Chairman who is usually the Chief Executive of the National Eye Centre, Kaduna. The National Secretariat is
situated at the FMOH Abuja. It is headed by a National Coordinator. There is a zonal
coordinator and one facilitator for each of the 6 geopolitical zones The National Committee is expected to meet twice yearly. The meetings are conducted on subcommittee levels and final
decisions are made by the Main Committee. The State PBL Committees are expected to operate in the same line.
Nigeria’s Vision 2020 Action Plan
The Mission of VISION 2020 – The Right to Sight is to eliminate the main causes of blindness in
order to give all people in the world, particularly the millions of needlessly blind, the Right to Sight. In line with the political structure, the NPPB representing the Federal Level provides
policy guidelines, planning support, monitoring, advocacy and coordination while the unit of implementation is the state or local government. In Nigeria, in order to render affordable,
accessible and efficient eye care service within the framework of VISION 2020, three essential elements would be employed namely:
Disease control Human resource development, Infrastructure and technology
These will be implemented through effective and efficient management, community participation and ownership elements which will be complemented by suitable Information, Education and Communication system, adequate resource mobilization and strong, persistent, coherent and coordinated advocacy.
General Objectives of the Nigeria’s Vision 2020 Action Plan
To control the major diseases that cause avoidable blindness in Nigeria
To train and appropriately deploy the human resources necessary for eye care delivery in Nigeria.
To provide needed technology and infrastructure for eye care delivery in Nigeria To advocate at all levels for the prevention of avoidable blindness
To achieve behavioural change through Information Education and Communication (IEC)
To mobilize resources for the implementation of VISION 2020 activities in Nigeria Sub-Objectives of the Nigeria’s Vision 2020 Action Plan
To strengthen cataract surgical service with a Cataract surgery rate (CSR) of at least 2000
To eliminate blindness due to trachoma To eliminate avoidable causes of childhood Blindness To eliminate blindness due to onchocerciasis To eliminate visual impairment and blindness due to refractive errors/low vision and
rehabilitate the irreversibly blind To reduce blindness due to Glaucoma
To attain the integration of primary eye care (PEC) into Primary health care (PHC) To train/retrain, equip and appropriately deploy ophthalmologists, ophthalmic nurses,
optometrists, opticians, equipment technicians and other staff for effective eye care
delivery system. To develop/strengthen technology and infrastructure for eye care
To mobilize communities and improve their participation in VISION 2020
To mobilize resources for VISION 2020
The General Strategy/Framework of Action Plan
The NPPB/Nigeria VISION 2020 National Steering Committee will work in tandem with all stakeholders (governments, private individuals, UN agencies, NGDOs etc) in strengthening and
advancing the VISION 2020 programme with shared responsibilities defined at the National, zonal, state, LGA and Community levels.
NATIONAL POLICY ON PUBLIC-PRIVATE PARTNERSHIP
The present administration has embarked on fundamental reforms of the health sector with a view to attaining the Millennium Development Goals (MDGs) and other National Health Policy targets. A central aspect of these health sector reforms is to mobilize and harness all resources – across both public and private sectors – for the benefit of the population. Accordingly, it is desirable to develop a national public private partnership (PPP) policy in health PPPs are not a new concept in Nigeria. Indeed, they are already practiced in different ways in every state. This policy therefore aims to build upon these current efforts, and to provide a framework for more sustained and effective action. This PPP policy affords all the tiers of government, interest groups, including other stakeholders to identify with any or all sections of the recommendations that are outlined in it. The challenge and/or expectation are to harness all
the abundant health care resources for the benefit for the people of Nigeria One of the key challenges to policy makers is how to form effective partnerships among
different players in such a way that health care can be served efficiently, effectively, and equitably. It is vital to understand the operation of different players, their strengths and
weaknesses, and based on such understandings, establish new relationships that will entail the act of learning, compromise, understandings and shared responsibilities. This collaboration will also allow for tolerance and the creation of an enabling environment and synergy that allows them to contribute more to the good of the general public than would have been achieved individually (NPPPP, 2005)
Principles, Values and Concepts In addition to the principles already mapped out in the National Health Policy, the following key principles will underpin all PPP actions in the health sector.
Governments (Federal, State and Local) share the obligation to ensure an enabling environment for the entire spectrum of (public and private) health provision. This obligation goes side by side with the parallel responsibility for ensuring that all people
are protected from harmful health practices, and have rights as consumers of health services.
A “public private partnership” is a collaborative relationship between the public and
private sectors aimed at harnessing (and optimizing the use of all available resources, knowledge, and facilities required to promote efficient, effective, affordable, accessible,
equitable and sustainable health care for all people in Nigeria.
Effective partnerships among private sector institutions, civil society organizations, and
governments will allow fulfillment of their social expectations without compromising core missions.
All formal (contractual) partnerships shall be based on written agreements specifying
the purpose, duration, and exit arrangements.
Partnership agreements shall clearly state the rights and obligations of all stakeholders. Such rights and obligations shall be enforceable.
Best practices shall be encouraged/rewarded based on potential to improve upon the quality of care provided
While for-profit institutions have a right (or an obligation) to make a profit, this has to be balanced against the equally important considerations of ensuring safety quality, and equity.
PPP shall be recognized as a long-time process which requires perseverance, regular attention, and maintenance.
There shall be ongoing communication/interaction on health issues by all stakeholders
in the public and private sectors. As part of such interactions and consultation, private sector organizations shall have opportunities to contribute towards the planning and implementation of policy.
There shall be decentralization of powers by government and acceptance of the expanded role of the private sector and the community.
Part of the wider governmental obligations will include provision of basic amenities
such as water supply, environmental sanitation, and power supply.
In keeping with these principles, all compendia of regulations, codes of ethics, guidelines and
other documentation pertaining to PPP shall be freely available to those in the public and private sectors, and also to consumers of health care, through annual publication, websites,
and other media.
Partners in Partnership The public sector “players” potentially involved in PPPs include the Executive and Legislative
bodies in all tiers of Government, as well as other public institutions (including the key health parastatals).
The private sector players are exceedingly diverse, and range across: the multiplicity of health
providers, enterprises, economic institutions (e.g. banks), and distribution companies,
Chambers of Commerce, Labour Unions, Faith Based Organizations, Non-Governmental Organizations, Philanthropists, Clubs/Societies, other Civil Society Organizations and Cooperatives. Other key partners include the Professional council, and Professional associations. A final stakeholder group are the consumers of health care – as individuals, family and community members.
Types of Partnerships
One key form of PPPs will be specific contractual relationships – whereby the private sector performs certain functions, or deliver specific programmes, on behalf of government. Such
PPPs may be employed by all tiers of government. In such partnerships, the responsibilities of both the private and public partners will be explicitly negotiated and documented at the outset
in the form of a partnership agreement, contract or Memorandum of Understanding (MoU).
Other ‘partnerships’ will be based around governments (Federal, State and LGA) carrying out specific institutional functions in the public interest, and for the public good. These include the
core governmental roles in regulating, and sustaining an enabling environment for, health markets.
Amongst the alternative types of partnership are ; Public Driven Partnerships can be Initiated
by public administrations who own more than 50% shares, having a Board of directors, and decision making will highly dependent on the public sector, who will have More than 50 per
cent involvement. Private Driven Partnerships: This will mainly be initiated by the private sector. Profit orientation may or may not be a primary goal (but would in any case need to be balanced alongside the principles of ensuring safety, quality and equity). The private partner will have more than 50% involvement in PPP while the Public sector acts as a monitoring and standard setting body. Goal/Mission of the National Policy on Public Private Partnership in the Health sector
In pursuance of the National Health Policy the goal is to strengthen the national health system
in order to provide effective, efficient, quality, accessible and affordable health service, the goal for public, private partnerships in health care provisioning is to promote and maintain all
forms of partnership and collaboration between the public establishments and the private sector with a view to attaining and sustaining the desired level of health development in
Nigeria, (as reflected in the MDGs, and other national policy targets).
Objectives The primary objectives of the National Public Private Partnership Policy in Health shall be to:
Build confidence and trust in the public and private health sectors , Harness confidence and trust in the public and private sectors for the attainment of
Millennium Development Goals, and other National Health Policy Targets. Promote and sustain equity, efficiency, accessibility and quality in health care
provisioning through the collaborative relationships between the public and private sectors.
Identify areas of need in which collaborations and partnerships are desired on long and short-term basis
Develop the regulatory framework for public and private interactions and collaborations in health care delivery in the country.
Facilitate universal access to a Minimum Health Package.
Support capacity building across the public and private sectors in health care provisioning
Contribute to the sustainability of the overall health system
Build the National Health Management Information System (NHMIS).
Underscore the contribution/roles of each of the sectors/partners in the partnership to
health care delivery.
Roles and Responsibilities of the Private Sector
Private for Profit Partners shall: Ensure and sustain professional and technical standards of health services in line with
national or state standards (i.e. be accredited). Submit reports (financial, Health Management Information Systems, etc) in line with
agreed reporting requirements. Establish and maintain the requisite capacities (management and administrative
expertise and systems) to negotiate, and participate in, PPPs. Fulfill reporting requirements (including HMIS reporting)
Ensure and provide training Participate in the transfer of technology
Build Operate and Maintain (BOM) Build Operate and Transfer (BOT) Undertake research Create financial concessions- to promote equity in service provision Ensure transparency in accounting Provide quick emergency relief
Private Not-for-Profit shall:
Ensure and sustain professional and technical standards of health services in line with
national or state standards (i.e. be accredited) Submit reports (financial, HMIS, etc) in line with agreed reporting requirements
Establish and maintain the requisite capacities (management and administrative expertise and systems) to negotiate, and participate in PPPs (including having they
systems to facilitate the receipt of grants from state authorities) Provide quick emergency relief
Encourage community participation in service delivery Undertake capacity building and training
Be part of the network of the referral system Monitor the community in order to identify eligible beneficiaries for government
supported programmes and services Provide advocacy to promote and sustain PPP Facilitate data collection from rural communities Be involved in, and promote, operational research Participate in planning, administration, and ownership of health and other social
programmes Ensure transparency in accounting
(Culled from National Policy on Public Private Partnership for Health in Nigeria, FMoH 2005)
THE ROLE OF OPTOMETRY IN PUBLIC HEALTH – Healthy Eyes, Healthy People…
Accidents involving the eye are greatly preventable with an increased knowledge of safety and
prevention. Forty thousand eye injuries are sports related each year. More than 2,000 injuries
occur each year from fireworks, and 1,000 eye injuries occur EACH DAY in the workplace.
Children's educational advancement is greatly deterred by vision problems. Only 14 percent of
kids entering first grade have ever had an eye exam. Most parents and educators do not
recognize that vision disorders are the number-one cause of handicapping conditions in
children!
“In Nigeria, 84% of all causes of blindness were either preventable or treatable. This is comparable to other reports from Nigeria and other countries in Africa such as Rwanda, Ghana, Mali, Sudan, Tunisia, Central African Republic, Niger, Cameroon, Kenya and Ethiopia and in South Asia (Bangladesh, Pakistan and India). …” – NNBVIS 2007.
These pointers above are just but a few reminder of the fact that majority of blinding
conditions are preventable. How then do we have so much blindness around our communities
and what do can we do to ameliorate and reverse these trends?
Optometrists with training and experience in public health need to
Assess community needs for vision care services, to determine which factors contribute
to treatment and prevention of visual system anomalies
To develop and apply quality assurance systems
To participate and provide leadership in health-related agencies
To foster public awareness of the need for vision care
Optometrists in public health are expected to have the capability to develop
Administer, and evaluate eye and vision health programs in research projects
Design and conduct epidemiological field studies
Use statistical methods for these data analyses
Develop and implement vision health education programs
Develop occupational health and eye safety programs.
WHY GET INVOLVED? ARE THERE ANY GAINS TO THIS?
Implication of Poor Optometric Participation in Public-Private ventures
1. Lack of social recognition by members of the public and government
2. Lack of government’s recognition during policy development, monitoring and
evaluations, research mobilization, and expert contribution to planning and strategy
formulation of vision related programs.
3. Reduced scope of optometric practice and consequently constricted Job opportunities
4. Lack of purpose in professional pursuit in the aspect of community and social
responsibility
5. Non-realization of World health targets like VISION 2020’s Right-to-Sight Initiative
Benefits of Optometric participation in Public-Private ventures
1. Increased local, National, and International recognition and acceptance of Nigerian
Optometrists.
2. Increased tendency to attract national and international support or assistance in
various public health-related projects and researches.
3. Produce closer-to-reality local statics for national planning so as to reduce reliance on
foreign assessment, and assessment by comparison to other countries.
4. Developmental economists have shown that the global cost of visual impairment is up
to $3 trillion, and the 6th largest cause of DAILY loss is attributable to avoidable blindness. The implication is that by investing more in eye care, governments get
returns by reducing the economic burden of blindness on all concerned, and get to make savings as the rate of past economic losses reduce.
5. In a family, where one member who often would be a bread winner suffers from blindness, the whole family gets drawn into poverty, a child would have to drop from
school to serve as a guide and provide personal support to that family member, others may also have to become emergency employees so as to earn funds to cater for such a
family. As cataract is the commonest cause of such situation, treatment leads to eventual restoration to economic activities and the freeing of other family members to pursue their goals.
Considering the MDG goals, the achievement of health thematic aspects will be accelerated if
only eye health could become of utmost importance at state and local government levels of
healthcare, and primary health would then have “eyes that see” and propel the vision of a
globe free of all inequalities, marginalization, non-equitable distribution of resources, etc.
CONCLUSION
In view of all we have been sharing, and despite the challenging realities, we strongly believe that “WE CAN” change the current trends and restore the dignity of humanity, by s upporting the basic right of all to sight. All stakeholders have to come together, the Federal Government through the auspices of the currently re-packaged NATIONAL EYE HEALTH PROGRAMME serving as an active clearing house for the activities of all organizations in a public-private mix; elucidation of action plans and programmes that address long-term needs, close working with the terms, goals, and strategies of VISION2020: THE RIGHT TO SIGHT INITIATIVE, and strengthening the health information systems to accommodate eye care data management, robust monitoring and evaluation of programmes and encouragement of research activities to ensure sustainability of such programmes through re-programming as the case may be.
We need massive campaigns that will cut across all media systems and tools, to re-educate the masses, and reap the benefits of behaviour change communications; Corporate bodies need to
do more in the support of organizations running programmes and projects that give leverage to prevention of blindness activities in underserved communities; Local NGOs have to seek
partnerships with several state governments yet to elucidate clear vision2020 strategies and activities, with an aim of jointly developing sustainable and working systems of primary and
secondary care in those localities.
Innovations centering on health insurance schemes may be a great way of dealing with the
dilemma of lack of ability for out-of pocket payment for care.
Many optometrists and optometric practices have a tradition of embarking on Outreaches to
various communities. Some do it as a means of fulfilling their corporate responsibility to the
host locality, some out of public-health drive of disease prevention, but many others see it as a
fast profit-making venture and faster advertisement opportunity. Perhaps, after today, we are
being urged to see our undertakings as a call to the realization of the set goals of VISION 2020’s
Right-to-Sight initiative, such that outreach visits will henceforth be an opportunity to generate
records, offer health education on eye health, and provide quality eye care or referral to the
public. Records generated can be made available to the ever teaming streams of students and
their supervisory academic researchers who would willingly make analysis from your generated
data. To do this, we are advised to here on proceed with a detailed clinic record sheet or other
input and storage devices to our outreaches so that relevant data can be collected.
As primary eye care providers, we are educators, advocators, facilitators, and spokespersons.
We must utilize our role and ability to make a greater impact on the vision health of our
patients. By doing this, we are in turn enhancing their overall health, and therefore promoting
public health within our communities and profession. This is the first time vision health has
been placed "at the table of public health,” and this is your opportunity to get involved and
make an important difference.
Professional Reflection
Most often than not, the Nigerian Optometric Association is seldom called to the table of
deliberations on health matters in our respective states and the national levels at large. Most
recruiting offices would never even request for a membership certification as verification of
authenticity. This is a clarification to us that we have not shown our relevance to the Nigerian
people, due to the common self-centered attitudes which reflect in our poor participation in the
execution of Corporate and Social responsibilities, adamancy to embrace the nations’ call for
public private partnerships. Recognition comes with responsibility. If we have not been assigned
one yet by our government or the populace, let us not forget that assigned us by the profession.
Let this serve as a wakeup call to a duty we have ignored for long, as I charge the NOA today,
to lead the way in encouraging chapters and individuals toward the propagating the
optometric gospel, by actions and sacrifices, individually and collectively, so we can uplift this
profession to enviable standards.
REFERENCES
Adeolu O.O. (2010). ICT For Public Health Care Delivery In Nigeria: Challenges, Opportunities
and Milestones Paper presentation at the e-Nigeria 2010 Conference.
Blindness in Nigeria: A public health challenge awaiting our collective action in The NATION Newspaper, October 2012.
Faal H, Minassian D.C., Dolin P.J., Mohamed A.A., Ajewole J., and Johnson G.J. ((2000). Evaluation of a national eye care programme: resurvey after 10 years. Br J Ophthalmol, 84: 948-951.
Federal Republic of Nigeria Revised National Health Policy Federal Ministry Of Health Abuja September, 2004.
Kevin D. F (2009); Public Health Optometry Economics in Optometric Care Within the Public Health Community, Pp. 1-12.
National and State Population Projections (2002). Nigerian Population census 1991. Analysis.
Vol. VI. National Population Commission, Abuja. Nigeria. p.23
National Policy on Public Private Partnership for Health in Nigeria Federal Ministry of Health, Abuja. November, 2005.
National Programme for the Prevention of Blindness, Federal Ministry of Health, Abuja, Nigeria.
Negrel A.D., Avognon Z., Minassian D.C., Babaqbeto M., Oussa G., Bassabi S. (1995): Blindness in Benin. Med Trop, 55:409-414.
Nigeria Vision 20:2020 The First National Implementation Plan (2010 – 2013) Vol.II: Sectoral Plans and Programmes, May 2010.
Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. World Population Prospects: The 2006 Revision and World Urbanization
Prospects: The 2005 Revision. http://esa.un.org/unpp
Preamble to the Constitution of the World Health Organizatio as adopted by the International Health Conference, 1946.
The Nigeria national blindness and visual impairment survey 2005-2007
Wilson MR, Mansour M, Ross-Degnan D, Moukouri E, Fobi G, Alemayehu W, Martone JF, Casey R, Bazargan M. Prevalence and causes of low vision and blindness in the Extreme North
Province of Cameroon, West Africa. Ophthalmic Epidemiol 1996;3:23-33.
World Bank Nigeria: Country Brief http://web.worldbank.org/ WBSITE/EXTERNAL/COUNTRIES/AFRICAEXT/NIGERIAEXTN/0, menu PK: 368906~ page PK:
141132~ pi PK: 141107~ the Site PK: 368896, 00. Html