Embed Size (px)
DESCRIPTION
Citation preview

PUBLIC HEALTHDr. KICHA .D.
SUBMITTED BYSUBMITTED BY : :ASOGWA INNOCENT KINGSLEYASOGWA INNOCENT KINGSLEY
ML-508 ML-508

INTRODUCTION HEALTH FOR ALL HEALTH FINANCING IN NIGERIA SOCIAL HEALTH INSURANCE NHIS AND HEALTH FOR ALL CONCLUSION

Over the years, nations have realized the need for developing effective health systems
Such systems seek to protect their citizens from financial consequences of ill health.
Health care affordability and access have become central themes.
Providing Health for All is a function of access, affordability and equity.

Characterized by:
Lack of access to basic healthcare Inadequate preventive health care services. Inadequate health resources. Inefficient utilization of scarce health
resources Goals of equitable access to quality health
care rarely achieved. Poorly performing health systems.

Poor funding. o About US$9.44.00 per capita(WHO recommends
minimum US$34.00.o < 5% of total budgetary expenditure (WHO
recommends minimum of 15%) Poor health indices
o High IMR: 100/ 1,000 (NDHS 2003)o MMR: 1100/ 100,000 live births (WHO 2007)o Reduced life expectancy (about 43 years)
Inequitable distribution of health care resources between urban and rural areas
Stewardship role of government – Ineffective.
Limited access to quality healthcare.


5.85
4.4
5.44.53.8
1.8
0
1
2
3
4
5
6
7
2007 2008 2009 2010 2011 2012 2013
Per
cent
Median National HIV Prevalence: Median National HIV Prevalence: 1992- 20051992- 2005

0
1
2
3
4
5
6
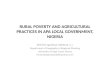
Total Health Expenditure as Ratio of GDP
Percent
YEAR

12.397.41
1.86.14
65.87
6.39
Percent
Federal Government
State Governments
Local Government
Donor
Household
Firms

Declaration by WHO members in 1978 for attainment by year 2000.
Global priorities and targets that would enable people worldwide to reach and maintain the highest attainable level of health.
Fundamental principle based on equity – equal health status for people and countries and an equitable distribution of health resources.
Attainment of the HFA goals anchored on primary health care

“… the attainment by all peoples of the
world by the year 2000 of a level of health that will permit them to lead a socially and economically productive life”.
Alma Ata declaration of 1978

Development of a global strategy and framework.
Nations and regions to adapt based on global strategy according to particular health problems and conditions.
Equity, solidarity and social justice core to goal attainment.
Funding and allocation of healthcare resources key to attaining goals.
Primary health care as core operational strategy.
Multisectoral approach. Improvement in healthcare facilities.

Primary health care adopted as means of achieving HFA.
Community participation an integral part of strategy.
Bamako initiative and DRF as parts of effort to improve resources and their allocation.
Strategies short of attaining HFA goals. Millennium Development Goals
introduced to augment other strategies.

General Taxation- up till late 80’s User fees Bamako initiatives DRF Donors Firms Social Health insurance – 2005 to
date.

Gaining global acceptance. Introduced in Nigeria in 2005. Based on mutual ethic of social
solidarity. Equity in access and in financing as core
attributes. Community participation expressed
through contribution into the fund.

Ensures that all people in need have effective access to at least essential care.
Alleviates the burden posed by ill health, loss of income etc.
Coverage reduces the indirect costs of disease and disability, such as care of family members, lower productivity, and hampered education and social development of children due to sickness.
Plays a significant role in poverty reduction
Incorporates all strategies for achieving HFA, including the MDGs.

“Implementing universal social health protection might turn out to be a milestone for achieving the MDG by 2015”
ILO (2007)

An agency of the Federal Government established by Act 35, 1999 to
promote, regulate and administer the effective implementation of social health insurance programmes in order to ensure easy access to qualitative and affordable health care services to all Nigerians.

• Improve access to good healthcare services (physical and financial)
• Protect families from the financial hardship of huge medical bills
• Limit the rise in the cost of health care services• Equitable distribution of healthcare costs
among different income groups• Improve standard of healthcare in Nigeria• Improve and harness private sector participation• Ensure equitable distribution of health facilities within
the Federation• Remove discrimination and ensure equitable
patronage of all levels of healthcare• Ensure the availability of funds to the health sector for
improved services.

Based on social health insurance principles. Contributions are income – related. Operated on Public – Private Partnership
basis. Compulsory for certain populations such as
formal sector workers. Contributions pooled into a single fund for
Formal sector programmes. Financing separate from health service
delivery.

To secure access to adequate health care for all Nigerians at an affordable rate (universal coverage) by the year 2015.

Formal Sector Programme (FSP)o Public Sector Programme (PSP)
Fed. Civil Service, State Civil Service, Local Government Civil Service, Tertiary Institutions, Military, Police and other Uniformed Services.
o Organized Private Sector Programme (OPSP)
Informal Sector Programme (ISP) Rural Community, Urban Self- Employed, Voluntary Participants, Retirees, Other Vulnerable Groups

For those in formal employment Compulsory for these workers Contributions are paid by employers and
employees Total contribution is equal to 15% of basic
salary Enrollees enjoy a benefit package made of
health services from three levels of healthcare Can attend private or Government hospital.

For those in the rural communities, self employed, the poor, pregnant women and Children Under 5 years
Requires targeted subsidy from Governments and other bodies
Efforts are on to secure Government financing of the subsidy gap.
Benefit package in line with the minimum basic primary care
Services to be provided mainly by Primary health centres.

NHIS well structured to achieve HFA. Programmes designed to cover all
citizens of Nigeria. Incorporates the core features of HFA
– equity, community participation, intersectoral collaboration etc.
NHIS advocacy needed for achieving HFA.

THANK YOU